


Abstract
Atherothrombotic events in coronary arteries are most often due to rupture of unstable plaque resulting in myocardial infarction. Radiolabeled molecular imaging tracers directed toward cellular targets that are unique to unstable plaque can serve as a powerful tool for identifying high-risk patients and for assessing the potential of new therapeutic approaches. Two commonly available radiopharmaceuticals—18F-FDG and 18F-NaF—have been used in clinical research for imaging coronary artery plaque, and ongoing clinical studies are testing whether there is an association between 18F-NaF uptake and future atherothrombotic events. Other, less available, tracers that target macrophages, endothelial cells, and apoptotic cells have also been tested in small groups of patients. Adoption of molecular imaging of coronary plaque into clinical practice will depend on overcoming major hurdles, ultimately including evidence that the detection of unstable plaque can change patient management and improve outcomes.
Cardiovascular disease is the number one cause of death in the United States, despite numerous advances in prevention, diagnosis, and treatment (1). Nearly half these deaths are due to acute myocardial infarction, and up to 75% of myocardial infarctions are the result of an acute thrombotic event after rupture of coronary artery plaque. Rupture-prone plaques often do not cause significant obstruction (2) and are not detectable by stress imaging, the approach most commonly used to assess risk. Identification of the rupture-prone, or vulnerable, plaque could add prognostic value and thus has become a major focus in cardiovascular diagnostics. Molecular imaging with radiopharmaceuticals has the potential to play a key role in the assessment of vulnerable plaque. In this review, we will describe advances in molecular imaging in the context of the pathophysiology associated with plaque growth and vulnerability.
TECHNICAL CHALLENGES IN PET IMAGING OF CORONARY PLAQUE
