


Abstract
Radionuclide myocardial perfusion imaging (MPI) plays a vital role in the evaluation and management of patients with coronary artery disease. However, because of a steep growth in MPI in the mid 2000s, concerns about inappropriate use of MPI and imaging-related radiation exposure increased. In response, the professional societies developed appropriate-use criteria for MPI. Simultaneously, novel technology, image-reconstruction software for traditional scanners, and dedicated cardiac scanners emerged and facilitated the performance of MPI with low-dose and ultra-low-dose radiotracers. This paper provides a practical approach to performing low-radiation-dose MPI using traditional and novel technologies.
Over the past 40 y, radionuclide myocardial perfusion imaging (MPI) has become a major tool in the noninvasive evaluation of coronary artery disease (CAD). During that time, advances in MPI technology and radiotracers have increased opportunities for improved diagnosis and treatment of patients with CAD. However, there were concerns about its overutilization (1), especially in lower-risk patients, which had coincided with a 6-fold increase in background radiation from medical imaging (2). In response, multiple professional societies have jointly developed appropriate use criteria (AUC) to encourage the appropriate use of MPI (3) and to lower the costs of and radiation dose from MPI. Manufacturers of nuclear medicine equipment have also responded to radiation concerns by introducing technologic advances that allow individualized low-dose protocols while maintaining or enhancing image quality, thereby paving the way for important changes in the practice of MPI. This paper will focus on the vital importance of appropriate patient selection, patient-centered techniques to reduce radiation dose, and practical ways to reduce the lifetime radiation dose for the individual patient as well as for the population of patients being considered for MPI.
THE VITAL IMPORTANCE OF RADIONUCLIDE MPI TO MANAGE CAD
Radionuclide MPI is the most mature cardiovascular imaging technique, with advanced quantitative tools and a vast evidence base in over 100,000 patients (4). Stress MPI with SPECT and PET is widely used to identify the hemodynamic significance of CAD. The greatest strength of MPI, however, is its established value for risk assessment (5). The extent and severity of ischemia and scarring on SPECT and PET MPI are powerful predictors of future cardiovascular events (5). In addition, left ventricular ejection fraction measured on SPECT and PET MPI has well-established incremental value for patient management and risk stratification (5). MPI is cost-effective for the management of CAD. In patients with stable angina pectoris, a noninvasive SPECT MPI–guided management strategy has been shown to be economically superior to an anatomic approach guided by invasive coronary angiography without significant differences in clinical outcomes (6). More recently, radionuclide imaging of myocardial blood flow with PET (and SPECT) has been shown to be an indispensable tool for the evaluation and management of CAD (7,8). Furthermore, several recent advances in PET and SPECT hardware and software facilitate rapid, high-count imaging, and low-dose imaging (9,10). With these unique capabilities, the clinical benefits of an appropriately performed MPI study are indisputable.
