


Abstract
Early detection of infection in acute pancreatitis (AP) affects the choice of treatment and clinical outcome. We used PET/CT with 18F-FDG–labeled autologous leukocytes to detect infection in pancreatic or peripancreatic fluid collections in patients with AP. Methods: Forty-one patients (28 men and 13 women) who were 21–69 y old (mean ± SD, 41 ± 11.5) and had AP and radiologic evidence of a fluid collection in or around the pancreas were studied. Leukocytes were separated from the patient’s venous blood, labeled with 18F-FDG, and reinjected intravenously; PET/CT images were acquired 2 h later. A final diagnosis of infection was based on microbiologic culture of fluid aspirated from the collection. Patients were treated with supportive care and antibiotics; percutaneous drainage or laparotomy was performed when indicated. Results: Blood glucose level, total leukocyte count, neutrophil count, and leukocyte labeling efficiency varied from 83 to 212 mg/100 mL (118 ± 30), 4,600 to 24,200/mm3 (11,648 ± 5,376), 55% to 90% (73 ± 10), and 31% to 97% (81 ± 17), respectively. Increased tracer uptake in the fluid collection was seen in 12 of 41 patients; 10 had culture-proven infection and underwent percutaneous drainage, and aspiration was unsuccessful in 2. The scan results were negative for infection in 29 patients; 25 had fluid culture results that were negative for infection, and aspiration was unsuccessful in 4. The sensitivity, specificity, and accuracy of the scan were all 100% in 35 patients for whom fluid culture reports were available. Conclusion: PET/CT with 18F-FDG–labeled leukocytes is a noninvasive and reliable method for the diagnosis of infection in pancreatic or peripancreatic fluid collections in patients with AP.
Acute pancreatitis (AP) is a clinical challenge with significant morbidity and mortality. In previous studies, 40%–70% of patients with AP had pancreatic or peripancreatic infections, which were largely responsible for late mortality (1). It is important to diagnose sepsis of pancreatic or peripancreatic necrosis. Although sterile pancreatic necrosis has relatively lower mortality rates (5%–10%) and can be managed conservatively, infected necrosis increases mortality rates substantially (20%–30%) and requires percutaneous or endoscopic drainage or surgical debridement (2). Radiologic diagnosis of infection in pancreatic or peripancreatic fluid collections depends on the detection of gas bubbles on contrast-enhanced CT (CECT) (3). In the absence of gas bubbles, infection is confirmed by fine-needle aspiration (FNA) of the fluid collection, Gram staining, and culturing for bacterial or fungal organisms (4).
Some authors have shown the usefulness of radionuclide-labeled leukocyte scintigraphy for the detection of infected pancreatic necrosis in patients with AP (5–10) and have even suggested it as an alternative to CECT for staging AP (10). However, these studies were limited to γ-camera scintigraphy with leukocytes labeled with 111In (5) or 99mTc (7–10), and image quality and resolution were unsatisfactory.
The feasibility of labeling leukocytes in vitro with 18F-FDG was first demonstrated by Osman and Danpure (11) and subsequently verified in both animals and humans by other groups (12,13). Rini et al. directly compared leukocytes labeled with 111In and leukocytes labeled with 18F-FDG in orthopedic infections and described similar sensitivities, specificities, and accuracies with both tracers (14). Dumarey et al. demonstrated the use of PET/CT with 18F-FDG–labeled autologous leukocytes in a heterogeneous group of 21 patients, 3 of whom had suspected pancreatic infection (15). However, to date there are no studies on the specific use of 18F-FDG–labeled leukocytes for the evaluation of pancreatic infection in patients with AP. The combination of the specificity of labeled leukocytes and the high spatial resolution of PET/CT with the 18F-FDG label may provide a means of early and specific detection of infection in pancreatic or peripancreatic fluid collections in the clinical setting of AP.
This prospective study was designed to assess the efficacy of PET/CT with 18F-FDG–labeled autologous leukocytes for the detection of infection in pancreatic or peripancreatic fluid collections in patients with AP.
MATERIALS AND METHODS
Study Design and Patient Selection
This study was performed in a tertiary care hospital between September 2010 and February 2012. The Ethics Committee of the Postgraduate Institute of Medical Education and Research approved this study, and all subjects gave written informed consent.