Imaging of coronary plaque with PET tracers is difficult because of the limited spatial resolution of PET, the small size of coronary plaque, and blurring caused by cardiac and respiratory motion. To partially mitigate motion of the coronary arteries, some investigators have performed end-diastolic imaging using only a part of the PET scan, but at the expense of increased image noise (3). We are exploring computational motion correction techniques that can potentially improve image quality, and we have demonstrated that these corrections can increase the target-to-background ratios of tracer uptake within coronary plaque and reduce image noise. The approach is likely to improve detection of small foci of tracer uptake within the coronary arteries (4).
THE BIOLOGY OF CORONARY PLAQUE
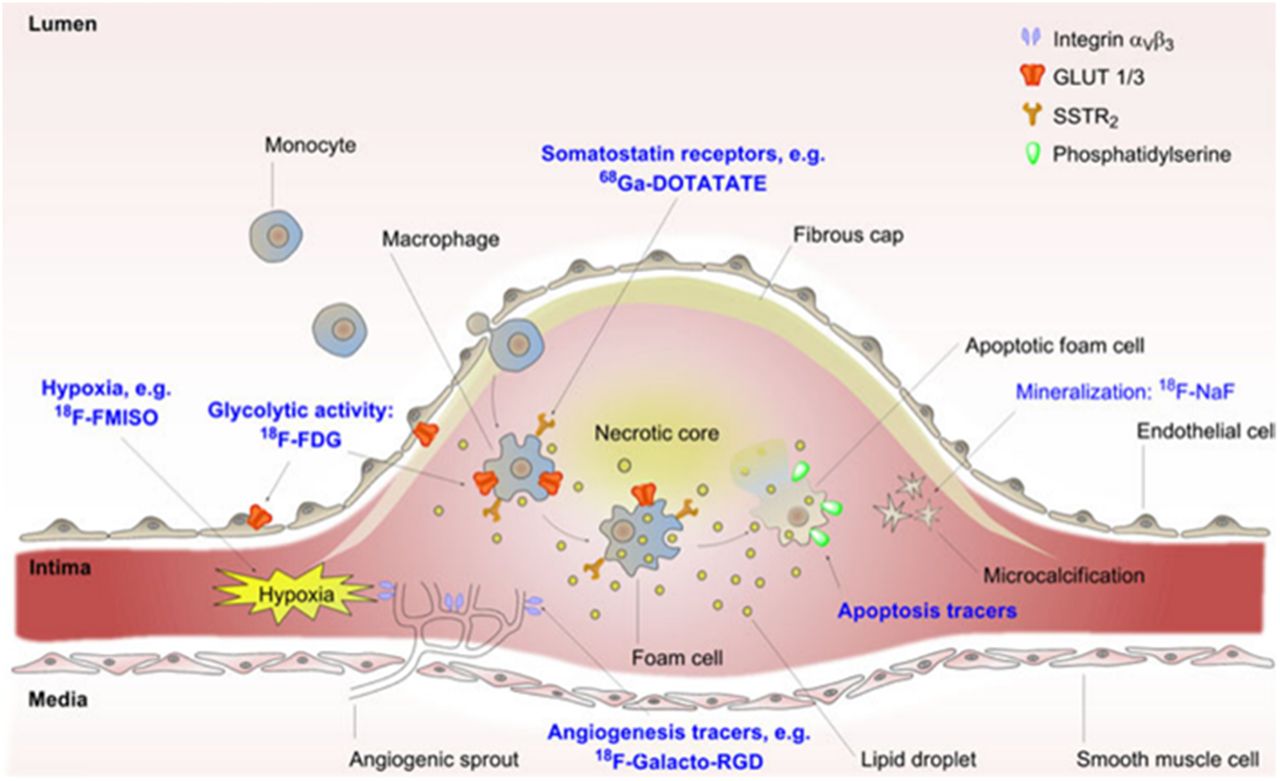
Atherosclerotic plaque develops in response to endothelial injury and entry of low-density-lipoprotein cholesterol into the intimal layer of the vessel wall. In response to this injury, monocytes are recruited into the vessel wall and differentiate into macrophages, which take up modified low-density lipoprotein (5). The inflammatory cascade initiated by the phagocytosis of oxidized low-density lipoprotein by macrophages stimulates angiogenesis and the formation of intraplaque neovessels, allowing the entry of red blood cells, leukocytes, lipids, and oxidized lipoproteins (Fig. 1) (6,7). Phagocytosis of red blood cells that enter the plaque by macrophages leads to the accumulation of iron, which promotes lipid peroxidation. This further stimulates the recruitment of new macrophages and expansion of the plaque. Macrophage apoptosis and the release of matrix metalloproteases (MMPs) destabilize the extracellular matrix. Histologic studies of ruptured plaque obtained from autopsy have described a milieu of inflammation characterized by macrophage infiltration, neovascularization, proteolytic remodeling of the extracellular matrix, apoptosis, and smooth muscle proliferation (6). Other processes that occur during plaque progression include calcium deposition by differentiation of mesenchymal cells into osteoclasts and osteoblasts. Microcalcification may occur as a repair mechanism in response to the intense necrotic inflammation and cell death found in plaque (8). These various biologic processes have served as potential targets for the development of molecular imaging agents labeled with radioisotopes or paramagnetic agents.
