


Abstract
SUV, which is an indicator of the degree of glucose uptake in 18F-FDG PET, can be applied as a prognostic factor in various malignant tumors. We investigated the prognostic impact of early changes in 18F-FDG PET uptake in patients with locally advanced breast cancer who received neoadjuvant chemotherapy. Methods: We retrospectively identified 87 patients who were treated with neoadjuvant chemotherapy followed by surgery for locally advanced breast cancer. All patients underwent 18F-FDG PET at baseline and after 3 cycles of neoadjuvant chemotherapy, and the SUVmax of the primary tumor was assessed in each scan. Pathologic slides were retrospectively reviewed, and the residual cancer burden (RCB) index was calculated to estimate pathologic response. RCB-0 indicates no residual disease; patients with residual disease were categorized as RCB-1 (minimal residual disease), RCB-2 (moderate residual disease), or RCB-3 (extensive residual disease). Results: There was a negative correlation between reduction in SUVmax and RCB index (r = −0.408; P < 0.001). On multivariate analysis, ΔSUVmax was a significant independent prognostic factor for recurrence-free and overall survival, and the respective adjusted hazard ratios were 0.97 (95% confidence interval, 0.95–0.99; P = 0.001) and 0.97 (95% confidence interval, 0.95–0.99; P = 0.015). When patients were categorized into groups according to pathologic response (RCB index ≤ 1 vs. ≥ 2) and metabolic response (ΔSUVmax ≤ 66.4% vs. > 66.4%), metabolic responders had significantly better recurrence-free and overall survival than metabolic nonresponders among poor-pathologic-response patients. In contrast, among metabolic responders, there was no survival difference according to pathologic response. Conclusion: The early change in 18F-FDG PET SUVmax after third-cycle neoadjuvant chemotherapy is an independent and good prognostic marker beyond pathologic response in patients with locally advanced breast cancer. We suggest that in these patients, the use of ΔSUVmax should be considered not only for the assessment of tumor response but for the prediction of posttreatment outcome.
In patients with locally advanced breast cancer, neoadjuvant chemotherapy has been widely accepted as a standard treatment because it can improve the surgical options and provide survival outcomes equivalent to those of conventional adjuvant chemotherapy (1–3). Moreover, neoadjuvant chemotherapy can assess sensitivity to chemotherapy, which can be helpful in modifying subsequent treatment according to an individual’s response (4).
Pathologic complete response (pCR) has been used as a surrogate marker for treatment outcome in some subtypes of breast cancer, because in these subtypes the survival outcome has been better for women who had pCR than for those who did not (5–8). Breast cancer, however, is a heterogeneous disease with varying biologic characteristics, and the pathologic response to neoadjuvant chemotherapy is not always matched by prognosis. A recent metaanalysis found that in subgroups having slowly proliferating tumors, such as luminal-type, pCR did not correlate with prognosis (7,8). Among the tools to evaluate pathologic response, the residual cancer burden (RCB) index has been adopted for neoadjuvant chemotherapy. This index has a scoring system more advanced than the simple dichotomization of response as pCR or residual disease only (9), and it can provide strong prognostic information derived from the primary tumor dimensions, the cellularity of the tumor bed, and the axillary nodal burden.
18F-FDG PET is a molecular imaging modality that reflects the biologic characteristics of a tumor and can predict its behavior and the patient’s prognosis (10–12). In addition, 18F-FDG PET is a sensitive technique for assessing response to therapy; studies have found that early changes in 18F-FDG uptake by tumors after 1 or 2 courses of neoadjuvant chemotherapy can predict pathologic response (13–16). The aim of the present study was to investigate the prognostic impact of early changes in 18F-FDG uptake in breast cancer patients who received neoadjuvant chemotherapy, especially compared with the RCB index.
MATERIALS AND METHODS
Patients
Between January 2004 and December 2011, 196 women with clinical stage II or III primary breast cancer received neoadjuvant chemotherapy. Of these, 87 patients who underwent 18F-FDG PET/CT before starting the therapy and again after the third cycle were identified. Patients with distant metastasis or bilateral breast cancer were excluded. The study was approved by the institutional review board of Gangnam Severance Hospital, Yonsei University, Seoul, Republic of Korea, in accordance with good clinical practice guidelines and the Declaration of Helsinki, and the requirement to obtain informed consent was waived.