Forty-one consecutive patients (28 men and 13 women; mean age, 41 y; SD, 11.5 y) with AP and radiologic evidence of fluid collection in or around the pancreas were studied. Patients who had received antibiotics in the preceding 7 d and those with a severity of illness precluding a move to the nuclear medicine department were excluded. The inclusion criterion was ultrasound or CECT evidence of pancreatic or extrapancreatic fluid collections, with or without pancreatic necrosis. None of the patients was diabetic. The fluid collections were classified in accordance with the revised Atlanta classification (16) at the time of analysis. The characteristics of the patients are shown in Table 1.
Characteristics of Patients
Each patient was subjected to PET/CT after injection of 18F-FDG–labeled leukocytes. Each patient also underwent ultrasound- or CT-guided FNA of the pancreatic or peripancreatic fluid collection within 24 h of PET/CT imaging, and the aspirate was sent to a laboratory for Gram staining and culturing.
Preparation of 18F-FDG–Labeled Leukocytes
The total leukocyte count and the differential leukocyte count measured on the day preceding the injection of 18F-FDG–labeled leukocytes were recorded. Patients fasted for 4 h before the collection of blood. After the blood glucose level was assessed, 40 mL of venous blood was collected in a heparinized syringe, which was then kept upright in a stand at 37°C for 60–70 min to separate the plasma. All other syringes, tubes, pipettes, and needles were kept under ultraviolet light for 30 min before the procedure. The plasma was transferred to a sterile centrifuge tube and centrifuged at 450g for 5 min. The supernatant plasma was removed and placed in a second centrifuge tube. The white cell pellet at the bottom of the first tube was reconstituted with 2.5 mL of heparinized normal saline, and 314.5–555 MBq (8.5–15 mCi) of 18F-FDG were added to the suspension. This radiolabeled suspension was kept at 37°C for 25–30 min, with gentle shaking every 5 min. During this time, the supernatant plasma was centrifuged at 450g for 25 min to obtain cell-free plasma. After incubation, 12 mL of heparinized normal saline were added to the radiolabeled suspension, the tube was centrifuged at 450g for 5 min, and the supernatant was removed. The whole labeled cell suspension and supernatant were measured separately in a dose calibrator to calculate the efficiency of cell labeling. The radiolabeled white cell sediment was reconstituted with 4 mL of the patient’s own cell-free plasma and reinjected intravenously. For assessment of the viability of the labeled cells, an aliquot of the labeled cell preparation was stained with 0.4% trypan blue and examined under a light microscope for the presence of any blue (nonviable) cells.
PET/CT Imaging
Whole-body PET/CT images (from the vertex of the skull to mid thigh) were acquired 2 h after injection of the 18F-FDG–labeled leukocytes with a dedicated PET/CT scanner (Discovery STE 16; GE Healthcare). PET images were acquired over 7–9 bed positions at 2 min for each bed position and reconstructed through iterative reconstruction. CT images were acquired with the integrated 16-slice CT scanner and the following parameters: voltage, 120 kVp; beam current, 250–350 mA; and slice thickness, 3.75 mm. For the first 18 patients, no intravenous contrast material was used, because diagnostic CECT had been performed earlier. For subsequent patients, contrast-enhanced PET/CT was performed directly (except when clinically contraindicated) as a single investigation instead of as separate CT and PET/CT studies. For these patients, oral contrast material (76% sodium diatrizoate) was mixed with 2 L of water and administered at 60–120 min after radiotracer injection; intravenous contrast material (iohexol) was injected 45 s before acquisition of the CT scan was begun.
Outcomes and Follow-up
Two experienced nuclear medicine physicians unaware of the clinical course, culture data, and any previous CT scan results interpreted the scans in consensus with a radiologist. Tracer activity in the liver, spleen, and bone marrow was regarded as normal physiologic uptake of labeled leukocytes. Tracer activity in the brain, renal collecting system, and urinary bladder was attributed to free 18F-FDG, as reported earlier (14,15). The absence of tracer activity in the abdomen outside the liver and spleen was regarded as normal. Non–tracer-avid fluid collections were considered noninfected (Fig. 1), and minimal diffuse tracer activity in the vicinity of a fluid collection was regarded as background activity due to inflammation (Fig. 2). Markedly increased tracer activity in the pancreas or a pancreatic or peripancreatic fluid collection was attributed to infection (Fig. 3). The maximum standardized uptake values (SUVmaxs) for these regions were calculated with standard processing software (Advantage Windows; GE Healthcare). Increased tracer activity in regions other than the abdomen (especially the lungs) was recorded. The microbiologic culture report for fluid aspirated from a collection was used as the gold standard for the diagnosis of infection.

