


Abstract
Paragangliomas and pheochromocytomas are genetically heterogeneous diseases. The purpose of this study was to determine the sensitivity and specificity of PET with 3,4-dihydroxy-6-18F-fluoro-L-phenylalanin (18F-DOPA) for the detection and staging of pheochromocytomas/paragangliomas. Furthermore, we assessed whether the genotypes of pheochromocytomas and paragangliomas correlate with the uptake of 18F-DOPA. Methods: We retrospectively analyzed 101 consecutive patients who underwent 18F-DOPA PET or 18F-DOPA PET/CT for known or suspected pheochromocytomas or paragangliomas. Maximum 18F-DOPA tumor uptake was quantified relative to uptake in the liver. Results: Histopathology, cross-sectional imaging, and follow-up indicated the presence of paragangliomas and pheochromocytomas in 68 patients and the absence of a tumor in 33 patients. The average 18F-DOPA uptake by paragangliomas and pheochromocytomas, expressed as a tumor-to-liver ratio, was 5.9 ± 5.2. There was no significant difference in uptake among patients with von Hippel Lindau syndrome (VHL; n = 19), succinate dehydrogenase B–D mutation (n = 21), neurofibromatosis type 1 (n = 1), RET (n = 1), no germline mutation (n = 20), or unknown mutation status (n = 6) (P = 0.84). All 8 patients with an SDHD mutation were true-positive on 18F-DOPA PET. There were 2 cases of false-negative results each in the group with SDHB (2/12) and VHL mutations (2/19) and 1 false-negative result in the subgroup of patients with unknown mutation status (1/6). Overall, 18F-DOPA PET yielded a sensitivity of 93% and a specificity of 88% for the detection of paragangliomas and pheochromocytomas on a patient basis (positive and negative predictive value, 94% and 85%, respectively). Conclusion: 18F-DOPA PET is a sensitive and specific imaging modality for the detection and staging of pheochromocytomas and paragangliomas in different genotypes, including VHL-, SDHB-, and SDHD-mutation carriers, and in patients with no germline mutation.
Pheochromocytomas and paragangliomas are tumors arising from sympathetic and parasympathetic paraganglia throughout the body. The World Health Organization defines pheochromocytomas as tumors with an intraadrenal origin, whereas extraadrenal paragangliomas are defined as tumors arising from other locations (1). A more symptom-oriented classification defines pheochromocytomas as tumors originating from the sympathetic neuroendocrine system (which can be located in the adrenal medulla or in extraadrenal abdominal, intrapelvic, or thoracic locations), whereas paragangliomas are tumors that derive from the parasympathetic system predominantly located in the head and neck region. These tumors usually do not secrete catecholamines and are also known as glomus tumors (2).
Pheochromocytomas and paragangliomas can occur sporadically or in the context of hereditary syndromes. Approximately 25% of patients with pheochromocytomas or paragangliomas are carriers of a germline mutation of the following susceptibility genes: RET, von Hippel Lindau (VHL), succinate dehydrogenase B–D (SDHx), or neurofibromatosis type 1 (NF1) (3,4). These different mutations are correlated with various biologic properties of pheochromocytomas and paragangliomas: the risk for malignancy ranges from none in SDHC, less than 3% for SDHD, and up to about 25% for SDHB mutation carriers. In addition, the risk for the development of multiple lesions is higher in patients with VHL or SDHD mutation (55% and 48%, respectively) than in those with NF1, SDHB, or SDHC mutations (11%–12%) (data taken from the European-American-Pheochromocytoma-Paraganglioma-Registry based in Freiburg).
3,4-dihydroxy-6-18F-fluoro-phenylalanin (18F-DOPA) PET has been developed to investigate the activity of the dopaminergic system in neurologic disorders (5). After intracellular uptake, 18F-DOPA is decarboxylated by DOPA decarboxlyase to 18F-dopamine and trapped intracellularly. However, various neuroendocrine tumors also have the ability to accumulate and decarboxylate 18F-DOPA. These tumors include pheochromocytomas, paragangliomas (6), medullary thyroid cancer (7), and insulinomas (8), among others (9). In pheochromocytomas and paragangliomas, 18F-DOPA PET has been used for several years to detect pheochromocytomas, to differentiate pheochromocytomas and paragangliomas from other tumors, and to stage patients with known or suspected malignant pheochromocytomas and paragangliomas. Overall, a high diagnostic accuracy of 18F-DOPA PET has been observed in a small series of patients (6,10). However, there are only limited data evaluating whether the uptake of 18F-DOPA and the sensitivity of 18F-DOPA PET correlate with the underlying genotype of pheochromocytomas or paragangliomas (11,12).
Therefore, the aim of this study was to investigate whether the tumor-specific genotype of patients with pheochromocytoma and paraganglioma syndrome affects 18F-DOPA tumor avidity in a large series of patients.
MATERIALS AND METHODS
We retrospectively analyzed 136 consecutive patients referred between January 2006 and December 2010 who underwent 18F-DOPA PET (n = 108) or 18F-DOPA PET/CT (n = 28) for known or suspected pheochromocytomas or paragangliomas or for surveillance in patients with a prior history of pheochromocytomas or paragangliomas.
