


Abstract
The identification of new molecular targets for diagnostic and therapeutic applications using in vitro methods is an important challenge in nuclear medicine. One such method is immunohistochemistry, increasingly popular because it is easy to perform. This review presents the case for conducting receptor immunohistochemistry to evaluate potential molecular targets in human tumor tissue sections. The focus is on the immunohistochemistry of G-protein–coupled receptors, one of the largest families of cell surface proteins, representing a major class of drug targets and thus playing an important role in nuclear medicine. This review identifies common pitfalls and challenges and provides guidelines on performing such immunohistochemical studies. An appropriate validation of the target is a prerequisite for developing robust and informative new molecular probes.
The discovery of novel molecular tumor targets is of key importance in nuclear medicine. For successful tumor imaging and targeted tumor radiotherapy in patients, nuclear medicine needs to rely on adequate identification of specific tumor targets with in vitro methods in large series of human tumor samples. One such specific tumor target is a receptor to which only the natural ligand or specifically designed molecules will be able to bind with high affinity. In addition, to be a specific tumor target, a receptor preferably must be sufficiently expressed only in tumor cells, not in other tissues, organs, or compartments. In the literature, there are numerous such examples of receptors massively overexpressed in tumors but not in normal physiologic tissues. Clearly, nuclear medicine is dependent on target specificity if it wants to fulfill its role of accurately diagnosing tumors and safely treating tumors with as few side effects as possible.
The G-protein–coupled receptors (GPCRs), one of the largest families of cell surface proteins, represent one such ideal target for nuclear medicine. Not only do they regulate, after activation by hormones and neurotransmitters, a considerable part of the physiologic processes in the body, but they also represent a major class of drug targets and thus play an increasingly important role in medicine. Indeed, more than 30% of the clinically marketed drugs do act through GPCRs and are therapeutically successful in a large spectrum of human diseases. It is therefore evident that reliable information on the expression and precise distribution of GPCRs, particularly in normal and diseased human tissues, is highly desirable. The cellular density of GPCRs is usually considerably lower than that of other cellular parameters—such as hormones, for instance—sometimes challenging their detection with current in vitro methods. The present article focuses on GPCRs, even though other classes of targets (enzymes, kinases, transporters, steroid hormones, and growth factor receptors) would also have been subjects of interest.
VALIDATION
It is of prime importance that GPCRs be evaluated in vitro first, in a large series of human tumor samples, so that clear information on their incidence and density can be given for these tissues. GPCRs can be detected in vitro in human tissues by various methods. Human tissue samples are not homogeneous but extremely complex, as they usually include many distinct cell types and compartments (epithelial cells, endocrine cells, nerves, vessels, and immune cells, among others) as well as pathologic tissues (e.g., tumors, inflammatory tissues, and degenerative tissues). Therefore, it is mandatory to use morphologic methods to accurately identify the cell types that do express GPCRs. Various morphologic methods exist to measure and localize these receptors, including receptor messenger RNA detection with in situ hybridization; receptor protein localization with in vitro radioligand binding using receptor autoradiography, a method based on the same principle as in vivo imaging in patients, namely the binding to tumor tissue of a radiolabeled analog showing specificity and high affinity to the investigated receptor; and immunohistochemistry with specific antibodies, the subject of the present commentary.
Immunohistochemistry has become popular because it is an easy-to-perform morphologic method. It has an excellent resolution at the cellular level; it can be performed on readily available formalin-fixed tissues rather than on the more difficult-to-obtain fresh-frozen material; it has a rapidly increasing number of available commercial and noncommercial antibodies; and its data are generally considered easy to interpret (see below for caveats, however). The consequence is a plethora of papers describing immunohistochemistry findings for GPCRs in human tissues. Unfortunately, several of the published papers show that data are often questionable because of the use of poorly validated antibodies or protocols (1,2). Several papers have therefore recently documented the need for relevant, well-designed immunohistochemical protocols and correctly characterized antibodies (3–6). The authors of these papers also suggest that, to prevent poorly relevant publications on GPCR immunohistochemistry and subsequent further controversial discussions, the scientists publishing immunohistochemistry studies should follow recommendations or even clear rules (3,4,7). An initiative to introduce such recommendations has recently been taken by the journal Endocrinology (8); adherence to such a strategy by all journals reporting immunohistochemical data would be beneficial. Valuable in this regard is also a set of recommendations on the validation of immunohistochemical assays in diagnostic settings, recently published by the College of American Pathologists (9). Because nuclear medicine is basically dependent on the precise definition and identification of receptor targets in vitro, basic scientists in the nuclear medicine field should be aware of this initiative.