18F-FDG–labeled leukocyte PET/CT images of patient with noninfected peripancreatic fluid collection. (A) Maximum-intensity-projection image showing no tracer uptake in central abdomen. (B–D) Coronal fused PET/CT (B), transaxial CT (C), and corresponding transaxial fused PET/CT (D) images showing large cystic non–tracer-avid peripancreatic fluid collection extending into lesser sac region. Fluid aspirated from collection was sterile on culture.

18F-FDG–labeled leukocyte PET/CT images of patient with peripancreatic fluid collection showing mild inflammation. (A) Maximum-intensity-projection image showing minimal tracer uptake in central abdomen, with nonhomogeneous uptake in liver and patchy uptake in basal segment of left lung. (B–D) Coronal fused PET/CT (B), transaxial CT (C), and corresponding transaxial fused PET/CT (D) images showing fluid collection with mildly tracer-avid margins (SUVmax, 3.0) in neck, body, and tail of pancreas. Fluid aspirated from collection was sterile on culture.

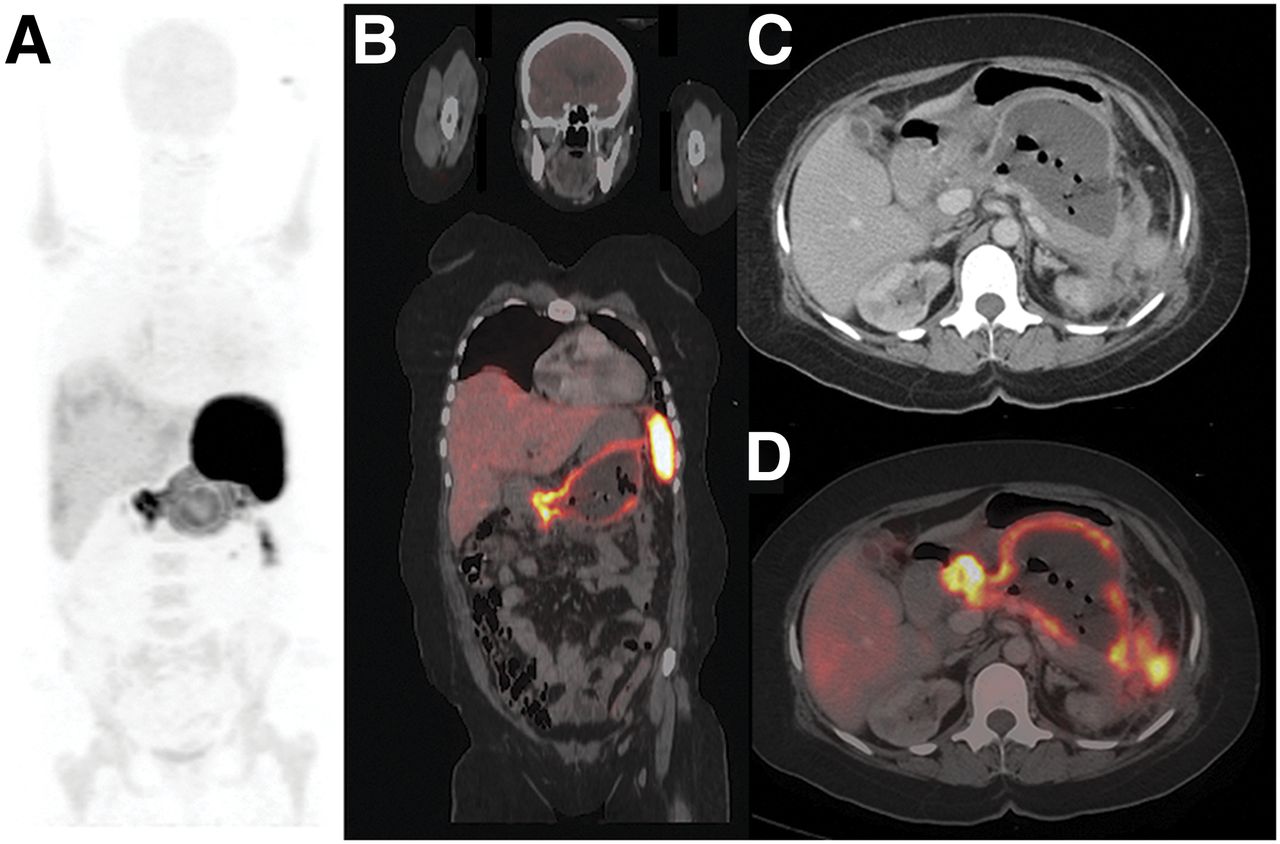
18F-FDG–labeled leukocyte PET/CT images of patient with infected peripancreatic fluid collection. (A) Maximum-intensity-projection image showing intense tracer uptake in central abdomen (SUVmax, 35), extending to spleen and left paracolic region. Mild irregular tracer uptake can be seen in both lungs. (B) Coronal fused PET/CT image showing large fluid collection with markedly tracer-avid margins replacing body and tail of pancreas. (C) Transaxial CT image at level of pancreas showing air bubbles in fluid collection. (D) Corresponding transaxial fused PET/CT image showing intense tracer uptake along margins of fluid collection. Fluid aspirated from collection showed growth of E. coli on culture.