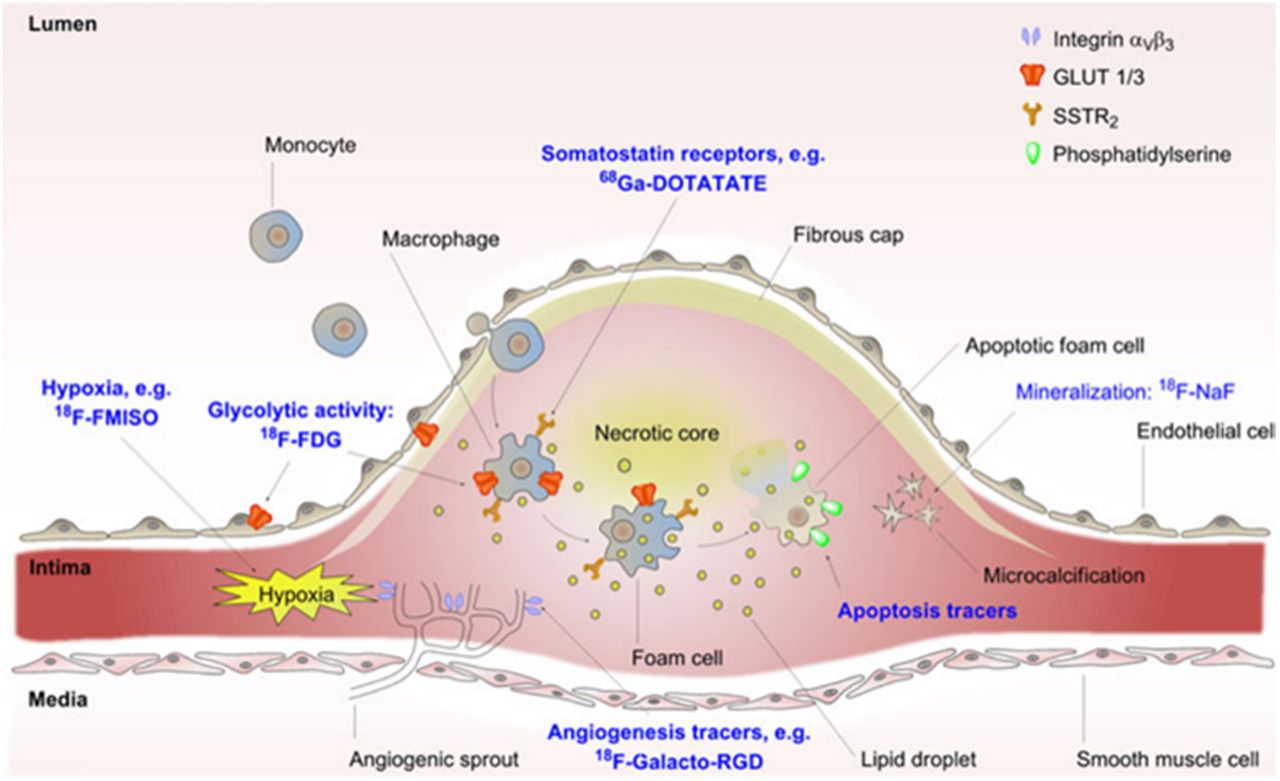
Schematic representation of key pathophysiologic characteristics of rupture-prone plaque and potential molecular imaging targets for its detection. FMISO = fluoromisonidazole; GLUT = glucose transporter. (Adapted with permission from Dr. Andreas Kjaer (7).)
18F-FDG: IMAGING INFLAMMATION WITH A UBIQUITOUS METABOLIC SUBSTRATE
The selective accumulation of 18F-FDG in metabolically active macrophages has been exploited for the detection of inflamed plaque in several clinical studies. The first description of the uptake of 18F-FDG in human atherosclerotic plaque and its proposed relationship to intraplaque macrophages was described in 2001 by Yun et al. (9). In the carotid arteries, increased 18F-FDG signal was shown to relate to high-risk anatomic imaging characteristics, including positive remodeling and low attenuation on coronary CT angiography (CTA) (10). Although 18F-FDG allows assessment of plaque in moderate-sized and large arteries, its use for monitoring plaque activity in the coronary vascular bed has been challenging. The feasibility of using 18F-FDG for coronary plaque imaging was initially described by Rogers et al. (11). We subsequently reported that 12 of 20 patients with recent acute coronary syndromes had increased 18F-FDG uptake in stented culprit coronary lesions—with a target-to-background ratio greater than 2.0—compared with 1 of 7 in patients with stable coronary artery disease (12). A limitation of coronary imaging with 18F-FDG is that its uptake by the myocardium frequently cannot be suppressed, despite a high-fat and low-carbohydrate diet (12). This high background 18F-FDG uptake makes interpretation of the signal originating from the coronary arteries problematic.
