


Abstract
This prospective study evaluated the accuracy of electrocardiogram-gated blood-pool SPECT (GBPS) for the assessment of left ventricular (LV) and right ventricular (RV) ejection fraction (EF), end-diastolic volume (EDV), and end-systolic volume (ESV) in patients with dilated cardiomyopathy (DCM), using cardiac magnetic resonance (CMR) imaging as the reference standard. Methods: Thirty-two patients (24 men and 8 women; mean age, 51 y) with a diagnosis of idiopathic DCM underwent GBPS and CMR. LV and RV parameters including EDV, ESV, and EF from GBPS were calculated using fully automated gradient software and compared with those obtained by CMR. Results: Biventricular volumes were underestimated by GBPS, compared with CMR (P < 0.001). We found no statistical difference between these 2 methods in the assessment of LV EF (P = 0.23), whereas RV EF was overestimated by GBPS (P < 0.001 vs. CMR). Regression analysis yielded significant correlations between GBPS and CMR in the assessments of biventricular parameters (r = 0.83 for LV EDV, 0.88 for LV ESV, 0.89 for LV EF, 0.86 for RV EDV, 0.86 for RV ESV, and 0.62 for RV EF; all P < 0.001). Comparison of the deviations of RV indices between GBPS and CMR with the ratio of RV EDV to LV EDV showed that there was a statistically significant trend for RV volumes to be underestimated and for RV EF to be overestimated as the biventricular volumetric ratio decreased (r = 0.61 for RV EDV, 0.68 for RV ESV, and −0.55 for RV EF; all P < 0.001). Conclusion: For patients with DCM, GBPS correlated well with CMR for the assessment of biventricular parameters, but RV indices should be cautiously interpreted.
Dilated cardiomyopathy (DCM) is the third most common cause of heart failure and the most frequent cause of heart transplantation characterized by varying degrees of ventricular dysfunction and chamber dilation (1–4). Left ventricular (LV) ejection fraction (EF), end-diastolic volume (EDV), and end-systolic volume (ESV) have been regarded as the fundamental parameters in the evaluation and monitoring of cardiac impairment. And these indices have been shown to be powerful predictors of major cardiac events in DCM patients (5). In addition to LV parameters, right ventricular (RV) EF appears to be another complementary predictor of survival in idiopathic DCM patients (6). RV function estimation is warranted in the standard evaluation of patients with advanced heart failure because patients with biventricular failure usually have reduced survival to less than 2 y (7,8).
Over the years, several noninvasive imaging techniques have been developed to assess LV and RV function. These techniques vary considerably regarding precision, ease of use, availability, and costs. LV EF can be measured by 2- and 3-dimensional echocardiography, cardiac magnetic resonance (CMR) imaging, and different radionuclide methods such as planar multigated radionuclide angiography and gated myocardial perfusion SPECT. RV EF can be calculated by CMR and first-pass radionuclide ventriculography. Of these techniques, CMR is considered the reference standard method, which delivers accurate LV and RV parameters in a single examination. However, this approach is not widely available and is restricted in patients with implanted devices. In addition to the relatively high costs, data processing is also time-consuming.
Gated blood-pool SPECT (GBPS), a 3-dimensional count-based technique that is widely available and easy to perform, enables simultaneous assessment of biventricular function, regional wall motion, and LV synchrony—all at 1 examination (9–12). Regarding LV EF, previous studies have described a significant correlation between GBPS, echocardiography, and planar multigated radionuclide angiography (13,14). As for RV EF, studies showed a significant correlation between GBPS and first-pass radionuclide ventriculography (15). Furthermore, as recently reported, GBPS has correlated well with CMR for the estimation of LV and RV parameters (16–19).
However, the feasibility of this technique in a particular DCM group with significantly dilated ventricles was unknown. Therefore, the purpose of this study was to investigate the accuracy of GBPS for the assessment of LV and RV indices in patients with DCM, using CMR as the reference standard.
