


REPLY: We thank the authors for their interest in our recent paper (1) reporting the dynamic range of current 3-dimensional PET systems and the corresponding weight-based dose limits (MBq/kg) for accurate measurement of tracer activity and myocardial blood flow (MBF). They suggest that the proposed translation of phantom-measured to patient-recommended dosing may lead to counting rates (CRs) that exceed the recommended limits in some patients. We agree that the cardiac phantom scans are a simplified representation of patient imaging conditions, and that the phantom results should not be used alone without comparison to patient data confirming the weight-based dose limit that allows accurate quantification of MBF on a particular scanner, as shown in our paper. In this regard the authors are commended for comparing their patient-measured CRs with those obtained using the cardiac torso phantom. However, we note that their phantom-measured peak CR was obtained using a different method than we recommended, which is to determine the instantaneous total activity in the scanner field of view and the corresponding dead-time correction factor (DTF) (or prompt CR) at which quantitative accuracy is maintained with a less than 10% bias. The measured or simulated phantom CRs reported by van Dijk et al. after injection of their standard dose of 740 MBq do not appear to have any relation to the 10% bias criteria recommended in our paper. Their phantom data do appear to us to be fully consistent with the spread of patient values around the lines-of-best-fit, although prediction bounds were not included in their figures.
To further clarify, our original methodology determined the maximum DTF with a less than 10% bias in reconstructed activity (Fig. 1A). These values are closely related to the prompt coincidence CR (Figure 1B), which can also be used to establish and confirm the dynamic range for accurate quantification. Comparative data from our Discovery 690 demonstrate a measured activity bias of less than 10%–12% at a CR of less than 5,000–6,000 kcps and DTF of less than 1.5–1.6 for this particular scanner. As illustrated in Figure 1C, our peak patient CRs are in excellent agreement with the instantaneous phantom CR corresponding to an injected dose of 9–10 MBq/kg (and <10% activity bias). This dose used in our clinical practice is slightly lower than the 11.4 MBq/kg maximum value listed for the Discovery 690 scanner in the original paper and accounts for the population variability in peak DTF and CR observed due to differences in patient height, body habitus, or other non–weight-based factors as we reported initially. The distribution of CRs in our patient data is similar to that reported by the authors, with a large percentage of patients having higher peak CRs than observed in the phantom scan with equivalent injected dose. However, the authors should not assume that these higher CRs are associated with inaccurate measured activity values, because they did not report the CR (or DTF) limit required to maintain accuracy on their particular scanner. The lower peak CR observed in the 50-kg weight-equivalent phantom and in the smaller patients is a direct consequence of the recommended weight-based dosing. Although there is a clear trend to obtain higher CRs in larger patients, the correlation did not reach statistical significance because of limited sample size. This is in sharp contrast to the normalized CR per activity (kcps/MBq), which shows a significant negative correlation with patient weight (Fig. 1D) and is associated with higher CRs and DTF (and possible inaccuracy) in smaller patients when injected with a standard activity (e.g., 740 MBq), which is the current practice in many centers.
