


Abstract
We prospectively compared 11C-acetate with 18F-FDG in a PET/CT evaluation of multiple myeloma (MM), specifically on diagnostic accuracy, identification of high-risk patients, and monitoring of treatment response. Methods: Dual-tracer PET/CT was performed on 35 pathologically and clinically confirmed and untreated patients (26 with symptomatic MM, 5 with smoldering MM, and 4 with monoclonal gammopathy of unknown significance) and 20 individuals with normal marrow. Results: 11C-acetate showed significant incremental value over 18F-FDG (84.6% vs. 57.7%) for positively identifying patients with diffuse and focal symptomatic MM, and was negative in patients with indolent smoldering MM and monoclonal gammopathy of unknown significance. Three functional parameters—number of 11C-acetate–avid and 18F-FDG–avid focal bone lesions and 11C-acetate general marrow activity—strongly correlated with β-2-microglobulin as surrogate imaging markers of tumor burden. After induction chemotherapy, the metabolic change in 11C-acetate general marrow activity correlated with clinical response. Conclusion: Metabolic characterization of MM in diagnosis, risk stratification, and treatment monitoring can be done more accurately by assessing lipid metabolism with 11C-acetate than by assessing glucose metabolism with 18F-FDG.
Plasma cell neoplasm is a form of mature B-cell malignancy comprising a spectrum of monoclonal (M) proliferation of plasma cells ranging from monoclonal gammopathy of unknown significance (MGUS) to smoldering multiple myeloma (SMM) to symptomatic multiple myeloma (MM). MGUS, as a precursor of MM, is distinguished from SMM and symptomatic MM by having less than 10% bone marrow plasma cells and by having an M-protein level of less than 30 g/L. MGUS and SMM are defined as lacking the complications arising from hypercalcemia, renal insufficiency, anemia, and osteolytic bone lesions, the presence of any of which defines symptomatic MM and hence is an indication for treatment (1).
A whole-body radiologic survey is the conventional tool to evaluate osteolytic MM lesions but is insensitive early during disease development. MR imaging and 18F-FDG PET/CT are the current state-of-the-art tools for MM evaluation (2,3). However, MR imaging is less reliable in distinguishing active disease from scar or necrosis and thus is suboptimal for early assessment of treatment response (4). 18F-FDG PET/CT can assess treatment response (4–6) but is insensitive for diffuse disease.
This study aimed to investigate whether metabolic characterization by 11C-acetate, a marker of lipid metabolism upregulated in myeloma cell lines (7), may be superior to 18F-FDG for diagnosis, risk stratification, and treatment monitoring of plasma cell neoplasms.
MATERIALS AND METHODS
Patients
This study was approved by the Ethics and Research Committee, and the patients gave written consent to participate. Between July 2009 and July 2012, we consecutively enrolled suspected or confirmed untreated MM patients for 11C-acetate and 18F-FDG PET/CT. All patients underwent bone marrow trephine biopsy, immunofixation testing, measurement of serum β-2-microglobulin (b2m) concentration, and a whole-body radiologic survey within 2 wk before or after PET/CT. There were 35 patients (20 men and 15 women; mean age ± SD, 63.4 ± 11.7 y): 26 with symptomatic MM (19 stage I, 3 stage II, and 4 stage III according to the International Staging System (8)), 5 with SMM, and 4 with MGUS. Twenty controls (12 men and 8 women; mean age, 59.2 ± 10.9 y) with normal marrow were also included.
All patients fasted for more than 6 h before injection of 11C-acetate, and their blood glucose level was less than 8 mmol/L. 11C-acetate PET/CT (4-ring high-definition Biograph 40; Siemens) was performed at 20 min after injection, followed by 18F-FDG injection approximately 15 min after 11C-acetate imaging. 18F-FDG PET/CT was performed 60 min after injection.
Interpretation Criteria on PET/CT
Diagnosis of symptomatic MM on 11C-acetate and 18F-FDG PET/CT is summarized in Figure 1. Lesions smaller than 10 mm were excluded to avoid gross underestimation of maximum standardized uptake value (SUVmax) (by body weight). The SUVmax of the L3 vertebra was defined as the general marrow activity on the condition that there was no focally hypermetabolic disease. Patients with increased general marrow activity (greater than the threshold obtained by the receiver-operating-characteristic curve) for either tracer were classified as having diffuse MM.
