


Abstract
Idiopathic pulmonary arterial hypertension (IPAH) results in increased right ventricular (RV) workload and oxygen demand. It has been shown that myocardial oxygen consumption (MVO2) of the hypertrophied right ventricle of IPAH patients can be measured using PET and 15O-labeled tracers. This method is, however, not very suitable for routine clinical practice. The purpose of the present study was to assess whether MVO2 can also be determined in the right ventricle of IPAH patients from the clearance of 11C-acetate, a simple method that is in use for MVO2 measurements of the left myocardium. Methods: Seventeen of 26 IPAH patients performed the total PET study. Nine other patients were scanned only for 11C-acetate. 15O-H2O, 15O-O2, and 15O-CO scans were used to derive RV flow, oxygen extraction fraction, and blood volume, respectively, from which RV MVO2 was calculated. The rate of clearance determined by monoexponential curve fitting (Kmono) and the efflux rate constant k2 were derived from the 11C-acetate scan. The RV rate–pressure product was also determined by means of right heart catheterization, as an index of the RV MVO2, and was calculated as the product of systolic pulmonary artery pressure and heart rate. Results: Both 11C-acetate clearance rates, Kmono (R2 = 0.41, P = 0.006) and k2 (R2 = 0.45, P = 0.003), correlated with RV MVO2. They also correlated with RV rate–pressure product (Kmono, R2 = 0.41, P = 0.0005; k2, R2 = 0.48, P < 0.0001). Conclusion: 11C-acetate clearance rates correlated moderately with quantitative RV MVO2 measurements in IPAH. Therefore, 11C-acetate PET can be used only as an index of RV oxidative metabolism in IPAH patients.
- 11C-acetate
- 15O
- PET
- monoexponential curve fitting
- pulmonary arterial hypertension
- right ventricle
- myocardial oxygen consumption
- rate–pressure product
The oxygen consumption (MVO2) of the normal right myocardium is less than that of the left heart as a result of a lower afterload (1). In idiopathic pulmonary arterial hypertension (IPAH), elevated pulmonary vascular resistance causes right ventricular (RV) hypertrophy and ultimately fatal RV failure. To gain insight on the pathophysiology of reduced pump function in the failing heart, quantification of MVO2 is important. A noninvasive method using state-of-the-art PET and 15O-labeled tracers has been validated as a means to measure MVO2 accurately (2–4). Using this method, it was recently demonstrated that the right ventricle consumes more oxygen in patients with severe IPAH than in those with mild PAH for generating similar RV power output (5). This method is, however, extensive and time-consuming (4), requiring 3 consecutive PET scans (15O-H2O, 15O-CO, and 15O-O2) and an on-site cyclotron to produce the short-lived 15O tracers (6). PET using 11C-acetate has been proposed as a more practical method to estimate MVO2. With 11C-acetate being the precursor of acetyl-CoA in the tricarboxylic acid cycle, the rate of 11C-acetate clearance determined by monoexponential curve fitting (Kmono) is closely related to MVO2 of the left heart (4,7–10).
It is not known, however, whether 11C-acetate can also be used to estimate RV MVO2. If so, the use of 11C-acetate PET would make future studies on oxidation in the failing right ventricle more convenient. Recently it was shown for the left ventricle that a single-compartment-model efflux rate constant (k2) correlated better with the rate–pressure product (RPP), a noninvasive index of myocardial oxygen demand, than Kmono (7). However, studies performing a direct comparison of MVO2 and different methods of 11C-acetate clearance determination in the human right ventricle are lacking. Therefore, the purpose of the present study was to assess whether the RV clearance rates of 11C-acetate correlate with RV RPP and the MVO2 (in standard units) of the hypertrophied right ventricle in IPAH patients. The MVO2 data have been presented previously to determine RV efficiency (5,11,12).
MATERIALS AND METHODS
Subjects
Twenty-six patients were included between April 2008 and November 2011. All patients had IPAH according to World Health Organization group I criteria with either New York Heart Association (NYHA) functional classification II or III–IV (13). The study was approved by the Medical Ethics Review Committee of the VU University Medical Center. All patients signed a written informed consent form. Seventeen patients had paired determinations of MVO2 obtained from 15O-labeled tracers and 11C-acetate clearance. For the other 9 patients, only an 11C-acetate scan was available and they were included in the correlation between 11C-acetate clearance rate and RPP. They did not undergo 15O scans because of logistic reasons (n = 3) or because they participated in another PET study (n = 6). All patients had clinically stable IPAH under optimal treatment, except for 2 patients who were newly diagnosed with IPAH NYHA class III and were included before treatment. The change in 6-min walk distance was less than 10% within 6 mo before inclusion. During the study, PAH therapy was continued, which was either single or combination treatment with intravenous prostacyclin, endothelin receptor antagonist, or phosphodiesterase-type 5 inhibition. Exclusion criteria were cardiovascular disease, atrial fibrillation, and anemia (hemoglobin < 12 g/dL). A control group was not included because the normal right myocardium is too thin to be measured reliably using PET and 15O tracers.
