


Abstract
123I-N-ω-fluoropropyl-2β-carboxymethoxy-3β-(4-iodophenyl)nortropane (123I-FP-CIT) is commonly used to assess the dopamine transporter in the striatum. However, recent studies suggest that this tracer may be used also to assess binding to monoamine transporters in the midbrain or diencephalon, which may reflect predominantly serotonin transporter (SERT) binding. However, it is still unclear at what time point after injection SPECT should be performed for optimal assessment of SERT with123I-FP-CIT. Therefore, we examined the time course of extrastriatal 123I-FP-CIT binding. Methods: Nineteen healthy, male subjects were included, and SPECT images were acquired up to 3 h after 123I-FP-CIT injection. Region-of-interest analysis was performed, and specific-to-nonspecific binding ratios were calculated. Results: Specific-to-nonspecific 123I-FP-CIT binding ratios in the midbrain and diencephalon were significantly higher 2 h after injection than 1 h after injection and remained stable between 2 and 3 h after injection. Conclusion: The optimal time frame for assessing 123I-FP-CIT binding to extrastriatal SERT is between 2 and 3 h after injection of the tracer.
In 2000, the radiotracer 123I-N-ω-fluoropropyl-2β-carboxymethoxy-3β-(4-iodophenyl)nortropane (123I-FP-CIT) was registered in Europe to assess striatal dopamine transporter (DAT) binding, and it is now commonly used to study the integrity of nigrostriatal dopaminergic neurons in vivo (1). Recently, the same tracer was licensed in the United States. The optimal time point for measuring striatal DAT is between 3 and 6 h after bolus injection of 123I-FP-CIT (2).
In vitro studies showed a high affinity of 123I-FP-CIT for the DAT. However, this tracer also has a moderate affinity for the serotonin transporter (SERT) (3). Indeed, in healthy controls we showed that, after administration of the selective serotonin reuptake inhibitor paroxetine, 123I-FP-CIT binding was significantly blocked in the SERT-rich midbrain and diencephalon (4). Likewise, another recent study showed that thalamic binding of 123I-FP-CIT could be blocked by the selective serotonin reuptake inhibitor citalopram (5). The relative anatomic segregation between striatal DAT and extrastriatal SERT binding sets the condition for 123I-FP-CIT SPECT studies to examine also SERT in vivo. Interestingly, recent clinical FP-CIT SPECT studies showed not only loss of striatal DAT but also loss of midbrain SERT binding in dementia with Lewy bodies and in Parkinson patients with depression (6,7). In these 2 studies, 123I-FP-CIT binding in SERT-rich areas was measured 3 h after injection, but it is not known whether this time point is optimal for assessing FP-CIT binding to SERT.
Abi-Dargham et al. studied 4 healthy controls and showed that peak specific 123I-FP-CIT binding in the midbrain occurred at 72 ± 37 min after injection, followed by slow washout (3). In a previous study, we measured SERT binding in the midbrain and diencephalon only at 1 and 3 h after injection of 123I-FP-CIT (4). These preliminary studies gave us an idea of the fast kinetics of 123I-FP-CIT binding to extrastriatal SERT. However, since it is incompletely known what the optimal time point is for assessing SERT binding in extrastriatal areas using 123I-FP-CIT, the aim of the present study was to examine the time course of FP-CIT binding in the midbrain and diencephalon. Because previous 123I-FP-CIT studies showed that the optimal time point to assess striatal DAT is between 3 and 6 h after injection, and the binding potential is lower in the midbrain and diencephalon than in the striatum, we expected the optimal time point to assess extrastriatal SERT binding to occur earlier than 3 h after injection (1,2,4).
MATERIALS AND METHODS
Subjects
Nineteen healthy male volunteers with a mean age of 23.5 y (range, 19–37 y) were included in this study. There were no known medical conditions or use of any medication, nor was there a history of any psychiatric disorder or abuse of alcohol, drugs, or nicotine. Written informed consent was obtained, and the study was approved by the medical ethics committee.
