


Abstract
PET/CT is a valuable tool to detect lymph node (LN) metastases in patients with biochemical failure after primary treatment for prostate cancer (PCa). The aim was to assess the predictive role of imaging parameters derived by 11C-choline PET/CT on survival outcomes—overall survival, locoregional relapse-free survival, clinical relapse-free survival (cRFS), and biochemical relapse-free survival (bRFS)—in patients treated with helical tomotherapy (HTT) for LN recurrence. Methods: This retrospective study included 68 patients affected by PCa (mean age, 68 y; age range, 51–81 y) with biochemical recurrence after primary treatment (median prostate-specific antigen values obtained at the time of PET/CT scan, 2.42 ng/mL; range, 0.61–27.56 ng/mL) who underwent 11C-choline PET/CT from January 2005 to January 2013 and were treated with HTT in correspondence of the pathologic choline LN uptake. PET-derived parameters, including maximum/mean standardized uptake value (SUVmax and SUVmean, respectively) and metabolic tumor volume (MTV) with a threshold of 40%, 50%, and 60% were calculated. The best cutoff values of PET-derived parameters discriminating between patients with and without relapse, after treatment guided by PET, were assessed by receiver-operating-characteristic (ROC) curve analysis. Univariate and multivariate Cox regression analysis including the most predictive PET-derived parameters and survival outcomes were performed. Results: The median follow-up was 20 mo (mean, 26 mo; range, 3–97 mo). 11C-choline PET/CT showed pathologic LN uptake in 4 patients at the pelvic level, in 5 at the abdominal level, in 13 at both the pelvic and the abdominal level, and in 46 at the abdominal or pelvic or other sites. The 2-y overall survival, locoregional relapse-free survival, cRFS, and bRFS were 87%, 91%, 51%, and 40%, respectively. On the basis of ROC curves, the most discriminative cutoff value for MTV values was an MTV threshold of 60% (MTV60) of greater than 0.64 cm3. No significant cutoff values were found for SUVmax or SUVmean at univariate analysis, whereas MTV60 was confirmed as an independent predictor in multivariate analysis and significantly correlated with bRFS and cRFS. MTV60 and extrapelvic disease well predict the risk of cRFS. Conclusion: 11C-choline PET/CT performed as a guide for HTT on LN recurrence is predictive of survival. In particular, MTV60 and extrapelvic disease were the best predictors of tumor response for bRFS and cRFS in PCa patients with LN recurrence after primary treatment. This information may be useful in emerging treatment strategies.
Approximately 70% of patients treated with radical prostatectomy for prostate cancer (PCa) experience long-term biochemical recurrence; however, it is known that biochemical recurrence does not necessarily change into cancer-specific death (1–4). The demand for and type of salvage treatment are strictly dependent on the site of cancer recurrence (local vs. distant), concomitant diseases, and overall life expectancy (5–7). Lymph node (LN) recurrence in patients with PCa is considered an unfavorable prognostic factor, and androgen-deprivation therapy (ADT) is commonly administered as standard treatment (5). Although ADT delays PCa progression, it is associated with several side effects with a negative impact on patients’ quality of life (8). Moreover, there are no definitive results showing a better overall survival (OS) in patients immediately treated with ADT and in those treated with deferred ADT. Therefore, the European Association of Urology suggests an active surveillance for asymptomatic patients with metastatic PCa (5,9).
The traditional imaging modalities, such as bone scintigraphy and CT, are lacking in sufficient sensitivity for the detection of small-volume metastatic disease in patients with low prostate-specific antigen (PSA) levels. Therefore, there is no definitive clinical recommendation regarding the use of these imaging modalities to assess metastatic disease when PSA levels are below 10 ng/mL (10). 11C-choline PET/CT might be a good candidate for the identification of low-volume metastases, with a reported pooled sensitivity and specificity of 85% and 88%, respectively, on a per-patient basis (12 studies, 1,055 patients) in a recurrent setting (11).
It has been described that 11C-choline PET/CT–guided salvage LN therapy, either by surgery, surgery followed by adjuvant radiotherapy (RT), or RT alone, may be an effective strategy with long-term disease control and a possible curative intent (11–14). Recently, our group reported that 11C-choline PET/CT–guided hypofractionated helical tomotherapy (HTT) with simultaneous integrated boost (SIB) on positive LNs detected by 11C-choline PET/CT is well tolerated and associated with a high early biochemical response rate (15). Although they require a final validation in randomized controlled trials, image-guided tailored treatments are promising, and the availability of an imaging modality enabling the prediction of treatment efficacy would be of relevant clinical impact, helping in proper patient management (16,17).
