


TO THE EDITOR: The unrivaled sensitivity of PET for imaging molecular interactions remains largely unexploited in oncology. At present, PET mainly uses 18F-labeled FDG PET to diagnose and stage cancer by imaging primary and macroscopic metastatic deposits. We wish to draw attention to the opportunity of extending the use of 18F-FDG PET to detect and quantify micrometastatic disease. The methodology we propose—using a PET scanner that covers the entire length of the patient and optimized tumor-to-background tissue contrast—will maximize the sensitivity of 18F-FDG PET, offering the best chance for detection and quantification of micrometastases.
For cancer patients in the adjuvant setting, clinical decisions after radical surgical treatment of the primary tumor are based on risk factors identified from the surgically removed primary tumor and regional nodes. Patients considered at risk of disease relapse are presumed to have micrometastatic disease occult to current detection methods: all are therefore treated with toxic adjuvant chemotherapy. Until imaging and staging methods are advanced enough to provide evidence of micrometastatic status, we are restricted to this masked treatment approach. Although this approach improves overall relapse and survival rates, the disadvantages are: first, risk overestimation leading to overtreatment; second, inability to define patients who do or do not benefit; third, inability to assess real-time treatment response; and fourth, treatment toxicity, especially long-term side effects. For example, in the United States over 140,000 patients are diagnosed each year with colorectal cancer. On the basis of indicators of statistical risk, approximately 27% of early-stage (I + II) and 61% of late-stage (III + IV) colorectal cancer patients receive chemotherapy in addition to surgery (1). Yet cure is likely in a large number without adjuvant treatment, as in stage III node-positive colon cancer, for which 44% of patients were reported disease-free 5 y after surgery alone (2). Furthermore, for those who experience the inconvenience and toxicity of adjuvant treatment, not until months later does it become apparent that many patients may not have benefited (3). A method to detect and quantify micrometastasis would therefore greatly affect the staging and management of patients in the adjuvant setting, supporting the rational assessment of adjuvant chemotherapy risk–benefit for individual patients and sparing unnecessary treatment morbidity and costs. Such a method could also be used to optimize patient response to chemotherapeutics on a personalized medicine basis and would additionally support the assessment of new anticancer drugs to accelerate their clinical development.
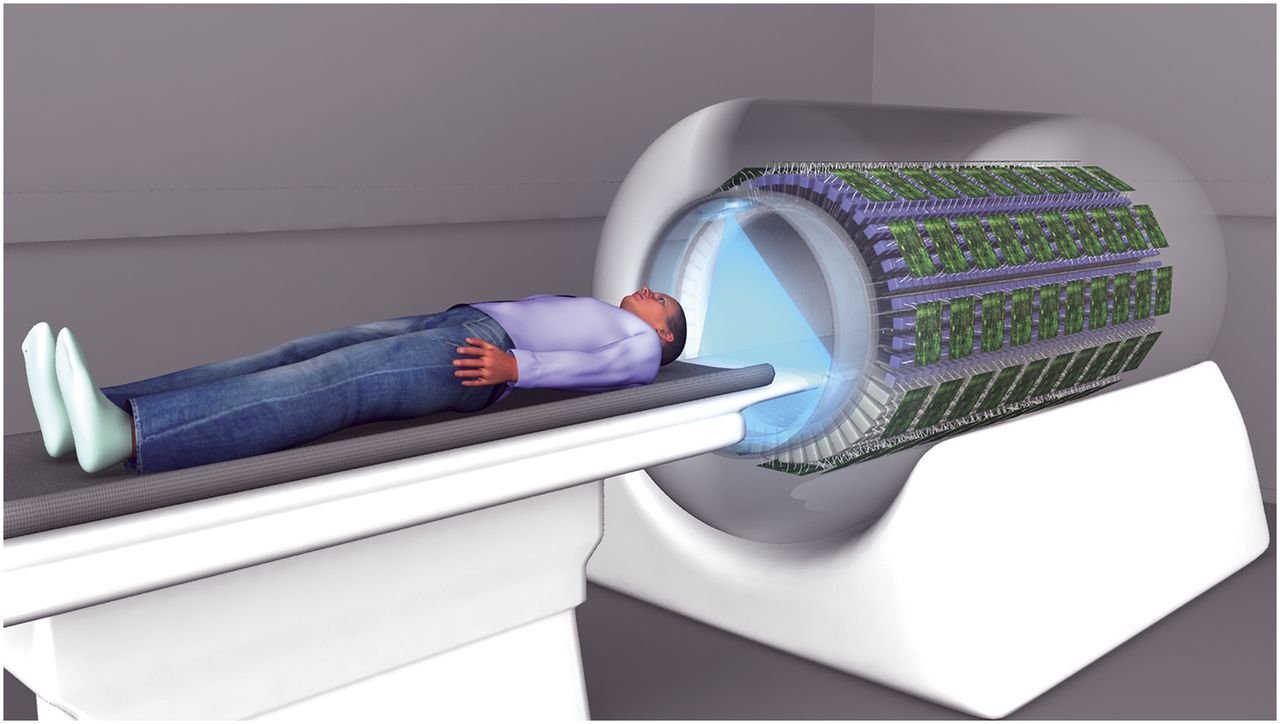
The clinical usefulness of 18F-FDG PET for macroscopic tumor detection has been restricted in oncology as a result of the limited sensitivity and specificity of the methodologies used (4). It is possible that MR imaging may supersede 18F-FDG PET for gross tumor localization, given its higher spatial resolution and radiation-free capabilities for measuring tumor glucose concentrations (5). However, the intrinsically higher sensitivity of PET for detecting low levels of tracer makes 18F-FDG PET better placed to detect microscopic disease. Nevertheless, improvements in sensitivity and specificity, and detection throughout the body, would be necessary. This need could be addressed in 2 ways. First, the contrast between tumor and background tissue may be increased by approximately 4-fold if the interval between administration of 18F-FDG and patient scanning is increased from the routinely used 60 min to about 300 min: this increase in the interval results in wider distribution of tracer, greater accumulation in tumor, extended renal excretion, and a higher washout from normal tissue (6,7). Second, the development of total-body PET—a 2-m-long tunnel of coincidence detectors operating in the time-of-flight mode (Fig. 1)—could significantly increase the efficiency of tracer detection compared with conventional PET scanning at equivalent injected doses (8,9). We propose an imaging protocol that would involve administering about 740 MBq (20 mCi) of 18F-FDG to a patient with an interval of 3 half-lives (∼330 min) before a total-body PET scan. Here it is predicted that the improvement in the quality of the image data would be equivalent to a 100-fold gain in noise-equivalent counts compared with using a conventional scanner and imaging at 60 min after tracer administration. This improvement results from the expected increase in contrast (6) combined with the improved detection efficiency of the total-body scanner (8,9) and accounts for the decay of the radiotracer during the extended uptake time. Therefore, we hypothesize that whole-body localization and quantification of microscopic disease should be possible—either as detectable hot spots or as raised mean levels of tissue and organ concentrations. Enhanced whole-body detection of highly differentiated tumor would be achieved, although assessment of global activity in common sites of metastasis, such as lymph basins, may be needed to ensure detection of early disease.