The reference standard to determine the presence or absence of tumor lesions was histopathology or cross-sectional imaging (MRI or CT), including follow-up imaging. To ensure the correct diagnosis, patient records were reviewed again. Patients with data judged insufficient to establish the diagnosis were removed from the analysis. For this retrospective study, the University of Freiburg Institutional Review Board waived the consent requirements.
Molecular Genetic Analysis
Genomic DNA was extracted from peripheral blood samples using standard procedures. Genetic analysis of the exonic and flanking intronic regions, including splice sites; mutations for all exons of the VHL (NM_000551.2), SDHB (NM_003000.2), SDHC (NM_003001), and SDHD (NM_003002.2) genes; and exons 10, 11, 13, and 16 of the RET (NM_020975.4) gene was performed as described previously (4,13). In addition, a screening search was performed for large deletions or rearrangements of the genes VHL, SDHB, SDHC, and SDHD.
18F-DOPA PET and 18F-DOPA PET/CT
At our center, 18F-DOPA PET was introduced for imaging of paragangliomas and pheochromocytomas about 10 y ago (14). Since then, it has been used clinically for their detection and staging. In this study, we retrospectively analyzed these scans and correlated 18F-DOPA uptake with the genotype of the patients.
18F-DOPA was synthesized by modifying a previously reported procedure (15). Patients were instructed to fast for at least 6 h before PET or PET/CT to standardize imaging conditions.
18F-DOPA was injected intravenously at an average of 286 ± 55 MBq (median, 296 MBq; range, 105–408 MBq). PET was started 47 ± 18 min (median, 42 min) after radiotracer injection.
Whole-body PET images were acquired in 2-dimensional mode on a dedicated bismuth germinate PET system (2-ring ECAT EXACT 921 or 3-ring ECAT EXACT 922; Siemens/CTI). One-minute transmission scans were obtained with 3 rotating 68Ge line sources for segmented attenuation correction. Eight to 12 bed positions with 5-min emission times each were measured, covering an axial range of 70–100 cm (10.8- or 16.2-cm axial PET field of view, 1.7-cm bed overlap).
Images were reconstructed with attenuation-weighted ordered-subset expectation maximization (2 iterations, 8 subsets, 6-mm gaussian postfiltering representing the default whole-body protocol of the scanner software).
Combined whole-body PET/CT images were acquired on a 64-slice Gemini TF lutetium yttrium orthosilicate PET/CT system (Philips Healthcare). CT acquisition parameters were 120 kVp and 200–400 mAs (dose-modulation–enabled, depending on patient weight) for contrast-enhanced full diagnostic scans and 25 mAs for low-dose CT. PET images were acquired for 1.5 or 2 min per bed position, depending on patient body weight. CT data were used to correct for photon attenuation.
CT and MRI
CT was performed on different multislice scanners (Siemens Definition [Siemens Medical Solutions] or Brilliance 64 [Philips]).
MRI was performed on different 1.5-T systems (Magnetom Avanto, Espree, or Symphony; Siemens Medical Solutions), each equipped with a phased-array surface coil (Body Matrix; Siemens Medical Solutions). However, the standard CT protocol consisted of a biphasic contrast-enhanced arterial phase CT scan of the head and neck, thorax, and upper abdomen and a portal-venous phase scan of the abdomen. The slice thickness was 3 mm in the head and neck and thorax and 4–5 mm in the abdomen.
The standard MRI protocol comprised an axial T2-weighted spin-echo sequence with fat saturation and a native axial T1-weighted spin-echo sequence. Additional coronal T2-weighted spin-echo sequences of the head and neck, and axial and coronal half-Fourier acquisition single-shot turbo spin-echo sequences of the abdomen, were usually part of the sequence protocol. Contrast-enhanced 3-dimensional magnetic resonance angiography was usually performed during the arterial passage of the contrast medium in the head and neck. After contrast injection, coronal and axial T1-weighted spin-echo sequences with fat saturation were added for exact localization of the tumor. Because of scanner-specific sequence protocols, the slice thickness of the sequences varied between 3 and 5 mm.
Image Analysis
All PET images were analyzed by 3 observers. A positive PET scan result was defined as a focal 18F-DOPA accumulation in a location at which physiologic tracer uptake is usually absent. Two observers were aware of the clinical diagnosis and additional imaging studies and performed all quantitative PET (18F-DOPA tumor uptake) and cross-sectional imaging (tumor size) measurements. A third observer was unaware of the clinical diagnosis and additional imaging studies and reviewed all PET images with regard to lesion detectability. 18F-DOPA tumor uptake was measured by determination of the maximum tracer uptake in the tumor relative to the average tracer uptake in the liver using ROVER (Region of Interest Visualization, Evaluation, and Image Registration software package; ABX GmbH). A volume of interest covering the tumor with the highest 18F-DOPA accumulation was defined on PET images. Then, a volume of interest with a diameter of 4 cm was placed in the liver, excluding the large intrahepatic bile ducts. 18F-FDOPA uptake was expressed as the maximum activity concentration in the lesion divided by the mean activity concentration in the liver. In patients with metastatic or multiple lesions, only the lesion with the highest 18F-DOPA uptake that had histologic or anatomic imaging confirmation (index lesion) was used for further quantitative analyses. All CT and MRI scans were read by 1 board-certified radiologist. Standard diagnostic MRI or CT criteria were applied to correctly classify the tumor lesions.