The role of 11C-choline PET/CT to predict survival outcomes in patients treated with radical prostatectomy who develop biochemical failure has been recently reported, thus suggesting its possible role for prognostic stratification of PCa patients (18,19).
The aim of the present study was to assess the predictive role of imaging parameters derived by 11C-choline PET/CT, such as standardized uptake value (SUV) and metabolic tumor volume (MTV), in a population of patients previously treated with choline PET/CT–guided HTT SIB for LN recurrence in terms of 2-y OS, locoregional relapse-free survival (lRFS), clinical relapse-free survival (cRFS), and biochemical relapse-free survival (bRFS).
MATERIALS AND METHODS
Patient Population
This retrospective study included 68 consecutive patients (mean age, 68 y; age range, 51–81 y) with PCa relapse after primary treatment, referred to San Raffaele Scientific Institute for 11C-choline PET/CT from January 2005 to January 2013 and for HTT with SIB on positive 11C-choline PET/CT LN recurrence (from February 2005 to March 2013), as described in our previous study (15). All patients signed an informed consent form, which included permission for anonymous publication of disease-related information. This single-institution study was approved by the ethical committee of the San Raffaele Scientific Institute.
Eligibility criteria to be included in the present study were the availability of PET-derived parameters at positive LN level; availability of clinical, biochemical, and pathologic data of interest for multivariate Cox regression analysis and follow-up information regarding the survival status; and written informed consent for anonymous publication of disease-related information according to the Declaration of Helsinki. Patients with distant bone metastases detected either by 11C-choline PET/CT or by other imaging modalities, such as bone scintigraphy or CT, were excluded. The presence of local recurrence and concomitant HTT on prostatic fossa were not considered exclusion criteria. Patient characteristics including clinical, biochemical, and pathologic features are summarized in Table 1.
Patient Characteristics (n = 68)
Imaging Analysis and 11C-Choline PET/CT–Derived Parameters
11C-choline PET/CT studies have been performed and qualitatively analyzed as previously described (15). In particular, for LN, focal choline uptake was considered pathologic when it was higher than background regardless of LN size. In addition to qualitative evaluation, semiquantitative 11C-choline PET/CT image analysis was performed, using an Advantage WorkStation (GE Healthcare), which allows the visualization of choline PET, CT, and PET/CT-fused sections in transaxial, coronal, and sagittal planes.
11C-choline PET/CT studies considered for the analyses were performed before the beginning of HTT, with a mean time from 11C-choline PET/CT to HTT of 2 mo (range, 0–10 mo).
Regions of interest for the most active LN lesion were manually drawn on transaxial PET images to obtain 3-dimensional volumetric measurements of maximum SUV and mean SUV (SUVmax and SUVmean, respectively). MTV was obtained as the sum in cubic centimeters (cm3) of the tumor volume of each single choline PET/CT–positive lesion using a semiautomated contouring program, setting different thresholds: 40% (MTV40), 50% (MTV50), and 60% (MTV60) (20). Those different MTV thresholds were considered for the assessment of their possible predictive role.
Treatment and Follow-up
As previously reported, the treatment was delivered with hypofractionated HTT (Tomotherapy Hi-Art II) on the entire LN chain (15). In particular, in the present selected population, positive pelvic or abdominal LNs showed by 11C-choline PET/CT images were treated with a median dose of 65.8 Gy (range, 50.0–74.2 Gy) in 28 fractions.
To evaluate the biochemical response in the present series of patients, the serum PSA value was recorded at the first follow-up, 3 mo after the end of HTT (PSA1), and compared with the values obtained at the time of PET/CT scan (PSA0). The biochemical response was classified as complete response (reduction of >50% of the initial PSA0 value), partial response (reduction of between 10% and 50% of the initial PSA0 value), stable disease (within 10% of initial values), or progression of disease (increase in serum PSA value of >10%) (15,21).
OS, lRFS, cRFS, and bRFS were investigated by number of events as dead/relapse. OS was defined as the time between the end of HTT and patients’ last available follow-up. Survival outcomes (lRFS, cRFS, and bRFS) were defined on 11C-choline PET/CT performed 3 mo after HTT and repeated subsequently if the patient presented a rise in PSA. In particular, they were measured from the end of HTT to the date of progression, when progression occurred during follow-up. The average clinical and instrumental follow-up after the end of HTT was 26 mo, with a median of 20 mo (range, 3–97 mo).
