


Abstract
PET with O-(2-18F-fluoroethyl)-l-tyrosine (18F-FET) has gained increasing importance for glioma management. With regard to the occurrence of 18F-FET–negative glioma, we investigated the value of 18F-FET PET monitoring of primarily 18F-FET–negative gliomas concerning the detection of progression and malignant transformation. Methods: We included 31 patients (26 World Health Organization [WHO] grade II, 5 WHO grade III) with primarily 18F-FET–negative glioma and available 18F-FET PET follow-up. 18F-FET PET analysis comprised maximal tumor-to-background ratio (TBRmax) and dynamic analysis of tumoral 18F-FET uptake over time (increasing vs. decreasing) including minimal time to peak (TTPmin). PET findings were correlated with MRI and clinical findings of progression as well as histology of recurrent tumors. Results: Twenty-three of 31 patients experienced tumor progression (median progression-free survival, 41.7 mo). Fourteen of 23 patients showed tumoral 18F-FET uptake concurrent to and 4 of 23 before MRI-derived or clinical signs of tumor progression; 2 of 23 patients presented signs of progression in MRI when no concomitant 18F-FET PET was available, but subsequent follow-up PET was positive. In 3 of 23 patients, no 18F-FET uptake was detected at tumor progression. Overall, 20 of 31 primarily 18F-FET–negative glioma turned 18F-FET–positive during the follow-up. At first occurrence of tumoral 18F-FET uptake, TBRmax was significantly higher in patients with malignant transformation (11/20) than in those without malignant progression (3.2 ± 0.9 vs. 1.9 ± 0.5; P = 0.001), resulting in a high detection rate for malignant transformation (for TBRmax > 2.46: sensitivity, 82%; specificity, 89%; negative predictive value, 80%; positive predictive value, 90%; and accuracy, 85%). Although static evaluation was superior to dynamic analysis for the detection of malignant transformation (for TTPmin ≤ 17.5 min: sensitivity, 73%; specificity, 67%; negative predictive value, 67%; positive predictive value, 73%; and accuracy, 70%), short TTPmin was associated with an early malignant transformation in the further disease course. Overall, 18 of 31 patients experienced malignant transformation; of these, 16 of 17 (94%) evaluable patients showed 18F-FET uptake at the time of malignant transformation. Conclusion: 18F-FET PET monitoring with static and dynamic evaluation is useful even in primarily 18F-FET–negative glioma, providing a high detection rate of both tumor progression and malignant transformation, partly before further signs of progression in MRI. Hence, 18F-FET uptake indicating malignant transformation might influence the patient management.
MRI represents the diagnostic gold standard in neurooncology, because it allows noninvasive evaluation of intracerebral neoplasms and represents the basis for therapy planning and monitoring. Because of its primarily morphologic information, standard anatomic imaging acquired by MRI lacks specific and reproducible information about tumor biology and activity (1).
Thus, molecular imaging with PET visualizing metabolic pathways has been increasingly implemented into clinical routine for neurooncologic settings and the workup of patients with glioma (2). In particular, radiolabeled amino acids and their analogs such as O-(2-18F-fluoroethyl)-l-tyrosine (18F-FET) PET are of substantial interest for neurooncologic imaging, because of their high uptake in biologically active tumor tissue and low uptake in normal brain tissue (3). During recent years, 18F-FET PET has been increasingly used to optimize and individualize the specific therapy: 18F-FET PET has shown its value for biopsy guidance and planning of surgery and radiotherapy (4–6). Furthermore, dynamic 18F-FET PET has shown utility for the estimation of tumor grade (7–9) and a remarkably high prognostic value in newly diagnosed glioma using the analysis of the time–activity curves including the parameter minimal time to peak (TTPmin), for which short TTPmin was associated with worse outcome (10,11). Besides these clinically relevant features at primary diagnosis, 18F-FET PET imaging was shown to improve disease monitoring by early identification of tumor recurrence and progression and discrimination from posttherapeutic changes (12–17). In patients with low-grade glioma, 18F-FET PET even enables the detection of malignant transformation (18).
However, around 30% of low-grade glioma and 5% of high-grade glioma do not present an enhanced 18F-FET uptake at primary diagnosis (8,10,11) and it remains unclear whether a consecutive reevaluation of these primarily 18F-FET–negative gliomas provides valuable information in the assessment of a possible progression or even malignant transformation in low-grade glioma. In particular, it remains to be evaluated whether tumor progression might be missed by follow-up 18F-FET PET imaging because of absent 18F-FET avidity of the tumor and, conversely, if a new tumoral 18F-FET enhancement is stringently attended by tumor progression or even malignant transformation.