IMMUNOHISTOCHEMISTRY REQUIREMENTS
What is necessary to make an immunohistochemistry investigation convincing? At first, rather basic information is needed, namely a full description of the antibody characteristics (antibody name, manufacturer, code number, antigen sequence if known, species raised in, monoclonal/polyclonal designation, clone designation if applicable, lot number for polyclonal antibodies). It should further be confirmed that the antibody has been tested successfully in cell lines expressing the receptor, and negative controls in cell lines devoid of the receptor or in wild-type/knock-out mice should also be provided (3,4,10,11). Preferably, such data should be available for both fresh frozen and the corresponding formalin-fixed materials.
TESTING IN HUMAN TISSUES
Validation of a GPCR antibody in cell lines does not necessarily warrant its specificity in human tissues. The antibody needs to be further tested in human tissues.
Control Tissues
One should take care to identify and use adequate control tissues—as far as they are known—to validate the chosen antibody; that is, choose positive controls containing a known, established human target tissue expressing the receptor of interest. Adjacent nontarget tissue should clearly not react, that is, should “stain negatively.” Antigen preabsorption tests, or negative controls, performed with an excess of antigenic peptide (if available) on adjacent sections of the same tissue samples should also be provided. Various antigen retrieval methods and different antibody concentrations should be applied in initial testing. Also, frozen tissues may be tested. In many instances, immunohistochemistry works on frozen tissues; this is important because some targets do not survive formalin fixation and need to be analyzed on frozen tissues. All results should be carefully evaluated to obtain an optimal protocol. Once the protocol is established, any further tests should strictly adhere to it. Precaution should be taken when pancreatic islets are used as positive controls for validation of hormone receptors—as commercial providers often do—because the islets have been shown to be occasionally “immunostained” nonspecifically (12).
Localization Within Cells
For GPCRs, it is not sufficient to simply show the presence of the immunoreactive product in the cell; it is essential to document where in the cell the immunohistochemical reaction product is localized. By definition, GPCRs are cell surface receptors with 7 transmembrane-spanning domains. Therefore, under normal conditions, we expect to see immunoreactivity localized at the cell membrane (10,11,13–15). A typical example of the somatostatin receptor sst2 expressed in a neuroendocrine tumor is shown in Figure 1A. This membrane-bound localization of such a GPCR is at odds with the cellular location for other receptor families, such as the androgen receptors (16), located by definition in the cytoplasm or nucleus. For GPCRs, diffuse cytoplasmic immunohistochemical staining is a doubtful result and most likely nonspecific but is often erroneously interpreted as specific staining demonstrating internalized receptors. Surely, GPCRs can be actively internalized from the cell membrane into the cell. Internalization is even part of the physiologic mechanism of action for many GPCRs. A condition usually necessary for this phenomenon to occur is an acute receptor stimulation by agonist treatment that triggers internalization of the receptor–ligand complex. Internalized receptors have a particular intracellular distribution, as they are usually internalized in circumscribed endosomes; thus, they are not diffusely distributed in the cytoplasm (17,18). Figure 1B shows an example of internalized sst2 receptors in a neuroendocrine tumor from a patient who received an infusion of the somatostatin analog octreotide during surgical removal of his tumor. As is evident in both examples of Figure 1, an illustration at high magnification is required to precisely evaluate the cellular localization of receptors. Often, authors do not take advantage of the high resolution of immunohistochemistry but limit themselves to publishing overview pictures of low magnification that sometimes mask poor-quality immunostaining.
