


Abstract
All patients with primary hyperparathyroidism should undergo localization studies before reoperation, but it is not known which method is most accurate. The purpose of this prospective study was to compare the performance of planar scintigraphy with 123I/99mTc-sestamibi, 99mTc-sestamibi SPECT (SPECT/CT), 11C-methionine PET/CT, and selective venous sampling (SVS) in persistent primary hyperparathyroidism. Methods: Twenty-one patients referred for reoperation of persistent hyperparathyroidism were included and investigated with 123I/99mTc-sestamibi, SPECT/CT (n = 19), 11C-methionine PET/CT, and SVS (n = 18) before reoperation. All patients had been operated on 1–2 times previously because of hyperparathyroidism. The results of the localization studies were compared with operative findings, histology, and biochemical cure. Results: Eighteen (86%) of 21 patients were biochemically cured. Nineteen parathyroid glands (9 adenomas, 1 atypical adenoma, and 9 hyperplastic glands) were removed from 17 patients, and 1 patient who was biochemically cured had an unclear histology result. The accuracy for localizing a pathologic parathyroid gland to the correct side of the neck was 59% (95% confidence interval [CI], 36%–79%) for 123I/99mTc-sestamibi, 19% (95% CI, 5%–42%) for SPECT/CT, 65% (95% CI, 43%–84%) for 11C-methionine PET/CT, and 40% (95% CI, 19%–65%) for SVS (P < 0.01 for 123I/99mTc-sestamibi vs. SPECT/CT). The corresponding accuracy for the correct quadrant or more specific site was 48% (95% CI, 27%–69%) for 123I/99mTc-sestamibi, 14% (95% CI, 3%–36%) for SPECT/CT, 61% (95% CI, 39%–80%) for 11C-methionine PET/CT, and 25% (95% CI, 9%–49%) for SVS (P < 0.02 for 123I/99mTc-sestamibi vs. SPECT/CT). In the 3 patients not cured, preoperative 123I/99mTc-sestamibi and SPECT/CT remained negative, SVS was false predictive in all, and 11C-methionine PET/CT in 1. 11C-methionine PET/CT accurately revealed the pathologic gland in 4 of 8 (50%) patients with a negative 123I/99mTc-sestamibi scan result, all of whom were biochemically cured after reoperation. Conclusion: Planar scintigraphy with 123I/99mTc-sestamibi performs well in complicated primary hyperparathyroidism and is recommended as first-line imaging before reoperation. 11C-methionine PET/CT provides valuable additional information if 123I/99mTc-sestamibi scan results remain negative. 99mTc-sestamibi SPECT/CT and SVS provide no additional information, compared with the combined results of 123I/99mTc-sestamibi and 11C-methionine PET/CT imaging.
- primary hyperparathyroidism
- persistent
- reoperation
- 123I/99mTc-sestamibi
- SPECT-CT
- 11C-methionine PET/CT
- selective venous sampling
- PTH
Primary hyperparathyroidism is a common endocrine disease, with a peak incidence in women aged 50–60 y (1). It is explained by a single parathyroid adenoma in 80%–85% of patients, double adenomas in about 4%, and parathyroid hyperplasia in 15%–20% of cases. Parathyroid carcinoma is rare and accounts for about 1% of cases. Despite excellent surgical results in experienced centers, approximately 2%–7% of patients will require reoperation because of persistent or recurrent hyperparathyroidism after primary surgery (2–4). Revision surgery is a far greater challenge because of distortion and scarring caused by previous interventions. The likelihood of supernumerary parathyroid glands and ectopic localization is increased and the complication rate markedly higher. Because of the difficulty in safely identifying and resecting abnormal parathyroid glands in the reoperative setting, consensus exists that preoperative localization studies should be performed before reoperation (5–7). Selective venous sampling (SVS) of parathyroid hormone (PTH) (8) has been the gold standard but is invasive. Of the several imaging procedures that have been developed, 99mTc-sestamibi scintigraphy is available in most centers, and performance can be improved by additional imaging of thyroid tissue with 123I-labeled sodium iodide (9,10). The performance of SPECT with 99mTc-sestamibi as the tracer can be improved by combining it with CT (SPECT/CT) (11). The accuracy of 11C-methionine PET, which was successful for localization of persistent or recurrent hyperparathyroidism in a small series (12), can also be improved by integrated CT (PET/CT). Although 99mTc-sestamibi SPECT/CT, 11C-methionine PET/CT, and SVS all were considered useful and of additive value in the reoperative setting of hyperparathyroidism (13,14), the performance of different localization techniques have not been directly compared in a prospective setting before reoperation of complicated primary hyperparathyroidism. The aim of the present prospective study was, therefore, to compare the performance of 123I/99mTc-sestamibi scintigraphy, 99mTc-sestamibi SPECT/CT, 11C-methionine PET/CT, and SVS in patients referred for reoperation of persistent hyperparathyroidism and relate the results to operative findings, histology, and biochemical cure.