MATERIALS AND METHODS
Study Population
From February 2009 to January 2010, consecutive patients with a diagnosis of idiopathic DCM at Fu Wai Hospital were prospectively included in this study. The diagnosis of idiopathic DCM was based on diffuse LV hypokinesis, LV EF less than 45%, a left end-diastolic dimension of more than 55 mm for men or more than 50 mm for women on echocardiography, and normal coronary arteries on coronary angiography or coronary CT angiography, with the exclusion of other etiologic factors that may cause LV dysfunction based on patient history (4). Patients were excluded if they had any of the following conditions: clinical instability, uncontrolled arrhythmia, pacemakers or other implantable metal devices unsuitable for CMR examination, and cardiac events between GBPS and CMR examination. The interval between GBPS and CMR was set at less than 48 h so as to minimize the change of cardiac function in these separate examinations. All patients signed informed consent before inclusion in the study, and the protocol was approved by the Institutional Ethics Committee.
GBPS Data Acquisition and Processing
Red blood cells were labeled in vivo with an injection of 925 MBq of 99mTc-pertechnetate 20 min after intravenous administration of 5 mg of pyrophosphate.
A dual-head γ-camera (e.cam; Siemens Medical Solution USA, Inc.) equipped with a low-energy high-resolution collimator was used to collect images at 32 views over a 180° noncircular orbit. Acquisition parameters consisted of an energy window of 15% centered on 140 keV, an R-R acceptance window of ±10%, 8 frames per cardiac cycle, 25 s per view, a 64 × 64 matrix, and a zoom of 1.45.
All studies were reconstructed by standard filtered backprojection with a Butterworth filter (cutoff frequency, 0.35 cycles/cm; order, 5.0). Datasets were reconstructed manually by an experienced physician according to the orientation mode of the American College of Cardiology. All data were analyzed using fully automated gradient software: Quantitative Blood Pool SPECT (version 2007; Cedars-Sinai Medical Center). For processing, midventricular locations were determined by the maximum activity in the likely ventricles, and a continuous dynamic biventricular surface was generated by the combination of spatial and temporal information. Volumes were computed from the number of voxels greater than 50% of maximum volumetric counts, and EF was computed from count changes in areas with counts greater than 35% of maximum volumetric counts (20).
Cardiac MRI
The imaging protocol was described previously by our group (21). In brief, CMR data were acquired on a 1.5-T scanner (Magnetom Avanto; Siemens), and breath-hold true fast imaging with steady–state precession cine CMR was used to obtain images with superior signal-to-noise ratio (22). Multiplane localizers were used to identify the cardiac position and the usual cardiac imaging planes by standard iterative scouting techniques. Continuous slices encompassing the entire left and right ventricles from apex to base were obtained during breath-hold using the following parameters: slices thickness, 8 mm; matrix, 256 × 256; 25 phases per cardiac cycle; and field of view of 350–400 mm, depending on the patient's chest size. Each slice was acquired in a separate breath-hold cycle at end-expiration.
Images were analyzed by a trained observer unaware of clinical and GBPS data, using commercially available software (MASS, version 5.0; Medis Medical Imaging Systems). For the LV datasets, short-axis endocardial and epicardial contours were manually drawn in end-diastole (start of R-wave) and in end-systole (smallest cavity area). Papillary muscles and trabeculations were not excluded from the ventricular volume so as to simplify CMR measurements for optimal reproducibility according to recommendations of the Society of Cardiovascular Magnetic Resonance (23). For the RV datasets, endocardial contours were manually traced at end-diastole and end-systole, and only the portion of the volume below the level of the pulmonary valve was included. All sets of drawings were reviewed by a CMR expert who had no access to the GBPS data. CMR values were computed by the modified Simpson rule (24).
Statistical Analysis
The statistical analyses were performed using SPSS 13.0 (SPSS Inc.). Data were described as mean ± SD and median with ranges. A paired t test was used to compare means, and linear regression analysis and the Pearson correlation coefficient were used to assess the strength of the relationship between EF values and volumes for GBPS and CMR. Bland–Altman analysis was applied to assess agreement and to evaluate the systematic trends in differences. To test the processing variability in GBPS and CMR, all datasets were processed again by the same observer and another experienced observer for the evaluation of intra- and interobserver reproducibility in both LV and RV parameters. Both observers had 5 y of experience with GBPS data. Statistical significance was defined as a P value less than 0.05 for all tests.
