


Abstract
See an invited perspective on this article on page 1043.
This multicenter phase II study investigated a selective radiotherapy dose increase to tumor areas with significant 18F-misonidazole (18F-FMISO) uptake in patients with non–small cell lung carcinoma (NSCLC). Methods: Eligible patients had locally advanced NSCLC and no contraindication to concomitant chemoradiotherapy. The 18F-FMISO uptake on PET/CT was assessed by trained experts. If there was no uptake, 66 Gy were delivered. In 18F-FMISO–positive patients, the contours of the hypoxic area were transferred to the radiation oncologist. It was necessary for the radiotherapy dose to be as high as possible while fulfilling dose-limiting constraints for the spinal cord and lungs. The primary endpoint was tumor response (complete response plus partial response) at 3 mo. The secondary endpoints were toxicity, disease-free survival (DFS), and overall survival at 1 y. The target sample size was set to demonstrate a response rate of 40% or more (bilateral α = 0.05, power 1-β = 0.95). Results: Seventy-nine patients were preincluded, 54 were included, and 34 were 18F-FMISO–positive, 24 of whom received escalated doses of up to 86 Gy. The response rate at 3 mo was 31 of 54 (57%; 95% confidence interval [CI], 43%–71%) using RECIST 1.1 (17/34 responders in the 18F-FMISO–positive group). DFS and overall survival at 1 y were 0.86 (95% CI, 0.77–0.96) and 0.63 (95% CI, 0.49–0.74), respectively. DFS was longer in the 18F-FMISO–negative patients (P = 0.004). The radiotherapy dose was not associated with DFS when adjusting for the 18F-FMISO status. One toxic death (66 Gy) and 1 case of grade 4 pneumonitis (>66 Gy) were reported. Conclusion: Our approach results in a response rate of 40% or more, with acceptable toxicity. 18F-FMISO uptake in NSCLC patients is strongly associated with poor prognosis features that could not be reversed by radiotherapy doses up to 86 Gy.
Radiotherapy is a major component in the treatment of nonresectable locally advanced non–small cell lung cancer (NSCLC) (1). Although concomitant radiochemotherapy (CCRT) is the current standard for curative-intent treatment, the tumor control rate and survival probabilities remain disappointing. Improvements in radiotherapy techniques should yield better intrathoracic control; a reduction in secondary distant dissemination; less normal-tissue damage; and as a consequence, reduced mortality caused by cancer, toxicity, or worsening of preexisting comorbidities. The identification of the adequate target volumes and the delivery of sufficiently high total doses are closely linked. Phase II studies have shown that higher doses could only be delivered to smaller target volumes (2,3). The RTOG 0617 randomized trial reported lower survival probabilities in the patients having received more than 60 Gy, possibly because the target volumes were too large (4). Therefore, it is tempting to reduce the target volumes and escalate the radiotherapy dose only to the most aggressive parts of the tumor. For example, the dose could be selectively increased in the tumor areas with the highest 18F-FDG uptake (5,6). Because oxygen is the most powerful radiosensitizer (7), we hypothesized that the hypoxic areas in the tumor would be relevant targets for selective dose escalation.
In a phase II study, we used 18F-misonidazole (18F-FMISO), a PET/CT tracer for hypoxic cells, to identify and delineate hypoxic areas as biologic target volumes (BTVs) for escalated total dose radiotherapy associated with concomitant chemotherapy. A rigorous quality assurance protocol was set to ensure that all PET/CT images were acquired under reproducible conditions. The presence of 18F-FMISO uptake was assessed by consensus by trained experts (8). The BTVs were centrally delineated. The primary endpoint was the tumor response at 3 mo after CCRT. The secondary endpoints were acute and late toxicity, as well as disease-free survival (DFS) and overall survival (OS) at 1 y.
MATERIALS AND METHODS
Study Design and Patients
The design of the study is described in Figure 1. Between June 6, 2012, and March 19, 2015, the patients with NSCLC referred to the participating centers for CCRT were prospectively preincluded. Fifteen academic centers included patients into the study.