Hence, we systematically evaluated the clinical value of consecutively repeated dynamic 18F-FET PET monitoring of primarily 18F-FET–negative glioma in a cohort of patients with newly diagnosed, histologically proven glioma.
MATERIALS AND METHODS
Patient Evaluation
Patients with newly diagnosed, histologically confirmed glioma with a concurrent 18F-FET PET scan with tumoral uptake not exceeding the background activity in the visual analysis (18F-FET–negative) were included in this retrospective study. Clinical follow-up was obtained at regular intervals (every 6 mo for World Health Organization [WHO] grade II glioma and every 3 mo for WHO grade III glioma) in clinical routine.
All patients were investigated longitudinally with routine MR imaging as well as dynamic 18F-FET PET. Whenever possible, MRI and PET imaging were performed concomitantly. All patients gave written consent to undergo 18F-FET PET. The requirement to obtain informed consent for inclusion in the present analysis was waived by the local ethics committee.
Tumor Progression
Tumor progression was defined according to Response Assessment in Neuro-Oncology Criteria (19,20) by either MRI-derived signs of progression (increase of > 25% of T2/fluid-attenuated-inversion-recovery alteration, new contrast enhancement, new lesion) or clinical deterioration (i.e., new neurologic symptoms, worsening as indicated by Karnofsky performance score, an increase in administered steroid medication). In the case of tumor progression, a histologic confirmation via stereotactic biopsy or surgery was performed whenever possible.
PET Acquisition and Mode of Evaluation
Dynamic 18F-FET PET scans (40 min; 16 frames) were acquired with an ECAT Exact HR+ scanner (Siemens) according to standard protocols and evaluated on a Hermes workstation (Hermes Medical Solutions) as described previously (8). In first visual analysis, tumors were classified as 18F-FET–positive, if an increased 18F-FET uptake above cerebral background activity was observed; consequently, they were rated as 18F-FET–negative if tumors were not delineated from cerebral background activity in the PET scans. For the assessment of the maximal tumor to background ratio (TBRmax), the maximal SUV of the tumor was corrected for the mean background activity in the healthy contralateral hemisphere.
As described previously (8), dynamic PET data were evaluated in the case of new tumor uptake beyond the background activity. Within the 40-min dynamic scan, the time–activity curves were classified as increasing or decreasing. Additionally, the time to peak (TTP) was assessed in each slice within the tumor, and consequently the shortest TTP in at least 2 consecutive slices was defined as TTPmin. Regarding the exclusion of noise artifacts in the beginning of the PET acquisition due to low counting rates, only slices 11–16 (3–40 min after injection) were analyzed in the dynamic evaluation. According to the length of our frames, TTP is appointed for 4, 7.5, 12.5, 17.5, 25, and 35 min in frames 11–16, respectively.
MRI
Patients underwent routine MR imaging with a 1.5-T (Magnetom Symphony; Siemens) or a 3.0-T (Signa HDx, 3T; GE Healthcare) magnet. In all patients, axial T2-weighted sequences and T1-weighted sequences before and after intravenous administration of 0.1 mmol/kg gadobenatedimeglumine contrast agent (MultiHance; BraccoImaging) were acquired. Images were interpreted by an experienced radiologist using a PACS workstation (Sienet Magic View 1000; Siemens).
Histopathologic Evaluation
PET-guided stereotactic biopsy procedures or neuronavigated microsurgery with MR and PET image fusion (Brainlab) were used to ensure a spatially precise tissue-sampling procedure throughout the intracerebral tumors (21). Histologic classification and tumor grading were performed according to the current WHO guidelines (22).
Statistics
Statistical analysis was performed with SPSS Statistics (version 23; IBM). Descriptive statistics were used for patients’ characteristics and 18F-FET PET data (time–activity curves, TTPmin, and TBRmax). Normal distribution was assessed using the Shapiro–Wilk test. Contingency tables using the Fisher Exact test described the differences in the distribution of categoric parameters. An unpaired t test was used, evaluating continuous and normally distributed variables in 2 groups. Progression-free survival, time to malignization, and time to 18F-FET positivity were calculated using Kaplan–Meier-curves. Receiver-operating curves were calculated to define the optimal cutoff TBRmax for the differentiation between tumors with and without malignant transformation using Youden J statistic. Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were determined as measures of diagnostic quality in tests using the defined cutoff values of TBRmax and TTPmin. Statistical significance was defined for 2-tailed P values below 0.05.