Statistical Analysis
Quantitative data are presented as mean ± SD, median, and range. The Mann–Whitney U test and the Kruskal–Wallis test were used for unpaired comparisons between quantitative parameters. The Spearman rank test was used to correlate 2 linear variables. P values less than 0.05 were considered statistically significant.
Statistical analysis was performed using SPSS software (version 19; IBM).
RESULTS
Patients and Imaging
Consecutive patient files (n = 136) were reviewed for this study. Thirty-five patients (26%) were excluded from the analysis after the data were judged insufficient to establish a definitive diagnosis independent from the findings of the PET scan. The molecular genetic analysis of the excluded patients was as follows: SDHB, n = 4; SDHD, n = 6; unknown, n = 17; no mutation, n = 4; RET, n = 3; and NF1, n = 1. In 101 patients, histopathology (n = 37) or cross-sectional (MRI, n = 50; CT, n = 13) or functional (DOTATATE PET follow-up, n = 1) imaging was available as the gold standard to determine the absence (n = 33) or presence (n = 68) of paraganglioma and pheochromocytoma lesions. Fifty-six patients were men (55%) and 45 were women (45%), with a mean age of 44 ± 17 y (median, 45 y; range, 7–80 y) (Table 1). The time interval between 18F-DOPA PET or PET/CT and morphologic imaging was 26 ± 37 d (median, 12 d; range, 0–180 d).
Patient Characteristics (n = 101)
Correlation Between 18F-DOPA Uptake and Mutation Status
In 68 patients, histopathology (n = 36) or additional imaging (MRI, n = 25; CT, n = 6; and DOTATATE follow-up, n = 1) revealed the presence of at least 1 pheochromocytoma or paraganglioma lesion. Genetic testing results for germline mutations were available for 62 of 68 patients (91%) (Table 2).
Characteristics of Patients with Proven Pheochromocytomas or Paragangliomas (n = 68)