123I-FP-CIT SPECT
Radiosynthesis of 123I-FP-CIT was performed as described earlier (8). Approximately 115 MBq of 123I-FP-CIT (range, 110–120 MBq) was injected intravenously as a bolus. All study subjects underwent SPECT at 1, 2, and 3 h after injection of 123I-FP-CIT. The scan duration at each time point was approximately 35 min. Each study participant was pretreated with potassium iodide to block thyroid uptake of free radioactive iodide. SPECT was performed on a 12-detector, single-slice dedicated brain scanner (NeuroFocus), using an acquisition protocol as described earlier with slight modifications (interslice distance, 5 mm; acquisition time, 210 s per slice) (4,9).
Image Reconstruction and Analysis
Images were corrected for attenuation and reconstructed in 3-dimensional mode, as described earlier. For quantification, a region-of-interest analysis was performed to determine specific binding activity in the midbrain and brain stem (herein called midbrain), diencephalon (Fig. 1), and striatum as described earlier (4,9). Briefly, the 4 consecutive slices with the highest striatal, diencephalic, and midbrain binding were selected to assess binding to DAT and SERT, respectively. Activity in the cerebellum (Fig. 1) was assumed to represent nondisplaceable activity (nonspecific binding and free radioactivity). Finally, a specific-to-nonspecific binding ratio was calculated as ([activity in region of interest minus nonspecific binding] divided by nonspecific binding) (10,11).

Transversal slice at level of midbrain and upper cerebellum obtained 2 h after injection of 123I-FP-CIT, showing placement of fixed regions of interest on both midbrain and cerebellum.
Statistical Analysis
Data on SERT were not normally distributed; therefore, a nonparametric Wilcoxon signed ranks test was used for statistical analysis, to compare SERT binding ratios at 1 and 2 h, 2 and 3 h, and 1 and 3 h after injection, and consequently data are expressed as median and range. Data on DAT were normally distributed. Therefore, a parametric paired t test was to use to compare DAT binding ratios at 1 and 2 h, 2 and 3 h, and 1 and 3 h after injection, and data are expressed as mean ± SEM.
RESULTS
Extrastriatal 123I-FP-CIT Binding
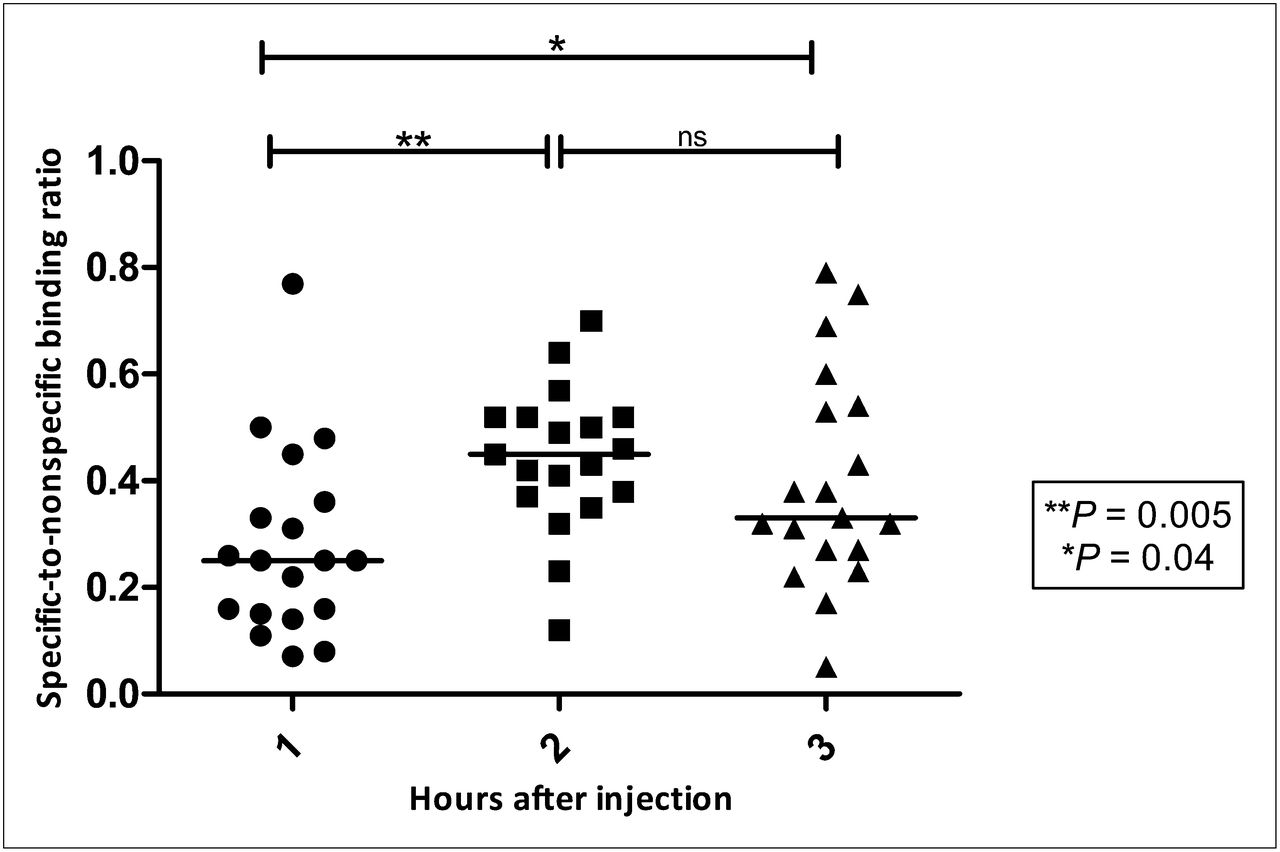