The clinical data of each patient were reviewed, and the pathologic findings were recorded. The modified Scarf–Bloom–Richardson system was used for tumor grading. Expression of estrogen receptor, progesterone receptor, human epidermal growth factor receptor 2 (HER2), and Ki-67 was evaluated using formalin-fixed, paraffin-embedded tissue obtained from core biopsy or surgery. Immunohistochemistry staining was performed with appropriate antibodies for estrogen receptor (6F11; Novocastra), progesterone receptor (16; Novocastra), HER2 (4B5; Ventana Medical Systems), and Ki-67 (MIB-1; Dako). Estrogen receptor and progesterone receptor were determined by nuclear staining, which was scored from 0 to 8 using the system of Allred et al. (17). The results were categorized as positive when the total score, expressed as the sum of the proportion score and the intensity score, was 3 or greater. For HER2 evaluation, membranous staining was graded as 0, 1, 2, or 3 (18). A tumor with a score of 3 was considered positive, and equivocal results (in the case of a score of 2) were further tested by fluorescent in situ hybridization to confirm HER2 amplification (PathVysion HER2 DNA probe kit; Abbott-Vysis). The patients were categorized into 4 intrinsic subtypes using a Ki-67 cutoff of 14%, according to the criteria recommended by the St. Gallen panelists (19).
Neoadjuvant Chemotherapy
All but two of the patients received anthracycline-based neoadjuvant chemotherapy. The other two were treated with cyclophosphamide (600 mg/m2), methotrexate (40 mg/m2), and 5-fluorouracil (600 mg/m2) every 4 wk. Sixty-eight women received doxorubicin (50 mg/m2) and docetaxel (75 mg/m2) every 3 wk; 19 received cyclophosphamide (600 mg/m2), doxorubicin (60 mg/m2), and 5-fluorouracil (600 mg/m2) every 4 wk; and 2 received doxorubicin (60 mg/m2) and cyclophosphamide (600 mg/m2) every 3 wk. After completion of the neoadjuvant chemotherapy, the patients underwent breast-conserving surgery or mastectomy with axillary lymph node dissection, followed by anti-HER2 therapy, endocrine therapy, or radiotherapy according to the standard guidelines.
18F-FDG PET or PET/CT Method
The patients had fasted for at least 6 h and had a blood glucose level of less than 140 mg/dL before the 18F-FDG (5.5 MBq/kg of body weight) was intravenously administered. Sixty minutes afterward, whole-body emission scans were obtained on an Allegro PET camera (Philips) (for patients imaged before 2008) or PET/CT scans were obtained on a hybrid scanner (Biograph 40 TruePoint or Biograph mCT 64; Siemens Healthcare Solutions USA, Inc.) (for patients imaged between 2008 and 2011). Whole-body CT images were obtained first for attenuation correction using automatic dose modulation with a reference of 40 mA and 120 kV without contrast enhancement. Then, PET data were acquired from the skull base to the proximal thigh for 3 min per bed position in 3-dimensional mode. The PET images were reconstructed using ordered-subset expectation maximization. For semiquantitative evaluation, SUVmax was calculated by measuring 18F-FDG uptake by the primary tumor in the region of interest, as follows: SUVmax = [maximal radioactivity concentration in region of interest]/[injected dose/patient’s weight (kg)]. The percentage reduction in SUVmax (ΔSUVmax) after the third cycle of chemotherapy was calculated as [100 × (baseline SUVmax − third-cycle SUVmax)]/baseline SUVmax.