MATERIALS AND METHODS
Patients
This was a prospective study of 21 patients referred to the Helsinki University Central Hospital because of persistent primary hyperparathyroidism. Characteristics of the patients are given in Table 1. None of the patients had multiple endocrine neoplasia type 1 or 2. All patients had been operated on at least once previously for primary hyperparathyroidism (range, 1–2) and had undergone some kind of imaging before the first operations (Table 1). Three patients had also undergone previous thyroid surgery (Table 1). None of the patients fulfilled the criteria for cure of hyperparathyroidism on the first postoperative day (normal serum Ca-ion concentration and ≥50% decrease in plasma PTH concentration, compared with preoperative concentration) after the first 1–2 operations. Hyperparathyroidism persisted in all patients on follow-up, and the patients were evaluated for reoperation. The indications for reoperation are given in Table 1. Patients were prospectively investigated with 123I/99mTc-sestamibi, 99mTc-sestamibi SPECT/CT (n = 19), 11C-methionine PET/CT, and SVS (n = 18) and thereafter operated on again. The results of the localization studies were compared with operative findings, histology, and biochemical cure. The study was conducted according to the guidelines of the Declaration of Helsinki, and the study protocol was approved by the institutional review board. All patients gave written informed consent before participating in the study. All laboratory tests were performed at the Helsinki University Central Hospital Laboratory using standard methods. Blood tests were performed in the morning in the fasting state.
Characteristics of Primary Hyperparathyroid Patients
Localization Studies
Planar scintigraphy with 123I/99mTc-sestamibi, 99mTc-sestamibi SPECT/CT (n = 19), 11C-methionine PET/CT, and SVS (n = 18) localization studies were performed before reoperation. The results of the localization studies were reviewed by 5 readers.
123I/99mTc-sestamibi and 99mTc-sestamibi SPECT/CT studies were performed according to the 2009 guidelines of the European Association of Nuclear Medicine (15), after a 2-h fast. A 123I-iodide capsule of 13.7–15.3 MBq (mean ± SD, 14.5 ± 0.49) was administered orally 3 h before the imaging. Immediately after the planar 123I imaging, 714–941 MBq (mean ± SD, 842 ± 57.1) of 99mTc-sestamibi were intravenously injected, and an early planar acquisition was initiated 5 min thereafter. A dual-energy-window procedure was used to acquire simultaneous imaging of both radiopharmaceuticals. A late planar imaging with identical energy window settings was performed 2 h after the first imaging and was followed by a SPECT/CT acquisition from the thyroid area. Imaging was performed with 2 γ-cameras. A triple-head Prism 3000XP (Picker) γ-camera equipped with a low-energy general all-purpose collimator was used for planar imaging of 6 patients. The image matrix was 256 × 256. Window settings were 140 keV ± 8% for 99mTc and 159 keV ± 7% for 123I. An Infinia SPECT/CT device (GE Healthcare) equipped with a low-energy high-resolution parallel-hole collimator was used for planar imaging of 15 patients. The images were acquired using a zoom of 1.6 and a 256 × 256 matrix. Window settings were 140 keV ± 7% for 99mTc and 159 keV ± 5% for 123I.
SPECT/CT was performed with the Infinia. A 99mTc window setting (140 keV ± 10%) was used for SPECT acquisition of 60 projections with 30-s acquisition times. CT slices (10 mm thick) were acquired (2.5 mA; 140 kV; dose–length product 127 mGy × cm) and used for attenuation correction of SPECT images.
Early and late planar 99mTc and 123I window images were transferred to an Odyssey FX computer (Picker). The images were normalized using manually delineated thyroid area regions of interest. Subtraction images, in which 123I images were subtracted from 99mTc-sestamibi images, were calculated from early and late images.