To avoid data bias due to systematic variability of image acquisition on different scanners, ratios of maximum tumor uptake to liver were compared in datasets acquired by separate scanners using the Kruskal–Wallis test and were correlated to injected doses and uptake times using the Spearman rank test. The tumor-to-liver ratio did not differ significantly between scanners (P = 0.77) and was not correlated to injected dose (P = 0.56) or uptake time (P = 0.44). Therefore, further analyses were performed by combining the datasets as appropriate.
The tumor-to-liver ratio of all tumors averaged 5.9 ± 5.2 (median, 4.2; range, 0–19.2) and did not differ significantly among patients with VHL (mean, 6.9 ± 5.7), SDHB (mean, 5.9 ± 5.3), SDHC (0.9), SDHD (mean, 6.0 ± 7.1), NF1 (2.8), RET (4.9), no germline mutation (mean, 5.8 ± 4.7), and unknown mutational status (mean, 4.4 ± 4.1) (P = 0.84). A separate comparison of the 4 largest subgroups—VHL (n = 19), SDHB (n = 12), SDHD (n = 8), and no mutation (n = 20)—confirmed this result (P = 0.81) (Fig. 1).
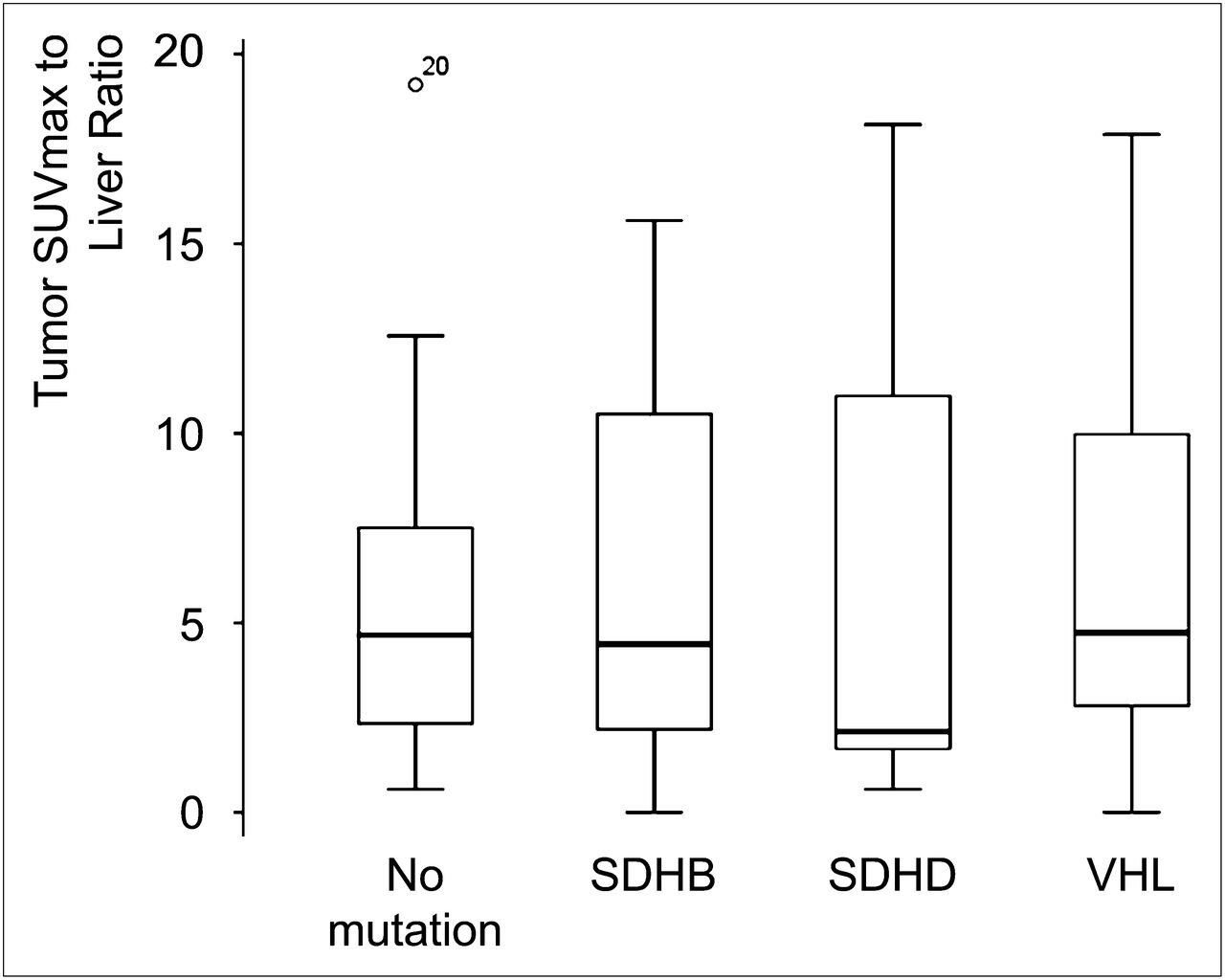
Box plots of ratios of tumor maximum standardized uptake value to mean liver showing median, lower and upper quartiles, range, and outlier (patient 20) in patients with and without germline mutations. SUVmax = maximum standardized uptake value.
In a patient-based analysis, all 8 patients with SDHD mutation and pheochromocytomas/paragangliomas were classified as true-positive on 18F-DOPA PET. There were 2 cases of false-negative results each in the groups with SDHB and VHL mutations and 1 false-negative metastatic index lesion in the group with unknown mutation status (Table 3). Therefore, 63 of 68 pheochromocytoma/paraganglioma patients were correctly classified by 18F-DOPA PET (sensitivity, 93%) (Figs. 2 and 3).
Patient- and Lesion-Based Sensitivity of 18F-DOPA PET According to Underlying Genotype

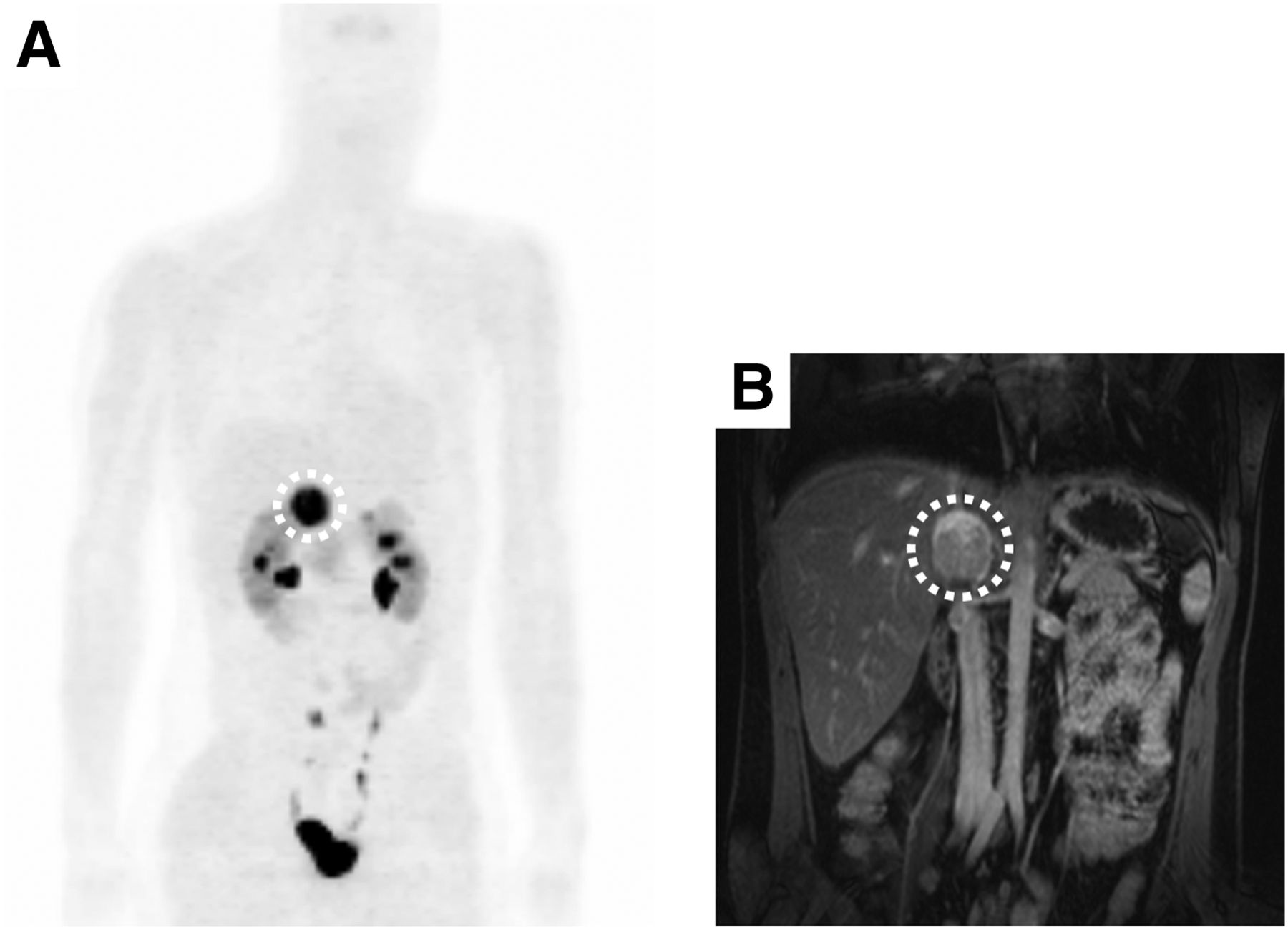
(A) True-positive 18F-DOPA PET study of 20-y-old woman with identified VHL germline mutation. (B) Corresponding MR image of biopsy-proven pheochromocytoma (circled).
