


Abstract
Here we compare translocator protein (TSPO) imaging using 6-chloro-2-(4′-123I-iodophenyl)-3-(N,N-diethyl)-imidazo[1,2-a]pyridine-3-acetamide SPECT (123I-CLINDE) and amino acid transport imaging using O-(2-18F-fluoroethyl)-l-tyrosine PET (18F-FET) and investigate whether 123I-CLINDE is superior to 18F-FET in predicting progression of glioblastoma multiforme (GBM) at follow-up. Methods: Three patients with World Health Organization grade IV GBM were scanned with 123I-CLINDE SPECT, 18F-FET PET, and gadolinium-enhanced MR imaging. Molecular imaging data were compared with follow-up gadolinium-enhanced MR images or contrast-enhanced CT scans. Results: The percentage overlap between volumes of interest (VOIs) of increased 18F-FET uptake and 123I-CLINDE binding was variable (12%–42%). The percentage overlap of MR imaging baseline VOIs was greater for 18F-FET (79%–93%) than 123I-CLINDE (15%–30%). In contrast, VOIs of increased contrast enhancement at follow-up compared with baseline overlapped to a greater extent with baseline 123I-CLINDE VOIs than 18F-FET VOIs (21% vs. 8% and 72% vs. 55%). Conclusion: Our preliminary results suggest that TSPO brain imaging in GBM may be a useful tool for predicting tumor progression at follow-up and may be less susceptible to changes in blood–brain barrier permeability than 18F-FET. Larger studies are warranted to test the clinical potential of TSPO imaging in GBM, including presurgical planning and radiotherapy.
Glioblastoma multiforme (GBM) remains the most common and aggressive primary tumor of the central nervous system. With conventional radiotherapy, chemotherapy, and debulking surgery, mean survival from diagnosis is 14.6 mo (1).
GBM lesions are strongly enhanced on contrast-enhanced structural imaging (CT or MR imaging), but populations of glioma cells are also present in the peritumoral environment. Thus, in clinical trials the volume for radiotherapy has been defined as the region of enhancement plus an isotropic margin of 2–3 cm (1). The combination of MR imaging and O-(2-18F-fluoroethyl)-l-tyrosine PET (18F-FET) improves the sensitivity and specificity of tumor tissue detection (2,3). However, 18F-FET is not entirely glioma-specific, and increased uptake has been documented in astrogliosis secondary to infection, ischemia, radiation injury, demyelination, and hematoma (4–7). The 18-kDa translocator protein (TSPO) is a component of the mitochondrial permeability transition pore and is strongly expressed by glioma cell lines (8). In tissue resected from patients with astrocytoma, TSPO density correlates positively with malignancy and cell proliferation index and negatively with survival (9). 6-chloro-2-(4′-123I-iodophenyl)-3-(N,N-diethyl)-imidazo[1,2-a]pyridine-3-acetamide SPECT (123I-CLINDE; MAP Medical Technologies) has been validated as a second-generation TSPO tracer for use in humans (10) and recently in a GL26 mouse model of glioma (11). We present 123I-CLINDE SPECT, 18F-FET PET, and gadolinium-enhanced MR imaging results from 3 GBM patients at baseline compared with contrast-enhanced structural imaging at follow-up and hypothesize that 123I-CLINDE SPECT at baseline is an imaging biomarker of GBM progression.
MATERIALS AND METHODS
The study was performed in accordance with the ethical standards of the Declaration of Helsinki and approved by the ethical committee of the Copenhagen Capital Region (approval H-2-2010-086, amendment 39319). All subjects signed an informed consent form. Three patients in an advanced state of GBM (World Health Organization grade IV) were included and genotyped for the rs6971 polymorphism to determine the TSPO binder status as described previously (10). Before inclusion, all patients had undergone surgery and received radiotherapy and chemotherapy with temozolomide, bevacizumab and irinotecan. In addition, patients 2 and 3 had been treated with a cell-based immunotherapy. Patient 2 had undergone surgical resection between baseline and follow-up MR imaging. The patients were scanned with 123I-CLINDE, 18F-FET, and MR imaging within 2 d. Patients 1 and 2 were rescanned with MR imaging after 6 and 17 wk, respectively, and patient 3 was rescanned with CT after 4 wk. The patients received no treatment with angiogenesis-inhibiting drugs for 6 wk before the scans and no radiochemotherapy between scans.
