


Abstract
Current standard values of fetal dosimetry deriving from 18F-FDG injection in pregnant women are estimated from animal data. The present communication offers a revision of fetal dosimetry values calculated from recently published human data, in which fetal 18F-FDG uptake was directly observed in vivo. The final doses were obtained from the observed time-integrated activity coefficients and a new generation of anthropomorphic voxel-based pregnancy phantoms.
Fetal radiation dose estimates for administration of 18F-FDG were originally proposed in 1997 by Russell et al. (1), but with no information about possible placental crossover. In 2004, Stabin (2) amended the dose estimates to include placental crossover data observed in primates (3). Recently, Zanotti-Fregonara et al. (4) have quantified fetal uptake in 19 fetuses from 5 to 34 wk of pregnancy. Four women were in the early weeks of pregnancy, and the dose to the uterus was used as a proxy for the fetal dose. Starting from 10 wk, however, the fetus was more clearly visible inside the uterus, and therefore the 18F-FDG uptake in fetal tissues could be calculated directly in 15 cases.
By extrapolating with mathematic modeling from the data of Zanotti-Fregonara et al. (4) and by using the realistic voxel-based phantoms of Shi et al. (5), this brief communication recommends the best standardized values for estimating the dose to the fetus at any stage of pregnancy.
MATERIALS AND METHODS
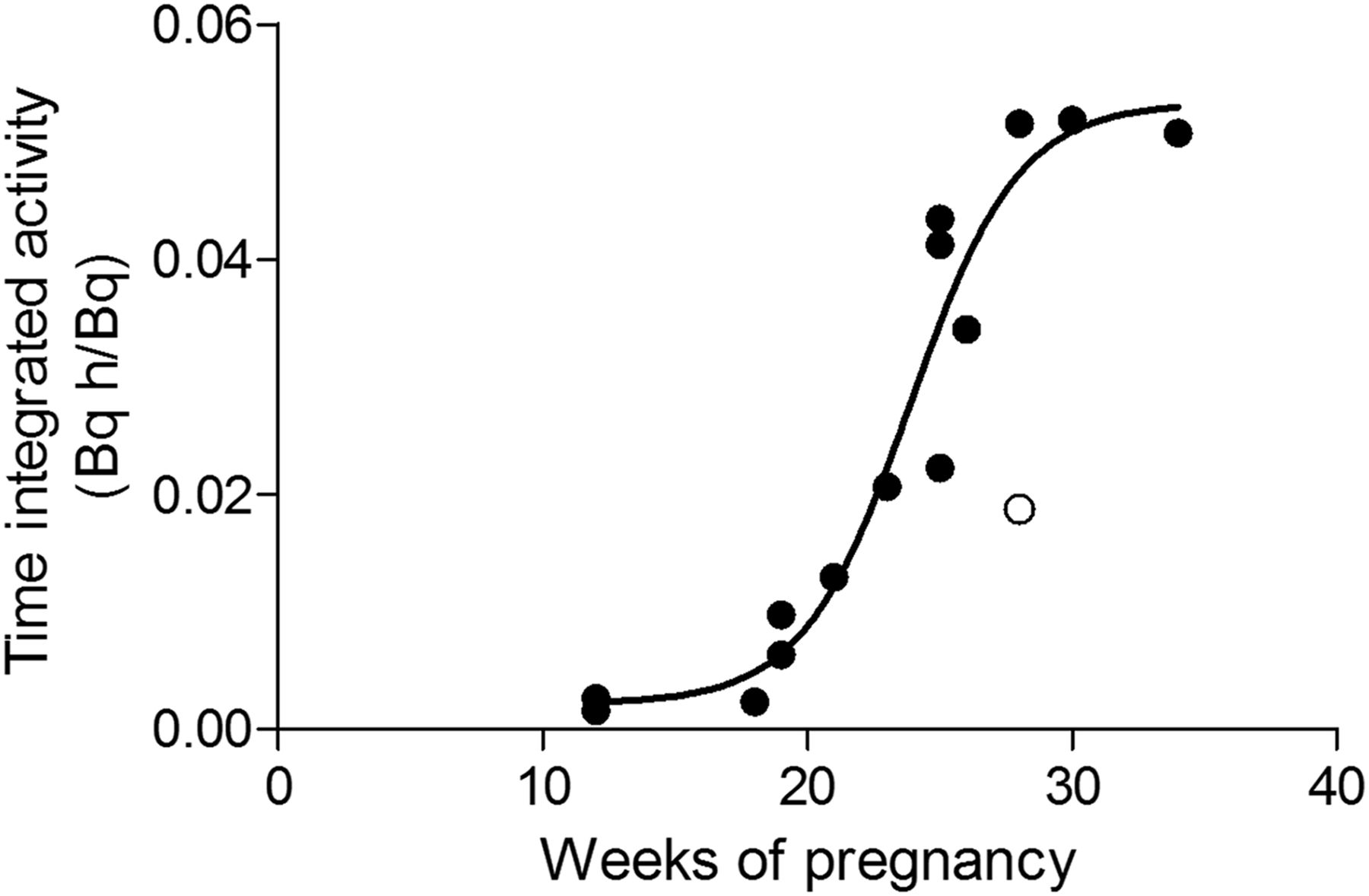
The fetal time-integrated activity coefficients of the 15 cases reported by Zanotti-Fregonara et al. (4) were fitted with the following logistic function: The function is characterized by these parameters: a (bottom value) = 0.00216 Bq h/Bq; b (slope factor) = 0.2128 wk−1; c (inflection point) = 23.9 wk; and d (top value) = 0.05328 Bq h/Bq. The fitting was performed after automatic elimination of one outlier (ROUT [robust regression and outlier removal] Q coefficient, 1.0%) (Fig. 1).