RESULTS
Patient Characteristics and Follow-up
Thirty-one adults were identified between 2005 and 2015 (mean age ± SD, 38.1 ± 11.8 y; age range, 20.4–67.8 y; 13 women and 18 men). Histologic evaluation in tissue specimens obtained by stereotactic biopsy (27/31 patients) or surgery (4/31) revealed 26 glioma WHO grade II (2 oligoastrocytoma, 24 diffuse astrocytoma) and 5 glioma WHO grade III (1 anaplastic oligoastrocytoma, 4 anaplastic astrocytoma). Patient management consisted of a watch-and-wait strategy (10/31), surgical resection as primary treatment (9/31), stereotactic brachytherapy (5/31), temozolomide chemotherapy (3/31), and combined radio-/chemotherapy (4/31).
During the follow-up, 23 of 31 patients experienced tumor progression after a median time of 41.7 mo (95% confidence interval, 20.8–62.7 mo). Of these, 18 patients presented with malignant transformation after a median time of 50.0 mo (95% confidence interval, 35.4–64.6 mo), which was confirmed by histopathology (9 biopsy, 7 surgery) in 16 of 18 patients (5 cases of WHO grade II to WHO grade III; 11 cases of WHO grade II to WHO IV). Two of 18 patients had significant clinical worsening accompanied by characteristic findings in MRI indicating malignant transformation (i.e., new contrast enhancement and massive edema) without further biopsy.
Overall, 20 of 31 initially 18F-FET–negative glioma patients became 18F-FET–positive, whereas 11 patients stayed 18F-FET–negative along the whole follow-up (8/11 without further signs of progression and 3/11 with signs of progression). The median time to first occurrence of tumoral 18F-FET uptake was 40.4 mo (95% confidence interval, 31.8–50.0 mo).
Direct Comparison of 18F-FET PET with MRI-Derived and Clinical Signs of Progression
18F-FET PET scans (n = 145) were evaluated in 31 patients. PET scans were correlated to clinical signs of progression as well as the MRI scans closest to the PET imaging (median interval, 10 d). The median number of evaluated PET/MRI scans was 4/4 per patient, with a median interval of 9.2/9.3 mo between the scans.
In 72 of 145 18F-FET–negative scans, there were no signs of progression in MRI, whereas in 3 18F-FET–negative scans concurrent MRI indicated progression. The rate of correct negative cases was 96%. In the case of enhanced 18F-FET uptake, 63 of 145 scans were associated with concurrent clinical or MRI-derived signs of progression. Seven scans showed enhanced 18F-FET uptake before clinical or MRI-derived signs of progression.
Patient-Based Analysis
Of the 23 patients with tumor progression during follow-up, 18F-FET PET turned positive in 20 patients: 14 of 20 patients showed 18F-FET uptake concomitant to signs of progression. Four of 20 patients showed a new 18F-FET uptake without concomitant signs of progression. However, in 3 of these, tumor progression was proven shortly after with histologically verified malignant transformation (2 cases of WHO grade III and 1 case of WHO grade IV; median time between 18F-FET–positive PET scan and malignant transformation, 7.0 mo), and 1 patient showed signs of progression after 64.2 mo. Two of 20 patients presented signs of progression as well as a new enhanced uptake in 18F-FET PET; nonetheless, no definite information concerning the temporal relationship between PET and MRI could be assessed in these 2 cases because of a time delay between MRI and subsequent 18F-FET PET examination. However, this subsequent 18F-FET PET scan was positive.
Among the 23 patients with tumor progression, 3 of 23 patients did not exhibit any tumoral 18F-FET uptake. All 3 patients showed signs of progression in MRI in terms of tumor enlargement but did not provide contrast enhancement as a sign of malignant transformation or any clinical worsening at that point of time. Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org) provides an overview.
Value of PET Parameters at First Occurrence of Enhanced 18F-FET Uptake
At the time of the first occurrence of enhanced tumoral 18F-FET uptake, a malignant transformation was diagnosed in 11 of 20 patients (55%), which was confirmed by histopathology in 10 of 11 patients (3 cases WHO grade II →WHO grade III and 7 cases WHO grade II → WHO grade IV); 1 patient showed characteristic findings in MRI representing a malignant transformation without histologic verification (Table 1).
