


Abstract
Previous radiation therapy of the liver is a contraindication for performing 90Y microsphere radioembolization, and its safety after internal radiation exposure through peptide receptor radionuclide therapy (PRRT) has not yet been investigated. Methods: We retrospectively assessed a consecutive cohort of 23 neuroendocrine tumor (NET) patients with liver-dominant metastatic disease undergoing radioembolization with 90Y microspheres as a salvage therapy after failed PRRT. Toxicity was recorded throughout follow-up and reported according to Common Terminology Criteria for Adverse Events (version 3). Radiologic (response evaluation criteria in solid tumors), biochemical, and symptomatic responses were investigated at 3 mo after treatment, and survival analyses were performed with the Kaplan–Meier method (log-rank test, P < 0.05). Results: The median follow-up period after radioembolization was 38 mo (95% confidence interval, 18–58 mo). The mean previous cumulative activity of 177Lu-DOTA-octreotate was 31.8 GBq. The mean cumulative treatment activity of 90Y microspheres was 3.4 ± 2.1 GBq, administered to the whole liver in a single session (n = 8 patients), in a sequential lobar fashion (n = 10 patients), or to only 1 liver lobe (n = 5 patients). Only transient, mostly minor liver toxicity (no grade 4) was recorded. One patient (4.3%) developed a gastroduodenal ulcer (grade 2). The overall response rates for radiologic, biochemical, and symptomatic responses were 30.4%, 53.8%, and 80%, respectively. The median overall survival was 29 mo (95% confidence interval, 4–54 mo) from the first radioembolization session and 54 mo (95% confidence interval, 47–61 mo) from the first PRRT cycle. A tumor proliferation index Ki-67 greater than 5% predicted shorter survival (P = 0.007). Conclusion: Radioembolization is a safe and effective salvage treatment option in advanced NET patients with liver-dominant tumor burden who failed or reprogressed after PRRT. The lack of relevant liver toxicity despite high applied 90Y activities and considerable previous cumulative activities of 177Lu-octreotate is noteworthy and disputes internal radiation exposure by PRRT as a toxicity risk factor in subsequent radioembolization.
- neuroendocrine tumors
- radioembolization
- peptide receptor radionuclide therapy
- 177Lu-DOTA-octreotate
- 90Y microspheres
Peptide receptor radionuclide therapy (PRRT) is an effective systemic treatment modality for metastatic gastroenteropancreatic neuroendocrine tumors (NETs) and is frequently performed as a first- or second-line therapy in progressive or functionally uncontrolled disease (1,2). The compound [177Lu-DOTA0,Tyr3]-octreotate (177Lu-octreotate) is often used for this purpose, with outstanding response and survival data available (1,3). Eventually, patients will progress again after a certain period of remission or disease stabilization, and a liver-dominant metastatic pattern—qualifying the patient for liver-directed therapy—may frequently persist over the course of disease.
Radioembolization with 90Y microspheres (90Y-RE) is a safe and effective treatment form for unresectable liver malignancy (4,5). Liver toxicity is encountered with an overall low incidence (6–9). Known risk factors are previous intraarterial therapy, chemotherapy, and high applied activities per target volume (7,9,10). Intraarterial delivery of β-emitting 90Y-loaded microspheres yields tumor-targeted internal radiation depending on the preferential arterial tumor vascularization. NETs are perfectly suited for transarterial treatment, and in particular for radioembolization, because of their typically prominent hypervascularity (11–13). The efficacy and safety of 90Y-RE have been demonstrated in this tumor entity (14–21), including patients after bland arterial embolization (22). However, no data are available on the safety of 90Y-RE after internal radiation with targeted radionuclide treatment.
Previous external-beam therapy accounting for hepatic radiation exposure constitutes a known relative contraindication for radioembolization (23,24). Whether there is an analogy to internally induced radiation exposure implying a clinical caveat to subsequent radioembolization is of major interest for the management of NET patients. Although previous PRRT does not yet constitute a formal contraindication for performing radioembolization, the question of whether 90Y-RE is safe and effective in patients for whom PRRT has failed has not been investigated but remains of high clinical relevance. We addressed this issue with a retrospective study assessing outcome and toxicity of 90Y-RE after previous PRRT.
MATERIALS AND METHODS
The efficacy and toxicity of 90Y-RE in patients after previously performed PRRT was retrospectively investigated from a single-center experience. For this purpose, a review and analysis of all patients being treated with radioembolization after PRRT in our institution were performed. The study was performed in accordance with the Declaration of Helsinki and with national regulations. Patients had provided informed consent for the scientific analysis of their data. Approval by the institutional review board is not required for retrospective studies on nonexperimental interventions at the authors’ institution. However, explicit approval from the local ethics committee was obtained for the prospective and retrospective assessment of outcome of NET patients throughout follow-up in our institution, including this retrospective investigation.