PET Scanning Protocol
Patients underwent the scanning protocol within 1 d, consisting of consecutively a 15O-H2O, 15O-O2, 15O-CO, and 11C-acetate scan under resting conditions (ECAT EXACT HR+; Siemens/CTI) or a hybrid PET/CT scan (Gemini TF 64; Philips Healthcare). After a light breakfast 2 h before the first scan, patients fasted until the end of the scanning protocol. The 15O scan protocol has been described previously (5,11,12), and a brief description can be found in the supplemental material (available online at http://jnm.snmjournals.org). After the last 15O PET scan and a 2-h break, the patients were repositioned on the scanner bed for a 48-min dynamic emission scan (29 frames) after an intravenous injection of 300 MBq of 11C-acetate in 3-dimensional acquisition mode (7). Six patients had a slightly modified imaging protocol (with the hybrid PET/CT scanner) using a dose of 370 MBq of 11C-acetate followed by a 3-dimensional 50-min dynamic PET acquisition (36 frames). This was followed by a low-dose CT scan (35 mAs) for attenuation correction. Systemic blood pressure, peripheral saturation, and heart rate were monitored at set intervals during the protocol.
Data Analysis
Analysis of 15O data has been described in detail previously (5,12,14), and a brief description can also be found in the supplemental material. For the present study, the volume of interest was the RV free wall, excluding the septum. 11C-acetate data analysis also has been described previously (7). In brief, a summed image (from 3 to 5 min after injection) was used to reslice the dynamic scan and to define regions of interest for the RV free wall. The 11C-acetate time–activity curve was analyzed by fitting the clearance phase to a single exponential, providing the clearance rate Kmono (min−1) (7). In addition, the entire 11C-acetate time–activity curve was fitted to a single-tissue-compartment model as proposed by Van den Hoff et al. (15). This model takes into account both influx and efflux of the tracer and the rate constant k2 (min−1), reflecting the oxidative flux through the tricarboxylic acid cycle (7). In this analysis, corrections were applied for both spillover from blood to myocardium and partial-volume effects (7). In addition, data reported by Sun et al. (8) were used to apply an average metabolite correction to the 11C-acetate arterial input function.
RV Hemodynamics
RV hemodynamics were obtained during right heart catheterization and cardiac MR imaging within 1 wk of the PET study when possible, according to procedures described previously (16). In 3 subjects, for logistic or personal reasons, the interval was 20–55 d between right heart catheterization and PET and 20–36 d between cardiac MR imaging and PET. Because these patients had stable IPAH under drug treatment, the interval was considered acceptable (12). RV RPP, commonly used as an index of myocardial oxygen demand, is defined as the product of systolic pulmonary arterial pressure and heart rate (5). Stroke work index was calculated as the product of stroke volume index and (mean pulmonary arterial pressure − mean right atrial pressure) (17).
Some fluctuation in pulmonary arterial pressure and heart rate may be present within hours to days and will contribute to the variance in the relationships presented in Figures 1 and 2 and Supplemental Figure 1. It can be assumed, however, that variability of pulmonary arterial pressure was relatively small within the study window, given the significant correlation between systolic pulmonary arterial pressure measured 1 d before the PET study and MVO2 determined during the PET study (5). Within the study period, mean heart rate varied between 60 and 105 bpm, based on 3 separate measurements in 23 of the 26 IPAH patients. The median coefficient of variation of heart rate in these patients was small (4.8%). In addition, heart rate variation did not affect the significance of correlations with RPP.