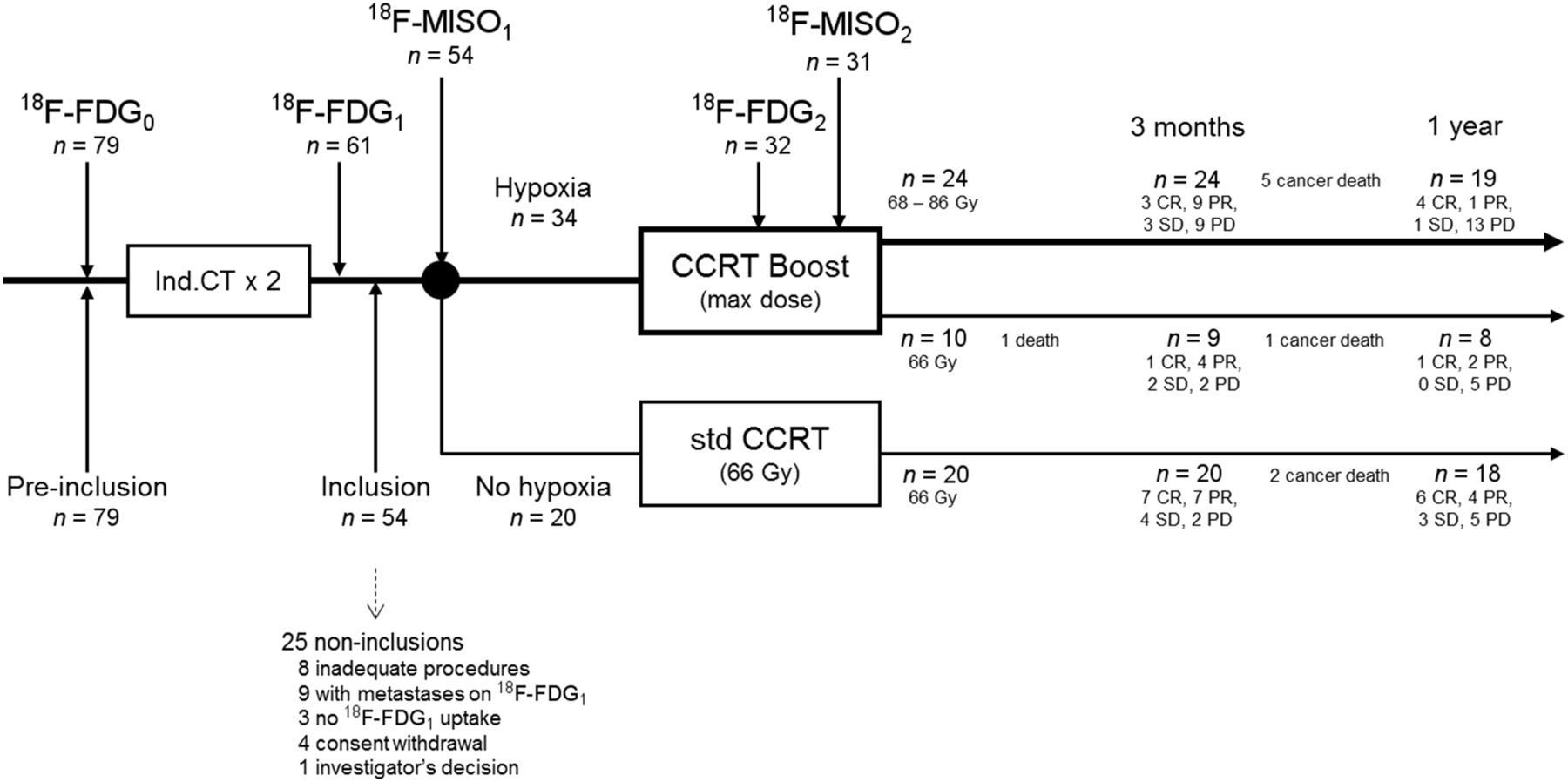
Study design/study flow. SD = stable disease; PD = progressive disease (RECIST 1.1).
The main inclusion criteria were age older than 18 y; histologic proof of NSCLC with a measurable tumor (RECIST1.1); World Health Organization performance status of 1 or less; eligibility for curative-intent CCRT (no pleural, pulmonary, or extrathoracic metastases and no comorbidity contraindicating CCRT); adequate lung function (forced expiratory volume ≥ 40% and diffusing capacity of the lung (divided by the alveolar volume ≥ 50% of the predicted values; PaO2 ≥ 60 mm Hg); a neutrophil count of more than 1.5 × 109 cells/L, platelet count more than 100 × 109/L, and hemoglobin more than 10 g/dL; and an estimated creatinine clearance of more than 60 mL/min. All patients had to receive cisplatin-based chemotherapy as the induction treatment and concomitantly with radiotherapy. Inclusion was confirmed after completion of a radiotherapy plan confirming that the dose objective (a minimum dose of 60 Gy in 99% of the planning target volume) and the constraints (lungs, spinal cord) could be met.
The noninclusion criteria were histology other than primary NSCLC; a nonevaluable lesion (complete remission after induction chemotherapy); no uptake or metastases on the first acquisition of 18F-FDG PET/CT (18F-FDG1 PET/CT) performed after the induction chemotherapy and before CCRT; contraindication of curative-intent radiotherapy (tumor extension, World Health Orgainziation performance status ≥ 2, coexistent disease); synchronous cancer or previous malignancy within 5 y before inclusion; patient already participating in another clinical trial; confirmed or suspected pregnancy and lactating females; renal insufficiency contraindicating cisplatin treatment; patients under legal protection; inability to comply with the follow-up procedures for geographic, social, or psychologic reasons; uncontrolled diabetes mellitus (blood glucose ≥ 10 mmol/L); and patients unable to give informed consent.
The eligible patients had to have at least 1 18F-FDG–avid lesion at 18F-FDG1 PET/CT. These patients were then considered to have hypoxic lesions if significant 18F-FMISO uptake was observed in the 18F-FDG–avid lesions on a subsequent first 18F-FMISO performed before CCRT (18F-FMISO1) PET/CT scan within 8 d. The evaluable population was formed from all the eligible patients who completed the protocol (a complete mandatory dataset is included at the end of the study). The patients who eventually withdrew their consent to participate were not evaluated.
The protocol and the consent form were approved by the Comité de Protection des Personnes Nord-Ouest 1 (July 21, 2011). All patients gave their written, informed consent. The study was registered in the Clinical Trials Protocol Registration System (NCT01576796; RTEP5 study). The clinical, biologic, imaging, and toxicities data were monitored by a certified clinical research unit.