The function is characterized by these parameters: a (bottom value) = 0.00216 Bq h/Bq; b (slope factor) = 0.2128 wk−1; c (inflection point) = 23.9 wk; and d (top value) = 0.05328 Bq h/Bq. The fitting was performed after automatic elimination of one outlier (ROUT [robust regression and outlier removal] Q coefficient, 1.0%) (Fig. 1).
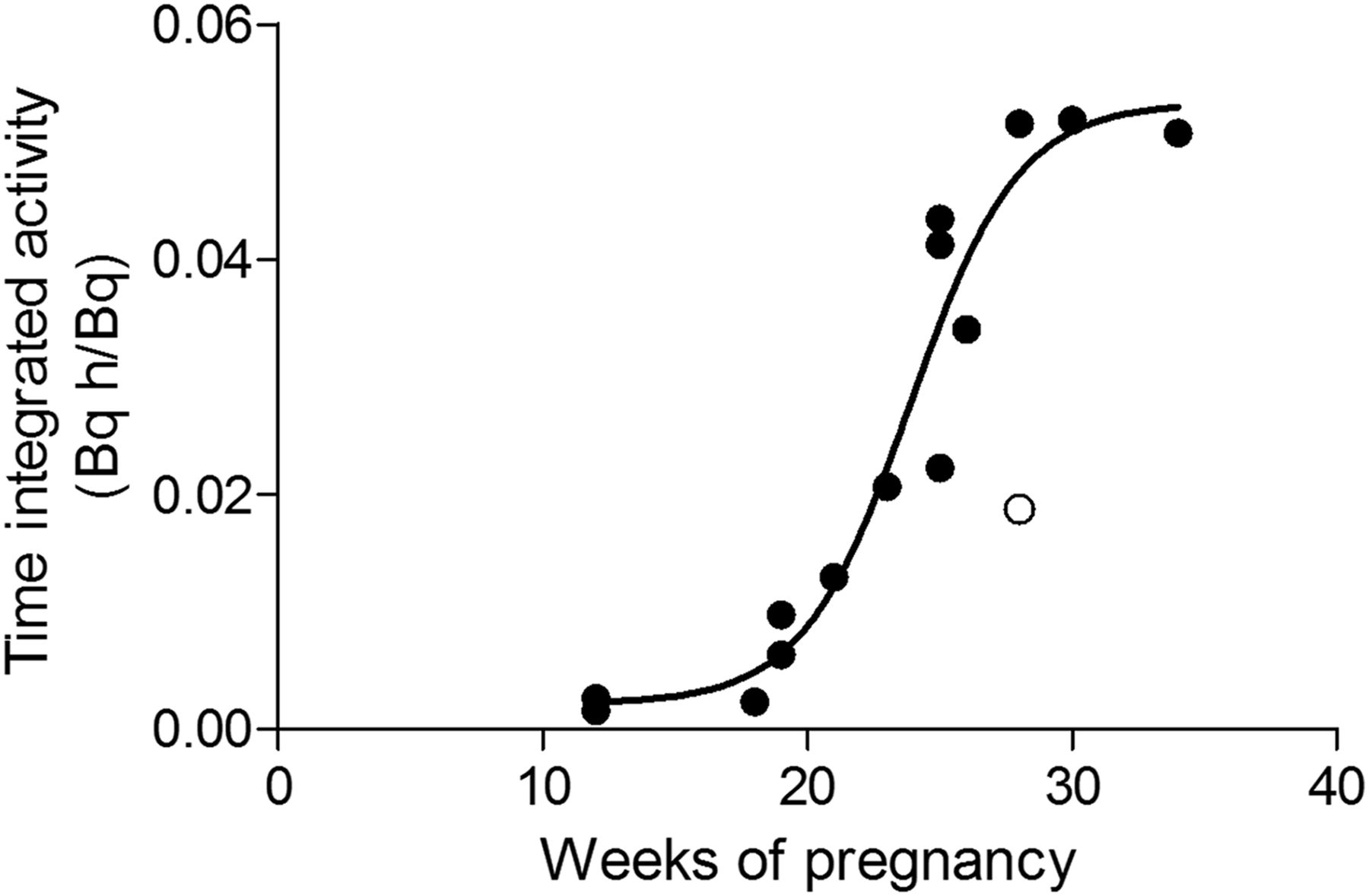
Sigmoid fitting through observed time-integrated activity data points reported by Zanotti-Fregonara et al. (4). Automatic detection of outliers removed one point (in white).