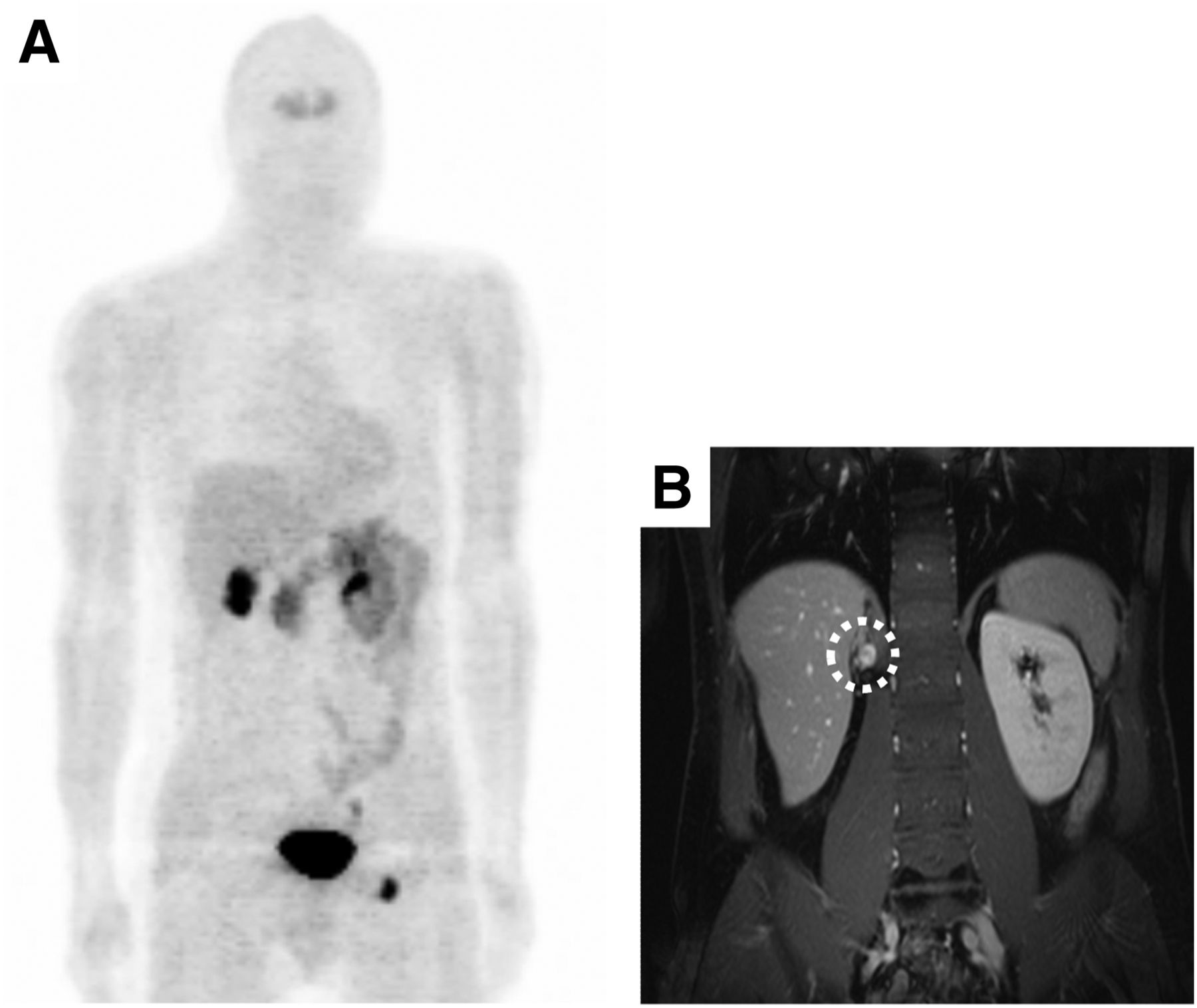
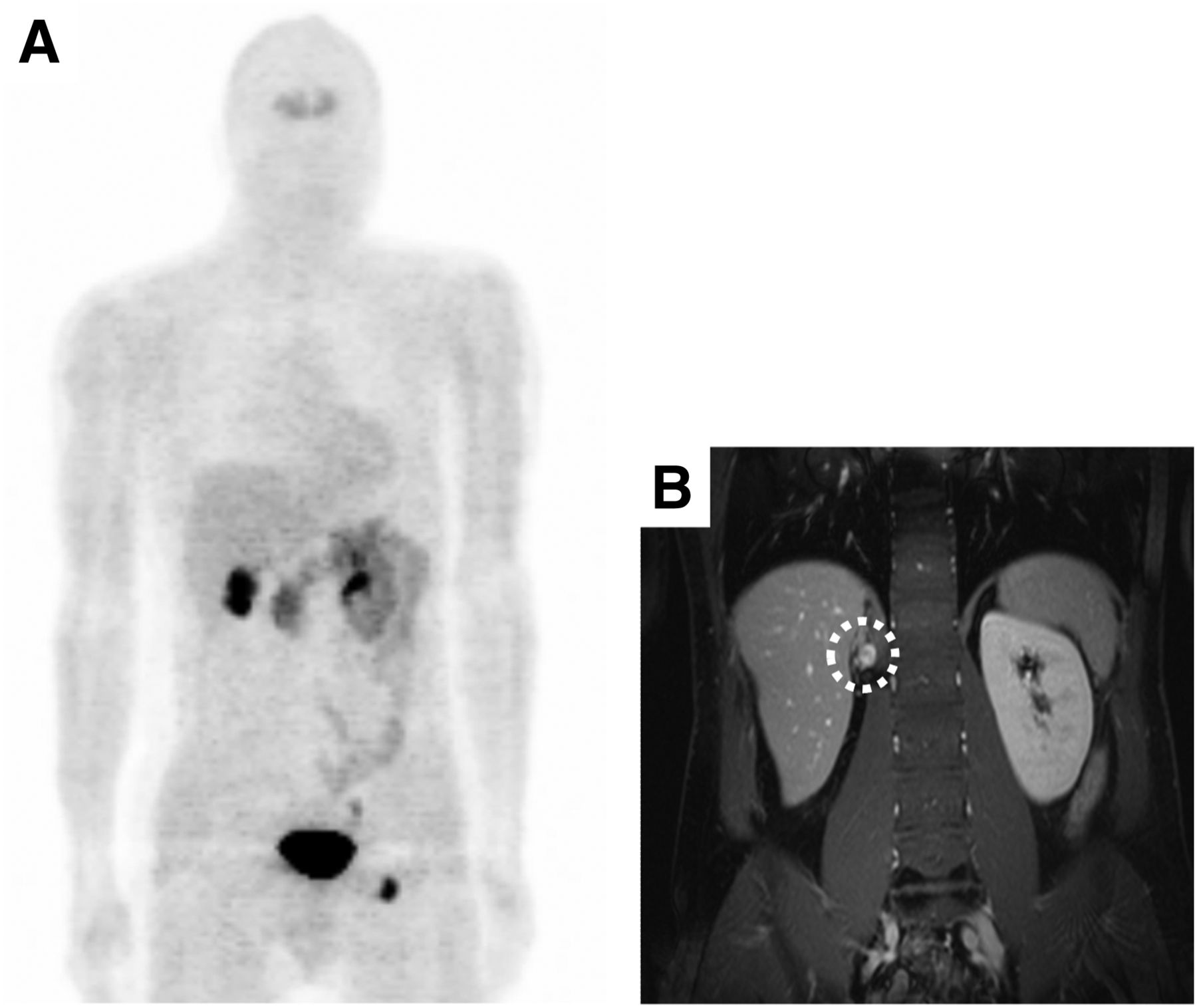
(A) False-negative 18F-DOPA PET study of 36-year-old man with identified SDHB germline mutation (focus in left groin corresponds to urine contamination). (B) MRI revealed presence of biopsy-proven metastatic paraganglioma. Circled area shows presence of biopsy-proven metastatic paraganglioma, which was false-negative in 18F-DOPA PET study.
Thirty-three patients showed no clinical or morphologic evidence of paragangliomas or pheochromocytomas. However, in 4 of the 33 patients (12%) PET scans depicted a false-positive 18F-DOPA accumulation. Focal 18F-DOPA accumulation not specific for pheochromocytomas or paragangliomas was verified by cross-sectional imaging and follow-up as an anatomic variant of pancreas morphology (n = 1), diverticulum of duodenum (n = 1), moderate focal accumulation in paraesophageal tissue without evidence of nodular structure (n = 1), or moderate focal accumulation in paracolic tissue without evidence of nodular structure (n = 1). Therefore, in a patient-based analysis, the specificity of 18F-DOPA PET was 88%, the positive predictive value was 94%, the negative predictive value was 85%, and the diagnostic accuracy was 91%.