THE NEED TO REDUCE RADIATION DOSE FROM MPI
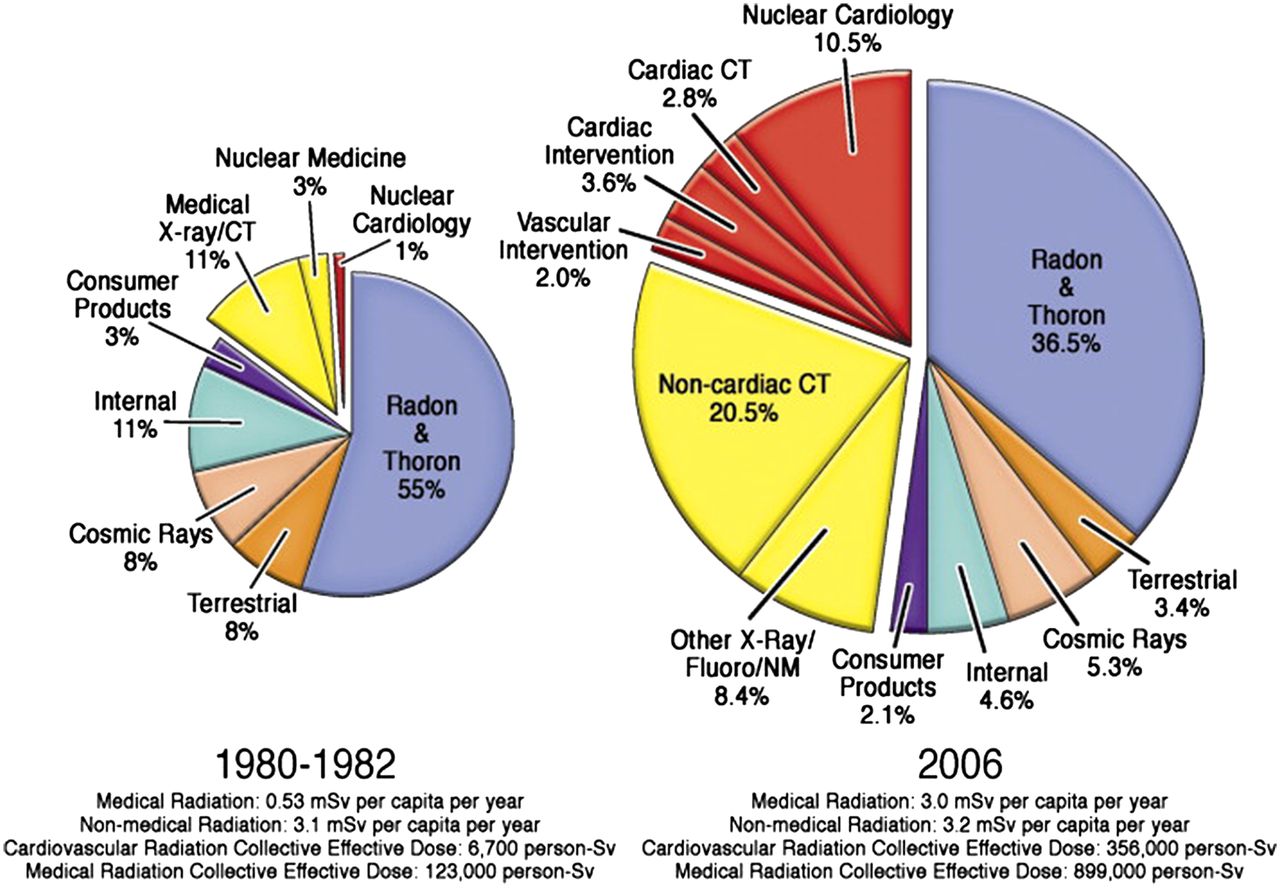
The primary concern about ionizing radiation from MPI relates to the stochastic effects and potential risk of the development of cancer decades later (11). Cancer risk is estimated on the basis of linear downward extrapolation of data from atom bomb survivors to the ranges of medical imaging–related radiation (11). The risk from a medical imaging–related low level of radiation dose is small and difficult to estimate accurately (2,11). However, the overall radiation burden to the U.S. population doubled from the early 1980s to 2006. Although in the early 1980s medical imaging accounted for 15% of the U.S. population’s per capita exposure to ionizing radiation from all sources (0.54 of 3.6 mSv), in 2006 48% of per capita exposure (3 of 6.255 mSv) came from medical imaging (12). Furthermore, the contributions of nuclear cardiology procedures to ionizing radiation increased 10-fold over this period (Fig. 1) (2). A standard rest–stress 99mTc MPI study can be performed with a dose of about 12 mSv (13), compared with an average natural background radiation dose in the United States of 3 mSv. The radiation dose from MPI is declining significantly with new technologies. No data exist to relate an increased risk of cancer from ionizing radiation at these levels (2). But the performance of millions of procedures has raised concerns over increasing radiation dose to the population and the consequent minimal risk of future cancer related to radiation from diagnostic imaging (12).

Increasing radiation burden in United States and contributions from medical imaging. Collective dose from medical imaging increased 6-fold in 2006 compared with early 1980s. (Reprinted with permission of (2).)
Efforts to reduce radiation dose from MPI are important, as long as the concomitantly increased level of image noise does not significantly compromise the ability of physicians to have confidence in making the correct diagnoses based on the images. Also, the risk of performing MPI must be balanced against the risk of missed or delayed diagnosis and treatment from not performing MPI. Radiation dose-reduction strategies and education may promote the safe and effective use of MPI. Informed patients and physicians may be more accepting of MPI, allowing more patients to benefit from this technology. Indeed, a focus on reducing radiation dose from imaging may compel us to more closely scrutinize the need for MPI and reduce the volume of unnecessary tests, thereby reducing lifetime cumulative radiation dose to the patient.