Overview of Patients Presenting with New 18F-FET Uptake in Follow-up
The remaining 9 of 20 patients did not show a malignant transformation (8 patients with histologic reevaluation without change of tumor grade; 1 without MRI-derived signs of malignant transformation).
The mean TBRmax was 2.6 ± 1.0 (range, 1.46–4.16) in the overall group and was significantly higher in patients with malignant transformation than in those without (3.2 ± 0.9 vs. 1.9 ± 0.5; P = 0.001). Receiver-operating-curve analysis revealed an optimal cutoff TBRmax of 2.46 for the detection of malignant transformation (area under the curve, 0.92; Jouden J, 0.71), leading to a sensitivity of 82%, a specificity of 89%, a negative predictive value of 80%, and a positive predictive value of 90%. The accuracy was 85%.
Concerning the kinetic analysis, the best cutoff for the detection of malignant transformation by TTPmin was ≤ 17.5 min: a short TTPmin ≤ 17.5 min was seen in most cases with malignant transformation (8/11 cases) (Fig. 1), but 3 of 11 patients with malignant transformation showed a TTPmin of 35 min. In contrast, for patients without malignant transformation (Fig. 2) only 3 of 9 presented with a short TTPmin ≤ 17.5 min, whereas most had a longer TTPmin (1/9 patient: TTPmin 25 min; 5/9 patients: TTPmin 35 min).
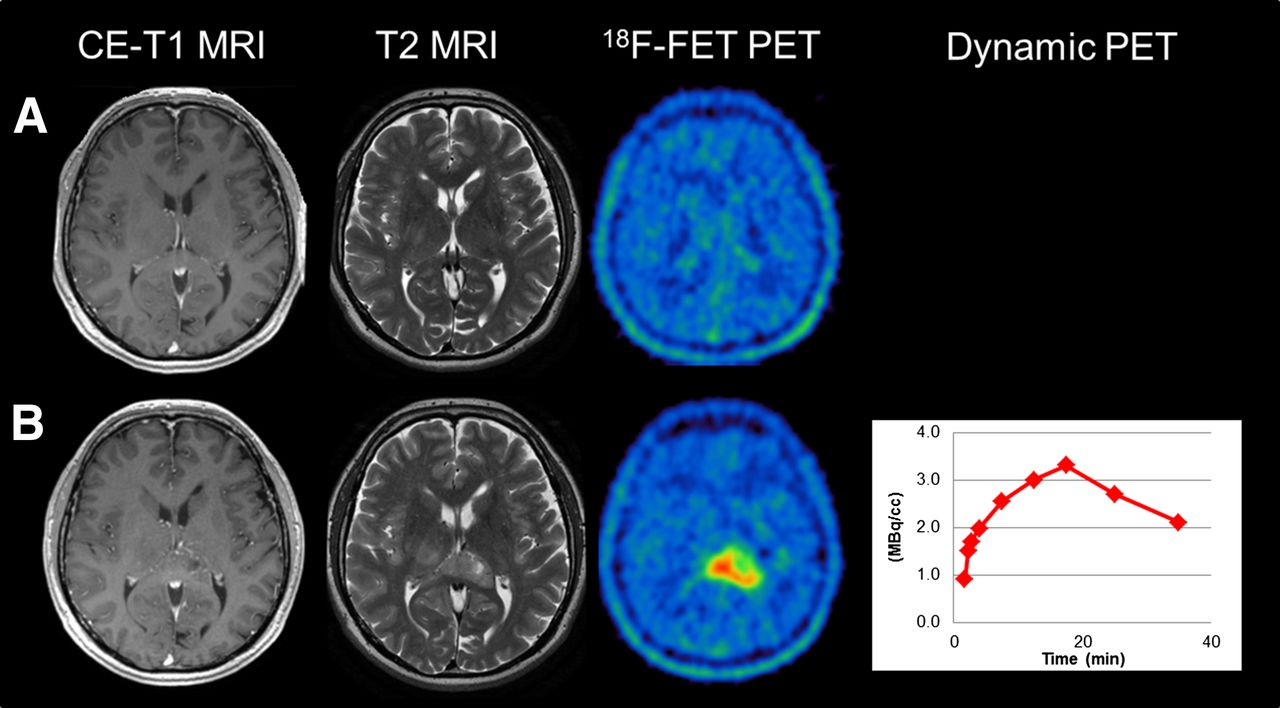
Example of a patient with 18F-FET–negative diffuse astrocytoma (WHO grade II) in left occipital lobe (A) presenting with first occurrence of enhanced 18F-FET uptake after 8 mo (TBRmax, 3.92; decreasing time–activity curves with TTPmin of 17.5 min) and concomitant malignant transformation to glioblastoma multiforme (WHO grade IV) (B).