In a lesion-based analysis, 18F-DOPA PET detected 180 of the 189 lesions identified by morphologic imaging (95%). The detection rates for the individual genotypes are summarized in Table 3.
18F-DOPA Uptake in Correlation to Tumor Size and Tumor Location
In 64 of the 68 pheochromocytoma/paraganglioma patients, the maximum pheochromocytoma/paraganglioma diameter of the index lesion was assessed via MRI (n = 51) or CT (n = 13) and averaged 3.1 ± 2.6 cm (median, 2.5 cm; range, 0.8–18.2 cm). The maximum tumor diameter differed significantly between genotypes, with larger tumors observed in patients with no germline mutation (mean, 4.2 ± 3.7 cm; median, 3.3 cm; and range, 1.4–18.2 cm) and unknown mutation status (mean, 4.6 ± 2.4 cm; median, 5.1 cm; and range, 1.2–7.8 cm) than in patients with SDHB (mean, 2.9 ± 1.7 cm; median, 2.5 cm; and range, 1.2–6.5 cm), SDHD (mean, 2.4 ± 2.6 cm; median, 1.3 cm; and range, 0.9–8.6 cm), and VHL mutations (mean, 2.2 ± 1.2 cm; median, 2.0 cm; and range, 1.1–4.5 cm) (P = 0.009). The Spearman rank test revealed a weak but significant correlation between maximum tumor diameter and the 18F-DOPA tumor-to-liver ratio (r = 0.53; P < 0.001).