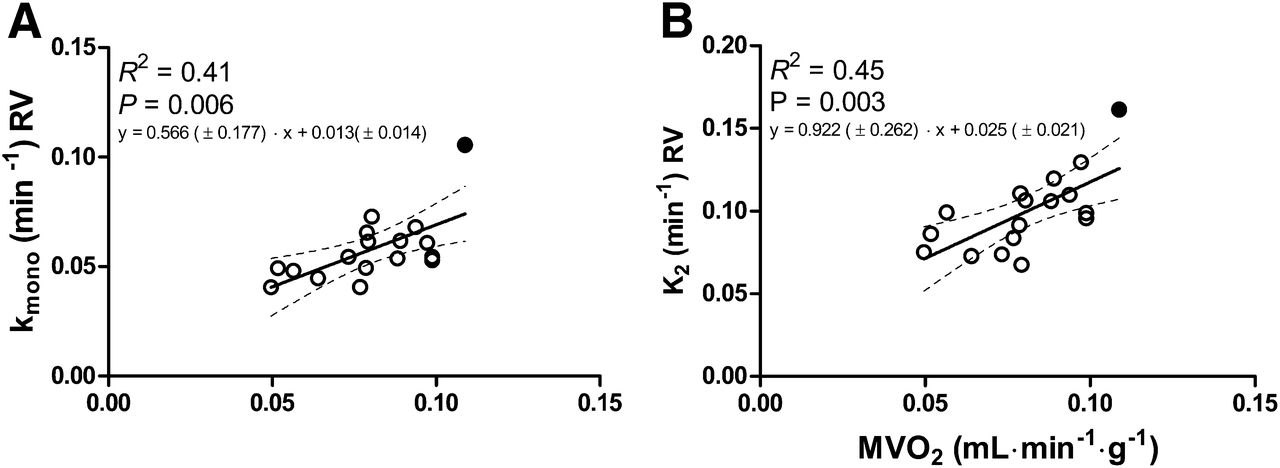
(A) Kmono and (B) tissue-to-plasma efflux rate constant of 11C-acetate as function of RV MVO2. Best fit is represented by thick line. Thinner broken lines represent 95% confidence interval. Equation of regression line is shown within panels (±SE). n = 17 IPAH patients. Treatment-naïve patient is shown as black dot.
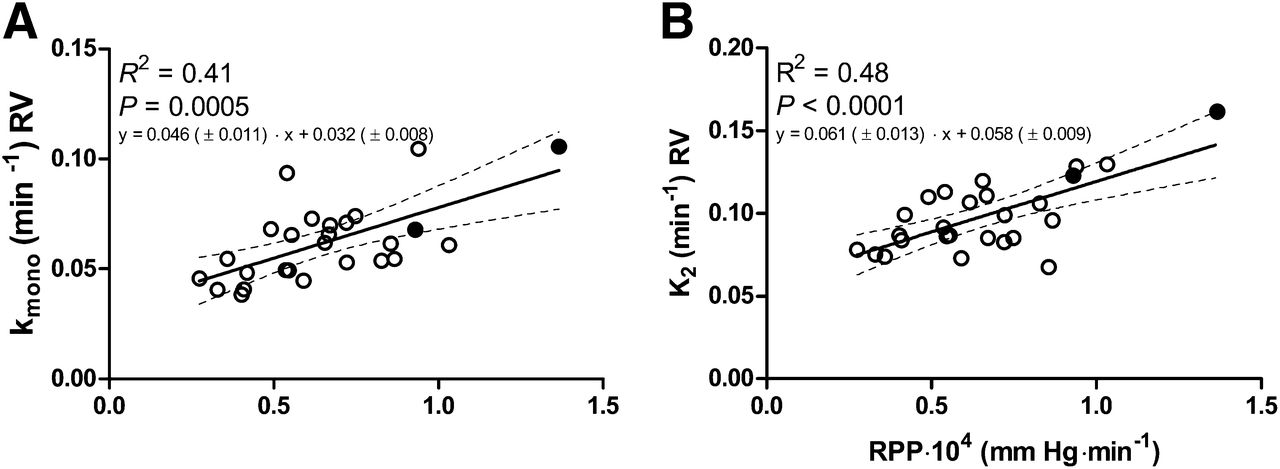
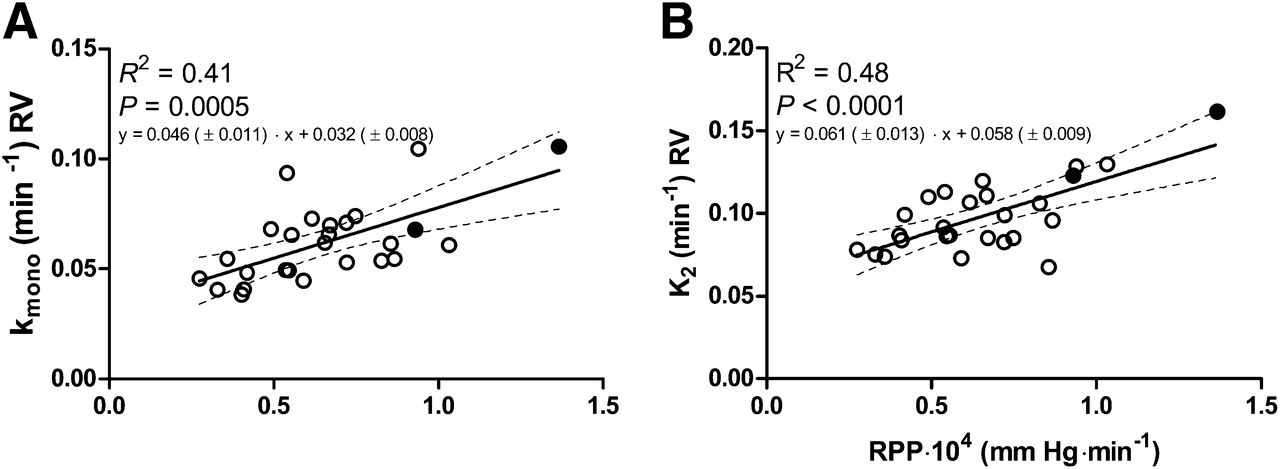
(A) Kmono and (B) tissue-to-plasma efflux rate constant of 11C-acetate as function of RPP. Best fit is represented by thick line. Thinner broken lines represent 95% confidence interval. Equation of regression line is shown within panels (±SE). n = 26 IPAH patients. Two treatment-naïve patients are shown as black dots.
Statistical Analyses
All results are expressed as mean ± SD, with ranges given in the tables. Linear regression analysis was used (Prism 5 for Windows; GraphPad Software). A P value of less than 0.05 was considered statistically significant.
RESULTS
In total, 26 patients (25 women and 1 man) were included. Two of the patients were newly diagnosed with NYHA functional classification III–IV IPAH and were treatment-naïve at the time of inclusion. As such, the study population comprised severely ill patients on the one hand and clinically stable patients on the other hand, resulting in heterogeneity of patient characteristics and hemodynamics (e.g., 6-min walk distance, cardiac output, and RV ejection fraction) (Table 1). The age range was also large. Table 2 summarizes RPP and PET-derived measures of RV MVO2. There was a significant correlation between Kmono and MVO2 (Fig. 1A). A similar correlation was found between k2 and RV MVO2 (Fig. 1B). Kmono and k2 also correlated significantly with RPP (Figs. 2A and 2B). There was no significant correlation between stroke work index and either Kmono or k2 (R2 = 0.06, P = 0.22, and R2 = 0.11, P = 0.11, respectively).
Clinical Characteristics and Hemodynamics at Time of Inclusion
RPP and PET-Derived Measures of RV MVO2
DISCUSSION