Patients
We evaluated 23 consecutive patients undergoing radioembolization at our institution after previous administration of PRRT. All patients had unresectable gastroenteropancreatic NET with liver-dominant disease. Apart from 1 patient, there was bilobar tumor spread. The baseline patient and tumor characteristics are given in Table 1. Inclusion criteria for radioembolization of gastroenteropancreatic NET patients were liver-dominant disease with regard to prognosis or symptoms, an Eastern Cooperative Oncology Group performance score of 0–2, an adequate liver function (bilirubin < 2 mg/dL, albumin > 3 mg/dL, no severely impaired PT/PTT), progressive or functionally uncontrolled disease despite standard treatment (surgery, chemotherapy, somatostatin analogs), absence of excessive lung shunting (<30 Gy calculated lung dose), and both favorable tumor uptake and missing intraabdominal shunting on 99mTc-macroaggregated albumin (MAA) imaging after diagnostic angiography. In our cohort, 19 patients were progressive by size or number according to Response Evaluation Criteria in Solid Tumors before implementation of 90Y-RE, and 4 patients were treated because of persistent hormone hypersecretion. Tumor-induced ascites was not seen as a contraindication to treatment and in fact were present in 3 patients. The portal vein was patent in all patients, although portal vein occlusion was not an exclusion criterion for treatment in our institution. Informed consent was obtained from all patients before evaluation (MAA angiogram) and each radioembolization session.
Baseline Characteristics
PRRT
PRRT was performed with 177Lu-DOTA-octreotate (177Lu-octreotate) at our institution using a common methodology as described in previous reports (25,26). Inclusion criteria for treatment with PRRT were histologically confirmed, unresectable, metastatic gastroenteropancreatic NET; sufficient tracer uptake (≥ normal liver) on baseline somatostatin receptor imaging; a glomerular filtration rate of more than 30 mL/min/1.73 m2; a white blood count of 2 × 109/L or more; and platelets more than 70 × 109/L. PRRT was performed by the administration of a mean activity of 7.9 GBq of 177Lu-octreotate per treatment cycle, aimed at 4 courses at standard intervals of 3 mo (10–14 wk). The 177Lu (IDB Holland) had a specific activity in the approximate range of 100–160 GBq/μmol at the time of administration. Peptide labeling (27,28) was performed to obtain an apparent specific activity of about 54 GBq/μmol (ratio of activity to the total amount of peptide). Nephroprotection was implemented with standard amino acid coinfusion according to the Rotterdam protocol (2.5% lysine and 2.5% arginine in 1 L of 0.9% NaCl; infusion of 250 mL/h) (29,30). Short-acting somatostatin analogs were required to be paused 1 d before administration of 177Lu-octreotate and long-acting analogs a minimum of 6 wk before PRRT. Informed consent was obtained from all patients before the initiation of therapy and before the administration of each treatment cycle.
Radioembolization Procedure
The radioembolization was always performed after exclusion of any intraabdominal and excessive pulmonary (lung-shunt fraction) deposition by a pretreatment diagnostic angiogram with planar and SPECT/CT MAA imaging after an intraarterial injection of 200–400 MBq of 99mTc-MAA. Aberrant vessels were coil-embolized before MAA injection to depict the flow expected in the treatment session. The treatment was performed 1–2 wk after diagnostic angiography. Resin microspheres (SIR-Spheres; SIRTEX Medical) were used in 21 patients and glass microspheres (TheraSphere; MDS Nordion) in 2 patients. The liver was treated either in a single session (whole liver, n = 8 patients; unilobar, n = 5 patients) or in a sequential lobar fashion (n = 10 patients). The prescription of activity was derived from the partition model (standard target dose, 120 Gy) and the body surface area method for treatment with glass and resin spheres, respectively. The administration of resin spheres was performed under intermittent or continuous fluoroscopic control; marked reduction of forward-flow or eminent stasis led to the termination of treatment, irrespective of the amount of activity given at that time point. Posttreatment 90Y bremsstrahlung imaging was performed to document target accumulation. Standard periinterventional medication included dexamethasone (4 mg twice daily for 2 d), ondansetron (8 mg intravenously during treatment), and pantoprazole (40 mg daily for 2 mo). Somatostatin analog medication in patients with poorly controlled tumor function was not discontinued but frequently intensified in the peri- and postprocedural period to avoid a potential tumor lysis–induced hormonal crisis.