Patients
Patient data, genotype, rescan modality, scan–rescan time intervals, and injected 123I-CLINDE dose are presented in Table 1.
Patients
Image Acquisition
After bolus injection of 123I-CLINDE, dynamic SPECT images were acquired with a triple-head IRIX camera (Philips Medical) for 2.5 h as previously described (10), and weighted mean images were generated for region analysis.
A single-frame static PET acquisition was performed 20–40 min after intravenous injection of approximately 200 MBq of 18F-FET on a 64-slice-CT Biograph TruePoint PET/CT scanner (Siemens). All PET scans were attenuation-corrected using low-dose CT performed immediately before the PET scan and were subsequently corrected for scatter and dead time. Images were reconstructed with an ordered-subsets expectation maximization 3-dimensional algorithm (6 iterations, 16 subsets) and a 5-mm gaussian filter. All patients fasted for at least 6 h before 18F-FET injection.
T1-weighted MR imaging was performed on a 3-T MR Verio scanner (Siemens). Gadolinium was used in a dose of 0.1 mmol/kg of body weight (Multihance [Bracco] or Gadovist [Schering]). Patient 3 was rescanned using a CT scanner (Siemens) and a CT contrast agent containing 70 mL of iodine (350 mg/mL) (Omnipaque; GE Healthcare).
Data Processing
The weighted mean 123I-CLINDE SPECT image was coregistered to the MR image of the same patient using interactive image overlay (12). 18F-FET PET images and the follow-up MR images were coregistered to the first MR image of the same subject, applying the automatic rigid-body model included with Statistical Parametric Mapping, version 8 (13).
The definition of volumes of interest (VOIs) with high 123I-CLINDE binding was standardized for all patients by automatically selecting voxels with a value above 1.5 times the mean cerebellar count. The delineation of high-uptake 18F-FET volumes was standardized as previously described (2). A trained neuroradiologist supervised delineation of the MR imaging volumes. Baseline MR imaging VOIs were delineated manually as the contrast-enhanced areas of the coregistered baseline MR image. Blood vessels were omitted. Volumes for SPECT, PET, and MR imaging were determined, along with common volumes. Furthermore, the Sørensen–Dice coefficient for SPECT, PET, and baseline MR imaging was calculated as  , with ∩ being the symbol of common volume. Volume of tumor progression was defined as the additional contrast-enhanced volume from baseline to follow-up. For patient 2, follow-up volume analysis was not performed because of surgical resection between the baseline and follow-up scans.
, with ∩ being the symbol of common volume. Volume of tumor progression was defined as the additional contrast-enhanced volume from baseline to follow-up. For patient 2, follow-up volume analysis was not performed because of surgical resection between the baseline and follow-up scans.
RESULTS
Table 2 shows the sizes of the 18F-FET and 123I-CLINDE VOIs as well as the volumes in common for high-binding 123I-CLINDE VOIs and high-uptake 18F-FET VOIs. The VOIs of increased 123I-CLINDE binding and 18F-FET uptake showed varying degrees of overlap (12%–42%). Binder status does not appear to determine the volume of 123I-CLINDE VOIs.
VOIs
Table 3 shows the volumes in common between baseline structural imaging and 123I-CLINDE or 18F-FET PET. In all cases, baseline MR imaging VOIs showed greater similarity to 18F-FET VOIs (Sørensen–Dice coefficients, 0.54, 0.69, and 0.40) than to 123I-CLINDE VOIs (Sørensen–Dice coefficients, 0.05, 0.36, and 0.18). The percentage overlap of MR imaging baseline VOIs was greater for 18F-FET VOIs (79%–93%) than for 123I-CLINDE VOIs (15%–30%).
Volumes in Common Between Baseline Structural Imaging and 123I-CLINDE or 18F-FET PET
Table 4 shows the volumes in common between tumor progression at follow-up structural imaging and baseline 18F-FET PET or 123I-CLINDE. In the 2 patients for whom follow-up tumor progression volumes were estimated, the volume with de novo contrast enhancement at follow-up overlapped to a greater extent with 123I-CLINDE VOIs than with 18F-FET VOIs (21% vs. 8% and 72% vs. 55%).