Twenty-seven pheochromocytoma/paraganglioma tumor lesions (40%) were located in the adrenals; 20 in the head or neck (29%); and 21 (31%) in extraadrenal abdominal, intrapelvic, or thoracic regions. The tumor-to-liver ratio showed no significant correlation with tumor location (P = 0.13).
Forty-five patients (66%) showed solitary lesions, 15 patients (22%) multiple lesions, and 8 (12%) metastatic pheochromocytomas or paragangliomas. In patients with multiple or metastatic disease, only the index lesion was included in the tumor-to-liver ratio analysis.
The sympathetic and parasympathetic nervous systems have a widespread distribution within the human body. Therefore, patients may present with multiple pheochromocytomas/paragangliomas in various areas of the body. The most commonly involved areas include the carotid body, jugular foramen, and middle ear, together with the mediastinum, sympathetic chain, and adrenal medulla. Patients with multiple lesions in these areas were classified as having multifocal disease (14,16,17). Metastatic disease was defined by the presence of lesions outside these areas.
The tumor-to-liver ratio showed no significant difference among patients with solitary lesions (mean, 5.0 ± 4.5; median, 3.9; and range, 0–17.9), the index lesion of multiple lesions (mean, 9.3 ± 6.7; median, 5.9; and range, 1.5–19.2), or the index lesion of metastatic lesions (mean, 4.7 ± 3.6; median, 4.1; and range, 0–11.0) (P = 0.09). The mutational background of multiple and metastatic lesions is provided in Table 4.
Genotype of Patients with Multiple or Metastatic Pheochromocytomas or Paragangliomas
DISCUSSION
In this study, we found no significant influence of germline mutations on tumor 18F-DOPA uptake in a group of 101 consecutive pheochromocytoma/paraganglioma patients. Differences in radiotracer avidity across patients with different germline mutations were small, and there was a much larger variability of 18F-DOPA uptake within each group of mutations. The average tumor-to-liver ratio was not significantly different between solitary lesions and the index lesion of patients with multiple or metastatic pheochromocytomas/paragangliomas. 18F-DOPA uptake was also not significantly influenced by the location of the paraganglioma index lesion. The overall sensitivity and specificity of 18F-DOPA PET on an individual patient basis was 93% and 88%, respectively. A similarly high sensitivity was observed in a lesion-based analysis (95%). These findings indicate that 18F-DOPA can be used for the detection and staging of patients with paraganglioma syndrome underlying VHL, SDHB, and SDHD mutations and in patients without mutation.
18F-DOPA enters cells via the amino acid transporter systems for large neutral amino acids (18). After transmembrane transport, 18F-DOPA is decarboxylated to 18F-fluorodopamine by amino acid decarboxylase, which is strongly expressed in tumors of neuroendocrine or neural origin (19). DOPA uptake is strongly dependent on amino acid decarboxylase and vesicular monoamine transporter 2 expression, as has been shown in preclinical (20) and clinical (21) studies. Several studies have reported the accumulation of 18F-DOPA by pheochromocytomas/paragangliomas. Specifically, 18F-DOPA PET is reported to be superior to 123I-MIBG scintigraphy in the detection of extraadrenal and hereditary pheochromocytomas/paragangliomas (21) and in tumors causing catecholamine excess (22). However, there are currently only limited data on the influence of pheochromocytoma/paraganglioma genotype on 18F-DOPA uptake. Because the biologic behavior of pheochromocytomas/paragangliomas—for example, risk of malignancy—differs substantially across the different germline mutations, such as risk of malignancy, it is not obvious if the rates of catecholamine synthesis and consequently 18F-DOPA uptake are similar.
In fact, 1 study has found a low sensitivity of 18F-DOPA PET to detect pheochromocytoma/paragangliomas in patients with SDHB mutations. In 15 patients with metastatic pheochromocytomas/paragangliomas, only eight 18F-DOPA PET scans were positive (sensitivity on a patient basis, 53%). In contrast, 18F-DOPA PET scans were positive in all 13 patients with metastatic pheochromocytomas/paragangliomas but no SDHB mutation. Similarly, 3 of 4 patients with SDHB mutation and nonmetastatic pheochromocytomas/paragangliomas had false-negative results on 18F-DOPA PET (patient-based sensitivity, 25%) (12). In patients with nonmetastatic paraganglioma without SDHB mutations, the sensitivity of 18F-DOPA PET was 100% (16/16 patients). Overall, the sensitivity of 18F-DOPA PET to detect pheochromocytomas/paragangliomas was only 47% (9/19 patients; 95% confidence interval, 25%–71%).