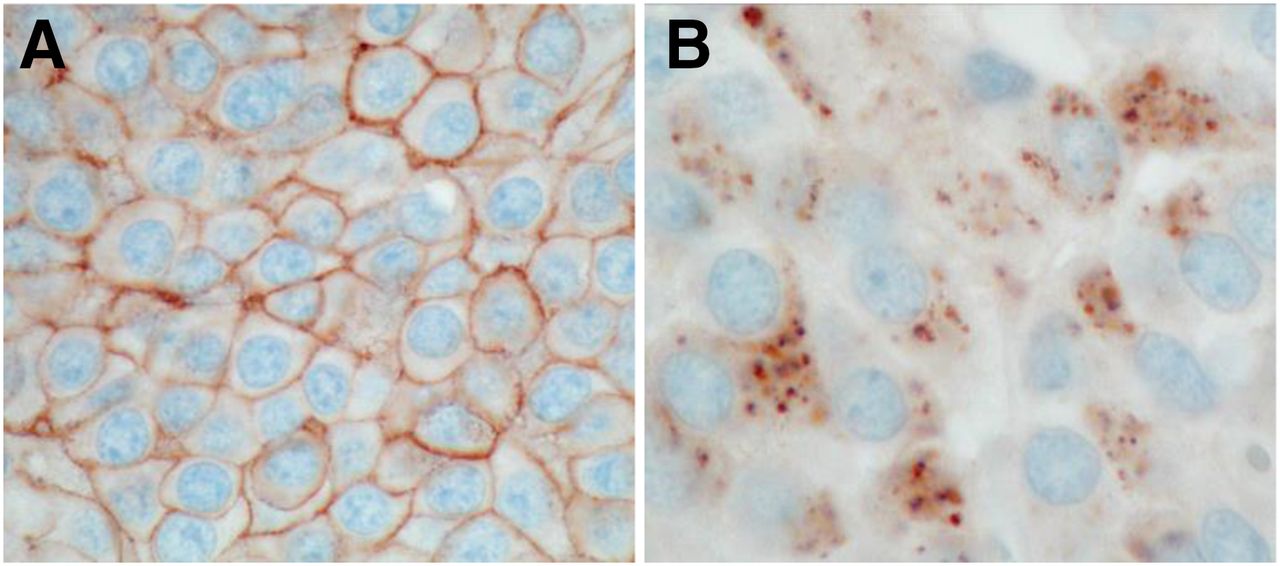
(A) Immunohistochemistry of sst2 in neuroendocrine tumor taken from octreotide-naïve patient. Strong membrane-bound somatostatin sst2 receptor staining is seen in tumor cells. (B) Immunohistochemistry of somatostatin sst2 receptor in neuroendocrine tumor from patient who received intravenous infusion of octreotide during resection of tumor. Because of octreotide application, receptors are not membrane-bound but have been internalized after octreotide binding and show typical endosome-related intracellular pattern.
Western Blot Testing
One should provide a Western blot with the used antibody in the same human tissues that were found to be immunohistochemically positive. Such a blot should confirm the identity of the receptor detected by immunohistochemistry by showing a single, specific band of the expected molecular weight (13,15,17).
Comparison with Other Receptor-Measuring Methods
One should compare the immunohistochemistry-based data with data obtained using another morphologic receptor-measuring method (in vitro receptor autoradiography, in situ hybridization) on the same samples. Although of fundamental importance, such a specificity test of course involves considerable additional work (13,15,19) and is therefore often omitted. It is, however, important to confirm the immunohistochemistry results against alternative methods such as receptor binding since the epitope identified by immunohistochemistry does not necessarily correspond to the binding site of the radioligand. In vitro receptor autoradiography is particularly suitable to analyze targets for nuclear medicine, as it is based on the high-affinity binding of a radiolabeled compound to the receptor and therefore represents the in vitro method corresponding to the in vivo imaging.
Comparison with Other Antibodies
Ideally, one should compare the obtained GPCR immunohistochemical data with the immuno-localization of the same GPCR using another antibody recognizing a different epitope of the receptor, when such a well-validated antibody is available (19).
Optimal Formalin Fixation
For every immunohistochemistry study, an optimal formalin fixation of the human tissue samples, according to the standard rules of surgical pathology, is mandatory (9).
In consideration of the enormous number of future drug targets and disease biomarkers (20–22), it is particularly relevant to use adequate in vitro methods to define the tumor target. Putting most of the above-mentioned recommendations into practice will likely prevent unnecessary controversies and reduce experimental discrepancies, as recently shown by examples in the field of receptors for somatostatin, chemokines, and glucagonlike peptide 1 (3,4,10,11,23,24).
CONCLUSION
Implementation of the tests described in this article would not only considerably add to the quality of published immunohistochemistry papers but also help in reproducing important new data and permitting more straightforward scientific progress. In particular, accurate in vitro target definition is crucial for clinical nuclear medicine, by reducing the number of unnecessary clinical trials on poorly defined targets.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 14, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 14, 2017.
- Accepted for publication August 10, 2017.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.