RESULTS
Thirty-five patients with normal coronary arteries on coronary angiography (n = 12) or coronary CT angiography (n = 23) were initially recruited. Three patients were excluded because they did not undergo CMR within 48 h of GBPS. The remaining 32 patients (24 men and 8 women; mean age ± SD, 51 ± 14 y) constituted our patient population. The GBPS calculations were totally automated beyond the image reconstruction and reorientation processing and succeeded in all patients without manual intervention. The mean interval between GBPS and CMR acquisitions was 21 ± 8 h (range, 3–34 h). According to New York Heart Association (NYHA) functional class criteria, 4 patients were classified as NYHA class III, and the remaining 28 patients were in NYHA class IV. Table 1 presents the clinical characteristics and imaging results of patients, and Table 2 presents the mean values of GBPS and CMR.
Clinical Characteristics and Imaging Results of Patients (n = 32)
Left and Right Ventricular Parameters Assessed by GBPS and CMR
LV Volumes and EF
GBPS-measured LV volumes were statistically lower than values obtained by CMR (EDV, 229 ± 68 vs. 261 ± 69 mL, P < 0.001, and ESV, 188 ± 68 vs. 216 ± 70 mL, P < 0.001). Comparisons of LV EDV and LV ESV from GBPS and CMR yielded significant correlations (r = 0.83 and 0.88, respectively; both P < 0.001) (Figs. 1A and 1B). Bland–Altman analysis revealed that GBPS underestimated both LV EDV and LV ESV (−32 ± 40 and −28 ± 34 mL, respectively; bias significantly different from 0, both P < 0.001). No significant trends were found for the estimation of LV EDV and LV ESV by GBPS (P = 0.95 and 0.76, respectively). The 95% limits of agreement of LV EDV and LV ESV were −109.8 to 45.1 mL and −94.7 to 38.6 mL, respectively (Figs. 2A and 2B).
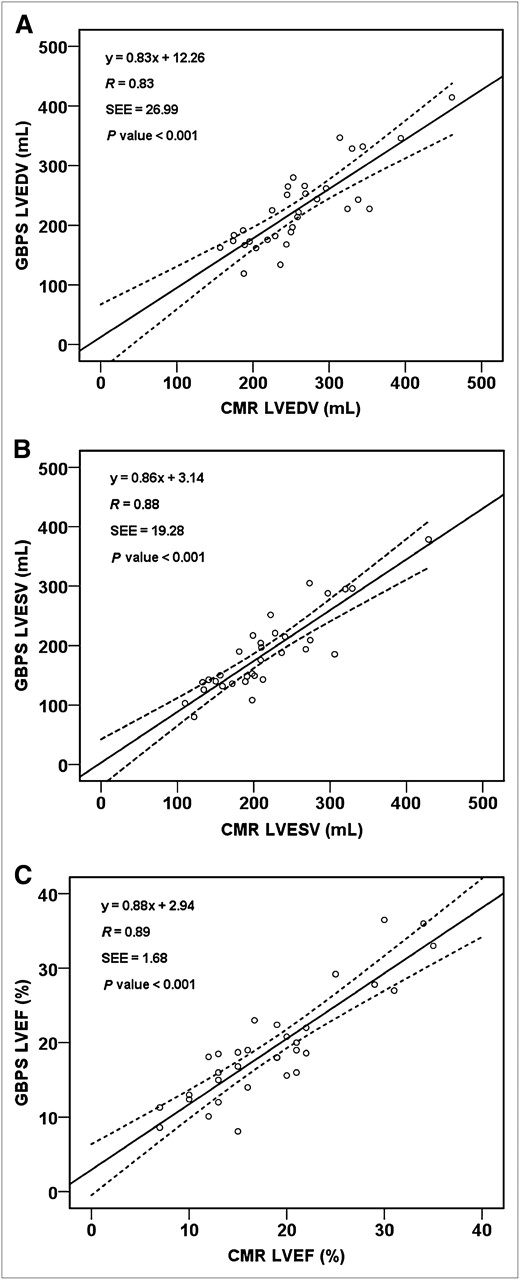
Linear regression of LV EDV (A), LV ESV (B), and LV EF (C) values from CMR and GBPS.