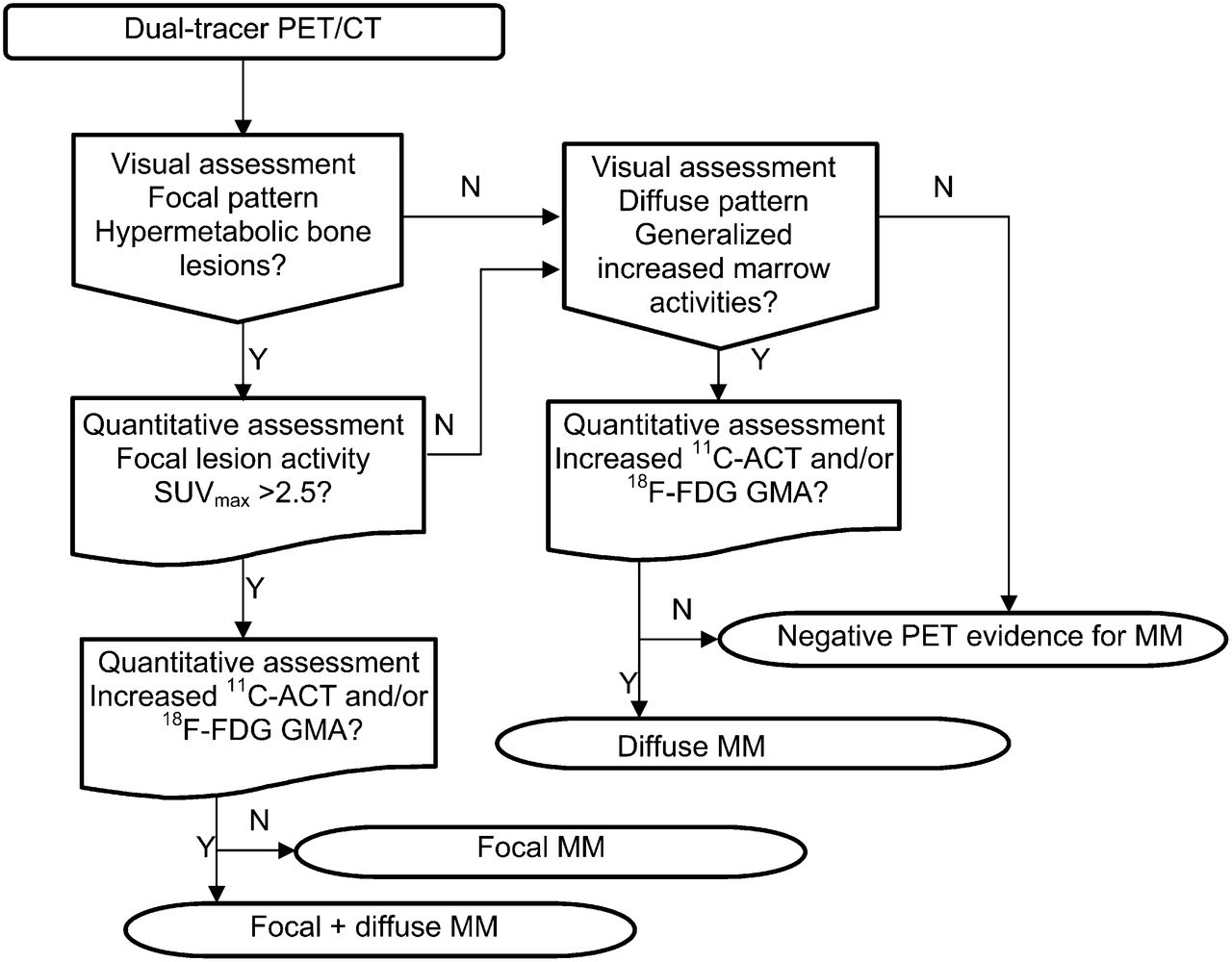
Algorithm for diagnosis and categorization of symptomatic MM on PET/CT. ACT = acetate; GMA = general marrow activity.