The main findings of this study are that the rate of clearance of 11C-acetate correlates with both MVO2, as measured using PET and 15O-labeled tracers, and RPP in the hypertrophied RV wall of IPAH patients, with little difference between Kmono and k2.
The significant correlation between 11C-acetate clearance rate Kmono and MVO2 in the hypertrophied right ventricle is in agreement with previous studies on the left myocardium in both control subjects (r = 0.71, P = 0.02) and patients with chronic myocardial infarction (r = 0.89, P < 0.001) (4,7–10).
Little is known about the rate of clearance of 11C-acetate from the normal right ventricle. Two previous studies reported a mean Kmono value of 0.040 ± 0.003 min−1 and 0.043 ± 0.009 min−1 in the normal right ventricle of control subjects, versus patients with heart failure or dilated cardiomyopathy, who had a mean Kmono of 0.055 ± 0.005 min−1 and 0.051 ± 0.007 min−1, respectively (9,18). It has been proposed that the higher clearance rate of 11C-acetate in these patient groups with left heart failure is likely due to an increased RV workload in left ventricular (LV) heart failure—that is, due to secondary pulmonary hypertension (9). In addition, Ukkonen et al. demonstrated in patients with congestive heart failure that higher oxidative metabolism in the right ventricle relative to that in the left ventricle was related to an increased ventilatory drive, reflected by the slope of increase of ventilation relative to carbon dioxide production, which in turn was associated with increased mortality in these patients (19). Therapeutic interventions for LV heart failure, such as exercise training in dilated cardiomyopathy patients, were shown to also have a positive effect on RV oxidative metabolism, with a significant reduction of RV Kmono (20). Similarly, cardiac resynchronization therapy in patients with idiopathic dilated cardiomyopathy also enhanced RV oxidative metabolism and metabolic reserve during stress (21). Despite differences in patient population and methodology, RV Kmono values in the present IPAH patients are in agreement with these previous studies, reflecting increased oxygen demand of the right myocardium as a result of increased afterload in IPAH.