Patients were treated in accordance with the protocol of the Postgraduate Institute of Medical Education and Research, which included fluid resuscitation, organ support, and antibiotics for documented infection. Fluid collections with complications such as compression of the stomach or infection were subjected to percutaneous catheter drainage. Patients with worsening organ failure underwent necrosectomy.
RESULTS
Of the 41 patients, 21 were febrile and 20 were afebrile at the time of the study. Patients were classified in accordance with the revised Atlanta classification (16) as follows: 21 had acute necrotic collections, 18 had walled-off necrosis, and 2 had pseudocysts. Normal physiologic biodistribution of 18F-FDG–labeled leukocytes was seen in the liver, spleen, and bone marrow in all patients. Minimal tracer activity detected in the brain and urinary bladder likely was due to 18F-FDG eluted from the leukocytes. No myocardial tracer activity was seen in any patient, and no normal physiologic tracer activity was detected in the intestines. Minimal tracer activity was seen in the renal pelvis in a few inadequately hydrated patients. However, most of the patients had no tracer activity in the kidneys or ureters.
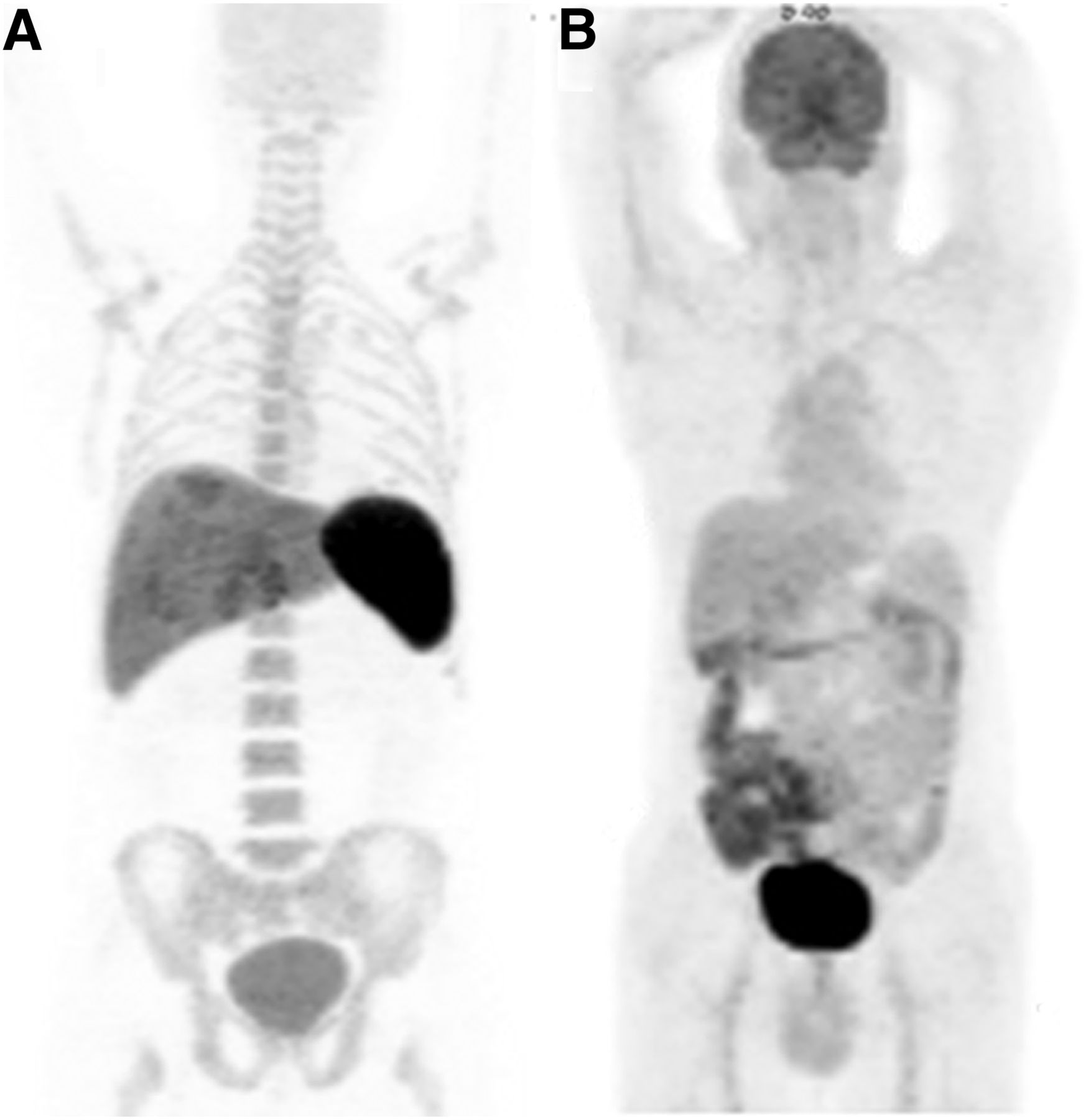