Pathology Assessment
All hematoxylin- and eosin-stained slides from the surgical specimens were reviewed, and the pathologic responses were evaluated. pCR was defined as no evidence of residual invasive cancer in the breast or axillary lymph nodes. Residual ductal carcinoma in situ was also defined as pCR. The RCB index was determined as described by Symmans et al. (9). Briefly, RCB index is derived from the primary tumor dimensions, the cellularity of the tumor bed, and the axillary nodal burden. RCB-0 indicates no residual disease; RCB-1, minimal residual disease; RCB-2, moderate residual disease; and RCB-3, extensive residual disease.
Statistical Analysis
To determine the optimal cutoff for ΔSUVmax, we applied the method of Contal and O’Quigley, which uses an algorithm that maximizes the hazard ratio (20). Recurrence-free survival was measured from the date of the first curative surgery to the date of the first tumor recurrence, including locoregional recurrence, distant metastasis, or death. Overall survival was measured from the date of the first curative surgery to the date of the last follow-up or until death from any cause during the follow-up period. The Kaplan–Meier method was used to estimate recurrence-free and overall survival. Multivariate Cox proportional-hazards regression was used to examine risk factors that showed statistical significance on univariate analysis. The concordance index, which is a measure of discrimination for model validation, was also examined.
All statistical analyses were performed using SPSS, version 18.0 (SPSS Inc.), and R (http://www.r-project.org) software. A P value of less than 0.05 was considered to indicate a statistically significant difference.
RESULTS
Patient Characteristics
The clinicopathologic characteristics of the 87 patients are presented in Table 1. There were 17 patients with pCR and 6 patients with minimal residual disease (RCB-1). The median follow-up period was 61 mo (10–107 mo), during which 24 patients (27.6%) had recurrence and 15 patients (17.2%) died. All deaths were associated with breast cancer.
Characteristics of the 87 Patients
Relationship Between ΔSUVmax and pCR
The mean ΔSUVmax of the 87 patients was 69.1% (range, 4.2%–100%). Patients with pCR had a higher mean ΔSUVmax than those without pCR (81.6 vs. 66.0, P = 0.016). There was a negative correlation between ΔSUVmax and RCB index (r = −0.408; P < 0.001). The mean ΔSUVmax (±SD) was 81.5% ± 21.1 in RCB-0 patients, 76.0% ± 15.8 in RCB-1 patients, 71.4% ± 22.9 in RCB-2 patients, and 52.9% ± 24.5 in RCB-3 patients (Fig. 1).