Not all macrophages within plaque are atherogenic. Proatherogenic M1 macrophages have been considered to promote destabilization of atherosclerotic plaque, whereas M2 macrophages are thought to be involved in repair of vulnerable plaque (13). However, M1 macrophages grown and differentiated in cell culture preferentially extract 3H-FDG compared with the M2 subtype, which has been shown to prefer deoxymannose as a metabolic substrate (14,15). Thus, the 18F-FDG extracted by plaque might depend on the relative abundance of M1 versus M2 macrophages within a plaque.
18F-NAF: USING MICROCALCIFICATION AS AN IMAGING TARGET
A potential target for molecular imaging of vulnerable plaque is vascular osteoblastic calcification, long considered a hallmark of atherosclerosis. Atherosclerosis has been shown to be associated with phenotypic conversion of vascular myofibroblasts into osteoblastic cells and to promote calcification (16). Calcification on a distensible surface (vascular endothelium) can induce a compliance mismatch, making it more prone to rupture at the tissue–calcium interface (17).
Because the fluoride ion in NaF exchanges with hydroxyl ions in hydroxyapatite crystals, osteoblastic calcification in atherosclerotic plaque can be detected with 18F-NaF, a radiopharmaceutical that has been used for bone scanning for over 40 y (18). In a prospective study of 40 patients with myocardial infarction and 40 with stable angina, Joshi et al. showed that 18F-NaF successfully identified vulnerable coronary lesions in 93% of the lesions implicated in causing the infarction (3). Increased uptake was also observed in 45% of the patients with stable coronary artery disease being referred for invasive coronary angiography. In these patients and in 40 patients with stable angina, regions of 18F-NaF uptake correlated with intravascular ultrasound findings of microcalcification, a necrotic core, and positive remodeling. 18F-NaF does not require any labeling and is readily produced by any cyclotron radiopharmacy facility. Because the myocardium does not extract 18F-NaF, 18F-NaF uptake can easily be detected in coronary plaque without being confounded by the uptake in the underlying myocardium that occurs with 18F-FDG. These practical considerations would simplify the application of 18F-NaF in the clinical work-up of patients.
To date, the use of 18F-NaF has been studied only in patients who have already had a coronary event or who are already being referred for invasive coronary angiography. A clinical use of 18F-NaF could be for further risk stratification of patients with stable disease before this adverse event occurs. Such application might allow us to further characterize risk in patients with vulnerable plaque characteristics detected by coronary CTA. From our work, an example of 18F-NaF uptake in the left main coronary artery of an unstable-angina patient showing vulnerable plaque characteristics on coronary CTA is presented in Figure 2.

An 85-y-old man with non-ST elevation myocardial infarction. (A and B) Coregistered motion-corrected 18F-NaF PET/CT and coronary CTA images show intense uptake (arrows) in recently ruptured plaque in left main and proximal left anterior descending arteries. (C and D) Coronary CTA images alone show the underlying atherosclerosis (arrows). (E) Invasive angiography shows severe stenosis (arrow) in mid to distal portion of left main coronary artery (Courtesy of Cedars-Sinai Medical Center).
αVβ3 INTEGRIN LIGANDS: IMAGING ANGIOGENESIS
Intraplaque neovascularization has been considered a hallmark of plaque vulnerability, and integrin-targeted imaging agents have been evaluated extensively for the detection of plaque neovascularization. The αvβ3 integrin is expressed on macrophages, migrating smooth muscle cells, and endothelial cells in the vasa vasorum and intraplaque microvasculature of coronary arteries (19). The tripeptide arginine–glycine–aspartic acid (RGD) has a high affinity for integrin αvβ3 and is often used as the primary binding motif in integrin-targeting imaging agents. 18F-galacto-RGD has been shown to preferentially bind to ruptured atherosclerotic plaque in the carotid artery of patients within a few weeks after experiencing a stroke (20). A major disadvantage of 18F-galacto-RGD is the long labeling time. 18F-flotegatide is physiologically similar to 18F-galacto-RGD and is easily labeled through click chemistry, which is faster and thus more practical for clinical applications (21). In a preclinical study, focal uptake of 18F-flotegatide by aortic plaque has been demonstrated in an apoE-deficient mouse model of atherosclerosis (21). In a preliminary proof-of-concept clinical study, we have observed selective extraction of 18F-flotegatide by plaque in patients with carotid artery disease (Fig. 3). Further investigation will be necessary to determine the clinical utility of 18F-flotegatide for imaging plaque vulnerability.