Figure 4 shows a comparison of the normal physiologic distribution of 18F-FDG–labeled leukocytes with that of 18F-FDG alone. The blood glucose level, total leukocyte count, neutrophil count, amount of 18F-FDG used, amount of radiotracer injected, and labeling efficiency are shown in Table 1. The trypan blue dye exclusion method revealed a leukocyte viability of greater than 99% in all patients. Radiation exposure to the staff performing the labeling procedure varied from 4 to 10 μSv (5.6 ± 1.4 μSv) for each patient.

Maximum-intensity-projection images showing normal physiologic distribution of 18F-FDG–labeled autologous leukocytes in liver, spleen, and bone marrow, with minimal uptake in brain (A), and normal physiologic distribution of 18F-FDG alone (B).
Increased uptake of 18F-FDG–labeled leukocytes, indicative of infection, was seen in pancreatic or peripancreatic fluid collections in 12 of the 41 patients, and bacterial culture results were positive in 10 of these 12 patients. The organisms included Escherichia coli (n = 5), Pseudomonas aeruginosa (n = 2), Staphylococcus aureus (n = 1), Enterococcus faecalis (n = 1), and Candida tropicalis (n = 1). In the other 2 patients, fluid aspiration yielded little material, which could not be evaluated. Radiotracer concentrations varied widely in the infected collections as well as at different regions within the same collection, with SUVmaxs ranging from 5.3 to 46 (median, 13.6). In the noninfected collections, SUVmaxs ranged from 1.1 to 5.1 (median, 1.8). SUVmaxs of greater than or equal to 5.3 were diagnostic of infection in this series of patients. Gas bubbles were detected on CT scans for 5 of the 12 patients with positive scan results, including the 2 for whom no final culture report was available.