11C-methionine PET/CT imaging was performed with the Discovery PET/CT VCT (GE Healthcare) at the Turku PET Centre. Patients fasted for 6 h before the study. The dose of intravenous 11C-methionine was 440 MBq. Approximately 20 min after injection, static PET/CT imaging in 3-dimensional mode covering the head and neck and mediastinum (4-min emission scans per position) was started. Attenuation correction was performed using a low-dose CT protocol (80 mAs, 140 kV). Transaxial, coronal, and sagittal images for visual analysis of the data were corrected for dead-time, decay, and photon attenuation and reconstructed in a 128 × 128 matrix. Images were reconstructed using 2 iterations and 28 subsets with a postprocessing filter of 6.0 mm in full width half maximum and a fully 3-dimensional maximum-likelihood ordered-subset expectation maximization reconstruction algorithm. In the cases showing corresponding anatomic findings on CT scans, any focal tracer accumulation exceeding normal regional tracer uptake was considered pathologic around the thyroid or mediastinum. PET images were analyzed visually.
PTH venous sampling was performed at the Helsinki University Central Hospital by an experienced intervention radiologist through the femoral vein (2). Nineteen samples were taken from each patient at fixed positions in the different veins. Serum samples from each individual investigation were analyzed for PTH in the same batch. SVS was considered positive when there was a 2-fold increase in PTH in one sample, with an elevated but decreasing concentration in a second adjacent sample in the direction of venous blood flow. The venous sampling results were interpreted by 3 investigators to categorize a patient into 1 of 6 groups or a combination of these groups: right side of the neck, left side of the neck, upper thyroid region, lower thyroid region, thymic-mediastinal region, or other ectopic region. If there was no positive gradient, SVS was categorized as negative.
Surgery and Histology
Reoperation was performed on each patient by an experienced parathyroid surgeon at the Helsinki University Hospital between November 2009 and February 2012. Patient 17 was operated on at a different hospital. On the basis of preoperative localization studies, a sternotomy was performed in addition to neck surgery for patient 10; a thoracic surgeon participated in this operation. Both previously removed parathyroid glands and the tissue and glands removed during reoperation were reexamined by an experienced pathologist.
Statistical Analysis
The results are expressed as mean and SD, unless otherwise stated. Differences between pre- and postsurgery laboratory measurements were examined with a Wilcoxon signed-rank test for plasma PTH and Student t test for serum Ca-ion. Planar scintigraphy with 123I/99mTc-sestamibi was considered the reference localization technique. SVS, SPECT/CT, and 11C-methionine PET were compared with the reference method. A McNemar test was used to compare accuracies between the different localization techniques with regards to the correct side of the neck (right or left) and the correct quadrant (right upper, right lower, left upper, and left lower) or other more specific localization (i.e., intrathyroidal, mediastinal). A finding was considered accurate if the lesion detected by the localization technique could be anatomically verified and removed by the surgeon, it was histologically confirmed as an adenoma or hyperplasia, and the patient was biochemically cured. Findings that were not verified on surgery or histologically, or findings that did not result in biochemical cure after operation of the corresponding site, were considered false predictive (i.e., not accurate). Because all patients had biochemical evidence of the disease, preoperative localization studies that remained negative were considered false-negative (i.e., not accurate). Cohen’s κ-coefficient was determined to quantify agreement of accuracies between the techniques. P values of less than 0.05 were considered statistically significant. The SAS software (version 9.2; SAS Institute Inc.) was used for the statistical analysis.
RESULTS
Biochemical Cure and Other Laboratory Characteristics
Both serum Ca-ion (1.46 ± 0.09 vs. 1.25 ± 0.10 mmol/L; reference interval, 1.16–1.30 mmol/L) and plasma PTH concentrations (169 ± 95 vs. 48 ± 64 ng/L; reference interval, 8–73 ng/L) decreased significantly after reoperation (both P < 0.0001). Eighteen (86%) of 21 patients were biochemically cured after reoperation. In the 3 patients with persistent disease after reoperation (Table 2; patients 3, 8, and 15), the thyroid or no tissue was removed. Preoperative 123I/99mTc-sestamibi and SPECT/CT results were negative in all of these patients, whereas SVS was false predictive in all and 11C-methionine PET/CT in 1 (patient 8).