Statistical Analysis
SPSS software (version 17.0; SPSS Inc.) and MedCalc software (version 12.1.4; MedCalc Software) were used for the analysis. Regarding PET-derived parameters, the best cutoff values discriminating between patients with and without relapse were assessed by receiver-operating-characteristic (ROC) curves, and a P value of less than 0.05 was considered statistically significant. The prognostic value of 11C-choline PET/CT parameters has been assessed. Univariate Cox regression analysis was used to test the correlation between PET-derived parameters (SUVmax and SUVmean and MTV40, MTV50, and MTV60) and survival outcomes (OS, lRFS, cRFS, and bRFS). Other potentially relevant clinical variables were also considered and tested, including PSA, ADT during/after HTT, duration of ADT before HTT, planning target volume, and site of LN recurrence (pelvic vs. extrapelvic). Then, a backward multivariate Cox regression analysis (with a threshold P value of 0.10) was performed for each of the considered endpoints including the variables with a P value of less than 0.10 at univariate analysis. Hazard ratios (HRs) were considered to express the strength of the association between each variable and the risk of relapse.
An internal validation of the resulting Cox models was performed by a 5-fold cross-validation procedure: the areas under the curve (AUCs) (and their 95% confidence intervals [CIs]) referring to the original models and to the corresponding models corrected for the cross-validation were reported.
RESULTS
PET-Derived Parameters and Predictive Cutoff Value
Positive LN lesions on 11C-choline PET/CT referring to HTT as well as median, mean, and range of all PET-derived parameters are shown in Table 2. In particular, 11C-choline PET/CT showed pathologic LN uptake at the pelvic level only in 4 of 68 patients and at the abdominal or pelvic level or other sites in 64 of 68 patients (Fig. 1).
Sites of 11C-Choline PET/CT–Positive Lesions and PET-Derived Parameters
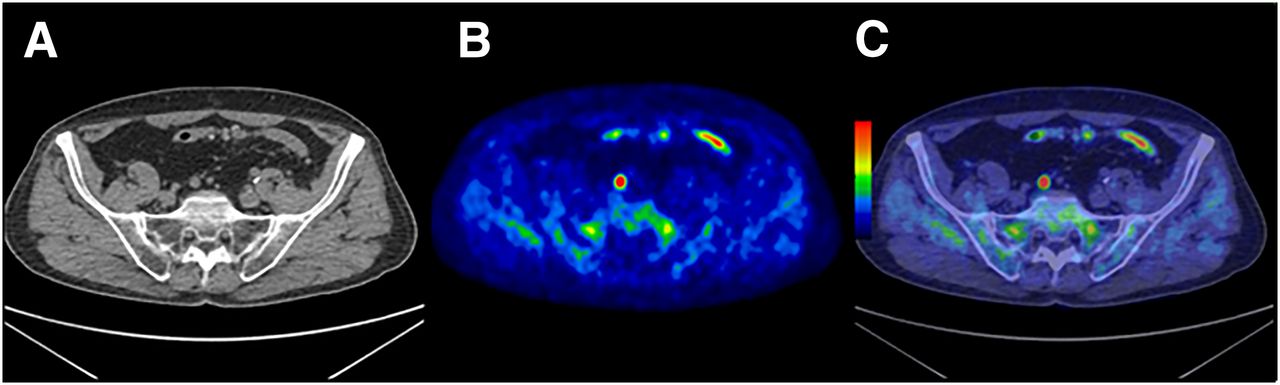
A 69-y-old man with PCa recurrence after primary treatment (Gleason score 4+4, pathologic stage at radical prostatectomy pT3apN0) underwent 11C-choline PET/CT for restaging purposes (PSA value at 11C-choline PET/CT, 1.70 ng/mL). Pathologic choline uptake was observed in presacral region on transaxial PET and PET/CT images (B–C), corresponding to presacral lymph node on transaxial CT image (A). SUVmax, SUVmean, and MTV60 were 13.80, 7.30, and 0.20 cm3, respectively. After HTT guided by 11C-choline PET/CT, PSA value was 0.03 ng/mL and patient has shown a complete response (98%). Patient was still alive at last follow-up of 10 mo.
The best predictive cutoff values for SUVmax and SUVmean and MTV40, MTV50, and MTV60 thresholds for cRFS and bRFS and their corresponding AUCs are shown in Table 3. No association with survival outcomes was observed for SUVmax and SUVmean. Because the discriminative power of the MTV cutoff values was quite similar, we decided to include in the subsequent Cox analysis only MTV60 greater than 0.64 cm3, which was the most discriminative value based on AUC.