Volumes in Common Between Tumor Progression at Follow-up Structural Imaging and Baseline 18F-FET PET or 123I-CLINDE
DISCUSSION
This study follows 4 previous studies demonstrating TSPO in 1–3 patients with GBM using the TSPO PET tracer 11C-PK11195 PET (14–17). To our knowledge, this is the first study to address the clinical value of TSPO imaging in GBM patients by comparing the second-generation TSPO SPECT tracer 123I-CLINDE with 18F-FET PET and contrast-enhanced structural imaging.
The first aim of the present study was to evaluate the similarity of 123I-CLINDE and 18F-FET VOIs. We found only limited VOI overlap, indicating that imaging of amino acid uptake and TSPO binding reflects different aspects of GBM pathology. Increased 18F-FET uptake has been documented experimentally and clinically in reactive astrogliosis secondary to infection, ischemia, radiation injury, demyelination, and hematoma, indicating that 18F-FET is not entirely glioma-specific (4–7). In contrast, no TSPO expression was found in reactive astrogliosis in a recent study in untreated human glioma patients (17). In addition to binding to glioma cells, TSPO tracers bind to myeloid cell lines, including glioma-associated microglia and macrophages (18). In contrast, uptake of 18F-FET is not increased in areas of infiltrating activated macrophages and activated microglia in experimental abscesses (4,19). It may be hypothesized that TSPO-negative but 18F-FET–positive areas represent primarily reactive astrocytosis, predicting a less aggressive development, but biopsy control confirmation is needed.
The second aim was to evaluate the correspondence between the VOIs of increased 18F-FET uptake, the VOIs of increased 123I-CLINDE binding, and volumes of MR imaging contrast enhancement at baseline. We found that 18F-FET VOIs overlapped more (93%, 80%, 79%) with contrast-enhanced VOIs than with 123I-CLINDE VOIs (15%, 30%, 30%). Contrast enhancement reflects a disturbed blood–brain barrier and could be related to treatment and tissue necrosis and not glioma cell proliferation per se (20). The binding of 123I-CLINDE to TSPO does not appear to be significantly increased in areas of disrupted blood–brain barrier (10). It is known that glioma cells diffusely infiltrate brain tissue without disrupting the blood–brain barrier (21).
The third aim was to evaluate how 18F-FET and 123I-CLINDE VOIs overlap with VOIs representing tumor progression from baseline to follow-up on contrast-enhanced structural imaging. Follow-up VOI analysis was not performed for patient 2 because debulking surgery had taken place between baseline and follow-up scans and extravasation of gadolinium was highly increased in the area around the operation cavity on the follow-up scan. It appears that the VOIs of increased 123I-CLINDE at baseline are a good visual predictor of tumor progression at follow-up (Fig. 1). In line with the visual interpretation, the percentage overlap with VOIs representing tumor progression is higher for 123I-CLINDE than for 18F-FET (21% vs. 8% and 72% vs. 55%) in patients 1 and 3. The findings correspond to previous reports demonstrating the contribution of TSPO to the uncontrolled cellular proliferation of glioma cells (22) and the correlation between TSPO density in surgically removed glioma tissue with clinical parameters such as survival time and tumor cell proliferation index (8,9). TSPO is expressed in glioma cells, suggesting that this method may be a more sensitive and specific marker of ongoing tumor cell proliferation and progression than conventional imaging methods. In addition, glioma-associated macrophages and monocytes contributing to tumor progression through the release of proinflammatory and proangiogenic factors may also add to the TSPO signal (23). Thus, the addition of TSPO imaging to18F-FET PET has the potential to add information about areas of very active tumor cell proliferation in GBM. This may explain why low-grade gliomas have few or no TSPO binding sites (17).