RADIATION DOSE REDUCTION BEFORE MPI: APPROPRIATE USE
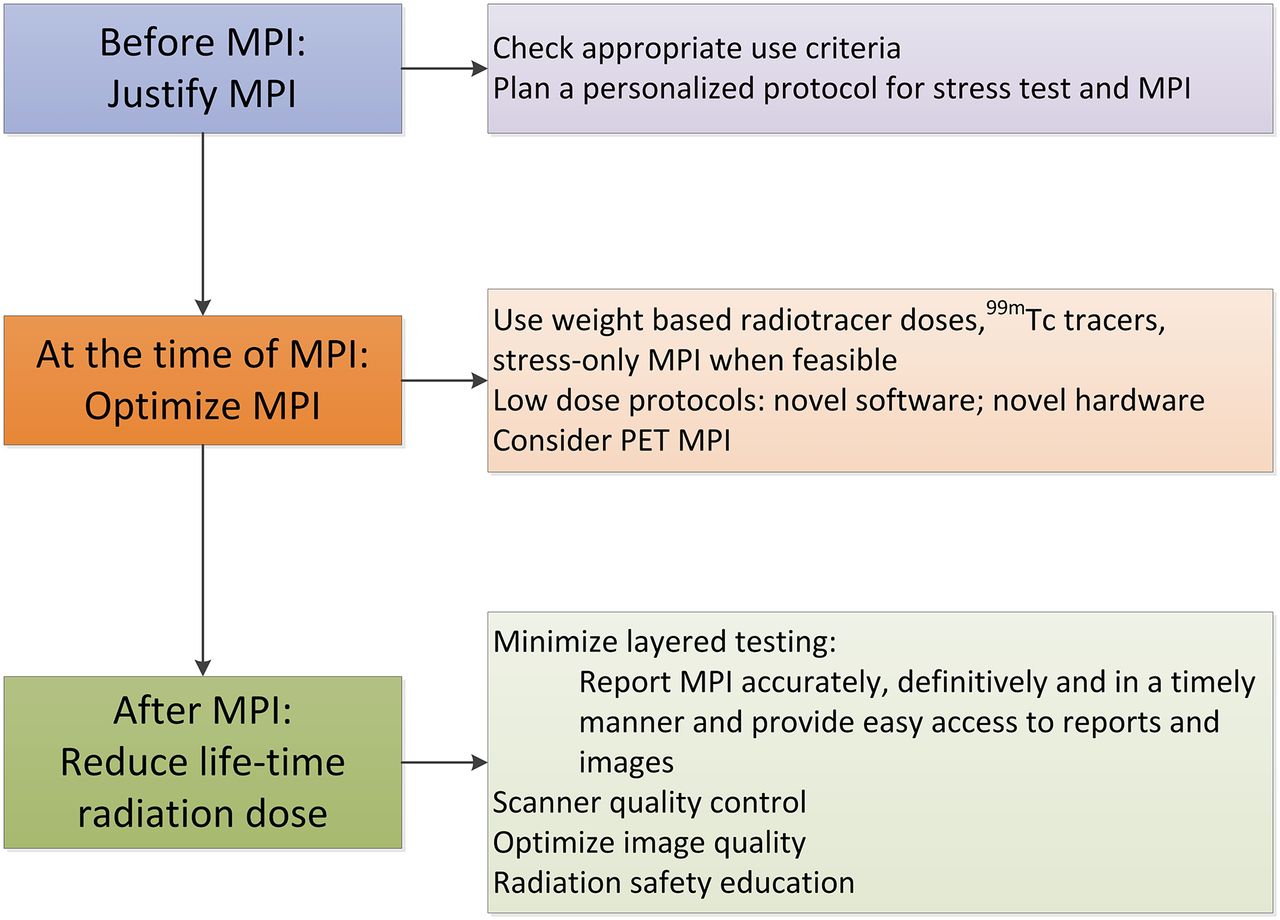
Radiation dose from medical imaging can be reduced before, at the time of, or after completion of the test (Fig. 2). One of the main ways to reduce radiation dose before the performance of a test is to avoid tests that are not needed.
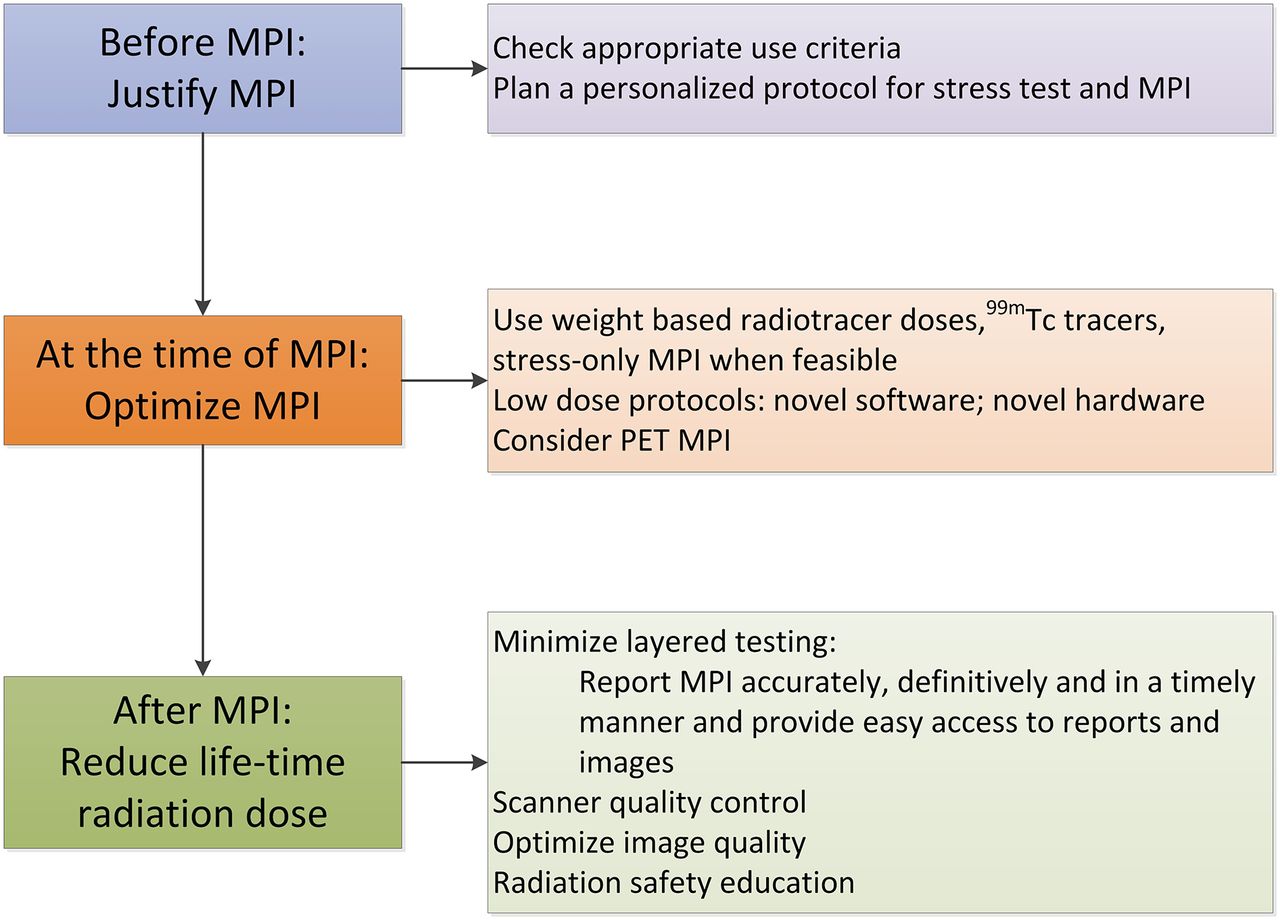
Practical ways to implement reduced-radiation-dose MPI program.
Over the last decade, several professional societies have developed AUC for various diagnostic tests and therapeutic procedures. Appropriate use is defined, by the RAND Corp., as an indication wherein the expected clinical benefit of the test outweighs the risks of the procedure. AUC for cardiac radionuclide imaging, first published in 2005, were most recently updated in 2009 (3). Indications for MPI were categorized on the basis of the median scores of 15 expert panelists. A range of 1–3 is considered rarely appropriate (also previously referred to as inappropriate), 4–7 may be appropriate (also previously referred to as uncertain), and 7–9 appropriate. Of a list of 67 indications for MPI, 9 were considered uncertain, 25 inappropriate, and the rest appropriate (3). Of note, the radionuclide AUC did not distinguish the indications for SPECT from PET MPI; the expert rating applied equally to SPECT and PET. The value of AUC in reducing radiation dose is obtained from avoiding the tests that may be rarely appropriate. When imaging is appropriate, the benefit of an optimal test generally outweighs its potential risk. The appropriateness of any given indication for MPI can be checked online using a radionuclide AUC app (https://itunes.apple.com/us/app/appropriate-use-criteria-auc/id391068250?mt = 8; Astellas Pharma US).