PET-Derived Parameter Cutoff Values
Biochemical Response
When changes between PSA0 (mean, 4.54 ng/mL; range, 0.61–27.56 ng/mL) and PSA1 (mean, 1.82 ng/mL; range, 0.00–33.14 ng/mL) were considered, a complete response was observed in 55 of 68 (81%) patients, a partial response in 8 of 68 (12%) patients, and a disease progression in 5 of 68 (7%) patients. No patients in the present series presented a stable disease.
Survival Outcomes
The median OS was 22 mo, with a mean value of 29 mo (range, 4–98 mo). Fifty-eight of 68 (85%) patients were alive during the study period, 46 of 58 (79%) of whom were followed-up for more than 1 y and 29 of 58 (50%) for more than 2 y. The mean (±SD) 2-y OS, lRFS, cRFS, and bRFS were 87% ± 5%, 91% ± 4%, 51% ± 8%, and 40% ± 8%, respectively. Given the low number of events during the study period for OS and lRFS (10 and 4, respectively), a multivariable analysis was restricted to cRFS and bRFS (24 and 32 events, respectively).
Correlation of PET-Derived Parameters with Survival Outcomes
Regarding OS (10 events), the only variable significantly associated with an increased mortality was the presence of positive extrapelvic disease (P = 0.02, HR = 11.8, 95% CI = 1.5–95) whereas MTV40, MTV50, and MTV60 were of borderline significance (P values ranging between 0.08 and 0.13). Concerning lRFS (only 4 events), none of the considered parameters was significantly correlated with an increased risk of local relapse.
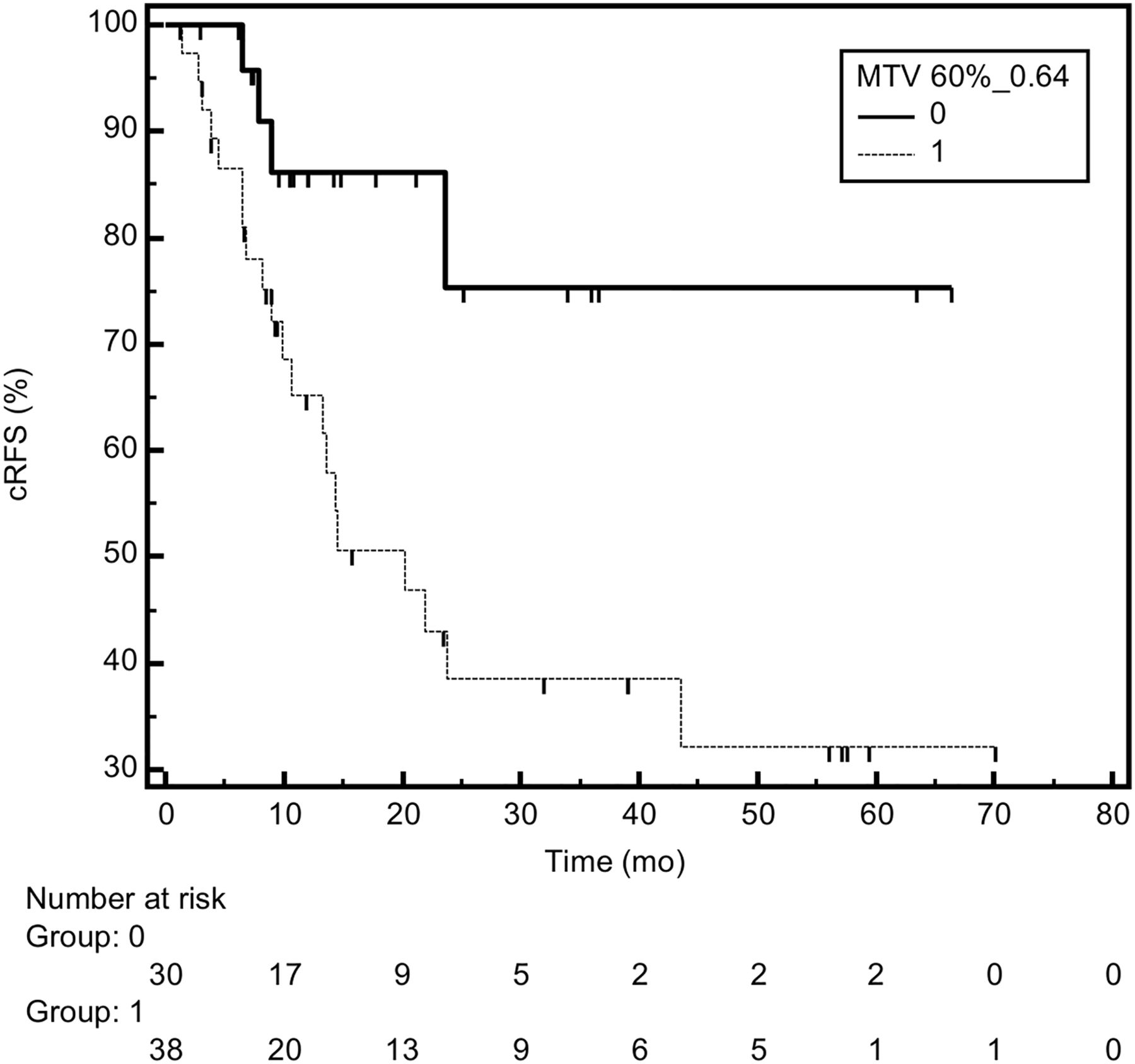
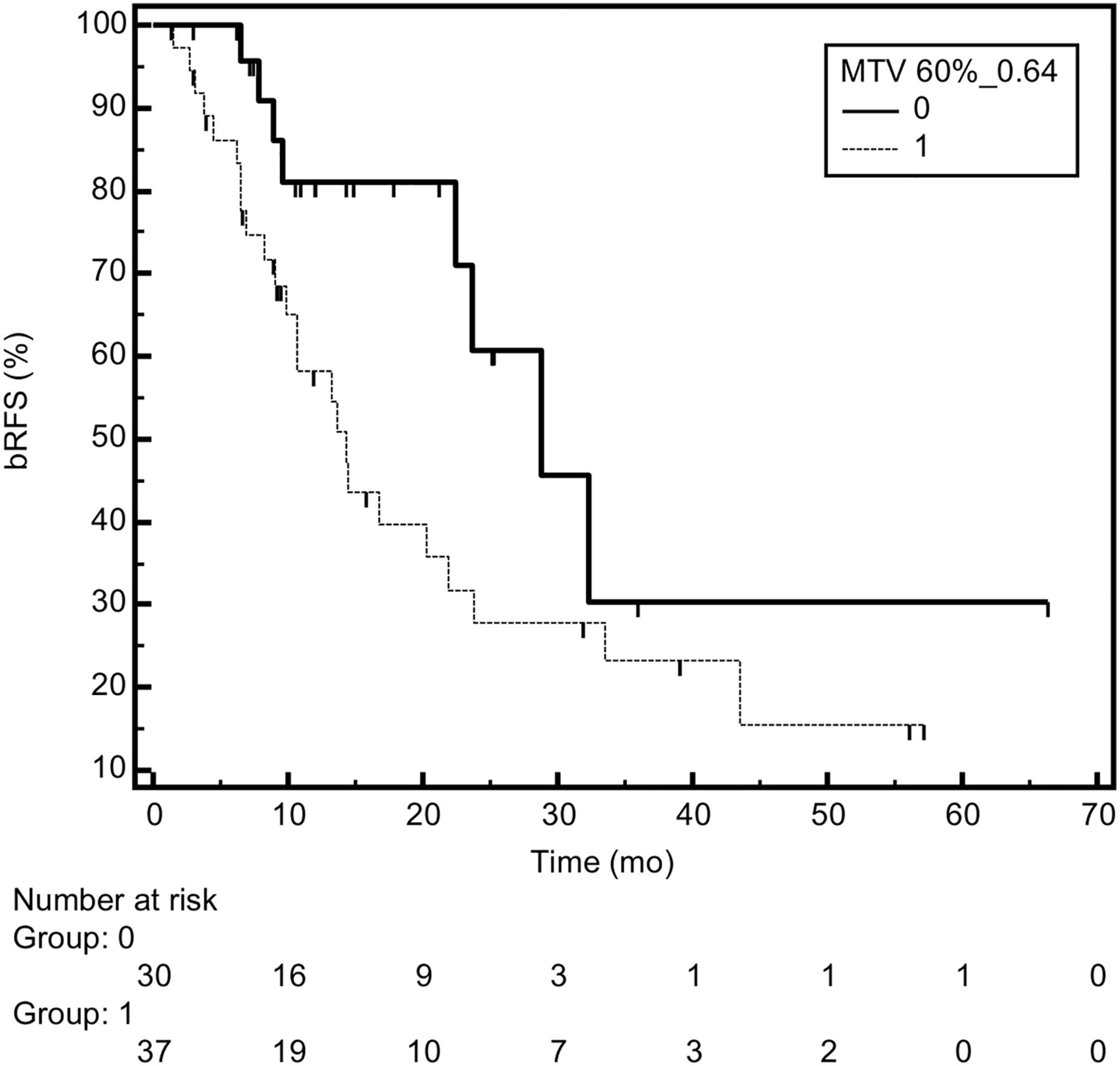
Significant results of univariate Cox regression analysis were used to examine the impact of PET-derived parameters on selected survival outcomes (cRFS and bRFS), as shown in Table 4. MTV60 greater than 0.64 cm3 was significantly correlated with an increased risk of clinical and biochemical relapse (HR = 3.7 and 2.3, respectively; P ≤ 0.04). Figures 2 and 3 show the actuarial risk of clinical and biochemical relapse, respectively, according to MTV60 (≤ or >0.64 cm3).