Results of Localization Studies, Operative and Histologic Findings, and Biochemical Cure in Patients Undergoing Reoperation
Surgical and Histologic Findings
None of the patients experienced any surgical complications after reoperation. Nineteen parathyroid glands were surgically removed from 17 patients who were biochemically cured. In addition, 1 of the 18 biochemically cured patients had an unclear histology result (Table 2; patient 19). Nine of the surgically removed glands represented adenomas, 1 atypical adenoma, and 9 hyperplasia (Table 2). In 7 patients (patients 1, 4, 6, 12, 16, 20, and 21), most of the localization studies implicated a pathologic finding in the right lower quadrant; in 5 of these patients, the operative finding was compatible with the right inferior parathyroid, and in 2 patients (patients 4 and 21) with an aberrantly low location of the right upper parathyroid gland. In 3 patients (patients 5, 9, and 13), a pathologic gland was removed from the right upper quadrant; 1 of these patients (patient 9) had an additional pathologic parathyroid gland removed from the left upper quadrant. In patient 9, only 123I/99mTc-sestamibi revealed a pathologic focus on both sides of the neck (Table 2). One other patient (patient 18) also had 2 hyperplastic glands removed, the left upper and lower parathyroid glands. However, none of the imaging techniques correctly identified both pathologic glands in this patient (Table 2). In 3 patients (patients 7, 11, and 14), the surgeon removed a pathologic parathyroid gland from the left lower quadrant; in one of these patients (patient 11) the gland was located in the carotid sheath and in one patient (patient 14) exploration was successful despite the fact that none of the localization studies identified the correct side (Table 2). In 2 patients (patients 2 and 6), the pathologic parathyroid gland was located within the thyroid gland and in 2 patients (patients 10 and 17) in the mediastinum (Table 2).
Localization Studies
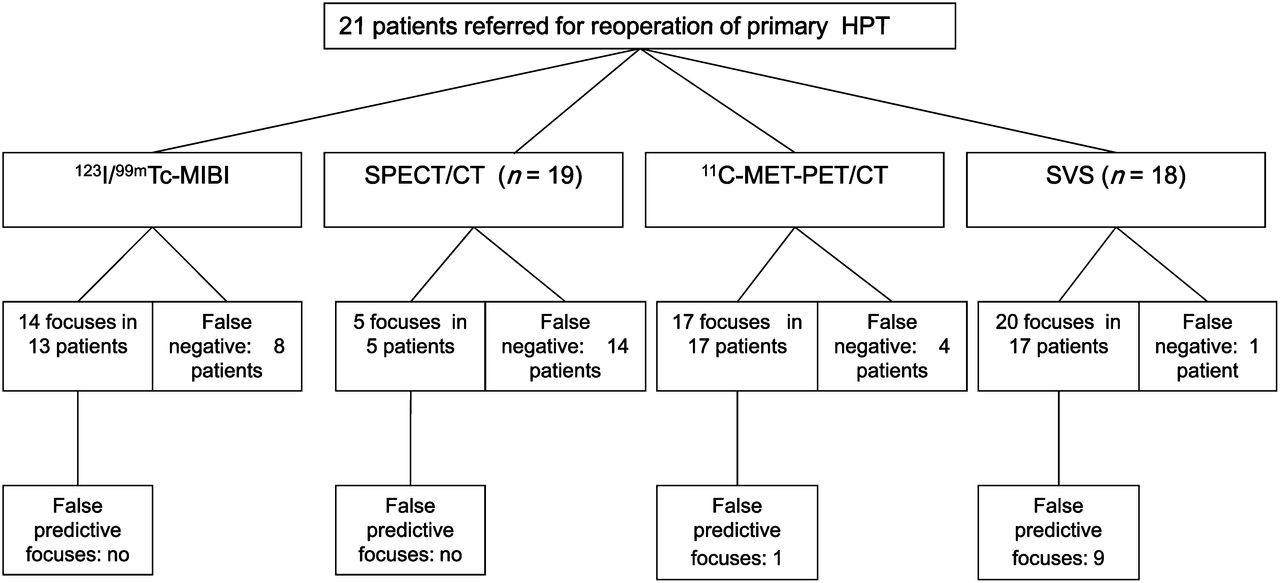
The total number of focuses detected with the different techniques, number of false-negative localization studies, and false predictive findings are shown in Figure 1. In 1 patient (patient 4), all localization techniques correctly identified the pathologic parathyroid gland (Fig. 2). 123I/99mTc-sestamibi was the only technique that accurately detected 2 pathologic parathyroid glands in patient 9, whereas none of the techniques accurately identified both pathologic glands in patient 18 (Table 2). 11C-methionine PET/CT correctly identified 4 pathologic focuses in 4 patients who were biochemically cured after reoperation and for whom the other imaging techniques remained negative (Table 2; patients 5, 13, 17, and 19; Fig. 3). 123I/99mTc-sestamibi was more accurate than SPECT/CT; Figure 4 demonstrates an example of this. This patient had a parathyroid adenoma located within the right thyroid lobe (Table 2; patient 6). Accuracies of the preoperative localization techniques for indicating the correct side of the neck and a correct more specific site are given in Table 3. In patients with persistent disease after reoperation (Table 2, patients 3, 8, and 15), preoperative 123I/99mTc-sestamibi and SPECT/CT results remained negative, whereas SVS and 11C-methionine PET were false predictive in 3 of 3 and 1 of 3 patients, respectively. Neither SPECT/CT nor SVS was of additional value, compared with the combined results of 123I/99mTc-sestamibi and 11C-methionine PET imaging.