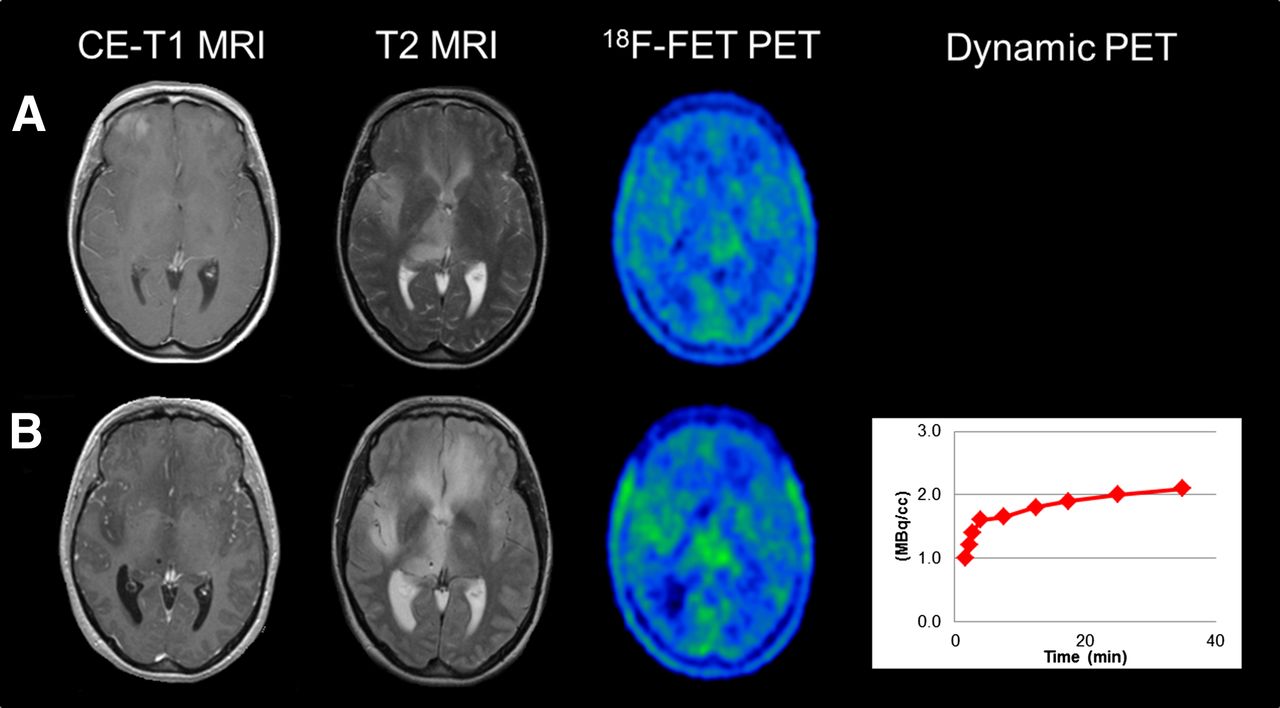
Example of a patient with an initial 18F-FET–negative diffuse astocytoma (WHO grade II) (A) presenting with new 18F-FET uptake in 18F-FET PET (TBRmax, 1.62; increasing time–activity curves with TTPmin of 35 min) after 54 mo without malignant transformation (B).
When the TTPmin cutoff of ≤ 17.5 min was used, the dynamic evaluation provided a sensitivity of 73%, a specificity of 67%, a negative predictive value of 67%, and a positive predictive value of 73%. The accuracy of the dynamic evaluation concerning malignant transformation at the time of newly enhancing uptake was 70%. However, all 3 patients with a short TTPmin but no malignant transformation at the time of the PET scan experienced a subsequent progression with histologically proven transformation to a WHO grade IV glioma shortly afterward (5.1, 8.4, and 9.0 mo after first 18F-FET uptake). On the contrary, among the remaining patients without malignant transformation (6/9) who had a TTPmin > 17.5 min, 4 did not show any signs of malignant transformation during the follow-up and merely 2 developed malignant transformation (after 7.1 and 14.0 mo).