Results of Univariate Analysis (Variables with P Value < 0.10)

cRFS curves according to MTV60 ≤ 0.64 cm3 (group 0, continuous line) or >0.64 cm3 (group 1, dotted line). P = 0.007.
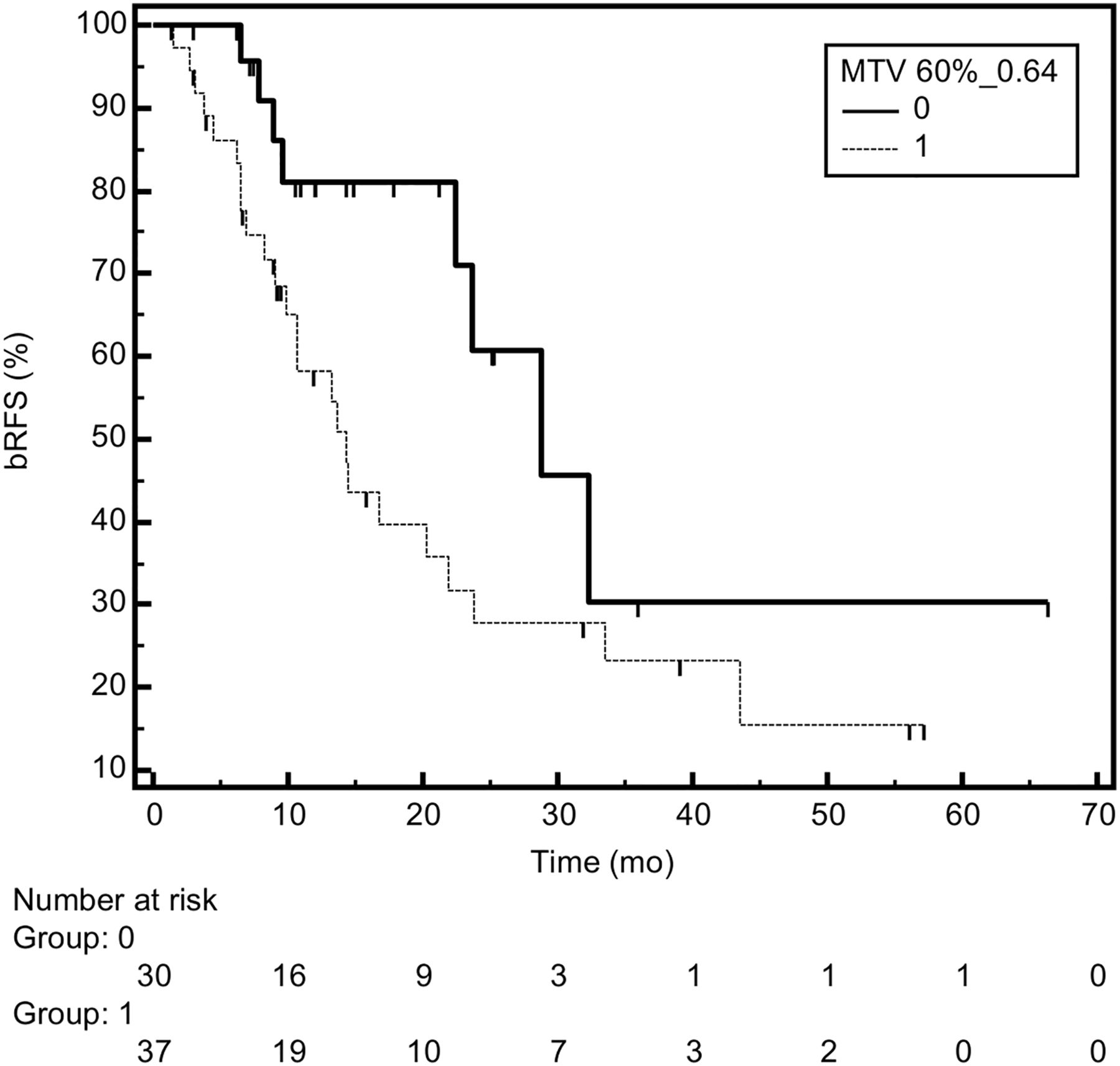
bRFS curves according to MTV60 ≤ 0.64 cm3 (group 0, continuous line) or >0.64 cm3 (group 1, dotted line). P = 0.04.