The AUC methodology has certain limitations. AUC were developed on the basis of expert opinion and expert interpretation of existing clinical and trial evidence, whereas guidelines are developed on the basis of clinical trial evidence. They do not include a list of all possible clinical scenarios. They are not directly based on the frequency with which the test reclassifies the extent or severity of a patient’s disease or directly affects the choice of treatment. Also, they do not take into account the costs of the test, cost effectiveness, relative performance of one test versus alternative tests, ionizing radiation, or the impact of repeat testing or layered testing.
Frequency of Appropriate MPI per AUC
The frequency with which MPI is used appropriately may vary from region to region and in different practices. In one study (14), from 6 sites in the UnitedHealthcare system, most of the MPI studies were performed for appropriate indications (85.6%) and only 14.4% were performed for inappropriate indications (rarely appropriate). Inappropriate studies (or rarely appropriate) were more common in asymptomatic individuals, women, and preoperative patients (14). The American Society of Nuclear Cardiology (ASNC) incorporated some of these indications into the Choosing Wisely campaign to reduce inappropriate use of MPI. Choosing Wisely is an effort by the American Board of Internal Medicine partnering with Consumer Reports and in collaboration with several medical societies (including the Society of Nuclear Medicine and Molecular Imaging [SNMMI], ASNC, and others), developed to curb the growth in the use of unnecessary imaging tests. It uses the philosophy of “5 things that physicians and patients should question.” Table 1 lists the SNMMI and ASNC Choosing Wisely points related to MPI (15,16).
Methods to Increase the Appropriate Use of MPI
Appropriate use of MPI can be increased only by improving knowledge about AUC for both referring provider and imaging provider. Unfortunately, educational efforts to reduce the rates of rarely appropriate studies have had mixed results. Initial short-term declines in the proportion of rarely appropriate tests ordered were not sustained over the long term (17).