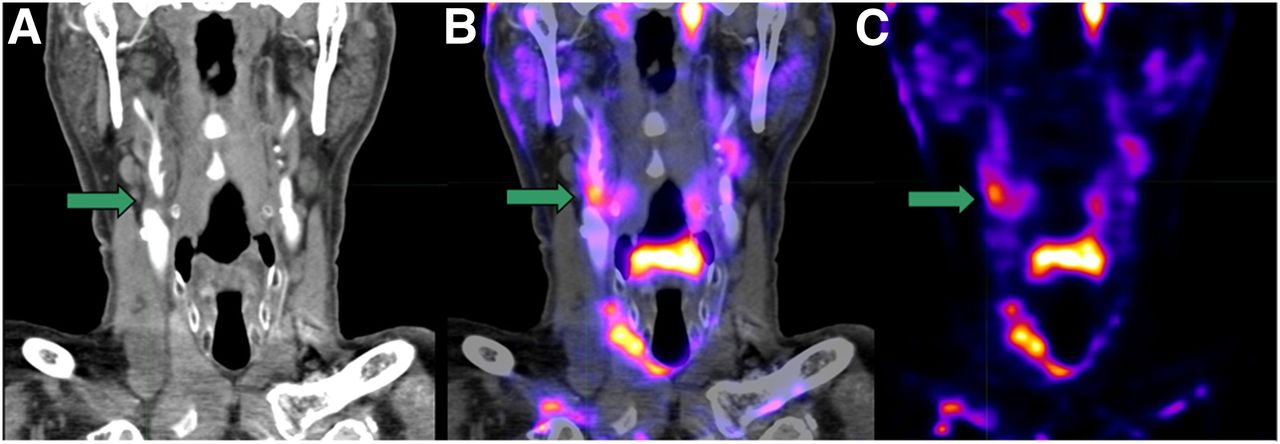
A 64-y-old man with transient ischemic attack suspected to result from microemboli from an occlusive carotid plaque. (A) CTA image shows loss of contrast opacification (arrow) at site of large atherosclerotic plaque in bifurcation of right common carotid and right internal carotid arteries. (B) Coregistered CTA and PET/CT image obtained with 370 MBq of 18F-flotegatide, a cyclic tripeptide that binds integrin on neovascular endothelial cells and macrophages, shows uptake by carotid plaque implicated in causing transient ischemic attack (arrow). (C) PET/CT image shows 18F-flotegatide uptake (arrow) by carotid plaque.
ADDITIONAL MACROPHAGE-TARGETED IMAGING AGENTS
Several other potential plaque-imaging agents, many of which are still in preliminary preclinical and clinical studies, have been described.
68Ga- and 64Cu-Labeled DOTATATE
Somatostatin receptor 2, commonly expressed in neuroendocrine tumors, has also been found on macrophages (22). Coronary artery uptake of a somatostatin receptor 2 ligand, DOTATATE, labeled with 68Ga has been observed in patients with neuroendocrine tumors who underwent imaging with 68Ga-DOTATATE (23). In a smaller study of 10 patients who underwent carotid endarterectomy, 64Cu-DOTATATE was used for PET/MRI of carotid artery plaque, and uptake of 64Cu-DOTATATE correlated independently with gene expression of CD163, a surrogate marker of activated macrophages (24). It is likely that this uptake is occurring in macrophages in the atherosclerotic plaque.