The results of the multivariate Cox regression analysis are shown for both endpoints in Table 5. Regarding clinical relapse, MTV60 and the presence of choline-positive extrapelvic disease were shown to be independently correlated (MTV60 > 0.64: HR = 4.1, P = 0.010; and extrapelvic disease: HR = 7.3, P = 0.0005), suggesting that patients with sole intrapelvic disease have a lower probability of experiencing a further clinical relapse. The model was rearranged by grouping patients with no risk factors (n = 8, MTV60 ≤ 0.64, only pelvic disease), 1 risk factor (n = 36, either MTV60 > 0.64 or extrapelvic disease), and 2 risk factors (n = 24, MTV60 > 0.64 and extrapelvic disease). In Figure 4, the risk of clinical relapse according to this risk factor stratification is plotted. The 2-y cRFS was 100% ± 10%, 62% ± 11%, and 11% ± 10%, with 0, 1, and 2 factors, respectively (log-rank test, P < 0.0001).
Results of Multivariate Analysis (Variables with P Value < 0.05)

cRFS curves according to number of risk factors. Group 1 = 0 factors (MTV60 ≤ 0.64, only pelvic disease, continuous line); group 2 = 1 factor (either MTV60 > 0.64 or extrapelvic disease, dotted large); and group 3 = 2 factors (MTV60 > 0.64 and extrapelvic disease, dotted small). P < 0.0001.
Regarding bRFS, MTV60 greater than 0.64 cm3, extrapelvic disease, duration of ADT before HTT, ADT during/after HTT, and planning target volume were found to be independently correlated with the risk of relapse; the HR of MTV60 greater than 0.64 cm3 was confirmed to be high (HR = 3.5, P = 0.014).
The 5-fold cross-validation procedure showed that the 2 models were sufficiently robust; regarding cRFS, the AUC of the original multivariable model (Table 5) was 0.76 (95% CI = 0.64–0.85) against an AUC equal to 0.75 (0.55–0.95) for the model corrected for the cross-validation. Similarly, the AUC of the original bRFS model (Table 5) was 0.82 (0.70–0.91) against an AUC equal to 0.81 (0.62–0.99) for the model corrected for the cross-validation.
Also the P values corrected for the cross-validation confirm the robustness of the models: for instance, for cRFS, the P values of the 2 predictive parameters were 0.02 (against 0.01 of the original model) for MTV60 greater than 0.64 cm3 and 0.003 (against 0.0005) for extrapelvic disease. The HR values corrected for the cross-validation were also similar to the original values: concerning cRFS, HRs of MTV60 greater than 0.64 cm3 and of extrapelvic disease corrected for the cross-validation were, respectively, 4.3 and 7.5 (against 4.1 and 7.3 of the original model).
DISCUSSION
11C-choline PET/CT is currently the most-established diagnostic tool used in PCa imaging to define the extent of disease in restaging the clinical setting when PSA serum values increase (22); in particular, its valuable role in guiding tailored treatments in patients with LN recurrence has been demonstrated (11,15,16,23,24). The rationale of the present paper was to evaluate whether 11C-choline PET/CT study, performed to restage PCa patients and to guide tailored treatment on LN recurrence, also had a role in predicting patient outcome in a population previously treated with HTT with SIB on positive LNs detected by 11C-choline PET/CT.