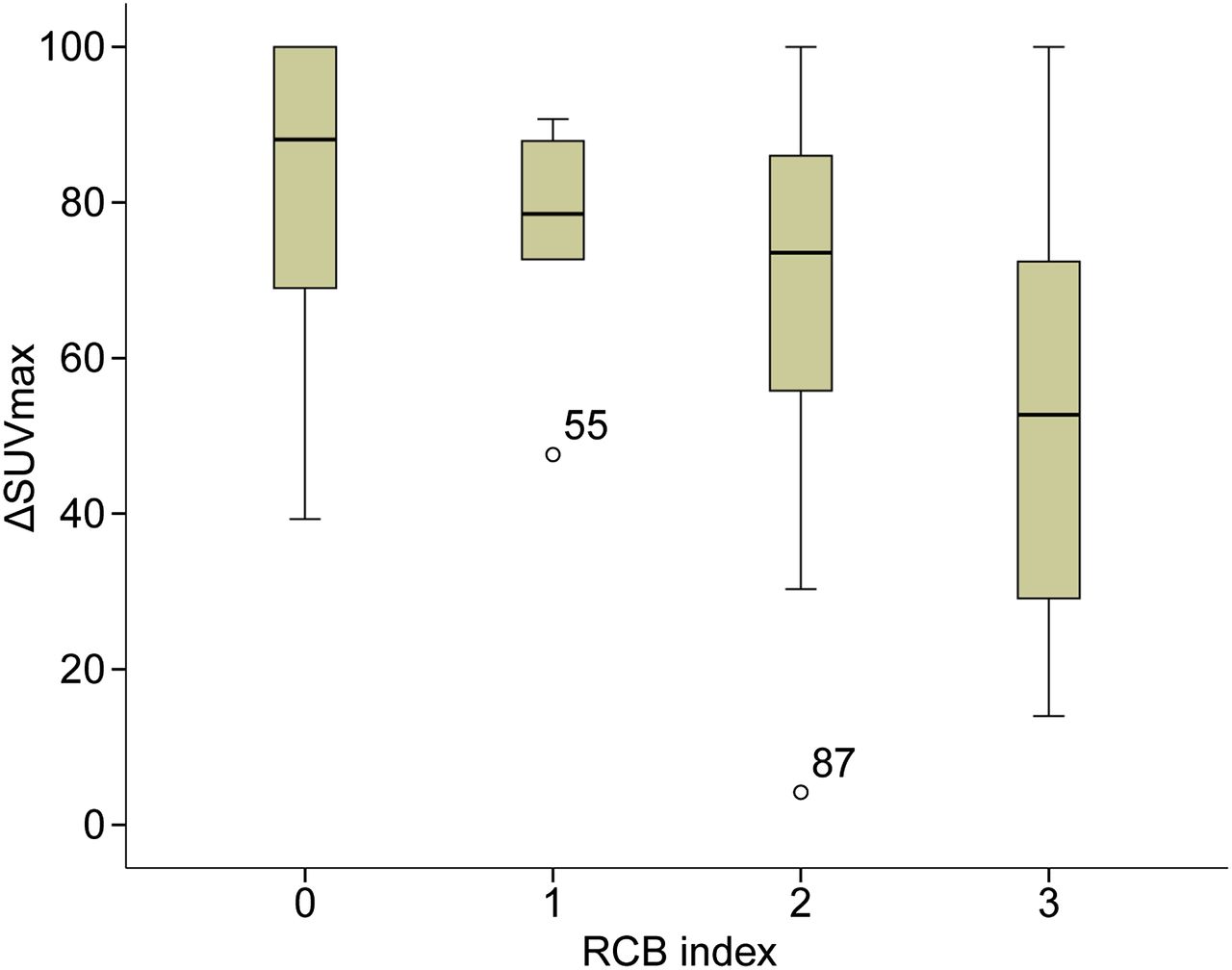
Comparison of ΔSUVmax according to RCB index.
Prognostic Impact of ΔSUVmax
On univariate analysis, an increased risk of recurrence was associated with advanced clinical N stage (P < 0.001), subtype (P = 0.003), and ΔSUVmax (P < 0.001) (Table 2). On multivariate analysis, clinical N stage, subtype, and ΔSUVmax were significant independent prognostic factors for recurrence-free survival, and the concordance index for this model was 0.82 (Table 3).
Univariate Analysis of Recurrence-Free and Overall Survival
Multivariate Analysis of Recurrence-Free and Overall Survival
On univariate analysis for overall survival, the significant factors were clinical T stage (P = 0.045), N stage (P = 0.005), subtype (P = 0.038), and ΔSUVmax (P = 0.014) (Table 2). Although the Kaplan–Meier overall survival estimation showed a statistical difference according to RCB index (P = 0.034), the prognostic value of RCB index was not retained in the multivariate analysis because of statistical insignificance found on univariate Cox analysis (P = 0.120). In multivariate analysis, ΔSUVmax and clinical N stage were significant independent prognostic factors for overall survival (P = 0.015 and 0.05, respectively), and the concordance index of this model was 0.87 (Table 3).
Using the method of Contal and O’Quigley, we selected 66.4% as the optimal cutoff to maximize the difference between recurrence-free and overall survival for ΔSUVmax. Patients were categorized as metabolic responders if ΔSUVmax was greater than 66.4% and as metabolic nonresponders if 66.4% or less. There were 55 metabolic responders and 32 nonresponders, and they significantly differed in recurrence-free and overall survival (Fig. 2). In our current data, the smallest SUVmax reduction required to achieve a pathologic response (RCB-0 or RCB-1) was 39.3%. When we used this value as a cutoff for ΔSUVmax in the current study, similar results were observed. We further investigated whether there was any survival difference according to ΔSUVmax among the molecular subtypes of breast cancer. There was a statistically significant difference in recurrence-free survival and a tendency toward a difference in overall survival between metabolic responders and nonresponders for the luminal subtype (P = 0.005 and 0.061, respectively, Supplemental Fig. 1; available at http://jnm.snmjournals.org), and there was a statistically significant difference in recurrence-free survival between metabolic responders and nonresponders for the nonluminal (triple-negative and HER2) subtypes (P = 0.042).