Treatment Response Monitoring
Nine of the 26 symptomatic MM patients underwent follow-up PET/CT within 2 wk after completion of chemotherapy. Clinical response was assessed by the New Uniform Response Criteria (9), categorized as complete remission, very good partial response, partial response, no response, or progressive disease. Two patients with oligosecretory myeloma were assessed by repeated bone marrow aspiration.
Metabolic response was evaluated by percentage change in general marrow activity (GMA) for diffuse MM, and by percentage change in focal bone lesion (FBL) number for focal MM,
and by percentage change in focal bone lesion (FBL) number for focal MM,
Statistical Analysis
The avidity difference and focal bone lesion SUVmax between the 2 tracers were evaluated by χ2 and t tests, respectively. Serum b2m was correlated with general marrow activity, focal bone lesion SUVmax, and focal bone lesion number for both tracers (total of 6 parameters) by Pearson correlation analysis for their respective relationships to tumor burden in symptomatic MM patients with normal renal function. The metabolic and clinical responses were compared by correlation analysis. Statistical analysis was performed using SPSS, version 14.0 (IBM).
RESULTS
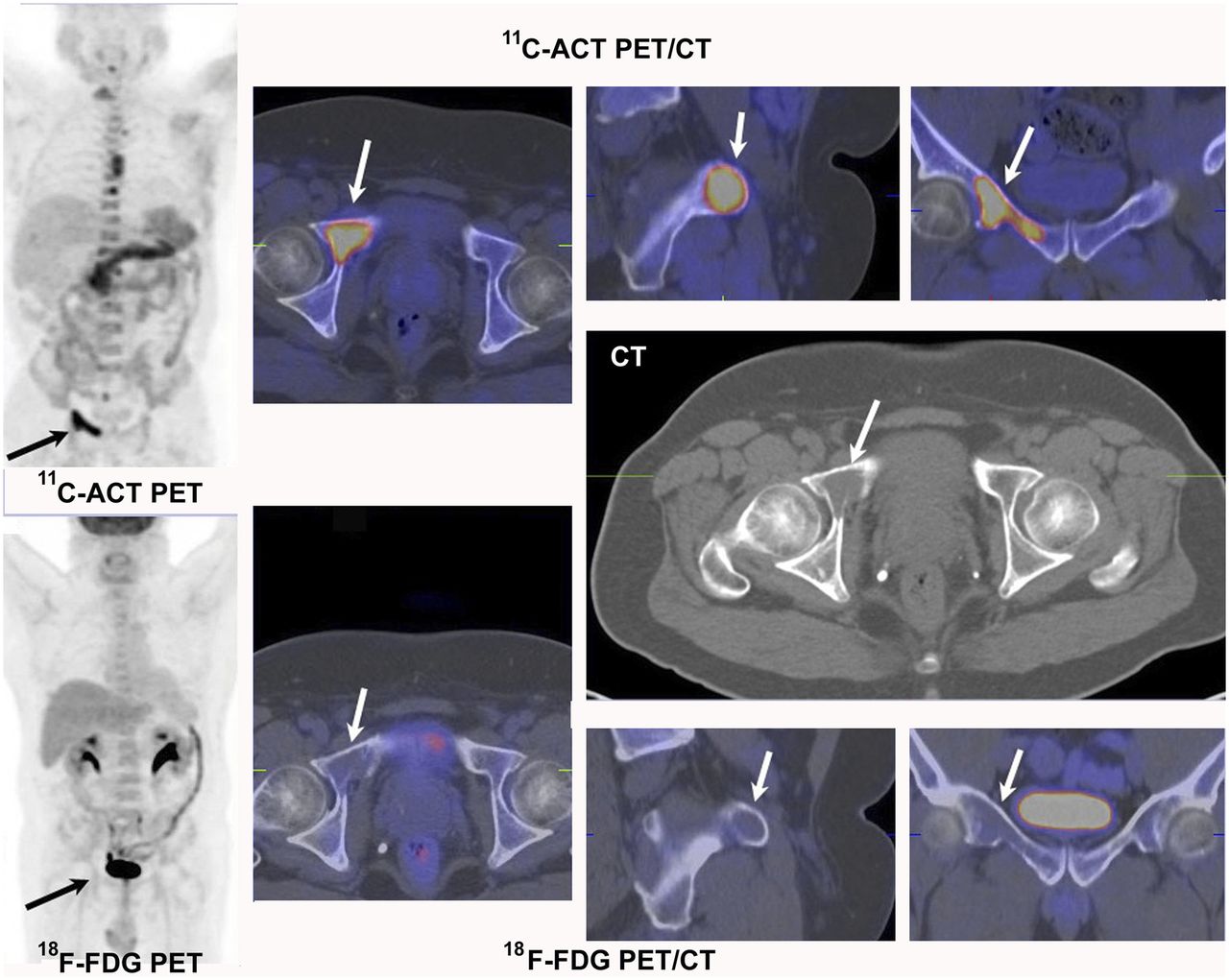
General marrow activity, focal bone lesion SUVmax, and focal bone lesion number for both tracers are summarized in Table 1. The mean 11C-acetate and 18F-FDG general marrow activity of controls were 2.34 ± 0.67 and 2.12 ± 0.57, respectively, which were used as negatives in receiver-operating-characteristic analysis. The thresholds of 11C-acetate and 