Bland–Altman plots of LV EDV (A), LV ESV (B), and LV EF (C) values from CMR and GBPS.
The assessment of mean LV EF by GBPS and CMR found no statistical difference (19% ± 7% vs. 19% ± 7%; P = 0.23). The Pearson correlation coefficient of LV EF between GBPS and CMR was 0.89 (P < 0.001) (Fig. 1C). Bland–Altman analysis revealed no bias for the estimation of LV EF by GBPS (1% ± 4%; bias not significantly different from 0, P = 0.24). No statistically significant trend was found for the measurement of LV EF by GBPS (P = 0.99). The 95% limit of agreement was −6.1% to 7.6% between GBPS and CMR (Fig. 2C).
RV Volumes and EF
The mean values of RV EDV and RV ESV were underestimated by GBPS, compared with CMR (170 ± 36 vs. 195 ± 37 mL, P < 0.001, and 117 ± 37 vs. 144 ± 37 mL, P < 0.001). Linear regression analysis yielded significant correlations in the measurement of RV EDV and RV ESV between GBPS and CMR (for RV EDV, r = 0.86 and P < 0.001; for RV ESV, r = 0.86 and P < 0.001) (Figs. 3A and 3B). Bland–Altman analysis showed that GBPS underestimated both RV EDV and RV ESV (−25 ± 19 and −27 ± 20 mL, respectively; bias significantly different from 0, both P < 0.001). No significant trends were found for the estimation of RV EDV and RV ESV by GBPS (P = 0.77 and 0.92, respectively). The 95% limits of agreement of RV EDV and RV ESV were −62.0 to 12.4 mL and −66.1 to 11.8 mL, respectively (Figs. 4A and 4B).
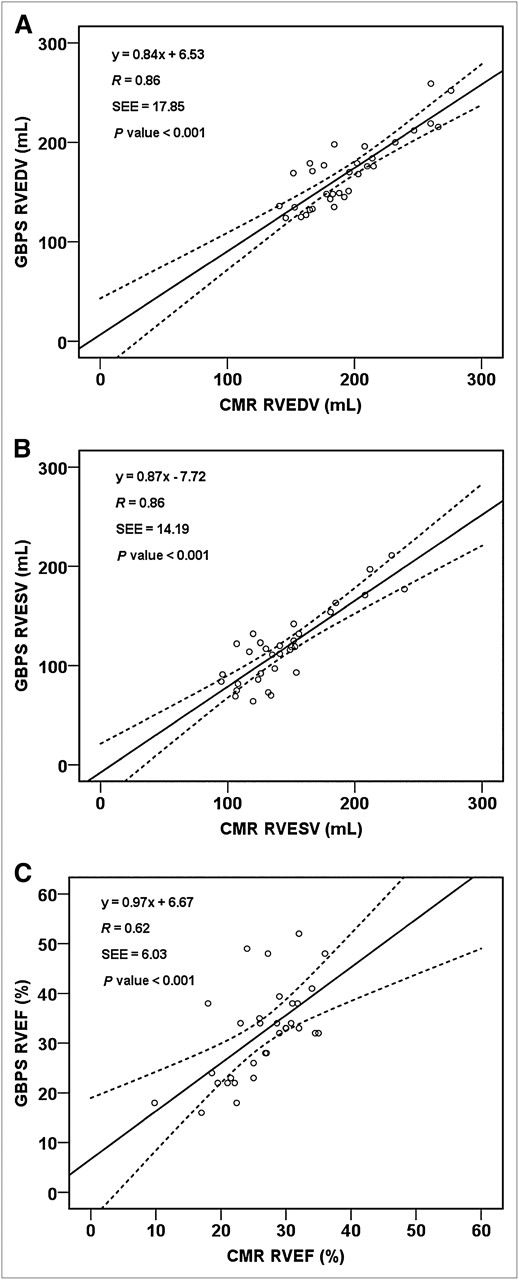
Linear regression of RV EDV (A), RV ESV (B), and RV EF (C) values from CMR and GBPS.