No abnormal uptake of 18F-FDG–labeled leukocytes was detected in the remaining 29 patients. For 25 of these patients, culture results were negative for infection, and aspiration was unsuccessful in 4. None of the 29 patients with negative scan results had any gas bubbles on CT scans. There were no false-positive or false-negative PET/CT scan results for 35 patients for whom fluid culture reports were available. Hence, the sensitivity, specificity, and accuracy of the scan were all 100%.
Fluid collections with positive scan and culture results were classified in accordance with the revised Atlanta classification (Table 2). Of the 10 patients with positive culture results, 6 underwent percutaneous catheter drainage of the fluid collection, 2 underwent percutaneous catheter drainage with endoscopic retrograde cholangiopancreatography, 1 had endoscopic retrograde cholangiopancreatography alone, and 1 required surgical debridement after percutaneous catheter drainage. The 2 patients with positive scan results were treated conservatively with antibiotics. All 12 patients recovered satisfactorily and have remained well on follow-up. The 29 patients with negative scan results were all treated conservatively and experienced a good recovery.
Details of Fluid Collections with Positive Scan and Culture Results
Patchy lung uptake of radiolabeled leukocytes, corresponding to segmental consolidation or segmental collapse with consolidation, on the fused CT images was seen in 14 of the 41 patients (34%). This finding was seen in 6 of 12 patients with positive scan results (50%) but in only 8 of 29 patients with negative scan results (28%). The total leukocyte count, neutrophil count, leukocyte labeling efficiency, amount of 18F-FDG used, and amount of tracer injected were similar in patients with positive scan results and patients with negative scan results (Table 1). However, more of the former patients (75%) than of the latter patients (41%) were febrile. No adverse effects were seen in any of the patients after the PET/CT scan with labeled leukocytes.
DISCUSSION
We have shown the utility of PET/CT with 18F-FDG–labeled leukocytes for the detection of infection in pancreatic or peripancreatic fluid collections associated with AP. Of the 41 patients studied, 12 had positive scan results, suggestive of infection, and 10 had culture-proven infection. Of the 29 patients with negative scan results, 25 had negative culture results, and adequate material could not be aspirated in 4. Of the 35 patients for whom fluid culture reports were available for comparison, none had false-positive or false-negative results for infection on PET/CT with 18F-FDG–labeled leukocytes; these findings signified sensitivity, specificity, and accuracy of 100% each for this small series of patients.
Pancreatic fluid collections that contain nonliquefied material are more likely to become infected. CECT suggests infection if gas bubbles are present in a collection because of the presence of gas-forming organisms. However, gas bubbles may also be present in a collection after spontaneous drainage into the gastrointestinal tract, marsupialization, or other drainage procedures (3). Gas bubbles were detected on CT scans for only 5 of the 12 patients with positive scan results (3 with fluid culture results positive for infection) in the present study.
The gold standard for the diagnosis of infection in pancreatic or peripancreatic fluid collections is FNA with Gram staining and culturing for bacterial or fungal organisms (4). Although most of these fluid collections are reabsorbed spontaneously within the first few weeks, drainage or aspiration of fluid at this stage could introduce infection. A negative FNA result in a patient with a high clinical suspicion of infection may necessitate repeated FNA (17). Percutaneous drainage of sterile pancreatic necrosis remains controversial and has the potential to introduce infection through colonization of the indwelling catheter (18). On the other hand, infected necrosis may necessitate surgical debridement and treatment with antibiotics.
Inflammation is a complex protective nonspecific tissue response as well as a consequence of injury; if caused by living microbes, the injury leads to infection (19). Acute inflammation is associated with vasodilatation, increased vascular permeability, and formation of exudate, followed by chemotaxis, leukocyte margination, and leukocyte emigration (20,21). Leukocytes have specific receptors for chemotactic factors produced by bacteria or present in plasma that result in attraction, particularly of polymorphonuclear leukocytes, to the site of infection. The principle mechanisms of uptake of radiolabeled leukocytes at sites of infection are cellular migration and target-specific localization (22). Osman and Danpure showed that 87% of 18F-FDG is associated with labeling of granulocytes (11). Although nonspecific uptake of 18F-FDG–labeled leukocytes may occur at noninfected inflammatory sites, our findings indicate a high specificity of 18F-FDG–labeled leukocytes for identifying infected fluid collections in the setting of AP.