At almost all time points examined and in all subjects, 123I-FP-CIT binding was higher in the midbrain and the diencephalon than in the cerebellum. The means and SEM for specific-to-nonspecific 123I-FP-CIT binding ratios 1, 2, and 3 h after injection are shown in Figure 2 for the midbrain and Figure 3 for the diencephalon. Two hours after injection, binding ratios were significantly (P = 0.005) higher than at 1 h after injection in the midbrain (median, 0.25 [range, 0.07–0.77] and 0.45 [range, 0.12–0.70]). A similar significant (P = 0.001) increase between 1 and 2 h after injection was observed in the diencephalon (median, 0.35 [range, 0.24–0.84] and 0.58 [range, 0.36–1.19]). Three hours after injection, these ratios were slightly but not significantly (P = 0.20) lower than 2 h after injection in the midbrain (median, 0.40 [range, 0.05–0.79]) and slightly but not significantly (P = 0.93) higher than 2 h after injection in the diencephalon (median, 0.66 [range, 0.00–1.11]).

123I-FP-CIT specific-to-nonspecific binding ratios in midbrain of young, healthy male volunteers 1, 2, and 3 h after injection. Data are expressed as individual datum and median.

123I-FP-CIT specific-to-nonspecific binding ratios in diencephalon of young, healthy male volunteers 1, 2, and 3 h after injection. Data are expressed as individual datum and median.
Striatal 123I-FP-CIT Binding
As expected, in the DAT-rich striatum, the binding ratios were much higher than in the midbrain area (Fig. 4). These ratios increased over time, up to 3 h after injection. Mean binding ratios (±SEM) were significantly higher at 2 h (5.02 ± 0.18) than 1 h (3.13 ± 0.21) after injection (P < 0.001) and at 3 h (5.76 ± 0.31) than 2 h after injection (P = 0.005; Fig. 4).

123I-FP-CIT specific-to-nonspecific binding ratios in striatum of young, healthy male volunteers 1, 2, and 3 h after injection. Data are expressed as mean and SEM.
DISCUSSION
In this study we found that the specific-to-nonspecific binding ratios of 123I-FP-CIT in the midbrain and diencephalon peaked 2 h after injection of the radiotracer and remained stable up to 3 h after injection. The finding that the specific-to-nonspecific binding ratios of 123I-FP-CIT in the striatum increased up to 3 h after injection is in line with a previous study showing that these ratios peaked and remained stable 3–6 h after injection (2).