The logistic function was chosen because it fitted the data points better than either a monoexponential or a quadratic function, in terms of Akaike score. Moreover, a runs test for randomness was not significant for the logistic fitting (P = 0.79) but was significant for the exponential (P = 0.007) and the quadratic curve (P = 0.025). Time–activity integrals for activity in the mother’s organs were taken from publication 128 of the International Commission on Radiological Protection (Table 1) (6).
Time-Integrated Activity Coefficients (6)
The final doses were calculated using the realistic voxel-based phantoms of Shi et al. (5), which are implemented in the forthcoming new version of OLINDA/EXM. The activity coefficient at 5 wk was assigned to the uterus of the nongravid female phantom. The coefficients at 13, 26, and 39 wk were assigned to the fetus of the first-, second-, and third-trimester pregnant phantom, respectively.
RESULTS
The interpolated time-integrated activity coefficients at different stages of gestation, as predicted by the logistic fitting, are reported in Table 2. The resulting dose estimates, calculated with OLINDA/EXM 2.0, are reported in Table 3. For comparison, Table 3 also reports the values previously suggested by Russell et al. (1) and Stabin (2), as well as the present dose estimates calculated with Cristy and Eckerman’s stylized phantoms (7), included in the first version of OLINDA/EXM (8). Differences between the values estimated with the two versions of the OLINDA/EXM software are mainly due to the assumed fetal masses. This is especially true for the 3-mo fetus, whose mass is 460 g in the OLINDA/EXM 1.1 phantom and 85 g in the newer ones of OLINDA 2.
Time-Integrated Activity Coefficients at Different Stages of Gestation
Fetal Dose per Megabecquerel of 18F-FDG Administered to Mother
DISCUSSION
Fetal dose estimates for 18F-FDG were originally calculated with no information on placental crossover and fetal uptake (1) and were later amended using placental crossover data observed in primates (2). With the recent publication of several case reports and small series of women who underwent a PET scan while pregnant (4), it has become possible to calculate 18F-FDG fetal uptake directly in living human subjects.
The observed time-integrated activity coefficients were well fitted by a logistic function, which performed better in terms of goodness of fit than either a monoexponential curve or a quadratic curve. The parameters of this function allow extrapolating the time-integrated activity coefficients, and hence the dosimetry values, at any week of pregnancy. Future case reports may further refine these estimates, especially if full dynamic data become available.
Because of sigmoid fitting, activity coefficients plateaued after 34 wk. It is possible that some increase may occur also in the last weeks of pregnancy, but the data suggest that this increase would be small, especially when compared with the uncertainties in dose estimate (9). Moreover, a final plateau is present in many, although not all, fetal growth curves (10,11). In all likelihood, an accurate fetal dosimetry in the very last weeks of pregnancy has probably little clinical relevance: if the PET scan cannot be postponed until delivery a couple of weeks later, labor can be induced before the beginning of diagnostic and clinical work-up.
According to our estimates, an administered activity of 200 MBq would deliver a fetal dose ranging from 5.2 mSv in early pregnancy to 1.4 mSv in late pregnancy. Considering the uncertainties in all internal dose values for radiopharmaceuticals, conservatism and rounding in general should be applied to reported values. However, these values are well below the threshold for deterministic effects and in a range where stochastic effects have never been observed (12).
CONCLUSION
Using the new activity coefficients published by Zanotti-Fregonara et al. (4) and the realistic voxel-based phantoms of Shi et al. (5), updated fetal doses are recommended: 2.6E−02 mGy/MBq in early pregnancy, 1.9E−02 mGy/MBq at 3-mo gestation, 1.4E−02 mGy/MBq at 6-mo gestation, and 6.9E−03 mGy/MBq at 9-mo gestation.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 1, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 27, 2017.
- Accepted for publication May 26, 2017.





{kind=link}