Kaplan–Meier survival curves according to cutoff of 64.4% for ΔSUVmax.
Comparison of ΔSUVmax and RCB Index
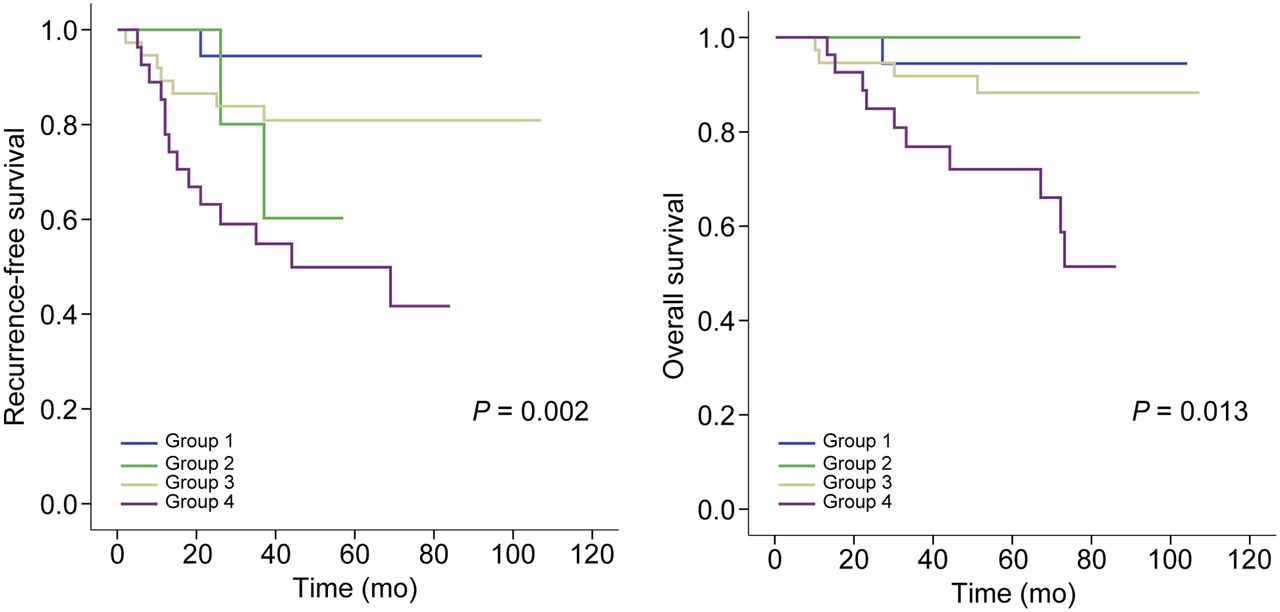
We investigated whether there were any survival differences according to metabolic response between patients with a good pathologic response (RCB index ≤ 1) and those with a poor pathologic response (RCB index ≥ 2). Patients were categorized into 4 groups according to RCB index and ΔSUVmax: group 1 comprised pathologic responders and metabolic responders; group 2, pathologic responders and metabolic nonresponders; group 3, pathologic nonresponders and metabolic responders; and group 4, pathologic nonresponders and metabolic nonresponders. Within the groups that included pathologic nonresponders, the Kaplan–Meier recurrence-free and overall survival estimates differed significantly according to ΔSUVmax (P = 0.007 and P = 0.017, respectively, Fig. 3). Conversely, within the groups that included metabolic responders, there was no difference in either recurrence-free or overall survival according to RCB index (P = 0.185 and 0.523, respectively). When we used pCR and non-pCR to discriminate pathologic response, similar results were observed (Supplemental Fig. 2).