18F-FDG general marrow activity for diagnosing diffuse MM were 3.79 and 3.03 (area under the curve, 0.974 vs. 0.820), respectively. Twenty-five of the 26 symptomatic MM patients had a diffuse pattern (13 diffuse; 12 focal and diffuse), with 21 (84%) identified by 11C-acetate (mean general marrow activity, 5.43 ± 1.73) and 12 (48%) by 18F-FDG (mean general marrow activity, 4.43 ± 1.25) with their respective thresholds. Nine (36%) of the 25 patients with diffuse MM were purely 11C-acetate–avid, and none was purely 18F-FDG–avid. Four of the 25 patients with diffuse MM were negative by both tracers, but all had a low serum b2m level of 1.5–2.2 μg/mL. All indolent plasma cell neoplasms (SMM and MUGS) were negative by 11C-acetate PET, whereas 2 cases of MGUS were false-positive by 18F-FDG. There were 13 patients with hypermetabolic focal bone lesions, all 13 detected by 11C-acetate and 10 by 18F-FDG (mean SUVmax, 14.0 ± 4.5 vs. 9.2 ± 4.9, P < 0.05). Three (23.1%) of the 13 patients had focal bone lesions purely avid for 11C-acetate, whereas none was purely avid for 18F-FDG. Figure 2 shows the PET/CT images of patient 14, who had focal bone lesions almost purely 11C-acetate–avid.
Patient Characteristics, Clinical Diagnosis, and Dual-Tracer PET/CT Diagnosis

Dual-tracer PET/CT of patient 14 showing biopsy-confirmed focal bone lesions (arrows) that are purely 11C-acetate–avid. ACT = acetate.
The overall sensitivity for symptomatic MM was significantly higher with 11C-acetate than with 18F-FDG (22/26 [84.6%] vs. 15/26 [57.7%], P < 0.05). The specificity for 18F-FDG and 11C-acetate PET/CT was 93.1% (27/29) and 100% (29/29), respectively.