Recently, in a large population of 302 hormone-naive prostatectomized patients, 11C-choline PET/CT was shown to be the most powerful predictor of PCa-specific survival, being suggested to accurately predict PCa-specific survival after radical prostatectomy as well as after PET/CT. 11C-choline PET/CT was positive in 101 of 302 patients (33%); in patients with positive 11C-choline PET/CT, median PCa-specific survival was 14.9 y (95% CI = 9.7–20.1 y), and in patients with negative 11C-choline PET/CT neither the median survival nor the 25th percentile was achieved because of the low number of PCa-specific deaths (n = 5) (19). Moreover, the predictive role of 11C-choline PET/CT on PCa-specific survival in 195 patients with PCa who underwent 11C-choline PET/CT for biochemical relapse during ADT also has been reported. If 11C-choline PET/CT was positive (57% of patients), 15-y PCa-specific survival probabilities were 42.4% (95% CI = 31.7%–53.1%) in androgen-sensitive patients and 17.8% (95% CI = 11.5%–24.1%) in androgen-resistant patients; whereas when 11C-choline PET/CT was negative 15-y PCa-specific survival probabilities were 95.5% (95% CI = 93.5%–97.5%) in androgen-sensitive patients and 53.7% (95% CI = 41.6%–65.8%) in androgen-resistant patients (18).
To the best of our knowledge, no studies have investigated the role of semiquantitative choline PET–derived parameters as biomarkers of survival outcomes in recurrent PCa patients. In different oncologic diseases, 18F-FDG PET–derived parameters have demonstrated predictive significance. In particular, SUV measurement has been described as a useful parameter describing tumor uptake (25–29). Notably, MTV can provide information complementary to that obtained by more commonly used SUV measurement, in particular a decrease in MTV according to 18F-FDG uptake correlates with higher long-term OS and may be used in the prediction of progression-free survival (30–32). Choline uptake is accelerated in cell proliferation of PCa and a useful indicator for detecting tumor location for patients with PCa (33). Volumetric data obtained by choline PET reflect metabolic tumor burden and might be used for evaluation of therapeutic effect. Changes of MTV correspond to the change of the target lesion and reflect the global response of the entire tumor to treatment (34).
In the present study, 11C-choline PET/CT–derived parameters related to tracer uptake (SUVmax and SUVmean) and to the volume of metabolically active disease (MTV) have been analyzed, and their possible correlation with survival outcomes have been reported. Results of biochemical response showed a complete response in 55 of 68 of patients, with a survival of 85% (58/68).
Results of univariate/multivariate analysis suggest that PET data are predictive of disease progression outside the irradiated field, with no further relapse in the irradiated areas (15). In particular, in this study choline uptake volume was higher for PCa with extrapelvic disease than intrapelvic disease when data for the univariate model for bRFS and cRFS were extrapolated.
As for the MTV parameter, the best cutoff values for each threshold (MTV40, MTV50, and MTV60) have been considered and, although they gave similar results, MTV60 resulted in being the most discriminative for bRFS and cRFS in univariate/multivariate analysis. Patient characteristics according to choline uptake indicate that the presence of extrapelvic disease and a high MTV60 are associated with cRFS according to risk factor stratification (P = 0.0005 and 0.010, respectively).
SUVmax and SUVmean were not significantly associated with bRFS and cRFS after normalization for the above-mentioned parameters, suggesting that MTV potentially provides better prognostic information than conventional quantitative parameters.
The major limitation of this study is that it is a retrospective study; thus, to obtain a homogeneous population needed for the analysis, approximately 18% of patients had to be excluded from the original patient population (15).
In addition, the manual drawing of the regions of interest might represent another limitation of this study. However, the regions of interest have been drawn by a single nuclear medicine physician with extensive PET/CT experience for radiation oncology applications. Because only 1 nuclear medicine physician was involved, interobserver variability is not a bias factor. Intraobserver, that is, interregion variability, is affected by many factors that are independent of the physician involved in drawing regions of interest, such as size of the LN, intensity of uptake, and partial-volume effect, so that, considering the primary aim of this study, intrasubject variability was not assessed.
CONCLUSION
The results of the present study indicate that SUVmax and SUVmean parameters were not significantly associated with the survival outcomes considered. As for MTV, MTV60 resulted in being the best predictor for bRFS and cRFS. In particular, MTV60 and the presence of choline LN pathologic uptake outside the pelvic region (extrapelvic disease) were independent prognostic factors for predicting bRFS and cRFS, suggesting that these parameters might be used to select therapeutic strategy, by identifying PCa patients with LN recurrence after primary treatment who will most likely experience poor prognosis.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 24, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication July 14, 2015.
- Accepted for publication August 28, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Initial Experience with Volumetric 68Ga-PSMA I&T PET/CT for Assessment of Whole-Body Tumor Burden as a Quantitative Imaging Biomarker in Patients with Prostate Cancer
- Evaluation of Prostate Cancer with 11C-Choline PET/CT for Treatment Planning, Response Assessment, and Prognosis
- What Medical, Urologic, and Radiation Oncologists Want from Molecular Imaging of Prostate Cancer