Accuracy of Preoperative Localization Studies

Summary of findings detected by 4 different localization techniques before reoperation of primary hyperparathyroidism. HPT = hyperparathyroidism.
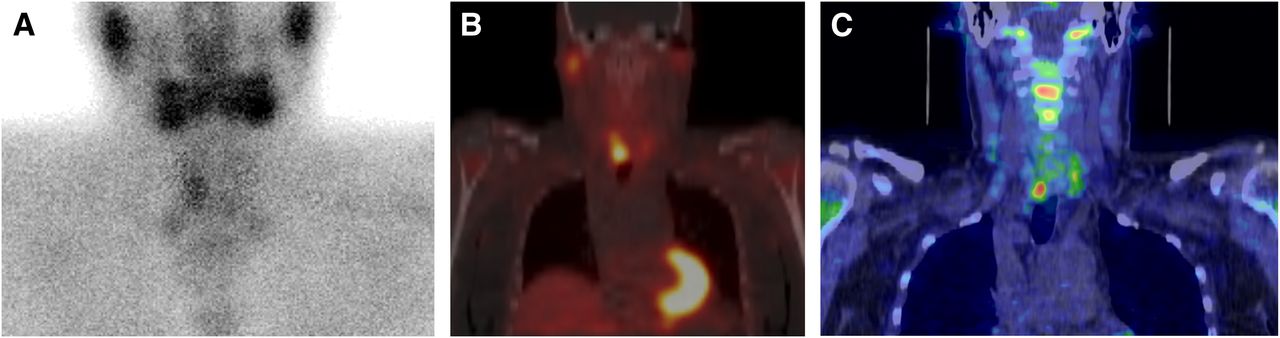
In patient 4, preoperative 123I/99mTc-sestamibi (A), 99mTc-sestamibi SPECT/CT (B), 11C-methionine PET/CT (C), and SVS (data not shown) all correctly localized pathologic parathyroid gland to right lower quadrant. Histology demonstrated parathyroid glandular hyperplasia.