Bland–Altman plots of RV EDV (A), RV ESV (B) and RV EF (C) values from CMR and GBPS.
GBPS-calculated mean RV EF was statistically higher than values obtained from CMR (32% ± 9% vs. 26% ± 6%; P < 0.001). The Pearson correlation coefficient of RV EF between GBPS and CMR was 0.62 (P < 0.001) (Fig. 3C). Bland–Altman analysis revealed that GBPS overestimated RV EF (6% ± 7%; bias significantly different from 0, P < 0.001). Compared with CMR, GBPS showed a trend toward higher RV EF with increasing magnitude of RV EF, as noted on the Bland–Altman plot (y = 0.53x − 9.63; r = 0.50, P = 0.004). The 95% limit of agreement was −8.8% to 20.1% between GBPS and CMR (Fig. 4C).
Influence of Ventricular Volumes on Estimation of RV Parameters by GBPS
Analyzing the results, we found that patients with a markedly enlarged left ventricle and relatively smaller right ventricle were more likely to show a larger magnitude of bias in the assessment of RV indices than were patients with similarly sized right and left ventricles. To assess the degree of bias between these 2 methods, we adopted deviational parameters, defining them as follows: deviation of RV EDV = (GBPS RV EDV – CMR RV EDV)/CMR RV EDV × 100%; deviation of RV ESV = (GBPS RV ESV – CMR RV ESV)/CMR RV ESV × 100%; and deviation of RV EF = (GBPS RV EF – CMR RV EF)/CMR RV EF × 100%. Thus, the more the parameter deviated from a score of 0, the larger the bias was between the 2 methods.
Linear regression yielded correlations between the ratio of RV EDV to LV EDV and the degree of deviations of the measured values (r = 0.61 for the deviation of RV EDV, r = 0.68 for the deviation of RV ESV, and r = −0.55 for the deviation of RV EF; all P < 0.001). These results indicated that there was a significant trend for RV EDV and RV ESV to be underestimated and RV EF to be overestimated by GBPS as the ratio of RV to LV volume decreased. Because of different trend slopes (0.41 for the deviation of RV EDV; 0.67 for the deviation of RV ESV), RV ESV was more vulnerable than RV EDV to the variation of ventricular size ratio.
Reproducibility
Tables 3 and 4 present the reproducibility of LV and RV parameters measured by GBPS and CMR, respectively. Both intra- and interobserver comparisons between repeated measurements of biventricular functional parameters show significant correlations in GBPS and CMR. For GBPS, between the same observer, r was 0.99 for LV EDV, LV ESV, LV EF, and RV EF and 0.97 for RV EDV and RV ESV; and between different observers, r was 0.98 for LV EDV, LV ESV, and LV EF; 0.96 for RV EDV and RV ESV; and 0.95 for RV EF (all P < 0.001). For CMR, between the same observer, r was 0.99 for LV EDV and LV ESV, 0.98 for LV EF, 0.97 for RV EDV and RV ESV, and 0.96 for RV EF; and between different observers, r was 0.98 for LV EDV and LV ESV, 0.97 for LV EF, 0.95 for RV EDV, 0.94 for RV ESV, and 0.92 for RV EF (all P < 0.001). No statistically significant differences were found between repeated measurements of any parameters (all P > 0.1).