11C-PK11195
Translocator protein is an 18-kDa protein that is expressed in the outer mitochondrial membrane of most cells. The activation of macrophages in inflammatory states is associated with increased expression of translocator protein. 11C-PK11195, a ligand that selectively binds to translocator protein, has been shown to bind to atherosclerotic plaque ex vivo, and increased carotid uptake of 11C-PK11195 has been observed in patients with symptomatic carotid stenosis (25).
Vascular Cell Adhesion Molecule 1
Vascular cell adhesion molecule 1 (VCAM1) plays an important role in the initial steps of monocyte recruitment to atherosclerotic lesions, and targeted imaging of VCAM1 with 18F-labeled anti-VCAM1 antibody has been used in preclinical studies to visualize atherosclerotic plaque (26). The high specificity of this tracer for binding with VCAM1 makes it an attractive molecular imaging agent for identification of inflamed atherosclerotic plaque.
11C- and 18F-Labeled Choline
Choline, a precursor of lipids crucial for the synthesis of cell membranes, is transported into rapidly proliferating cells, including macrophages and radiolabeled choline, and has been used for macrophage imaging. 18F-fluorocholine and 11C-choline have been shown to detect inflammatory changes in the aorta and carotid arteries (27,28). The ongoing Plaque at RISK Study is assessing the clinical use of this tracer for detecting vulnerable plaque in patients with carotid atherosclerosis (29). However, high endogenous uptake of choline by the myocardium may limit the translation of this tracer to use for clinical coronary plaque imaging.
18F-Fluorothymidine
18F-fluorothymidine is a PET tracer that is extracted by rapidly proliferating cells, including macrophages, for DNA replication. Vascular uptake of 18F-fluorothymidine has been demonstrated in both an ApoE knockout mouse model of atherosclerosis and a small cohort of patients with risk factors for atherosclerosis (30).
MATRIX REMODELING BY MMP
Loss of collagen and other extracellular matrix components in highly inflamed regions of plaque can reduce tensile strength and increase the risk of rupture. MMPs are believed to play a major role in matrix remodeling because they can degrade components of the extracellular matrix at neutral pH. Increased levels of MMP-1, MMP-3, MMP-8, and MMP-9 have been found in atherosclerotic plaque containing a predominance of vascular smooth muscle cells and macrophages (31). MMPs have therefore been considered ideal targets for molecular imaging of vulnerable plaque. In preclinical models of atherosclerosis, 123I- or 125I-labeled CGS 27023A, a broad-spectrum MMP inhibitor (32), and RP-805, a 99mTc-labeled broad-spectrum MMP-inhibiting macrocyclic compound, have been shown to bind to atherosclerotic plaque (33,34).
HYPOXIA
Hypoxia has been considered a characteristic of vulnerable plaque due to poor perfusion within the large necrotic core. Tracers for hypoxia have been evaluated for detection of rupture-prone plaque in preclinical and clinical studies. Selective uptake of 18F-fluoromisonadazole by plaque has been demonstrated in a rabbit model of atherosclerosis (35). In clinical subjects, 18F-flortanidazole uptake by carotid plaque has been observed in patients who experienced a transient ischemic attack due to plaque rupture (36).
APOPTOSIS
The presence of a large necrotic core is an important feature of vulnerable plaque with associated high levels of apoptosis. During apoptosis, phosphatidylserine, a phospholipid found in the intracellular aspect of cell membranes in viable cells, becomes exteriorized and thus available to high-affinity ligands such as annexin V (37). 99mTc-labeled annexin A5 has been used to detect apoptosis in vivo in a rabbit model of atherosclerosis (37). 99mTc-annexin-A5 uptake by carotid plaque was also demonstrated in a pilot study of patients with a recent history of stroke or transient ischemic attack. Annexin A5 binding was found to correlate with apoptotic activity measured with histochemical techniques in plaque obtained during endarterectomy (38).