Previous studies in which scintigraphy with radionuclide-labeled leukocytes was used to detect infected pancreatic necrosis were limited to γ-camera scintigraphy with leukocytes labeled with 111In (5,6) or 99mTc (7–10). The use of 67Ga SPECT/CT imaging, with high sensitivity and specificity, was also reported in this clinical context (23). However, image quality and resolution obtained with these tracers were unsatisfactory, especially for planar scintigraphy. Osman and Danpure (11) first described the in vitro labeling of leukocytes with 18F-FDG, and several groups subsequently used this tracer to detect different types of infection in both animals and humans (12–15). In the present study, the image quality provided by PET/CT with 18F-FDG–labeled leukocytes was clearly superior to that previously reported with 99mTc- or 111In-labeled leukocytes. An additional advantage of PET/CT with 18F-FDG–labeled leukocytes is the significantly reduced imaging time. Imaging with 67Ga requires 48–72 h, and scintigraphy with 99mTc- or 111In-labeled leukocytes requires up to 24 h. In comparison, PET/CT with 18F-FDG–labeled leukocytes was completed within 3 h of tracer injection. Therefore, a decision regarding conservative management or drainage of the fluid collection can be made on the same day.
Our labeling technique required only 40 mL of venous blood, and leukocyte labeling efficiency, viability, and image quality were comparable to those reported earlier (14,15). The use of radiologic contrast material with the PET/CT study also allowed grading of pancreatitis and evaluation for infection in a single study. Dumarey et al. reported SUVmaxs of 0.9–37.4 for infected lesions in a heterogeneous group of 21 patients, 3 of whom had suspected pancreatic infection (15). The SUVmaxs of 5.3–46 for infected pancreatic or peripancreatic fluid collections in the present study represented a similarly wide range. Two cases in which PET/CT with 18F-FDG–labeled leukocytes was used to detect pancreatic infection in patients with AP were reported earlier (24,25). However, to our knowledge, no previous study reported any specific SUVmax cutoff at which this radiotracer can identify abdominal infection.
Focal pulmonary uptake of radiolabeled leukocytes has been reported in patients with pneumonitis, atelectasis, pulmonary embolism, congestive heart failure, adult respiratory distress syndrome, and aspiration pneumonia (26,27). The patchy pulmonary tracer uptake in about one third of our patients was probably due to active lung infection or inflammation as part of the systemic disease; such a finding may be useful for monitoring the response to treatment. In contrast to the behavior of 18F-FDG and 67Ga, the absence of normal physiologic gastrointestinal uptake of 18F-FDG–labeled leukocytes makes this tracer ideal for assessing intraabdominal infections. We previously reported the incidental detection of pseudomembranous colitis with this technique in a patient being evaluated for pancreatic infection (25).
The present study had some limitation. It included only 41 patients. Although this number appears to be small, the total number of subjects reported to have had PET with 18F-FDG–labeled autologous leukocytes over a time span of 8 y (2002–2010) is only 76, including 70 patients and 6 healthy controls (28). The fact that the fluid collection could not be aspirated for culturing in some patients was another limitation of the present study. Although the use of radiologic contrast material differed between the first 18 patients and subsequent patients, this difference did not influence the PET/CT diagnosis, which was based only on the uptake of 18F-FDG–labeled leukocytes in the fluid collection. Finally, we did not compare PET/CT with 18F-FDG–labeled leukocytes and PET with 18F-FDG alone in this preliminary study. However, animal experiments by Pellegrino et al. showed that the focal uptake of 18F-FDG–labeled leukocytes was a specific phenomenon in infection and not the result of nonspecific accumulation of free 18F-FDG (29).
CONCLUSION
PET/CT with 18F-FDG–labeled autologous leukocytes is a reliable, accurate, noninvasive imaging technique for the detection and localization of infection in pancreatic or peripancreatic fluid collections in patients with AP. The absence of normal physiologic gastrointestinal and genitourinary tracer uptake is an added advantage in image interpretation.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We gratefully acknowledge the technical help provided by Nivedita Rana in cell labeling and by Ankit Watts, Raghava Kashyap, and Rajendra Kumar in conducting the PET/CT procedures.
Footnotes
Published online Jul. 3, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication January 7, 2014.
- Accepted for publication May 9, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.