Previously, a significant correlation between MVO2 and RPP of the total RV wall (R2 = 0.55, P = 0.0004) in IPAH patients was demonstrated (5).
Caution is needed when the 11C-acetate clearance rate is used for absolute quantification of MVO2. Clearance of 11C-acetate can be affected by metabolic shifts in remodeling RV myocardium in IPAH, because in the failing myocardium, other processes may result in an uncoupling between MVO2 and adenosine diphosphate phosphorylation—for example, by increased production of NO and reactive oxygen species (22). The assumed tight coupling of the rate of clearance of acetate via the tricarboxylic acid–to–oxygen use in the respiratory chain, as found in the normal heart, may be absent in diseased myocardium. In such cases, 11C-acetate clearance may severely overestimate adenosine triphosphate resynthesis and underestimate MVO2. On the other hand, earlier studies with healthy volunteers and experimental canine studies showed that changes in the availability of myocardial metabolic substrates or ischemia, without changes in hemodynamics, did not affect LV 11C-acetate kinetics, with similar relationships between Kmono and either MVO2 or RPP at normal baseline conditions (23–25).
In the left ventricle of healthy volunteers, Timmer et al. (7) found an improved correlation between LV RPP and the 11C-acetate clearance k2 (r = 0.75, P < 0.001), as compared with the correlation with Kmono (r = 0.46, P = 0.047). Here, we show that the correlation between k2 and RV RPP was only slightly better than that between Kmono and RV RPP (R2 = 0.49 vs. R2 = 0.41, respectively, Fig. 2). For the left ventricle in the present study population, we found no significant correlations between k2 or Kmono and LV RPP (Supplemental Table 1; Supplemental Figs. 1C and 1D). On the one side, our patient population showed a narrow range of RPP for the left ventricle under resting conditions. On the other side, the failing right ventricle in IPAH results in lower workload for the left heart, which itself may cause altered LV metabolism and mechanical efficiency. A recent study demonstrated that LV cardiomyocytes are atrophic because of unloading and reduced cardiac output in RV failure secondary to chronic thromboembolic pulmonary hypertension (26). It is possible that LV cardiomyocyte atrophy is also present in IPAH, causing smaller differences in LV oxidative metabolic levels and resulting in a lack of correlations between 11C-acetate clearance and LV RPP.
There were several limitations in our study. Measurement error as a result of performing the scanning protocols not simultaneously but in 2 sessions on the same day was unavoidable but may be important. The patient position in the scan may not have been exactly the same in the 2 sessions. Furthermore, there is a possibility that the myocardial metabolism may have altered during the day, as the 15O PET scans were performed 2 h after a light meal whereas the 11C-acetate PET scan was obtained about 6 h later. The protocol was, however, too extensive to have the patients remain fasting from the midnight before the scanning day till the end of the PET study. The protocol was standardized as much as possible to limit measurement error. In the present study, test–retest variability was not investigated, as adding a scan was not feasible for the present patient population. The reproducibility of 11C-acetate clearance rate measurements in humans has been demonstrated by Armbrecht et al. (24). The fact that the measurement of pulmonary artery pressure and heart rate for the calculation of RPP was performed on another day may also have contributed to error variance. Finally, we focused only on myocardial metabolic measurements under resting conditions. It is possible that other correlations would appear during exercise or if inotropic drugs were used. Unfortunately, the demanding study protocol and the severity of the disease did not allow strenuous exercise or medical interventions.
CONCLUSION
Clearance of 11C-acetate, expressed as either Kmono or k2, correlated with quantitative RV MVO2 and RPP measurements in the hypertrophied right myocardium of IPAH patients significantly, albeit moderately. Given the moderate correlation between RV 11C-acetate clearance with RV MVO2 and RPP, it must be concluded that the 11C-acetate clearance rate is only an index of RV oxidative metabolism in IPAH patients, which can potentially be used to monitor the efficacy of therapy in IPAH patients.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported in part by the Netherlands Organization for Scientific Research (VIDI 917.96.306). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 4, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication October 18, 2012.
- Accepted for publication February 13, 2013.





{kind=link}
{kind=link}