Reproducibility of GBPS Parameters
Reproducibility of CMR Parameters
DISCUSSION
Prior studies have demonstrated correlation between GBPS and CMR for the assessment of LV indices (17,18,25,26). Although these studies enrolled heterogeneous patients with normal and abnormal left ventricles, it remained unclear whether GBPS correlated with CMR in a restricted DCM population with enlarged left ventricles. By investigating patients with markedly dilated LV dysfunction, Akinboboye et al. (16) compared GBPS with CMR. They demonstrated correlation coefficients of 0.81, 0.84, and 0.93 for the estimation of LV EF, LV EDV, and LV ESV, respectively, between these 2 methods. Similar to the findings of Akinboboye et al., we found GBPS correlated well with CMR for the assessment of LV parameters in DCM patients. However, LV volumes were underestimated, and the limits of agreement were considerably wide. Several factors may explain these findings. The first factor is the self-attenuation by the blood pools, especially in markedly dilated ventricles. Second, the acquisition with 180° orbit, as had been previously emphasized (27), would result in an underestimation of ventricular volumes compared with 360° acquisition. Third, 8-frame GBPS, compared with the higher temporal resolution of CMR (25 phases per cardiac cycle), may have also increased the bias of LV volumes as it contained residual volume from systole–diastole on either side. Last, the inclusion of trabeculation and papillary muscles in drawing CMR LV endocardial contours exaggerated true cavity volume.
Different from the LV volumetric estimation, the measurement of LV EF between GBPS and CMR yielded no statistical difference, with narrow limits of agreement. The count-based calculation of GBPS may explain such an outcome, because the influence of self-attenuation may be equal both in diastole and in systole in severely reduced ventricular function, thus resulting in a negligible effect on LV EF.
Unlike the relatively simple left ventricle shape, the shape of the right ventricle is difficult to approximate to a certain geometry; therefore, only few imaging methods can evaluate RV parameters. In this respect, GBPS has the potential advantage of deriving RV volumes by count-based approaches rather than by geometric considerations. In a recent investigation, Sibille et al. (18) reported that RV parameters assessed by GBPS correlated well with those obtained by CMR (r = 0.80 for RV EDV, 0.86 for RV ESV, and 0.74 for RV EF). And Nichols et al. (19) demonstrated greater correlation coefficients between these 2 methods in patients with primary pulmonary hypertension or tetralogy of Fallot (r = 0.94 for RV EDV, 0.93 for RV ESV, and 0.85 for RV EF). Our study reconfirmed the significant correlation between GBPS and CMR. And we found that the differences in RV indices were more significant in patients with large left ventricles but relatively smaller right ventricles. Several reasons may explain these results. First, the enlarged right ventricle may facilitate the separation of left and right ventricles with thicker septa by a count-threshold approach (19). Contrarily, the smaller right ventricle may partially emerge into the dilated left ventricle at end-systole and make it difficult to identify the contour because of the limited spatial resolution of SPECT. From this perspective, RV ESV would be underestimated to a greater degree than would RV EDV and lead to an overestimation of RV EF. Second, the influence of self-attenuation may be more significant in patients with a relatively smaller RV because the dilated left ventricle would push the right ventricle to a greater depth. Third, no uniform rule for the assignment of the pulmonary valve plane in the postprocessing of both GBPS and CMR existed, thus potentially increasing the variation in results between these 2 modalities. Last, the acquisition protocol with 180° orbit and 8 frames may have also contributed to the bias of RV indices, similar to the bias of LV parameters.
There were some limitations to this study. First, although the 8-frame GBPS method requires less data storage and a shorter processing time than 16-frame (or more) GBPS, the latter may provide more accurate determinations of biventricular parameters, with higher temporal resolution (28). Second, it was proposed that 360° acquisition may offer more accurate results than 180° GBPS by increasing the sampling of GBPS data (27). But the total acquisition time of 360° GBPS using a 2-head γ-camera was much longer than that of 180°, thus making such an approach unsuitable for patients with poor ventricular function. Third, this study was limited to a relatively small number of patients. To further validate the correlation between GBPS and CMR, an investigation involving larger groups of DCM patients is warranted.
CONCLUSION
Biventricular functional parameters measured by GBPS correlated well with values obtained from CMR in patients with DCM, with systematically lower end-diastolic and end-systolic LV and RV volumes. However, RV volumes and RV EF assessed by GBPS should be cautiously interpreted.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 5, 2012.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication July 22, 2011.
- Accepted for publication November 29, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.