PET Imaging
The PET/CT machines were Biograph Sensation 16 (Siemens), Gemini (Philips), or Discovery LS (GE Healthcare). For each patient, 2 18F-FDG PET/CT and 2 18F-FMISO PET/CT scans were acquired using the same machine and under the identical operational conditions. Quality control (QC) was centrally supervised to secure homogeneity in the image quality in all participating centers. The QC procedures and results are provided in the supplemental materials (available at http://jnm.snmjournals.org).
The 18F-FDG PET images were acquired in treatment position (arms over the head, free breathing), at least 15 d after the last administration of chemotherapy. No chemotherapy was allowed between the PET/CT and the start of radiotherapy. Six to 8 bed positions per patient were acquired from the head to the upper third of the thighs. The images were acquired at a minimum of 60 ± 10 min after the 18F-FDG injection. The patients were required to fast overnight or for at least 6 h before the imaging to ensure that the serum glucose and endogenous serum insulin levels were low at the time of the 18F-FDG administration. The blood glucose levels were measured before each 18F-FDG PET acquisition. A total of 4.5 MBq/kg were administered intravenously after a rest period of at least 20 min. The first acquisition (18F-FDG1) after the induction chemotherapy started at T1 = 60 ± 10 min after injection. The second 18F-FDG PET (18F-FDG2) was performed during the fifth week of radiotherapy at a total dose of 40–46 Gy as previously demonstrated (9). The acquisition procedure followed conditions identical to those for 18F-FDG1, specifically, with a T2 = T1 ± 5 min.
The 18F-FMISO PET images were acquired under identical conditions. Two to 3 bed positions per patient were acquired for the thorax. The images were acquired at a minimum of 240 ± 20 min after the 18F-FMISO injection. A total of 4.5 MBq/kg were administered intravenously after a rest period of at least 10 min. A first 18F-FMISO PET (18F-FMISO1) was scheduled after induction chemotherapy, 48 h after the 18F-FDG1. The second 18F-FMISO PET (18F-FMISO2) was performed during the fifth week of radiotherapy, within 48 h after the 18F-FDG2.
For all the 18F-FDG and 18F-FMISO acquisitions, the CT scan data were used for random coincidences, scatter and attenuation correction, and anatomic localization. The PET images (18F-FDG and 18F-FMISO) were fused with the CT scan images. The 18F-FMISO PET images were finally smoothed with a gaussian filter (full width at half maximum, 5 mm).
PET Analysis
We previously showed (8) that the assessment of 18F-FMISO/18F-FDG uptake (presence vs. absence) was reproducible in a multicenter setting. In this study, 3 independent experts (of 9) reviewed the 18F-FMISO PET acquisitions and decided on the presence or absence of uptake within 48 h.
Because the interobserver agreement for the 18F-FMISO volume measurements was low (8), all images were centrally delineated in a single center (Rouen) by a nuclear physician and a radiation oncologist, via a dedicated network (Imagys Interface [QI/QO/QA/QC] and Keosys workstation). (Keosis Imagys Interface [QI/QO/QA/QC] is 21-CFR part 11–compliant. The Keosys company is ISO 9001 and ISO 13485 medical device–compliant. Images were stored and archived on a dedicated IIA class server.) For each patient, the CT image of PET 18F-FDG and 18F-FMISO was first coregistered to the planning CT scan (version 1.4, Oncoplanet; DosiSoft) with registration based on the lesion. The volumes of interest for 18F-FDG metabolic biological target volume (BTVm) were defined as the sum of the pixels above 40% of the SUVmax inside the primary tumor or nodes (10). The volumes of 18F-FMISO (biologic hypoxic target volume [BTVh]) were defined as the sum of pixels with an SUV 1.4 or more as previously validated (8). The coregistered 18F-FDG and 18F-FMISO PET/CT (DICOM), as well as BTVm (18F-FDGBTV) and BTVh (18F-FMISOBTV) (DICOM-RT), were transferred back to the local radiation oncologist by the same network.
In addition, the 18F-FDG and 18F-FMISO images on PET after the induction chemotherapy (PET1) and during radiotherapy (PET2 at 40–46 Gy) were used to calculate the maximum SUVs (PETSUVmax1 and PETSUVmax2)—that is, the highest-activity pixel value in the BTVs—and the percentages of variation in SUVmax (Δ%SUVmax) and BTV (Δ%BTV). The SUVmean yielded results similar to those of the SUVmax and are not presented here.
Radiochemotherapy Protocol
The microscopic extension around the BTVm (clinical target volume [CTV]) was obtained either by isotropic expansion around the tumor (6 mm for squamous cell carcinoma, 8 mm for adenocarcinoma) (11) or by delineation of the 18F-FDG PET/CT–positive mediastinal nodes (12). The isotropic CTV margin around the BTVh was set to 5 mm. The margin for the planning target volume (PTV) was 10 mm around the CTV (possibly 15 mm in the craniocaudal direction) to take into account internal movements and uncertainties in positioning.
All the dose calculations were corrected for heterogeneity. Intensity-modulated radiotherapy (IMRT) was not allowed. The total dose was prescribed by the International Commission for Radiation Units point. The dose delivered in the PTV had to be within 95% and 107% of the prescribed dose. The target total dose was 86 Gy, provided that the maximum dose to the spinal cord was strictly less than 46 Gy and that no more than 30% of the total lung volume (excluding the gross tumor volume) received more than 20 Gy. As minor constraints, no more than 30% of the esophagus or the heart could receive more than 50 or 35 Gy, respectively.