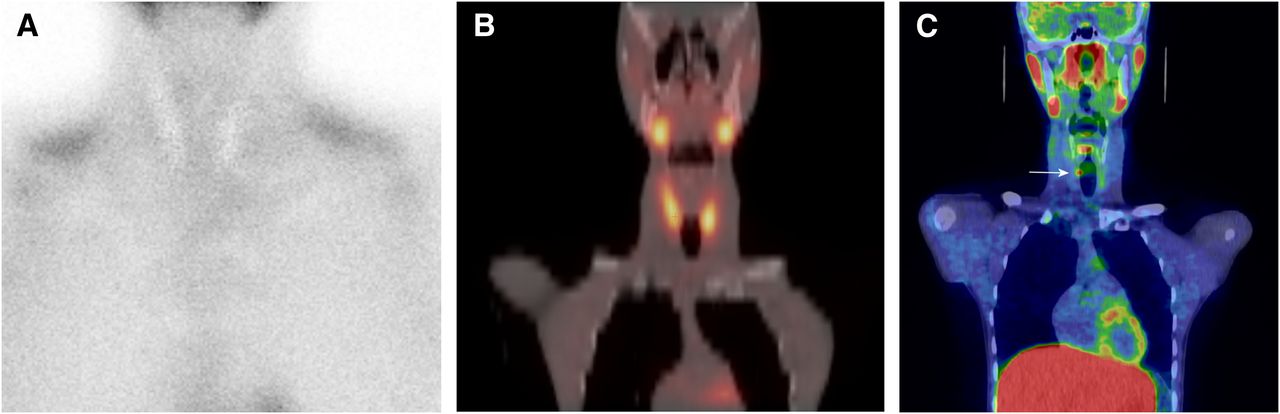
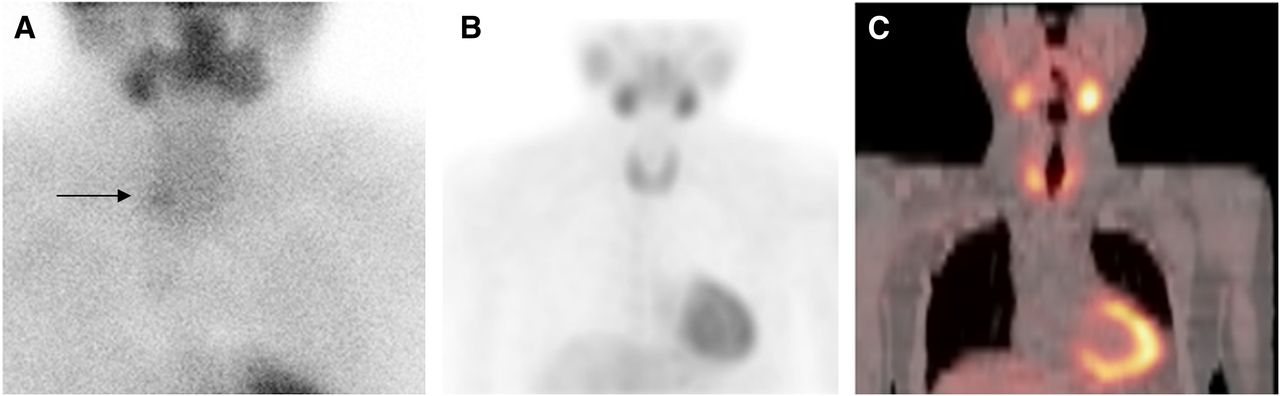
In patient 5, preoperative 123I/99mTc-sestamibi (A), 99mTc-sestamibi SPECT/CT (B), and SVS (data not shown) all remained negative. 11C-methionine PET/CT (C) correctly localized pathologic parathyroid gland (arrow) to right lower quadrant. Histology revealed atypical parathyroid adenoma.
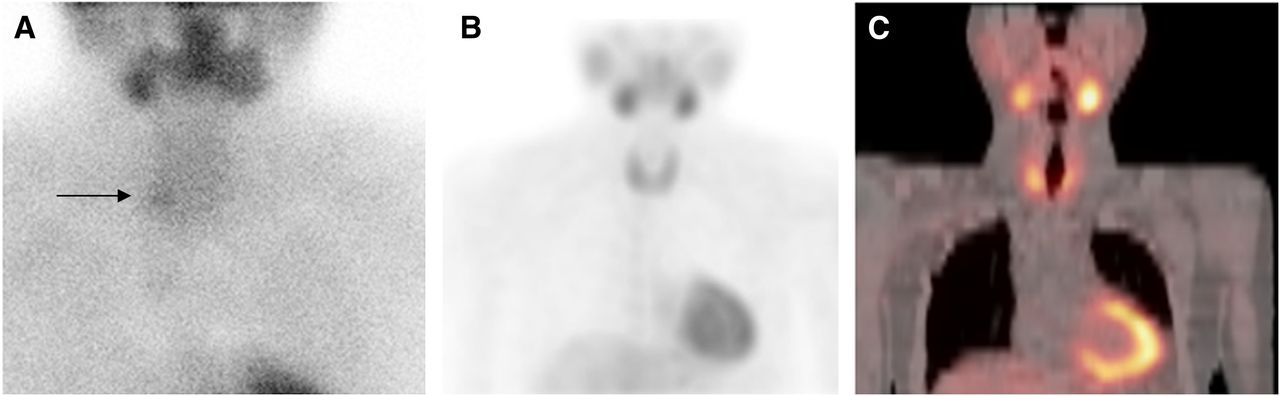
In patient 6, preoperative 123I/99mTc-sestamibi subtraction imaging (A) localized pathologic parathyroid gland (arrow) to right lower quadrant. 99mTc-sestamibi SPECT/CT remained negative as demonstrated by SPECT maximum-intensity-projection image (B) and SPECT/CT fusion image (C). Surgery and histology revealed parathyroid adenoma within right thyroid lobe.