123I-FP-CIT is still particularly known as a ligand for imaging DAT (1,2). However, recent research clearly shows that 123I-FP-CIT also binds to SERT in the midbrain and diencephalon areas (4,5). DAT is distributed mainly in the striatum, whereas SERT is distributed mainly in the midbrain and diencephalon. Furthermore, specific extrastriatal 123I-FP-CIT uptake can be blocked by administration of a selective serotonin reuptake inhibitor that blocks SERT (4,5). 123I-FP-CIT has a lower affinity for SERT than DAT, and the expression of DAT in the striatum may be higher than that of SERT in the midbrain and diencephalon (12,13), resulting in a lower binding potential to SERT than to DAT (3,14). Therefore we expected peak binding of 123I-FP-CIT to SERT earlier than peak binding of 123I-FP-CIT to DAT. In the current study we indeed found a lower binding potential for SERT: mean peak binding potentials were 0.48 for SERT versus 5.02 for DAT. In line with this finding, peak binding for SERT in the midbrain and diencephalon was indeed earlier than peak binding for DAT in the striatum.
At the peak binding time point, association and dissociation to and from the transporter are equal. Therefore, this time point is optimal for measurement of the transporter (10,14). However, the peak binding time point varies between study subjects. A secular equilibrium is reached at a time when the ratio of specific binding to nonspecific binding is stable (15). This provides an equivalent that is related to the density of available transporters. In the current study, there was no true equilibrium for DAT and SERT binding, but there was a transient equilibrium. Therefore SERT and DAT densities may have been overestimated (15,16). Nevertheless, in the current study, peak binding ratio was reached at 2 h after injection of the tracer and specific-to-nonspecific binding ratio remained stable up to 3 h. We therefore recommend measurement of SERT with 123I-FP-CIT between 2 and 3 h after injection of the tracer. Regarding count statistics, 2 h after injection is the most optimal time point for measurement. However, particularly in patients for whom a doubled in-scanner time to measure both SERT and DAT may be a problem, such as elderly or mentally ill patients, 3 h is a reasonable alternative.
As discussed earlier, 123I-FP-CIT is not a selective tracer for the measurement of SERT. By contrast, 2-((2-((dimethylamino)methyl)phenyl)thio)-5-iodophenylamine (123I-ADAM) is a selective SERT SPECT tracer (17). However, because 123I-FP-CIT is widely used for measuring striatal DAT in, for example, Parkinson disease and dementia with Lewy bodies, it would be unfortunate not to let it serve its full purpose, particularly because recent clinical 123I-FP-CIT SPECT studies showed not only loss of striatal DAT but also loss of midbrain SERT binding in dementia with Lewy bodies and in Parkinson patients with depression (5,6). This result suggests that information about extrastriatal SERT binding as measured with 123I-FP-CIT may be of interest for diagnostic as well as research purposes and can be obtained in the same scanning section in which striatal DAT binding is measured, without any additional radiation burden for the patients.
A relatively large interindividual variation in SERT binding potential was observed in our study sample. This observation is in accordance with the relatively large variation in SERT found in SPECT studies with the selective tracer 123I-ADAM (18,19), suggesting that the presently observed variation is not due to the nonselectivity of 123I-FP-CIT. In the current study, we measured specific-to-nonspecific binding ratios of 123I-FP-CIT in the midbrain and diencephalon only in healthy young, male subjects. There seems to be no large difference between healthy male and female subjects in brain SERT in several brain areas (20). It is therefore likely that peak SERT binding ratios of 123I-FP-CIT in the midbrain and diencephalon are similar between the sexes. It is known that central SERT decreases with healthy aging (21). Because we studied only healthy young controls, we cannot exclude the possibility that peak equilibrium is even earlier than 2 h after injection in the elderly, but further investigation is needed (15,16). We performed measurements on healthy subjects. Because several medical conditions can influence brain SERT (e.g., Parkinson disease and Lewy bodies dementia (5,6), panic disorder (19), and depression (22,23)), it is unknown at present whether peak extrastriatal SERT binding of 123I-FP-CIT is similar in subjects with any of these diseases. This topic also needs further investigation. Finally, we used a dedicated brain tomographic SPECT system. Because this system has a high in-plane spatial resolution (∼6.5 mm in full width at half maximum throughout the 20-cm field of view), we positioned the regions of interest on transversal slices.
CONCLUSION
When the radiotracer 123I-FP-CIT is used to examine SERTs in the SERT-rich midbrain and diencephalon of young, healthy subjects, we recommend imaging at a single time point, between 2 and 3 h after injection.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
One of the authors is a consultant at GE Healthcare. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online May 24, 2012.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication December 22, 2011.
- Accepted for publication March 15, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}