The patients received 5 daily fractions of 2 Gy every week, with all the beams being treated daily. The shape of each beam was checked (electronic portal image) on the first fraction. The position of the isocenter was imaged daily (by orthogonal image or cone-beam CT scanner). Concomitant chemotherapy was cis-platinum (50 mg/m2 days 1, 8, 29, and 36) and etoposide (50 mg/m2 days 1–5, and 29–33) or cis-platinum (80 mg/m2 days 1 and 22) and vinorelbine (15 mg/m2 days 1, 8, 22, and 29). Cis-platinum could be replaced by carboplatin AUC 5 in the case of renal insufficiency.
Follow-up Procedures
The efficacy and toxicity assessments were planned at 3 mo and 1 y after the end of treatment (clinical examination, CT scanner).
Endpoints
The primary endpoint was the tumor response on CT scan at 3 mo (RECIST 1.1). Complete response (CR) was defined as no residual tumor image. Partial response (PR) was defined as a more than 30% reduction in maximal diameter. Progressive disease was defined as a more than 20% increase in the maximal diameter, whereas variations between −30% and +20% were classified as stable disease. The secondary endpoints were early and late toxicity (Common Terminology Criteria for Adverse Events) as well as DFS and OS at 1 y from definitive inclusion.
Sample Size
This open-label, single-arm, nonrandomized, multicenter phase II study followed a Gehan 2-step design. In the first step, 6 patients had to be evaluable 3 mo after completion of treatment. If no CR or PR was observed, a response rate of more than 40% would be excluded, with 95% power and accrual stopped. If at least 1 response was observed, the number of additional patients to be entered in step 2 was calculated assuming an a priori response rate (complete or partial) of 40%, power 1-β = 95%, precision ε = 10% and the number of responses in step 1, that is, 19, 18, 15, and 8 additional patients if 1, 2, 3, or 4 responses in step 1, respectively.
The number of patients to include was calculated as follows to obtain 25 patients evaluable at 3 mo (and 15 patients alive at 1 y, a 50% OS probability). Assuming 5 deaths/lost for follow-up at 3 mo, 30 patients with hypoxic lesions should be recruited and receive CCRT. Assuming that 50% of 18F-FMISO1 PET/CT would demonstrate the presence of hypoxic lesions, 60 preincluded patients should have persistent 18F-FDG uptake on the postinduction chemotherapy 18F-FDG1 PET/CT. We anticipated that 20% of the patients would have a negative 18F-FDG1 PET/CT result after induction chemotherapy (9). Therefore, a total of 75 patients would have to be preincluded. The 30 patients without 18F-FMISO–avid lesions would be monitored for 1 y (a secondary endpoint).
Statistical Analysis
All analyses were conducted according to intent to treat, for example, irrespective of the radiotherapy total dose that was actually delivered. Descriptive statistics (n, mean, SD minimum and maximum) were calculated for the quantitative variables. Frequency and percentages with 95% confidence intervals (CIs) were determined for the qualitative variables. A Levene test was used to assess the equality of variances before comparing the quantitative variables between 2 or more groups (ANOVA). The survival probabilities were compared with a log-rank test. All the significance thresholds were set at 0.05 (2-tailed test). All the statistics were performed using SPSS software (version 20.0; IBM).
RESULTS
Patient Characteristics, Flowchart, and Descriptive Results
The study flow is shown in Figure 1. Seventy-nine patients were preincluded, and 54 patients were definitely included. The reasons for noninclusion were as follows: 8 inadequate procedures, 9 metastases and 3 with an absence of uptake on the 18F-FDG1 PET/CT, 4 consent withdrawals, and 1 investigator’s decision. Thirty-four patients were eligible for the experimental group (18F-FDG1–positive and 18F-FMISO1–positive).
The 54 definitively included patients were predominantly men (7 women and 47 men), with a mean age ± SD of 60.3 ± 7.7 y (Table 1). The histologic subtypes were 26 (48%) squamous cell carcinomas, 21 (39%) adenocarcinomas, and 7 (13%) undifferentiated carcinomas. The disease stages were mostly IIIA and IIIB. The descriptive data of the 79 preincluded patients were not significantly different (data not shown).
Baseline Characteristics of 54 Included Patients
In the experimental arm, 24 of 34 (71%) patients received increased radiotherapy total doses (86 Gy, 5 patients; 80 Gy, 2; 76 Gy, 8; 74 Gy, 5, 72 Gy, 2; 70 Gy, 2). Because of organ-at-risk constraints, the dose was limited to 66 Gy in 10 patients. Among the 20 patients without 18F-FMISO uptake, 19 received 66 Gy, and 1 received 68 Gy.
PET Description
The PET data are reported in Table 2. For the 54 included patients, the 54 18F-FDG1 and 54 18F-FMISO1 were available before the CCRT. In the 34 of 54 patients with hypoxia, 32 of 34 18F-FDG2, and 31 of 34 18F-FMISO2 could be performed during the CCRT at 42 Gy (missing PETs because of medical or technical problems). The mean time intervals between injection and imaging were 66 (SD = 10) and 236 (SD = 6) min for the 18F-FDG and 18F-FMISO PET/CT, respectively. A total of 103 lesions (40 primary tumors and 63 nodes) were observed in the 54 patients. The per-patient and per-lesion analyses gave similar results. We present only per-patient PET data.