DISCUSSION
To the best of our knowledge, this is the first prospective study directly comparing the performance of 4 localization techniques—that is, planar scintigraphy with 123I/99mTc-sestamibi, 99mTc-sestamibi SPECT/CT, 11C-methionine PET/CT, and SVS—in the setting of complicated primary hyperparathyroidism. The results demonstrate that 123I/99mTc-sestamibi, which in general is widely available, performs well also in the reoperative setting, with an accuracy of 59% for indicating the correct side of the neck and 48% for a more precise localization (i.e., the correct quadrant or other more specific site such as the mediastinum). In contrast, performance of both SPECT/CT using the present protocol and SVS was rather poor. SPECT/CT performed significantly worse than 123I/99mTc-sestamibi (19% vs. 59% for accurately predicting the correct side of the neck [P < 0.01] and 14% vs. 48% for predicting the more specific site [both P < 0.02], respectively).
Lavely et al. compared the performance of planar imaging, SPECT, and hybrid SPECT/CT in a large series of 110 patients with primary hyperparathyroidism and no prior neck surgery (16). All patients underwent surgical exploration, and 98 patients with single adenomas were included in the final analyses. However, 12 patients with multiglandular disease were excluded, and no data on the performance of the different imaging techniques among these more challenging patients were given (16). Furthermore, data on the percentage of patients who achieved biochemical cure after primary operation were not provided (16). The authors concluded that early SPECT/CT in combination with any delayed imaging was superior to single- or dual-phase planar or SPECT study in this setting (16). In the present study, SPECT/CT was performed at 2 h. It is possible that performance could have been enhanced by performing imaging already at 20 min, as in the study by Lavely et al. (16). However, of note, planar scintigraphy was performed using double tracers in the present study, whereas Lavely et al. used a single-tracer technique. 99mTc-sestamibi is not a parathyroid tissue–specific tracer but is also taken up by thyroid tissue. Comparison with a second tracer, taken up by the thyroid gland only, is therefore recommended (15). Previous studies have indeed reported an increased sensitivity of double-tracer studies (17,18). In line with this, we have also noted an increased sensitivity of 123I/99mTc-sestamibi, compared with 99mTc-sestamibi alone (unpublished data).
In a retrospective study, Witteveen et al. (19) reported that 99mTc-sestamibi SPECT imaging was of limited value in the reoperative setting of hyperparathyroidism in 19 consecutive patients, as compared with the performance of 99mTc-sestamibi SPECT in 23 control patients with sporadic hyperparathyroidism due to single-gland disease who underwent scanning before initial surgery. Thus, good performance of a technique before primary operation does not necessarily ensure good performance also in the reoperative setting.
SVS was introduced for localization of hyperfunctioning parathyroid glands in 1969 by Reitz et al. (20). Results from previous studies evaluating the accuracy of this invasive technique have not been consistent; the range of positive predictive results has varied markedly from 39% to 93% (2,8,21–28). Most of these studies have been retrospective and have not included direct comparison with modern imaging techniques. The differences in outcome can partly be explained by patient selection (from selected patients to 100% of patients) and selection based on histology (i.e., single adenomas vs. multiglandular disease). In the present prospective comparative study, SVS was positive in all but 1 patient, but overall accuracy was only 40%. Of all the different localization techniques, SVS was associated with the highest percentage of false predictive results. The accuracy of SVS for predicting the right quadrant or more specific site was 25%. SVS identified the correct side of the neck in one and the correct specific site (i.e., mediastinum) for another patient (patients 13 and 17, respectively; Table 2) for whom 123I/99mTc-sestamibi remained negative. However, for both of these patients 11C-methionine PET/CT accurately identified not only the correct side but also the correct more specific site (Table 2). On the basis of the present comparative study, SVS can no longer be recommended before reoperation of persistent hyperparathyroidism, at least not using the same study protocol.