The appropriateness of MPI can be tracked at the time of order entry using one of several online tools. The American College of Cardiology FOCUS (Formation of Optimal Cardiovascular Use Strategies) is a web-based quality improvement tool developed to track and improve the appropriate use of MPI. In a preliminary analysis, the proportion of rarely appropriate indications decreased from 10% to 5% for the sites participating in the FOCUS PIM (practice improvement module) (18). Also, decision support tools (DST), incorporated into physician electronic-order-entry systems, can guide the referring physicians through steps to ensure appropriate use of the test. One such system, the AUC-DST, showed that the frequency of appropriate tests increased from 49% to 61% and the frequency of rarely appropriate tests decreased from 22% to 6% 8 mo after the implementation of the AUC-DST (19). Ideally, the referring physician should ensure the appropriateness of the test at the time of order entry using clinical DST. Indeed, it has been mandated by law that documentation of AUC using DST for ordering advanced imaging tests (including SPECT and PET MPI) will, by January 2017, be a prerequisite to receiving payment for imaging services for Medicare patients (20,21). This measure likely will increase the rate of appropriate studies.
Because cardiovascular imaging has become fairly complex, choosing a suitable test from the many possible tests can be challenging for ordering physicians who may not be imaging experts. In complex cases, a discussion between the referring physicians and imaging physicians, who have expertise in multimodality imaging, can ensure that the most appropriate test is selected for a given indication and patient. In some cases, the most appropriate test may be a nonimaging exercise treadmill test, stress echocardiography, or MR imaging–based MPI. This discussion is facilitated by a systematic review (a “protocol plan”) of the patient’s history (Table 2), at least 1 d before the MPI, to change the test if needed and to contact the patient. Imaging laboratory personnel, fellows in training, or staff members experienced in imaging can prepare a protocol plan for the studies.
Steps to Create Protocol Plan for MPI
The appropriate use of MPI is expected eventually to reduce cumulative lifetime radiation exposure from imaging of patients with CAD, although this has not yet been studied directly on a large scale.
RADIATION DOSE REDUCTION DURING THE TEST: OPTIMIZE MPI
SNMMI and ASNC recommend a patient-centered imaging approach taking into account radiation dose. ASNC issued an information statement on reducing radiation exposure in MPI and recommended several methods that, if used appropriately, can reduce radiation dose to 9 mSv or less in 50% of patients referred for SPECT or PET MPI studies (22). Selection of protocols for MPI should also take into account the clinical question, the image quality, potential risks incurred from future testing stemming from the results of MPI and from radiation, costs, patient convenience, and assurances that the patient and staff are receiving the lowest possible radiotracer dose (23). However, image quality should not be significantly jeopardized by dose reduction. Patient characteristics such as body habitus, claustrophobia, ability to lie supine for imaging, and stress modality are also important considerations. Appropriate selection of radiotracer, the use of novel imaging protocols, and, when available, the use of novel reconstruction methods, hardware, collimators, and software are critical to reducing patient radiation dose.
Selection of Radiotracers
Estimated whole-body effective radiation dose (averaged over various organs and averaged for men and women) is directly related to the half-life of the radiotracer and dose of radiotracer administered (Table 3).
Estimation of Effective Radiation Dose from Various Myocardial Perfusion Radiotracers (13)
For SPECT MPI, 99mTc agents are preferred over 201Tl because of their shorter half-life, significantly lower effective dose, and superior image quality. For PET MPI, 82Rb and 13N-ammonia, when available, offer an even greater reduction in radiation dose compared with 99mTc SPECT. Radiation dose from PET MPI can be further lowered with imaging in 3-dimensional (3D) mode, as this mode offers much higher-count imaging and permits half-dose imaging, which may be especially useful in children. The mean estimated whole-body effective dose from SPECT and PET perfusion tracers is listed in Table 3.
For SPECT and PET MPI, a weight- or body mass index–based adjusted radiotracer dose may be better than a fixed dose for all, to balance low radiation dose with optimal image quality (24). Indeed, Marcassa et al. (25) recently documented a 58% radiation dose savings to patients, and a 50% dose reduction to cardiologists performing the test, by switching from a fixed-dose protocol to a weight-based 99mTc dosing protocol and finally to low-dose MPI using novel software-based reconstructions. A sample table of weight-based 99mTc dosing and estimated whole-body effective dose is included in Supplemental Table 1. Radiation dose from MPI can be additionally reduced using any of the protocols and technologies described below.
Stress-First or Stress-Only Imaging Protocols for Reduced-Dose MPI
Stress-first or stress-only MPI, as well as low-radiotracer-dose protocols (half-dose or less than half-dose) using novel scanners, collimators, or software, can significantly reduce radiation dose from SPECT MPI compared with standard-dose rest–stress MPI protocols. Stress-first SPECT imaging has several other advantages (Supplemental Table 2), and although supported by the imaging societies for over a decade now, the stress-first protocol has not been widely implemented because of several challenges (Supplemental Table 2). But a decline in the frequency of abnormal scan results from 41% in 1991 to 8.7% in 2009 (26) combined with the soaring costs of medical imaging (>6 million SPECT MPI studies per year) (2) makes a strong case for stress-only imaging.