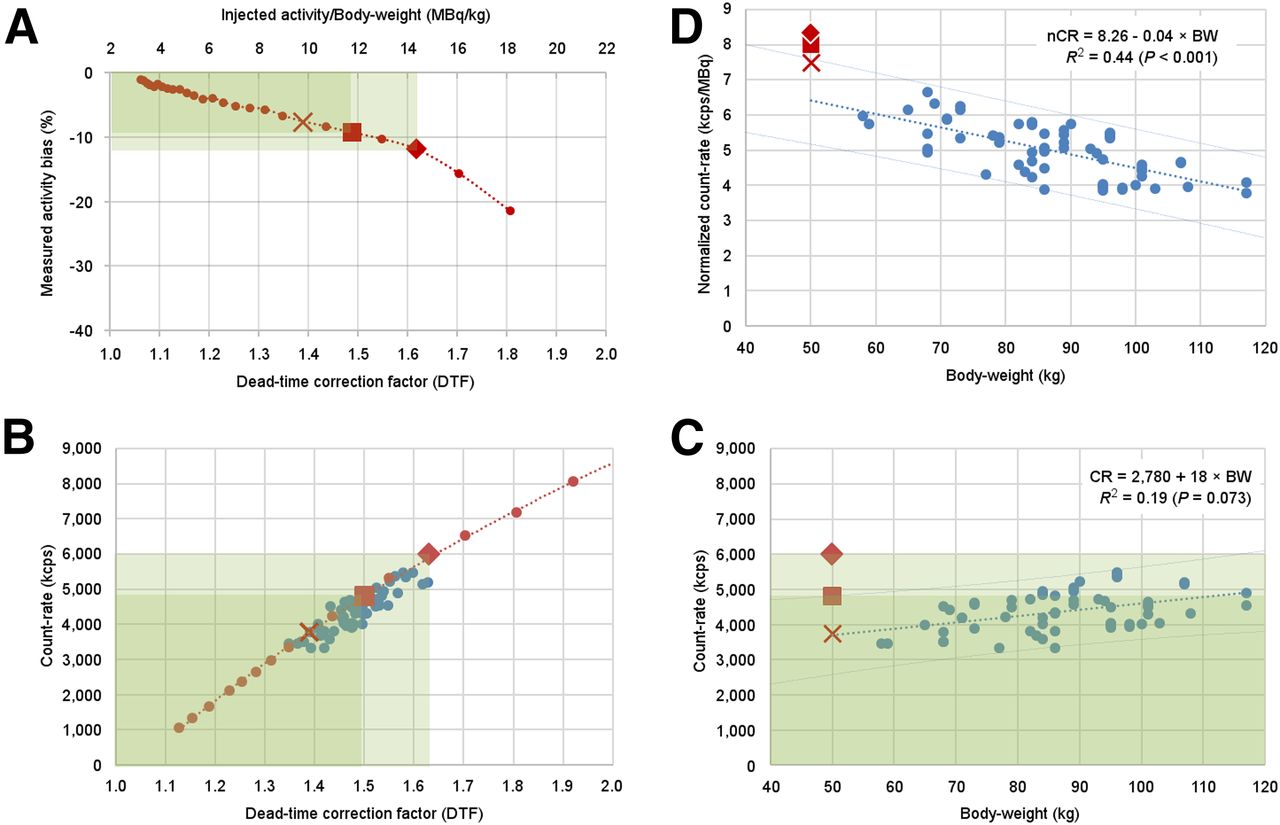
(A) Activity bias in decaying phantom study is < 10%–12% (square and diamond markers and green shaded areas) with DTFs < 1.5–1.6. (B) Prompt CRs are closely related to the DTF values in both phantom (red) and patient (blue) studies. (C) Fifty-kilogram weight-equivalent phantom study (red X) is consistent with peak measured patient CRs using 10 MBq/kg weight-based dosing. (D) Normalized CRs (nCRs) per MBq injected activity decrease with body weight (BW); therefore, smaller patients will have higher peak CRs and higher potential bias when using standard injected activity regardless of body weight.
The patient scan–revised versus phantom scan–predicted doses from the original paper are summarized in Table 1 with the limited available data for the Gemini/Ingenuity TF scanners. The phantom-predicted and patient-revised values were quite similar for the first 2 scanners listed, whereas the phantom-predicted dose was substantially underestimated compared with the patient-revised value in the third scanner. This highlights the need to validate the final weight-based dosing using patient scans acquired on any given scanner. If the phantom peak CR of 2,000 kcps reported by van Dijk et al. represents the accuracy limit on the Ingenuity TF scanner, then indeed their patient data would suggest that the clinical dose should be reduced below 4.6 MBq/kg. Their scanner appears to have very high CR capability (>9,500 kcps); we recommend that they determine the dynamic range of CRs and weight-based doses that will maintain quantitative accuracy in their patients’ scans.
Approximate Dead-Time and Prompt Coincidence CR Limits with <10% Activity Bias
Footnotes
Published online Jan. 26, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCE
- 1.↵





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.