18F-FET PET Characteristics at Time of Malignant Transformation
Eighteen of 31 patients experienced a malignant transformation during follow-up, which was assessed by histologic evaluation in 16 of 18 patients (9 biopsy, 7 surgery); 2 of 18 patients provided characteristic findings in MRI. One of 18 patients was lost to PET follow-up because there was no more 18F-FET PET evaluation in the course of disease. Sixteen of 17 evaluable patients (94%) had a positive 18F-FET PET scan at the time of malignant transformation, whereas only 1 patient did not show tumoral 18F-FET uptake. This single patient experienced tumor progression first in terms of tumor growth only without malignant transformation and belonged to the 3 of 23 progressive glioma patients with ongoing negative 18F-FET PET. The 16 of 17 18F-FET–positive patients presented with a mean TBRmax of 3.1 ± 0.9 (range, 1.6–4.2). Thirteen of 16 patients showed decreasing time–activity curves, with a TTPmin in the range of 12.5–17.5 min; 3 of 16 presented with increasing time–activity curves and a consecutive TTPmin of 35 min.
DISCUSSION
So far, it remains uncertain to what extent a monitoring of primarily 18F-FET–negative glioma using serial 18F-FET PET scans provides additional information in the clinical workup of those patients. To our knowledge, this is the first study systematically evaluating the possible clinical value of repeated dynamic 18F-FET PET monitoring of initially 18F-FET–negative glioma.
Sixty-five percent of our patients turned 18F-FET–positive during the follow-up, demonstrating that gliomas do change their 18F-FET uptake behavior throughout the disease course. Repeated 18F-FET PET showed a new tumoral uptake concomitant or even before clinical or MRI-derived signs of progression in most cases. In the minority (14%), tumor progression was not depicted by 18F-FET PET as it stayed negative. However, these patients presented with tumoral enlargement on MRI only and did not have a malignant transformation. Notably, in some patients (17%) new tumoral 18F-FET uptake preceded the MRI-derived and clinical signs of progression, and most of them experienced progressive disease with histologically proven tumor malignization after a median time of 7 mo only. This leads to the assumption that newly enhanced 18F-FET uptake of primarily negative gliomas indicates at least a progression concomitant or even before MRI-derived and clinical signs of progression. Notably, 55% of the patients with newly observed 18F-FET uptake had a concurrent malignant transformation, indicating that the change of uptake characteristics might be associated to more aggressive tumor features.
A remarkably high discrimination between glioma increasing in size and glioma undergoing malignant transformation was obtained by TBRmax, leading to a diagnostic accuracy of 85%, whereas dynamic evaluation reached an accuracy of 70% only. Nonetheless, although the dynamic evaluation seemed to provide less discriminability compared with TBRmax, which was mainly due to the occurrence of a short TTPmin in gliomas without histopathologic confirmation of malignant transformation at that time, the dynamic analysis was associated with the patient’s prognosis: in all patients providing a TTPmin ≤ 17.5 min who had no malignant transformation at that time and rather low TBRmax (< cutoff 2.46 TBRmax), the clinical follow-up revealed malignant transformation only 5–9 mo later. Notably, 1 of these patients was histologically rated as constant WHO grade II but presented with diffuse pleomorphic changes at that time already, yet without reaching the formal criteria of a WHO grade III glioma. Six months later, a malignant transformation to a glioblastoma was confirmed histologically. In contrast, only a few patients with a TTPmin > 17.5 min at the time of new 18F-FET uptake and unchanged WHO grade experienced subsequent malignant transformation after 7 and 14 mo. The features of kinetic analysis indicate that time–activity curves and particularly TTPmin are associated with patient’s prognosis in newly 18F-FET–enhancing glioma, which is in line with previous results reporting a short TTPmin in low- and high-grade glioma correlating with poor outcome (10,11).
Most of the patients had no tumor progression while staying 18F-FET–negative. Only a small part of patients had progressive disease despite a negative 18F-FET PET scan but, interestingly, with tumor enlargement only and without malignant transformation. Therefore, one might assume that an ongoing negative follow-up 18F-FET PET scan most likely indicates no malignant transformation at that point of time. Yet, this hypothesis cannot be proven by histology in our study, because it would not have been justified performing a stereotactic biopsy or surgery in these patients without any suspicion of tumor progression or malignant transformation.