A growing body of literature supports the utility of stress-first SPECT imaging (24,27–34). If the stress MPI results are normal, the rest scan can be avoided, with significant savings in cost, time, and radiotracer exposure to the patient (35% dose reduction) and to the laboratory staff (40% dose reduction) (35). Stress-first and stress-only PET MPI have not been as widely studied as stress-first and stress-only SPECT MPI.
Implementation of Stress-First MPI
A successful implementation of stress-only or stress-first protocols requires careful screening of patients ahead of the test. Experienced imaging physicians must be available to finalize the MPI report, definitively and unequivocally, before discharging the patient from the laboratory. A stress-only study is considered to have normal results when the myocardial perfusion is homogeneous and the ejection fraction and left ventricular volumes are normal during maximal stress, with no ischemic electrocardiogram changes (27). However, if the stress-first results are not normal, a rest scan can be completed on the same day with 3 times the stress radiotracer dose.
Patient Selection for Stress-First MPI
Patient selection is critical for a successful stress-first program. Patients without a prior history of myocardial infarction and an intermediate pretest likelihood of CAD are well suited for stress-first MPI. The pretest likelihood of CAD is calculated using the age, sex, and chest-pain characteristics (Supplemental Table 3). A stress-first imaging protocol is feasible with either exercise or pharmacologic stress and may be used in diabetic patients (27) as well as in morbidly obese patients (30). Patients with a low pretest likelihood of CAD, however, may be considered for treadmill testing alone without imaging. Even among women with an intermediate pretest likelihood of CAD and able to exercise on a treadmill, the WOMEN study (What is the Optimal Method for Ischemia Evaluation in Women?) demonstrated that an initial diagnostic strategy of exercise treadmill testing with imaging, when compared with exercise treadmill testing alone, did not provide any incremental diagnostic or prognostic benefit and reduced downstream costs (36).
Attenuation Correction for Stress-First SPECT MPI
Accurate identification and correction of attenuation artifacts is important in stress-first imaging algorithms to avoid interpretation of attenuation artifacts as real perfusion defects. Although gated SPECT is not helpful in identifying attenuation artifacts (because ischemic wall motion abnormalities typically resolve by the time of image acquisition), prone imaging can be used for troubleshooting fixed inferior-wall perfusion defects. Attenuation correction, however, is the most direct and effective method for correcting attenuation artifacts.
Attenuation correction using radionuclide or CT-based transmission scans significantly reduced the need for rest MPI imaging in as many as 37%–48% of patients scheduled for stress-first SPECT imaging (31,37). Indeed, the primary application of cardiac CT with SPECT and PET MPI is for attenuation correction, with a radiation dose ranging from 0.3 to 1.3 mSv with appropriate cardiac CT dose reduction methods (Supplemental Table 4) (13). The use of attenuation-corrected MPI with gated SPECT is essential for the best clinical application of stress-first or stress-only imaging.
Prognostic Value of Stress-Only Imaging
The excellent prognostic value of a normal stress-only SPECT result from conventional scanners is well established (Supplemental Table 5) (27). In a pooled analysis including 10,438 patients with stress-only MPI, a normal result was associated with an annual event rate of 0.7%, with a relative risk comparable to a normal rest–stress MPI result (5). This area has not been examined for PET MPI.
Novel Reconstruction Software, Scanners, and Collimators for MPI
Several recent advances in cardiac SPECT software, novel semiconductor detector solid-state SPECT scanners (cadmium zinc telluride [Spectrum Dynamics or GE Healthcare] or thallium-activated cesium iodide [CsI(Tl)] [Digirad]), and novel collimator design (38) have substantially improved image resolution and lowered radiation dose for MPI (10,39).
Novel iterative reconstruction methods (Astonish [Phillips], wide-beam reconstruction [UltraSPECT Inc.], Flash 3D [Siemens], n-SPEED [Digirad], and Evolution [GE Healthcare]) with resolution recovery and noise reduction provide higher image contrast (with sharper defects and borders) and significantly improve image quality, particularly for low-count imaging studies from half- and quarter-dose radiotracer protocols (40). Despite excellent image quality with shorter imaging times (41–44), not many studies have prospectively evaluated half-dose MPI with novel software. DePuey et al. (42) used half-dose 99mTc MPI and showed that low-dose MPI with conventional scanners using novel software (wide-beam reconstruction) provides good to excellent image quality in 93% of patients. The value of the novel software is that existing scanners can be upgraded with advanced software to reduce radiation dose, a much smaller capital investment than buying a new scanner.
Novel solid-state SPECT scanners offer a severalfold increased count sensitivity compared with the conventional NaI(Tl) scanners because they use cardiofocal imaging and either large parallel-hole or multiple-pinhole collimators (9,10,45). Also, attenuation correction is available for some of these scanners (Digirad and GE Healthcare). Iterative-reconstruction protocols combined with resolution recovery and noise reduction are standard for the novel scanners. Each of these enhancements enables low-dose and ultra-low-dose MPI.