Kaplan–Meier survival estimates. P values for log-rank results for recurrence-free survival were 0.054 for groups 1 and 2, 0.185 for groups 1 and 3, 0.394 for groups 2 and 3, and 0.007 for groups 3 and group 4. P values for log-rank results for overall survival were 0.598 for groups 1 and 2, 0.523 for groups 1 and 3, 0.464 for groups 2 and 3, and 0.017 for groups 3 and 4.
DISCUSSION
A potential advantage of neoadjuvant chemotherapy is the ability to monitor the degree of response. A previous randomized phase III study in which patients were randomly assigned to a regimen that would be maintained, versus one that would be prolonged or switched according to the early response to neoadjuvant chemotherapy, showed that response-guided neoadjuvant chemotherapy might improve survival in patients with early breast cancer (21). Thus, it is important to monitor early response in patients receiving neoadjuvant chemotherapy, and a wide variety of imaging and pathologic measurements have been used to assess the response so far.
Because 18F-FDG PET can reflect the biologic characteristics of tumors, it is an attractive method for assessing the response to neoadjuvant chemotherapy (12,13). Prospective clinical studies showed that an early change in 18F-FDG uptake is a surrogate marker of survival in patients with triple-negative breast cancer and even in patients with luminal HER2-negative breast cancer (22,23). The results of the present study also support these findings, and we additionally demonstrated that ΔSUVmax is a significant independent predictive and prognostic factor. Moreover, ΔSUVmax provided additional prognostic information in patients with pathologic nonresponse (high RCB index). Although pathologic response in metabolic responders failed to show a survival difference, ΔSUVmax was able to demonstrate the difference in recurrence-free and overall survival in pathologic nonresponders. Furthermore, we found that the smallest reduction in SUVmax required to achieve pathologic response was 39.3%, indicating that pathologic response becomes relevant only after a certain amount of metabolic response has occurred. Thus, metabolic response to neoadjuvant chemotherapy is more sensitive than pathologic response. Our previous study showed that in the adjuvant setting, prognosis correlates more significantly with the tumor-metabolism information provided by 18F-FDG PET than with tumor burden (24). These findings suggest that tumor biology significantly affects not only prognosis but also response to neoadjuvant chemotherapy.
There have been efforts to advance the assessment of response to neoadjuvant chemotherapy by combining pathologic response and biologic factors. To assess prognosis after neoadjuvant chemotherapy, M.D. Anderson Cancer Center has described a new staging system based on pretreatment clinical stage, estrogen receptor status, grade, and posttreatment pathologic stage (25). Another group has provided proof of principle that the addition of posttreatment Ki-67, grade, and estrogen receptor to RCB improves the prediction of long-term outcome (26). However, all such systems essentially need postoperative pathologic findings. 18F-FDG PET can provide prognostic information without pathologic findings and the surgery required to obtain them.
Our study had some limitations related mostly to its retrospective nature. Because of differences in study populations, methods of evaluation, and types of treatment, as well as the limited number of patients in each study, there currently is no standard optimal cutoff for categorizing patients as metabolic responders or nonresponders according to survival outcome. The cutoff we selected, 66.4%, differs from that of previous studies (22,23). However, this study did not aim to define the standard optimal cutoff but to determine whether metabolic response as assessed by 18F-FDG uptake can add information to pathologic response. Further prospective studies are required to determine the optimal cutoff.
CONCLUSION
We have highlighted the biologic and prognostic impact of an early change in 18F-FDG uptake in patients with locally advanced breast cancer who received neoadjuvant chemotherapy. The reduction in 18F-FDG PET SUVmax after the third cycle of neoadjuvant chemotherapy is an independent and good prognostic marker beyond pathologic response. We suggest that in these patients, the use of ΔSUVmax should be considered not only for the assessment of tumor response but for the prediction of posttreatment outcome.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This research was supported by grant 2013R1A1A2007759 from the Basic Science Research Program of the National Research Foundation of Korea (NRF), funded by the Ministry of Education, Science and Technology. No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Mar. 31, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication August 31, 2015.
- Accepted for publication March 8, 2016.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.