PET Data of 54 Included Patients
The patients with hypoxic lesions had significantly higher 18F-MISO1 SUVmax than the patients without hypoxia (P < 0.001). Similarly, the patients with hypoxia had higher 18F-FDG SUVmax1 (P = 0.02) and larger 18F-FDGBTV1 tumor volumes (P = 0.03). The BTVs delineated on PET after the induction chemotherapy were approximately 40% smaller with 18F-FMISO than with 18F-FDG (SD = 54%), without statistically significant differences between the radiotherapy dose groups. For the 34 hypoxic patients who underwent 18F-FDG (n = 32) and 18F-FMISO (n = 31) during CCRT, 18F-FDG SUVmax, 18F-FDGBTV, and 18F-FMISO SUVmax significantly decreased during CCRT.
Toxicity
Acute and late toxicities are listed in Tables 3 and 4, respectively. There was 1 grade 4 acute pneumonitis case among the 24 patients who received escalated radiotherapy doses. Three acute grade 4 toxicities were observed in the patients having received 66 Gy (whatever their 18F-FMISO uptake). One death (hemoptysis) occurred before the evaluation at 3 mo among the 10 patients with 18F-FMISO uptake and having received 66 Gy. No grade 4 or 5 late radiotherapy-related adverse events or acute/late cardiac toxicities were reported in the entire population. The causes of the 19 reported deaths are described below.
Acute Toxicity at 3 Months for 54 Included Patients
Late Toxicity for 54 Included Patients (1 Year)
Tumor Response and Survival
The survival curves are presented in Figure 2. The tumor response was evaluated at 3 mo (±7 d). The patient who died before evaluation at 3 mo in the 18F-FMISO–positive/66-Gy group was considered as having a nonresponding tumor. The response (CR+PR) rate at 3 mo was 31 of 54 (57% with 95% CI, 43%–71%). The corresponding figures were 17 of 34 (50%; 95% CI, 34%–66%) in the patients with 18F-FMISO uptake versus 14 of 20 (70%; 95% CI, 48%–85% in the patients without uptake (P = 0.25). In the 18F-FMISO–positive patients, the response rates were 12 of 24 (50%; 95% CI, 31%–69%) after the escalated radiotherapy doses and 5 of 10 (50%; 95% CI, 24%–76%) after 66 Gy.
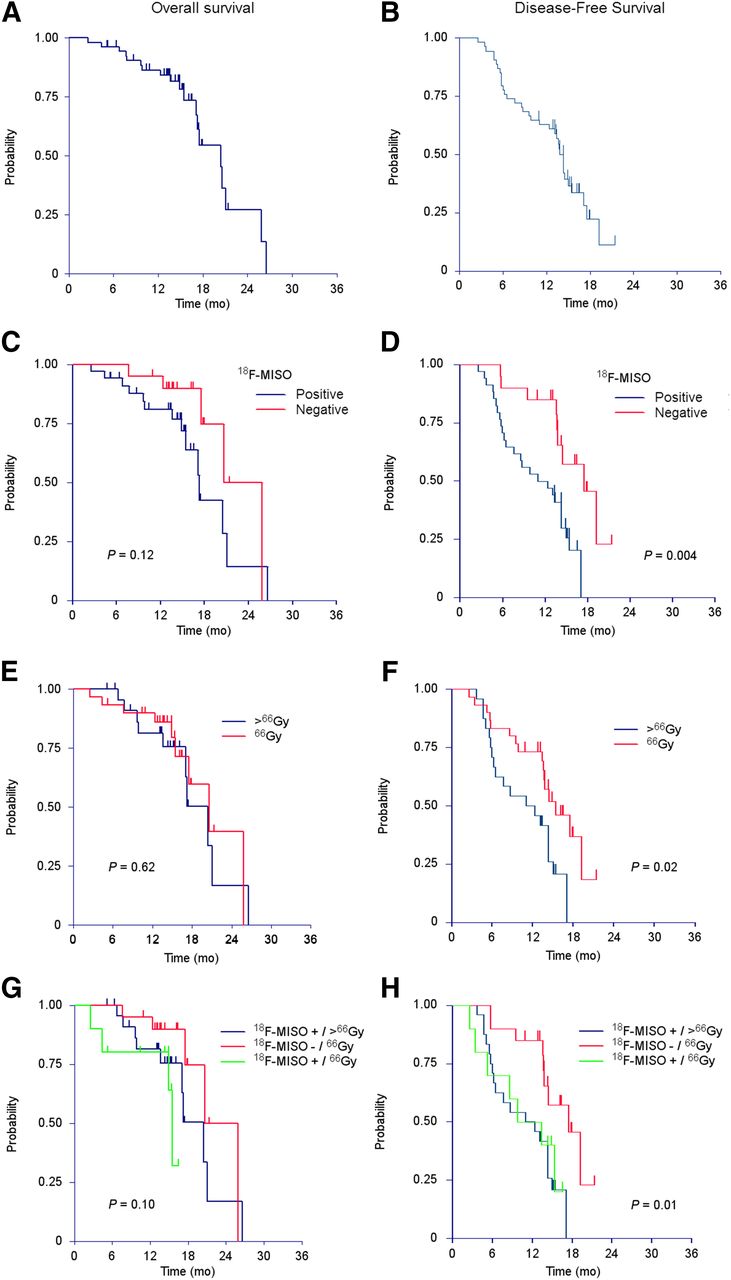
OS (left) and DFS (right), for entire population (A and B) as well as separation for the 18F-FMISO PET result (C and D), dose radiation (E and F), and both 18F-FMISO PET and dose radiation (G and H).