Challenges in quantifying tissue concentrations are expected using this paradigm but are considered surmountable—for example, resolution or contrast losses due to respiratory motion, and compensation of blood tracer activity remaining within the vasculature. To assess potential early microscopic disease presenting as raised mean tissue activity levels, time series scans and kinetic modeling methods may also need to be used and refined. The additional benefits of using kinetic analysis of serial 18F-FDG PET scans would be a gain in tumor glycolytic metabolism information relating to tumor biology and differentiation (e.g., by analyzing slope of 18F-FDG uptake over time), which could valuably increase the utility of the method for ultra staging, and thus patient management and adjuvant treatment decisions.
This proposed total-body PET-based imaging paradigm could offer the possibility of dramatically extending the proven sensitivity of 18F-FDG for tumor detection, enabling for the first time the geographic distribution and quantification of microscopic cancer throughout the body. This paradigm also offers the opportunity to obtain information to characterize tumor grade. Thus, 18F-FDG PET has the potential to become an efficient assessment tool for ultra staging, which could have a significant impact on primary and adjuvant therapy decisions, particularly if developed and used in combination with complementary assays of circulating tumor cells (10). In the adjuvant setting, this tool could meet the need for improved patient selection for, and individualized tailoring of, adjuvant therapy, providing significant patient and economic benefit.
Footnotes
Published online Mar. 6, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.





{kind=link}
Jump to section
Related Articles
Cited By...
- Development and Evaluation of mini-EXPLORER: A Long Axial Field-of-View PET Scanner for Nonhuman Primate Imaging
- Total-Body PET: Maximizing Sensitivity to Create New Opportunities for Clinical Research and Patient Care
- Total-body imaging: Transforming the role of positron emission tomography
- Molecular Imaging and Therapy with a Purpose: A Renaissance of Nuclear Medicine