Because of high count sensitivity, the novel scanners offer significant flexibility with imaging protocols. The initial focus of the novel high-sensitivity scanners was on rapid imaging (2- to 4-min imaging times), which is well suited for imaging patients with multiple comorbidities who may not otherwise tolerate longer acquisition times. However, low-radiation-dose, high-quality imaging is the current focus of the novel scanners (Table 4). Some protocols use a half-dose or less (single-day, 111–185 MBq [3–5 mCi]/333–555 MBq [9–15 mCi] of 99mTc) with imaging times of 8 and 6 min or longer for count-based imaging. The effective radiation dose from stress-only protocols with novel scanners is less than 2 mSv. However, enthusiasm for further dose reduction is tempered by the longer acquisition times, which may increase the likelihood of patient motion, especially if the acquisition duration is 7 min or more.
Radiation Dose from Low-Dose Protocols for Novel SPECT Scanners
In multicenter studies, rapid scanning with dedicated cardiac SPECT scanners provided comparable or superior image quality, with a much shorter scan duration than for standard-time scanning with conventional scanners (46,47). However, only one study directly compared low-dose dedicated cardiac SPECT scanning with conventional-dose scanning in the same patients, and one other study simulated low-radiation-dose rest and stress imaging. Einstein et al. (48) directly compared rest ultra-low-dose 99mTc dedicated cardiac SPECT imaging (133.96 MBq/3.62 mCi) with standard-dose conventional SPECT in 110 patients (mean body mass index, 26.1 ± 2.8 kg/m2; range, 17.1–30.9 kg/m2; mean acquisition time range, 9.7–15.2 min) from 3 sites and showed comparable image quality with a very low radiation dose when using the dedicated cardiac SPECT scanner (1.15 ± 0.24 mSv). Nakazato et al. (49) recently simulated low-dose rest and stress SPECT MPI in 79 patients (mean body mass index, 30.0 ± 6.6; range, 20.2–54.0 kg/m2) and showed that image quality is adequate even with very low-count images (∼1 million) and comparable to standard full-count images. Finally, low-dose 99mTc MPI with dedicated cardiac scanners is accurate for detecting obstructive CAD on invasive angiography (e.g., in one study visual analysis sensitivity was 92%, specificity 56%, and normalcy 98%) (50–52). Although the novel scanners offer significant advantages and high-quality imaging with a low radiation dose, they are expensive, at this time, with clinical imaging applications limited to cardiac imaging. An algorithm for reduced-dose SPECT MPI is shown in Figure 3.
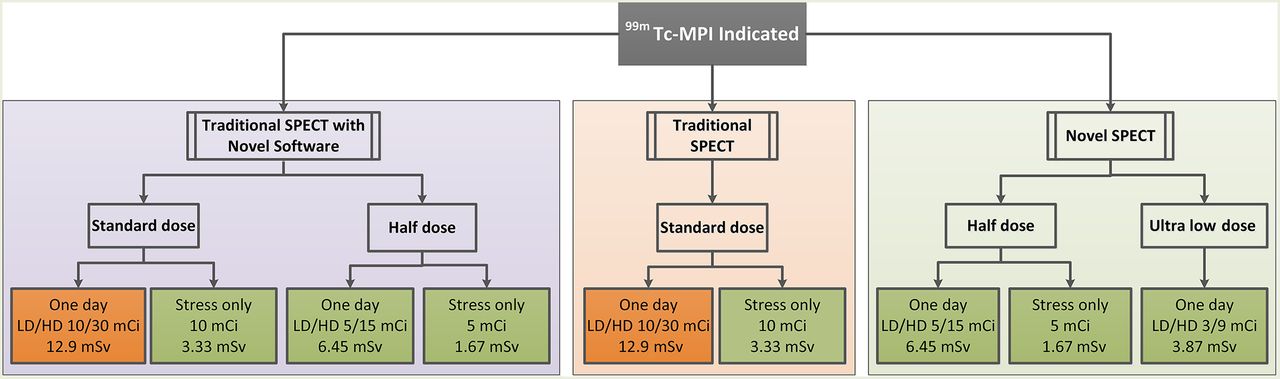
Patient-centered protocols for low-radiation-dose MPI: traditional SPECT (orange), traditional SPECT with novel software (purple), and novel SPECT scanners (green). Most MPI procedures that use novel protocols or novel technologies provide <9-mSv radiation dose from rest–stress 99mTc protocols. To achieve 50% of laboratory volume with <9-mSv dose, practices can implement several of the above options into their practice. LD = low dose; HD = high dose; 1 mCi = 37 MBq.