At the date of point, 35 patients were alive (a median follow-up duration of 14 mo [range 5–21 mo]), and 19 were alive without disease (15 mo [range, 11–21 mo]). Sixteen of the 19 deaths were due to cancer (9/10 in the high-radiotherapy-dose group, 3/4 in the 18F-FMISO–positive group, and 4/5 in the 18F-FMISO–negative group). The patient in the 18F-FMISO–positive/66-Gy group who died at 3 mo was discussed above. One patient in the high-radiotherapy-dose group was receiving nivolumab for progression under pemetrexed/bevacizumab maintenance. He died at home 17 mo after inclusion, and the cause of death remains unknown (drug toxicity or tumor progression). One patient in the 18F-FMISO group, without previous documentation of a relapse, was admitted to a palliative care unit with cognitive impairment, fever, and intestinal bleeding. He refused investigations and died at 18 mo. The OS and DFS probabilities at 1 y for the entire group were 0.86 (95% CI, 0.77–0.96) and 0.63 (95% CI, 0.49–0.74). Regarding the 18F-FMISO uptake, the OS at 1 y was 0.81 (95% CI, 0.67–0.95) when positive and 0.95 (95% CI, 0.85–1.0) when negative (P = 0.12). The DFS at 1 y was 0.50 (95% CI, 0.32–0.65) and 0.85 (95% CI, 0.60–0.95), respectively (P = 0.004). The DFS was lower after radiotherapy doses larger than 66 Gy (0.50 [95% CI, 0.29–0.68] vs. 0.73 [95% CI, 0.54–0.86], P = 0.02). In the 18F-FMISO–positive patients, the DFS was similar regardless of whether the radiotherapy dose was 66 Gy (0.50 [95% CI, 0.18–0.75]) or higher (0.50 [95% CI, 0.29–0.68]).
DISCUSSION
Our purpose was to increase the total dose of radiotherapy in the hypoxic parts of NSCLC in patients who were candidates for curative-intent chemoradiotherapy. Hypoxia has been shown to strongly reduce the radiosensitivity of tumor cells and to be associated with local failure (7). In this study, a key issue was to timely provide the radiation oncologists with a reliable target, anatomically and functionally defined, in a prospective multicenter setting. We have demonstrated that hypoxic areas were identified using 18F-FMISO PET in 34 of 54 patients (15 centers) and that higher radiotherapy doses (70–86 Gy) could be delivered without excessive toxicity in 24 patients with hypoxic areas. There were no statistically significant