11C-methionine has good specificity for hyperfunctioning parathyroid tissue, compared with the surrounding head and neck tissue (29), and 2 studies supported the use of methionine PET in difficult cases of negative localization before reoperation (30,31). However, data on the performance of 11C-methionine PET/CT in the reoperative setting of primary hyperparathyroidism are scarce. Tang et al. reported high sensitivities of 95% for 99mTc-sestamibi and 92% for 11C-methionine PET/CT for parathyroid adenomas and 59% versus 68% for hyperplasia, respectively, before initial surgery of hyperparathyroidism (32). In line with this, the accuracy of 123I/99mTc-sestamibi and 11C-methionine PET/CT in the present study in the reoperative setting of hyperparathyroidism was similar both with regards to the correct side (59% vs. 65%; κ-coefficient, 0.42) and more specific localization (48% vs. 61%; κ-coefficient, 0.57). 123I/99mTc-sestamibi was superior in 1 patient (patient 9; Table 2) for whom it accurately detected a pathologic parathyroid gland on both sides of the neck, whereas 11C-methionine PET/CT revealed only 1 lesion on the left side. Patient 18 also had 2 hyperplastic glands removed; 123I/99mTc-sestamibi accurately identified one of these while 11C-methionine PET/CT remained negative (Table 2). Oksüz et al. previously reported a case in which methionine PET/CT identified 1 lesion, but surgery confirmed 2 ipsilateral adenomas (33). In the present study, 123I/99mTc-sestamibi demonstrated no false predictive lesions, whereas 11C-methionine PET/CT was false predictive in 1 patient. On the other hand, 11C-methionine PET/CT correctly localized an adenoma to the right thyroid lobe in 1 patient, for whom the finding on 123I/99mTc-sestamibi was compatible with the right upper quadrant. In addition, 11C-methionine PET/CT accurately localized the disease in 4 of 8 (50%) patients for whom 123I/99mTc-sestamibi remained negative (Table 2). All 4 patients were biochemically cured after reoperation. Neither SPECT/CT nor SVS was of additive value, compared with the combined results of imaging with 123I/99mTc-sestamibi and 11C-methionine PET/CT. 11C-methionine PET is not available in all centers, and the complicated labeling procedure can be regarded as a limitation. However, on the basis of the present study, this technique can be recommended as the best second-line localization technique before reoperation of primary hyperparathyroidism in patients with negative 123I/99mTc-sestamibi results. 11C-methionine PET/CT thus represents a promising new technique for difficult cases of primary hyperparathyroidism before reoperation. The role of 11C-methionine PET/CT in primary hyperparathyroidism should still be evaluated in larger case series in the future.
Reoperation of hyperparathyroidism is associated with a high complication rate. However, none of the patients in the present study had any surgical complications. In 1 patient (patient 14), surgical exploration was successful despite the fact that none of the preoperative localization techniques was accurate. Three patients were not biochemically cured. One of them (patient 3) had previously undergone total thyroidectomy, because of papillary thyroid cancer, in addition to parathyroid surgery; preoperative SVS was false predictive in this patient and none of the imaging techniques was helpful because they all remained negative. The 2 other patients not cured had both had previous parathyroid surgery twice; SVS was false predictive in both (patients 8 and 15) and 11C-methionine PET/CT in one (patient 8). The 2 other imaging methods were not helpful because they remained negative. Histology was compatible with thyroid tissue in both instances.
CONCLUSION
All patients should undergo localization studies before reoperation of primary hyperparathyroidism. To the best of our knowledge, no previous studies have prospectively compared the performance of planar scintigraphy with 123I/99mTc-sestamibi, 99mTc-sestamibi SPECT/CT, 11C-methionine PET/CT, and SVS before reoperation of hyperparathyroidism. On the basis of our results, 123I/99mTc-sestamibi is recommended as the first-line investigation before reoperation. 11C-methionine PET/CT provides valuable additional information if 123I/99mTc-sestamibi remains negative. SVS is associated with false predictive findings, and 99mTc-sestamibi SPECT/CT is negative in many patients. These 2 techniques provided no additional information, compared with the combined results of 123I/99mTc-sestamibi and 11C-methionine PET/CT.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This study was supported by grants from the Research Funds from the University Central Hospital in Helsinki. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Tommi Noponen, Med. Phys., D.Sc, for expert technical help with the figures and Aapo Ahonen for his valuable comments on the manuscript.
Footnotes
Published online Apr. 3, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication November 1, 2012.
- Accepted for publication November 5, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}