The observation of cases with new 18F-FET uptake before further signs of progression, which even showed malignant transformation shortly afterward, indicates that 18F-FET PET might be able to identify malignant transformation before MRI by depicting subcellular changes in the tumor biology, leading to increased 18F-FET uptake. This would fit to the reported increasing 18F-FET uptake intensity of glioma and decreasing TTP during malignant transformation (18). Notably, 16 of 17 patients showed (newly occurring or already existing) 18F-FET uptake at the moment of malignant transformation in accordance with this hypothesis. The presence of contrast enhancement, on the contrary, might not be sensitive enough to reliably delineate malignant transformation. This hypothesis would be in line with literature describing a rate of up to 40% high-grade glioma in non–contrast-enhancing cerebral neoplasms at the time of initial diagnosis (23).
In the particular cases with tumor progression without any 18F-FET uptake, there was tumor growth in terms of significant enlargement of more than 25% in the T2/fluid-attenuated-inversion-recovery–weighted MRI, however, without signs of malignant transformation on MRI and according to the neuropathologic reevaluation. Of note, this cannot be related to any treatment effect in terms of a pseudoprogression, because none of these patients received prior therapy. Hence, it can be assumed that the mere morphologic tumor enlargement is not necessarily linked to pathophysiologic changes on the molecular level that would result in a change of 18F-FET uptake behavior, whereas malignant transformation leads to enhanced 18F-FET uptake in most of the cases.
The pathophysiologic mechanisms leading to 18F-FET uptake and the different dynamic uptake characteristics including TTPmin are not yet fully clarified. Particularly, it remains unclear which cellular mechanisms lead to the phenomenon of missing intracellular 18F-FET uptake in 18F-FET–negative gliomas. One might speculate that 18F-FET–negative gliomas are characterized either by a low expression or by low activity of the large neutral amino acid transporter at the tumor cells or at the brain capillary endothelial cells (24) responsible for intracellular uptake of amino acids (25). Besides, one might hypothesize that a rather low need of amino acids due to low protein synthesis of a glioma might lead to 18F-FET negativity, which would fit to the reported better outcome in patients without primary tumoral 18F-FET uptake compared with 18F-FET–enhancing tumors (26), but this hypothesis appears controversial as another study did not show a better prognosis in patients without tumoral 18F-FET uptake (10). Furthermore, it is still uncertain which cellular mechanisms are causing the different tumoral time–activity curves/TTPmin and their association to prognosis. Although changes in vascularization by neoangionesis and increased intratumoral microvessel density have been proposed as being related to the shape of the time–activity curves (10), there is no histopathologic study so far correlating these parameters to the different time–activity curves and TTPmin. When the hypothesis is that there possibly is an association between the tumoral vascularization and TTPmin, the finding of particular changes of TTPmin before malignant transformation would be in line with reports on increased regional cerebral blood volume in gliomas undergoing malignant transformation even 12 mo before contrast enhancement (27). Future studies should correlate PET findings with immunohistochemical and MR imaging parameters such as tumor perfusion/vascularization or the expression of the L-type amino acid transporter, to shed light into the pathophysiologic mechanisms of tumoral 18F-FET uptake.
Limitations of our study arise from the retrospective study design. Additionally, the included patients did not have a homogeneous treatment management. However, our study did not focus on patients’ outcome in general, which is certainly influenced by different therapies, but was intended to describe the 18F-FET PET findings of a primarily 18F-FET–negative glioma during follow-up and to correlate these findings, when available, with concomitant and follow-up MRI, clinical, and histologic results.
CONCLUSION
Monitoring of primarily 18F-FET–negative glioma using static and dynamic 18F-FET PET represents a feasible and useful approach, because it provides a remarkably high detection rate of both malignant transformation and progression with prognostic kinetic information at the time of 18F-FET positivity and in the course of disease, partly even before clinical and MRI-derived signs of progression. By implication, a repeated negative 18F-FET PET scan most likely indicates a favorable course of disease without progression or malignant transformation. Consequently, an enhanced 18F-FET uptake with short TTPmin indicating malignant transformation might lead to an earlier adequate treatment and improved clinical workup.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
Parts of this paper originate from the doctoral thesis of Florian Schweisthal.
Footnotes
Published online Mar. 31, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 10, 2015.
- Accepted for publication March 1, 2016.





{kind=link}
{kind=link}