differences in the tumor response rates at 3 mo, and the OS at 1 y was similar among the 3 treatment groups. The DFS probability was significantly lower in the 18F-FMISO–positive patients, regardless of the radiotherapy dose. To our knowledge, we present the largest series of patients with NSCLC receiving radiotherapy boosted based on the hypoxia PET/CT in multicentric and prospective conditions.
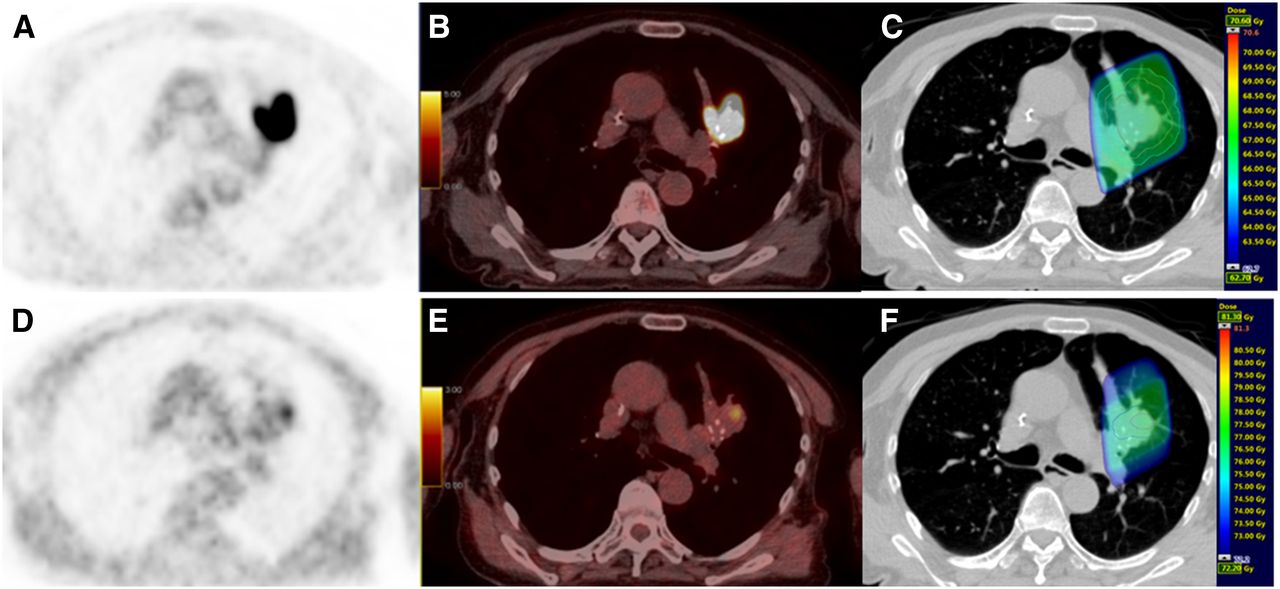
As a targeted treatment, radiotherapy critically depends on accurate delineation of the volumes to be irradiated. A conventional CT scan is necessary for planning (Hounsfield units being correlated to electronic densities) and for drawing the anatomic contours of the tumor and the organs at risk. As for functional information (e.g., glucose metabolism with 18F-FDG), the PET/CT images must be either acquired in the treatment position or registered onto the planning CT. 18F-FMISO is one of several tracers that accumulate in hypoxic areas (13) and was selected for this study because it is commercially available. Although this study was ongoing, the MAASTRO group demonstrated (using HX4) that hypoxia images were stable when PET/CT was repeated (14) and provided a representation of the tumor functional status that was different from 18F-FDG images (15). A planning study of 10 patients by the same group showed that hypoxia images could be used to consider delivering heterogeneous doses to the tumor, specifically higher doses to hypoxic areas (16). All the PET tracers of hypoxia yield a relatively low signal-to-noise ratio. Therefore, the initial step of this study was to validate a reproducible method to identify the tumors with hypoxic areas and delineate BTVs for radiotherapy (8). The patients with hypoxia were identified by at least 3 trained experts, and the delineation of all the BTVs was centralized in 1 center. An example of 18F-FDG and 18F-FMISO images with BTV are presented in Figure 3.
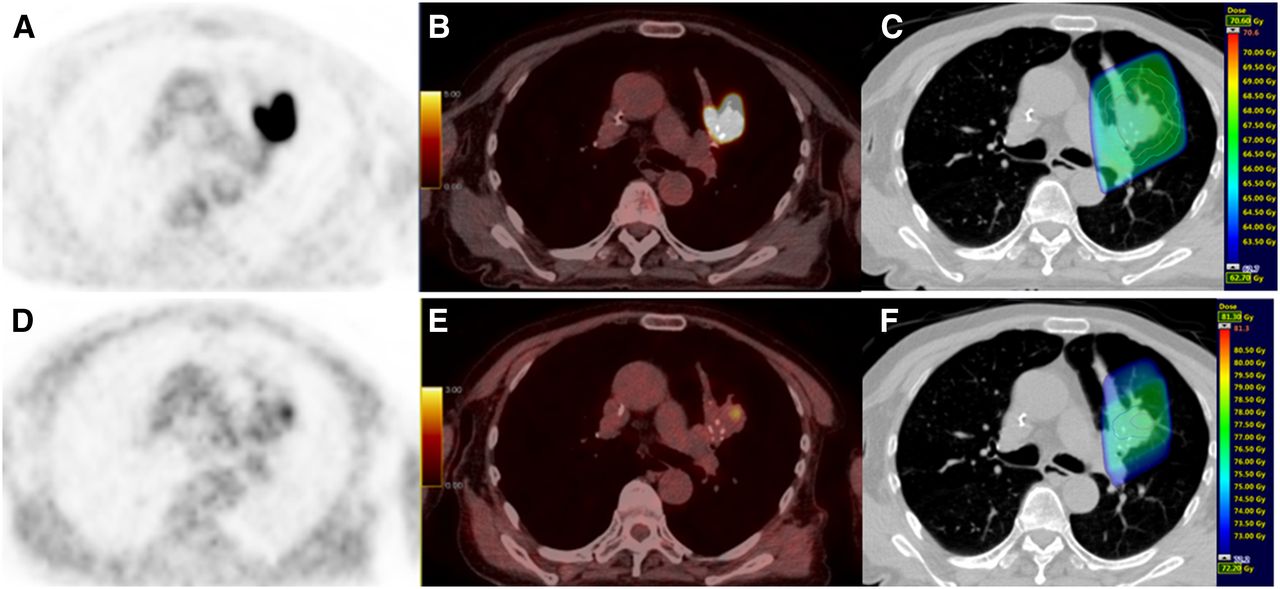
Example of patient with upper left lung NSCLC: 18F-FDG (A); 18F-FDG PET/CT (B); planning radiotherapy based on 18F-FDG (66 Gy) with BTVm (gross tumor volume), CTV, and PTV (C); PET 18F-FMISO (D); 18F-FMISO PET/CT (E); and boost based on 18F-FMISO PET (76 Gy) with BTVh and PTV boost (F).