Dose Reduction with PET
Most current-generation PET scanners image in 3D mode and are equipped with advanced hardware and software capabilities for high-resolution, low-dose imaging (9). With time-of-flight, high-definition iterative reconstruction and motion-frozen imaging, an effective spatial resolution of as low as 2 mm can be achieved with PET MPI (10). When combined with the low dose from PET tracers, PET MPI offers a significantly lower radiation dose than SPECT MPI. Stress-only imaging and low-dose CT imaging are additional dose reduction options for PET MPI but have not been as widely studied or implemented.
Stress-only PET MPI in 3D mode with myocardial blood flow assessment can be performed with less than a 1-mSv radiation dose. Typical adult patients referred for PET MPI, however, are high-risk patients and are not always suited to stress-only imaging. In addition, coronary flow reserve (CFR), an emerging risk marker of coronary vascular dysfunction, cannot be estimated with stress-only imaging. However, one recent study using 15O-water MPI suggested that hyperemic myocardial blood flow may be more accurate than CFR for the diagnosis of obstructive epicardial CAD (accuracy, 86% vs. 78%; P < 0.01) (53,54). On the other hand, another study suggested that although CFR and stress myocardial blood flow with 82Rb provide powerful risk stratification, estimates of CFR may be more robust and less variable than stress myocardial blood flow (54). If stress myocardial blood flow is confirmed to be superior to CFR with the clinical PET perfusion tracers, stress-only PET MPI may be more widely implemented. Combining stress-only MPI with low-dose CT coronary angiography (55) (if CT results are abnormal) or with calcium score (56) can identify significant CAD that may warrant aggressive medical therapy. Despite the significant advantages of superior image quality, better detection of CAD, and low-radiation-dose imaging, PET MPI and PET/CT MPI are not widely available, remain expensive, and are predominantly limited to pharmacologic stress (because exercise stress can be challenging with PET).
RADIATION DOSE REDUCTION AFTER THE TEST
Finally, several steps can be taken after completion of MPI to minimize the lifetime radiation dose. First, an accurate, clear, and unambiguous report and timely communication to the referring physician will reduce repeat, layered testing. Next, the MPI report should accurately list the administered radiotracer dose; soon, estimates of lifetime radiation exposure from medical imaging may become a requirement on the report. Periodic quality reviews of the laboratory for doses administered for MPI, image quality with low-dose MPI, and evaluation of the number of MPI procedures below the ASNC-recommended dose parameters of less than 9 mSv are suggested (22). Further, quality control of the scanners will optimize image quality and facilitate low-radiation-dose MPI. Last, staff radiation exposure should be followed according to ALARA (as low as reasonably achievable) principles, including rotation of duties for nuclear medicine technologists to avoid high radiation exposure to any individual technologist. A recent scientific statement on approaches to enhancing radiation safety in cardiovascular imaging (57) highlighted the need to educate referring physicians and health care providers on performing low-dose medical imaging and provided a list of online resources for radiation dose reduction from the various societies.
CONCLUSION
The rising barriers to radionuclide MPI from ionizing radiation and high costs mandate a change in the traditional practice of nuclear cardiology. The time to change is now. Novel imaging protocols and powerful imaging technologies have emerged to facilitate low-dose high-quality MPI. A secondary benefit of this change is that in the current challenging fiscal environment, medical facilities, practitioners, and practices can differentiate themselves by producing superior image quality at a faster pace and at a low dose. State-of-the-art nuclear cardiology practice requires embracing best practices for appropriate patient selection, patient-centered imaging protocols, use of novel protocols for traditional scanners, and adoption of laboratory practices to reduce lifetime radiation exposure for patients and staff members. The move to a lower radiation dose for MPI brings nuclear cardiology into the 21st century, spreading new best practices across the country and the world.
Footnotes
Published online Mar. 12, 2015.
Learning Objectives: On successful completion of this activity, participants should be able to (1) describe the application of appropriate use criteria for SPECT and PET myocardial perfusion imaging, (2) apply stress-only/stress-first myocardial perfusion imaging in clinical practice, and (3) list methods to perform low-radiation-dose myocardial perfusion imaging using traditional and novel technology.
Financial Disclosure: Dr. Dorbala was supported by NIH-NHLBI K23HL092299, has received a research grant from Astellas Pharma (unrelated to this work), and has investment interest with General Electric. The authors of this article have indicated no other relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, SAM, and other credit types, participants can access this activity through the SNMMI website (http://www.snmmilearningcenter.org) through April 2018.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication January 2, 2015.
- Accepted for publication February 27, 2015.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Worldwide Diagnostic Reference Levels for Single-Photon Emission Computed Tomography Myocardial Perfusion Imaging: Findings From INCAPS
- Using radiation safely in cardiology: what imagers need to know
- Simplified approach to stress-first nuclear myocardial perfusion imaging: implementation of Choosing Wisely recommendations
- Effective Dose in Nuclear Medicine Studies and SPECT/CT: Dosimetry Survey Across Quebec Province
- The impact of IUGR on pancreatic islet development and {beta}-cell function
- Trials of Quality Improvement in Imaging