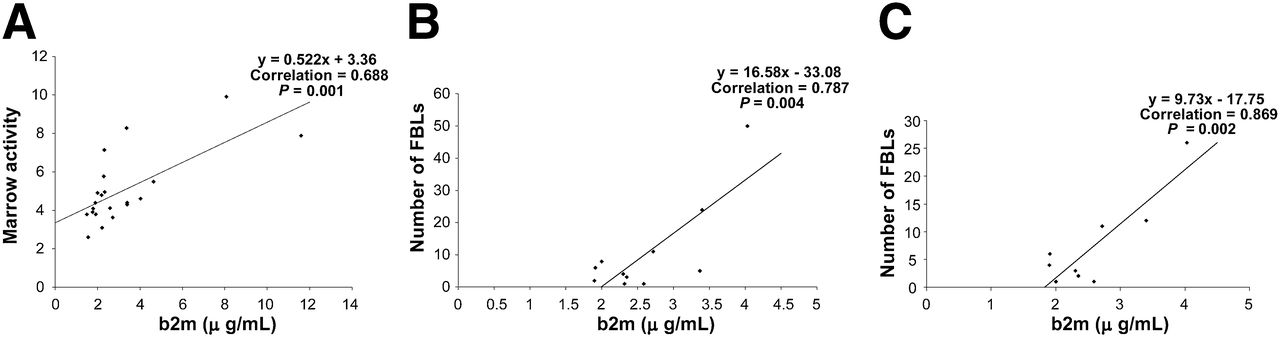
For the assessment of plasma cell burden by PET/CT, only 3 of 6 parameters—11C-acetate general marrow activity, 11C-acetate focal bone lesion number, and 18F-FDG focal bone lesion number—had a significant correlation with serum b2m level (Fig. 3).

Strong correlation between serum b2m level and 11C-acetate general marrow activity (A), 11C-acetate focal bone lesion number (B), and 18F-FDG focal bone lesion number (C). FBL = focal bone lesion.
Table 2 compares the clinical and metabolic responses. Pearson analysis showed good correlation between clinical response and percentage change in 11C-acetate general marrow activity (correlation coefficient, 0.911; P = 0.002). Patient 18 had focal and diffuse MM with a large osteolytic lesion in the C2 vertebra on pretreatment 11C-acetate PET. On posttreatment imaging, both general marrow activity and focal bone lesions were normalized, consistent with clinical complete remission (Fig. 4). Because pretreatment 18F-FDG PET/CT was negative, it was suboptimal for treatment monitoring.
Clinical and Dual-Tracer PET/CT Treatment Responses

(A and B) Patient 18 with focal and diffuse MM avid for 11C-acetate (arrows, A) but not for 18F-FDG (B). (C and D) Negative findings on posttreatment 11C-acetate (C) and 18F-FDG (D) PET/CT.
DISCUSSION
Compared with other 18F-FDG PET studies (5,6,10), our study had a lower 18F-FDG sensitivity (58%) for 2 reasons. First, our population was composed of patients with a clinically more common mixture of symptomatic MM (mainly stage I), SMM, and MGUS, instead of purely symptomatic MM. Second, our threshold of 18F-FDG general marrow activity (3.03) for diffuse MM was statistically based on receiver-operating-characteristic analysis compared with a control group, instead of being only qualitative. Some investigators chose splenic activity as the 18F-FDG reference (10); however, in patients with hematologic diseases, the spleen is known to be affected by a variety of diseases.
Our study showed that 11C-acetate performs significantly better than 18F-FDG in the detection of both diffuse and focal MM and with higher metabolic intensity. As reported by studies with myeloma cell lines (11), de novo lipid synthesis is elevated in proliferating abnormal plasma cells for biochemical processes such as membrane phospholipid synthesis, DNA replication, apoptosis, energy conversion, redox balance in hypoxic states, and signal transduction. Therefore, the use of 11C-acetate in the assessment of MM seems well justified on biochemical grounds.
Bartel’s group (5) reported that the presence of more than three 18F-FDG–avid focal bone lesions is an independent predictor for survival and that resolution of 18F-FDG avidity after treatment predicted favorable survival. However, the lower sensitivity of 18F-FDG limits its role in treatment assessment. Since 11C-acetate has higher sensitivity for MM and the posttreatment change in 11C-acetate general marrow activity correlates well with clinical response, 11C-acetate has potential for treatment monitoring, especially for nonsecretory or oligosecretory MM. Pretreatment serum b2m is an indicator of tumor burden and a significant predictor of survival in MM patients (12). 11C-acetate, as a surrogate imaging marker, might be useful for risk stratification and prediction of survival.
CONCLUSION
This preliminary study suggests that metabolic characterization of MM in diagnosis, assessment of tumor burden, and monitoring of treatment response can be assessed more accurately by lipid metabolism with 11C-acetate than by glucose metabolism with 18F-FDG.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 27, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication August 20, 2013.
- Accepted for publication November 19, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}