We did not gate our PET acquisitions on breathing movements. Because 18F-FMISO uptake is known to be low in lung tumors (SUVmax = 2.5 [±0.7] in our study), good-quality images cannot be obtained in respiratory gated mode, either for SUV measurement or for BTVh delineation. Our criteria for BTVh delineation was validated in free-breathing patients. We chose not to add further complexity to our design by requiring gated PET acquisitions and, for the sake of consistency, irradiations. In addition, mobile tumors are usually small and located in the parenchyma whereas most stage III tumors are large (and take up 18F-FMISO) and involve the mediastinum, that is, are mostly fixed. Lin et al. (17) have suggested a low reproducibility of 18F-FMISO PET images performed within 48 h. More recently, a preclinical study by Busk et al. (18) showed a good reproducibility of PET FAZA images acquired within 48 h (r = 0.82; range, 0.72–0.90), and Zegers et al. demonstrated the reproducibility of PET HX4 images in a human study (14). Mathematic simulations based on microscopic tumor tissue sections compared 18F-FMISO, FAZA, and HX4 and showed that 18F-FMISO provides a robust and reproducible signal 4 h after injection, with a lower contrast (19). Our observation that 18F-FMISO–avid tumors have a much worse prognosis confirms that hypoxia imaged on a single PET acquisition is a strong prognostic indicator, making it a relevant target volume for selective radiotherapy dose increase.
Radiobiologic and clinical data (7) suggest that total doses above 80 Gy are required to achieve tumor control in NSCLC. The RTOG 0617 (4) randomized trial reported reduced OS probabilities in patients receiving 74 Gy (vs. 60 Gy) in a target volume (median, 90 cc) defined on 18F-FDG PET/CT. Phase I–II studies have shown that doses in excess of 80 Gy could only be delivered to small tumors (2,3). Our BTVs delineated on 18F-FMISO PET/CT are approximately 40% smaller than those delineated on 18F-FDG PET/CT. Our results indicate that 18F-FMISO uptake is associated with a worse outcome, regardless of the radiotherapy total dose. An increased 18F-FMISO uptake was correlated with other poor prognosis features (larger tumor size, higher 18F-FDG SUVmax), and hypoxia might not be the sole reason for treatment failure. The absence of 18F-FMISO uptake identifies a group of tumors with better prognosis. Our OS and DFS at 1 y compare favorably with those reported by RTOG 0617 (0.80 [95% CI, 0.74–0.85] and 0.49 [95% CI, 0.42–0.56], respectively) in their patients treated to 60 Gy (4). Similar approaches are being evaluated in clinical trials increasing total dose to smaller subvolumes that are considered at higher risk of failure (high 18F-FDG uptake subvolumes on preradiotherapy 18F-FDG PET/CT (RTOG 1106 NCT01507428, PET Boost NCT01024829), residual tumor at midtreatment 18F-FDG PET/CT (RTEP 7, NCT02473133).
An extensive discussion about radiotherapy dose and delivery is beyond the scope of the present paper. Briefly, our patients were irradiated with a 3-dimensional conformal technique. When our trial was designed, IMRT was available in too few French centers. IMRT was used in approximately 50% of the RTOG 0617 patients with outcomes similar to 3-dimensional RT (4). The dosimetry benefits of IMRT have not been confirmed in a randomized trial (20). The dosimetry of protons is characterized by localized high-dose delivery and sharp fall-out (Bragg peak) (21). No significant differences in tumor outcome were observed in a randomized comparison of 3-dimensional proton therapy versus IMRT (22). Radiotherapy in stereotactic conditions is an accepted treatment for tumors up to 65 cc, provided that strict organ at risk dose–volume constraints are met (23). Our patients had mean 18F-FMISO–avid volumes of 33.5 cc, with large variability (SD = 52.2 cc; range, 1–234 cc). A few additional fractions could be delivered, intended as a concomitant boost, whereas the 18F-FDG–defined target volume is be treated conventionally (2 Gy per fraction), keeping the treatment duration around 6–7 wk. The positive results of accelerated radiotherapy (24) suggest that tumor proliferation during radiotherapy might have contributed to the failure of escalated radiotherapy dosage delivered over a protracted treatment time to improve the outcome in NSCLC (4).
CONCLUSION
This prospective phase II study demonstrates the feasibility of delivering higher radiotherapy doses to smaller target volumes identified by 18F-FMISO uptake without exceeding the tolerance to the normal organs. The benefit of this approach, possibly with larger doses per fraction in stereotactic conditions as a concomitant boost, remains to be investigated in a randomized trial.
DISCLOSURE
This study was supported by a grant from the French National Cancer Institute (PHRC 2011). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the patients who agreed to participate in this study and their respective referring pneumologists, nuclear medicine physicians, and radiation oncologists from the participating centers. We also thank the technologists from the Department of Nuclear Medicine (Centre Henri Becquerel) for their help in managing the patients. We are particularly thankful to Olivier Rastelli, Lucie Burel, Pierrick Gouel, Céline Breton, Dorianne Richard, and Dr. Louis-Ferdinand Pepin for their excellent collaboration.
Footnotes
Published online Mar. 2, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 8, 2016.
- Accepted for publication February 7, 2017.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prognostic Value of FDG PET Metabolic Parameters Before and After 42 Gy of Radiochemotherapy in Patients with Inoperable Stage III Nonsmall Cell Lung Cancer
- New developments in the imaging of lung cancer
- Prospective Evaluation of a Tumor Control Probability Model Based on Dynamic 18F-FMISO PET for Head and Neck Cancer Radiotherapy
- Oxygen-enhanced MRI Is Feasible, Repeatable, and Detects Radiotherapy-induced Change in Hypoxia in Xenograft Models and in Patients with Non-small Cell Lung Cancer
- Learning from Failure; Hypoxia Is an Evil Foe