CHALLENGES TO THE CLINICAL USE OF VULNERABLE PLAQUE IMAGING
Many hurdles remain on the path to using imaging tracers for clinical assessment of plaque at high risk for causing an acute coronary event. First, this review has focused on rupture-prone, vulnerable plaque; however, it is known that a substantial proportion of atherothrombotic events occur in areas of plaque erosion without rupture. The process of plaque erosion as the stimulus for thrombosis raises major problems in the practical application of molecular imaging for detection of high-risk plaque. Eroded plaque is smaller than rupture-prone plaque and therefore tracer accumulation may be reduced in eroded plaque. Further, there may be less inflammation associated with eroded plaque. Autopsy studies have suggested differences between women and men in the morphology of the underlying plaque associated with acute myocardial infarction (39). Coronary thrombosis arising from eroded plaque has been reported to be relatively frequent in women (40). As opposed to plaque that undergoes rupture, erosion-prone plaque is characterized by a thin fibrous cap, a relatively smaller lipid pool, and fewer inflammatory cells. Hence, molecular imaging approaches that are primarily directed toward detecting the histopathologic processes of plaque rupture may miss the less predominant but significant group of patients with erosion-prone plaque.
Second, it is not yet clear which of the tracers has the greatest chance for ultimate clinical application. Although several radiolabeled tracers have proven useful for identifying atherosclerotic plaque in preclinical models of disease, most clinical studies on the imaging of coronary plaque have been performed with 18F-FDG and 18F-NaF. This is related to the ease of synthesis of these imaging agents, their ready availability, and their historical use for other clinical applications. As mentioned previously, the inability to optimally suppress glucose uptake by the myocardium can interfere with visualization of 18F-FDG uptake by coronary plaque. Currently, 18F-NaF is considered to be the most promising easily available tracer for coronary plaque imaging in clinical subjects. Ligands for receptors selectively expressed by macrophages and luminal endothelial cells, as well as radiolabeled tracers for detecting hypoxia, angiogenesis, and apoptosis, have been used to detect active atherosclerotic plaque in only small clinical cohorts. Translation of these tracers to plaque imaging in clinical subjects will depend on their safety, affordability, and ease of synthesis. In most clinical molecular imaging studies, preferential binding of the tracer to unstable plaque is confirmed by demonstrating increased tracer uptake in plaque after the atherothrombotic event has occurred. To demonstrate that a molecular imaging tracer can identify unstable plaque in a clinically useful manner, it will be necessary to show that increased tracer uptake by coronary artery plaque is associated with a future cardiac event.
Third, to make molecular imaging clinically feasible, major technical advances in image acquisition and processing are required to overcome the limitations imposed by cardiac and respiratory motion of the coronary arteries and the small size of coronary plaque.
OUTLOOK
From an investigational standpoint, the emergence of PET/MRI will enable simultaneous characterization of the morphologic and biologic features of vulnerable plaque, with the combined methods providing greater potential for tissue characterization. Undoubtedly, further exploration of various approaches to using these agents with either PET/CT or PET/MRI in preclinical research will be important in clarifying the mechanisms of plaque progression and rupture and in developing and assessing novel therapeutic approaches. For vulnerable coronary plaque imaging to become a clinical tool, large-scale trials will be required to demonstrate the incremental value of plaque imaging in risk assessment and, ultimately, the ability of molecular imaging to affect clinical outcomes.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Feb. 9, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 12, 2016.
- Accepted for publication January 25, 2017.





{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- TECHNICAL CHALLENGES IN PET IMAGING OF CORONARY PLAQUE
- THE BIOLOGY OF CORONARY PLAQUE
- 18F-FDG: IMAGING INFLAMMATION WITH A UBIQUITOUS METABOLIC SUBSTRATE
- 18F-NAF: USING MICROCALCIFICATION AS AN IMAGING TARGET
- αVβ3 INTEGRIN LIGANDS: IMAGING ANGIOGENESIS
- ADDITIONAL MACROPHAGE-TARGETED IMAGING AGENTS
- MATRIX REMODELING BY MMP
- HYPOXIA
- APOPTOSIS
- CHALLENGES TO THE CLINICAL USE OF VULNERABLE PLAQUE IMAGING
- OUTLOOK
- DISCLOSURE
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.