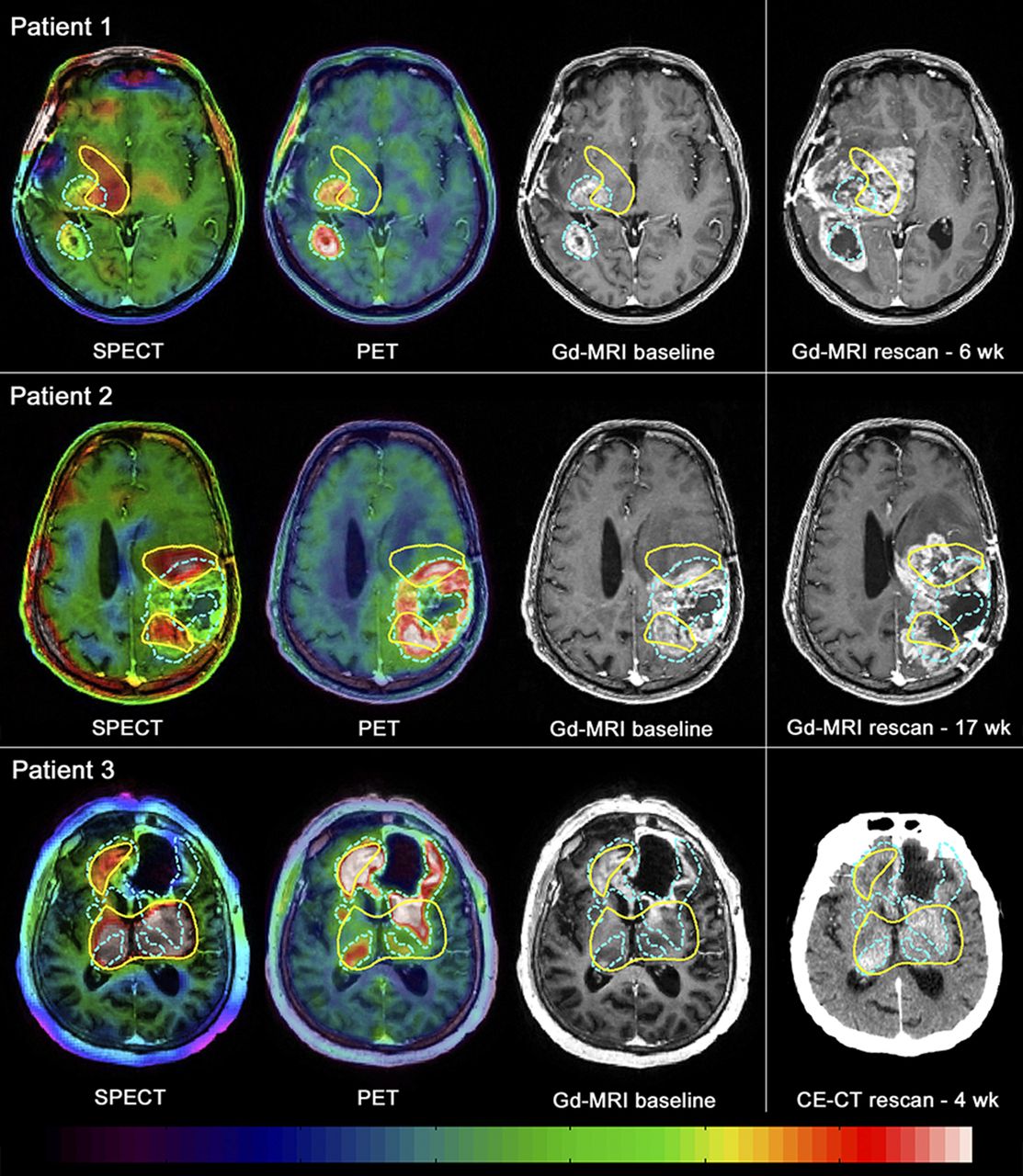
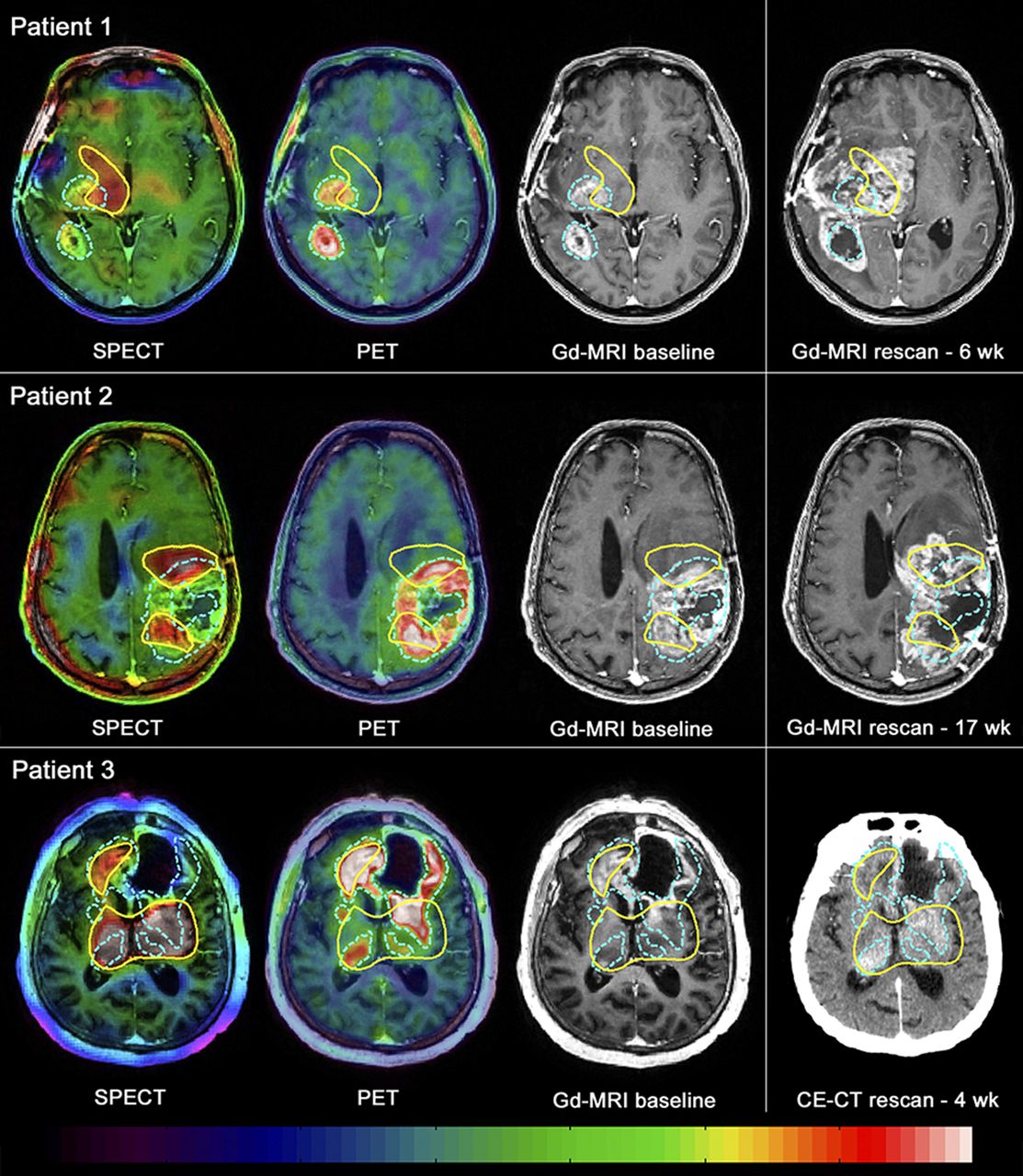
Weighted mean 0- to 150-min 123I-CLINDE SPECT scans, summed 20- to 40-min 18F-FET PET scans, and gadolinium- or contrast-enhanced (CE) structural scans at baseline and at rescanning. Blue VOIs show high 18F-FET tumor uptake, and yellow VOIs high 123I-CLINDE binding. Comparison of baseline and rescanning structural scans reveals that tumor expands predominantly in areas of high 123I-CLINDE binding.
CONCLUSION
These preliminary results from 3 patients with advanced GBM suggest that TSPO imaging is a sensitive and specific marker of GBM and that regional binding predicts areas of active tumor cell proliferation in GBM. Favorable implications can be foreseen for planning surgery and radiotherapy and monitoring the effect of oncologic therapy. 123I-CLINDE SPECT appears to be less susceptible to blood–brain barrier disruption than 18F-FET PET. However, to determine the exact role of TSPO imaging compared with imaging of amino acid transport, further studies are warranted.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was financially supported by the European Union’s Seventh Framework Programme (FP7/2007-2013), the Danish Council for Independent Research, the Research Committee of Rigshospitalet, and Desirée and Niels Yde’s foundation. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We acknowledge Svitlana Olsen and Melanie Ganz-Benjaminsen for technical assistance.
Footnotes
Published online Jul. 16, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication April 8, 2015.
- Accepted for publication July 6, 2015.





{kind=link}
Jump to section
Related Articles
Cited By...
- Prognostic Value of TSPO PET Before Radiotherapy in Newly Diagnosed IDH-Wild-Type Glioblastoma
- The Variability of Translocator Protein Signal in Brain and Blood of Genotyped Healthy Humans Using In Vivo 123I-CLINDE SPECT Imaging: A Test-Retest Study
- Combined PET Imaging of the Inflammatory Tumor Microenvironment Identifies Margins of Unique Radiotracer Uptake