In the current study, only 2 of 12 patients with underlying SDHB mutation had false-negative findings (sensitivity, 83%; 95% confidence interval, 52%–97%). One of these patients had a paraganglioma in the paracaval region, and the other in the upper abdominal paraaortal region. The 10 patients with true-positive findings comprised 4 patients with metastatic disease of non–head and neck extraadrenal origin; 4 patients with head and neck lesions, including 1 patient with multiple lesions; 1 patient with a solitary lesion in the adrenal; and 1 patient with a solitary extraadrenal lesion (Table 4).
In accordance with this observation, a recent study has reported that 18F-DOPA PET detected 26 of 26 head and neck paragangliomas in 10 patients, including the paragangliomas of 3 patients with SDHB mutation (23). In contrast Timmers et al. reported a low sensitivity of 18F-DOPA PET in patients with SDHB mutations (12). There are several potential explanations for these discrepant findings. First, there are differences with respect to tumor location, because only 1 of 20 SDHB mutation carriers in the Timmers study had a lesion located in the head and neck. Second, the following technical factors may explain the differences in reported sensitivities of 18F-DOPA PET:
The studied patient populations with SDHB mutations were relatively small, with wide and overlapping confidence intervals for sensitivity.
There may have been differences in lesion size that could have influenced the sensitivity of 18F-DOPA PET.
The available imaging technology may also play a role in lesion detectability. In the present study, all but 1 (false-negative liver metastasis imaged on an integrated PET/CT scanner) false-positive or false-negative 18F-DOPA PET finding was imaged on an older stand-alone PET device.
Third, and perhaps most important, the reference standard used by Timmers et al. (12) included the results of morphologic imaging, 18F-FDG PET, 123I-MIBG SPECT, and 18F-fluorodopamine PET. This combination of diagnostic tests likely identifies lesions that were missed by routine morphologic imaging studies. Therefore, 18F-DOPA studies in SDHB patients that were considered as true-negative in the present study may have turned out to be false-negative when compared with a reference standard including a combination of multiple functional and morphologic imaging studies.
Larger, preferably multicenter trials are needed to further define the sensitivity of 18F-DOPA in the subgroup of patients with SDHB mutation. However, our study indicates that the variability in 18F-DOPA uptake within a specific genotype is much larger than the variability across groups of patients with a specific germline mutation associated with pheochromocytomas and paragangliomas. This finding suggests that genotype is probably not a major factor influencing 18F-DOPA uptake in pheochromocytomas and paragangliomas.
This study has several limitations. First, as with all retrospective analyses, selection bias is a potential concern regarding the interpretation of our findings. Hypothetically, 18F-FDG– or 123I-MIBG–positive patients could have been less likely to undergo 18F-DOPA PET, potentially biasing our findings in favor of 18F-DOPA PET. However, 18F-DOPA has been the standard radiotracer in our clinic to study pheochromocytomas and paragangliomas for several years. 123I-MIBG SPECT or 18F-FDG PET has only rarely performed in this patient population. Our results are therefore unlikely to be prone to a selection bias.
Second, PET scans were acquired on 3 generations of PET scanners with varying uptake times and injected doses. This is because pheochromocytoma/paraganglioma is a relatively rare disease, and it thus took several years to recruit the large series of patients described in this study. However, the 18F-DOPA tumor-to-liver ratio did not correlate with injected dose (P = 0.56) or uptake time (P = 0.44), nor did it correlate with the PET devices (P = 0.77). Nevertheless, these confounding factors may have contributed to the variability of 18F-DOPA uptake observed in the present study. These factors may have masked small systematic differences in radiotracer uptake across different groups of patients. However, it is unlikely that such small differences in radiotracer uptake will significantly affect lesion detectability in clinical studies.
Third, histopathologic confirmation of a pheochromocytoma or paraganglioma was available in only 36 of 68 patients because of the retrospective nature of this study and the fact that biopsies were not clinically indicated in the remaining patients. However, standard diagnostic criteria for MR or CT images and all available clinical information were used to come to a definitive diagnosis. The University Hospital Freiburg is a center for patients with pheochromocytoma/paraganglioma syndromes and has extensive patient records that were reviewed to ensure the correct diagnosis. Because patients with SDHx or VHL mutations are at high risk for developing pheochromocytomas/paragangliomas, typical clinical and imaging findings on MRI and CT make pheochromocytomas/paragangliomas likely. Accordingly, the rate of false-positive diagnoses can be expected to be low.
Fourth, a recent study in pheochromocytomas/paragangliomas reported (24) increased detection rates due to enhanced 18F-DOPA tumor uptake and significantly decreased tracer uptake by the pancreas (higher tumor-to-background ratio) when carbidopa is administered before the 18F-DOPA injection. In the current study, we did not administer DOPA decarboxylase inhibitors, possibly influencing qualitative and quantitative PET measurements.
However, we believe that with the development of efficient and automated nucleophilic syntheses for 18F-DOPA, the clinical availability of 18F-DOPA PET is expected to increase significantly (25). Therefore, 18F-DOPA PET/CT may become the preferred imaging modality for the detection and staging of paragangliomas and pheochromocytomas.
CONCLUSION
18F-DOPA PET is a sensitive and specific imaging modality for the detection and staging of pheochromocytomas/paragangliomas in various genotypes, including VHL-, SDHB-, and SDHD-mutation carriers, and in patients with no germline mutation.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Jul. 26, 2012.
- © 2012 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication November 27, 2011.
- Accepted for publication April 2, 2012.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.