Assessment of Toxicity
Pre- and posttreatment laboratory tests included liver and renal function tests and complete blood counts. In addition to the outpatient laboratory tests from the referring physician every 2–3 wk for the first 2 mo and every 4 wk until 6 mo after treatment, a complete work-up was performed at regular follow-up visits in our department at 1, 3, and 6 mo after treatment. Clinical toxicities including pain, fever, fatigue, and gastrointestinal adverse events were assessed by thorough in-patient postinterventional and follow-up documentation including all recorded complaints and findings at the regular follow-up visits. The toxicity was classified according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE; version 3.03).
Assessment of Response to Treatment
Patients were restaged at 3 mo after treatment with CT or MRI. The radiographic imaging results were reevaluated by experienced radiologists to classify tumor response according to the Response Evaluation Criteria in Solid Tumors. Apart from this response categorization, restaging was supplemented by somatostatin-receptor imaging in 19 patients using 111In-diethylenetriaminepentaacetic acid-octreotide (OctreoScan; Tyco Healthcare) or 68Ga-DOTATOC PET/CT. Biochemical response was evaluated according to chromogranin A (CgA) plasma levels if they were significantly elevated at baseline (i.e., >150 ng/mL) (complete response being normalization of the CgA level [i.e., <110 ng/mL], partial response being more than 50% reduction but still elevated CgA level, stable disease being <50% change in CgA, and progressive disease being >50% increase in CgA). For the assessment of symptomatic response, frequency or intensity of symptoms related to tumor-specific hormone production, such as diarrhea and flushing in carcinoid syndrome, were documented at our institution at baseline and each follow-up visit at 1, 3, and 6 mo after treatment.
Survival Assessment and Statistical Analysis
Survival analyses were performed with the Kaplan–Meier method; overall survival (OS) was assessed from the start of radioembolization (first treatment session) and also for additional information from the start of PRRT (first treatment cycle). Any death was considered as an event for OS, irrespective of the cause. Survival outcomes were stratified by various variables and compared using the log-rank test. A P value of less than 0.05 was considered significant. SPSS software (version 18.0; SPSS) was used for all statistical calculations.
RESULTS
The median follow-up period after the first radioembolization session was 38 mo (95% confidence interval [CI], 18–58 mo). Thirteen of the 23 patients were still alive at the time of analysis. The mean treatment activity per patient was 3.4 ± 2.1 GBq, applied over 1.7 ± 1.1 treatment sessions.
The common acute adverse events within the first 3 d of treatment—abdominal pain, fever, nausea, and vomiting—were transient, and each occurred in less than 15% of the patients (grade 3), as listed in Table 2. No serious delayed toxicities according to CTCAE were noted. One of the 23 patients (4.3%) developed a gastroduodenal ulcer (CTCAE grade 2), although no apparent culprit vessel or corresponding MAA accumulation was identified on pretreatment imaging, even on retrospective review. No case of treatment-induced death or radiation-induced liver disease was observed. No hormone-related crises in functional tumors were recorded. The lung-shunt fraction was calculated to be less than 10% in all patients, and no pulmonary toxicity was observed.
Toxicities After Radioembolization According to CTCAE (Version 3.0) in Percentage per Patient
Radiologic imaging at restaging yielded a partial response in 7 patients (30.4%), stable disease in 14 (60.9%), and progressive disease in 2 (8.7%). Receptor-mediated functional imaging, when performed, indicated a significant remission in 11 of 19 patients (57.9%), stable disease in 6 (31.6%), and progressive disease in 2 (10.5%). Figure 1 shows imaging results for a patient with hepatic metastases of a pancreatic NET. Biochemical response according to CgA plasma levels, when available and elevated at baseline, comprised complete response (normalization of CgA) in 1 of 13 patients (7.7%), partial response (>50% reduction of elevated CgA) in 6 patients (46.2%), stable disease in 5 patients (38.5%), and progressive disease in 1 patient (7.7%). Symptomatic control in previously uncontrolled functionality was achieved in 4 of 5 patients (80%).

Pre- and posttreatment imaging of patient with progressive hepatic metastases (low tumor burden group; <25% liver infiltration) of pancreatic NET. Patient was treated by whole liver radioembolization in single session. MRI at baseline (A) and 3 mo after treatment (B) demonstrate partial remission. Intraprocedural angiogram (C) displays highly hypervascular tumor lesions before (left) and directly after (right) administration of 90Y microspheres, illustrating minor macroembolic effect of this treatment as opposed to primarily embolic therapeutic modalities such as bland embolization.
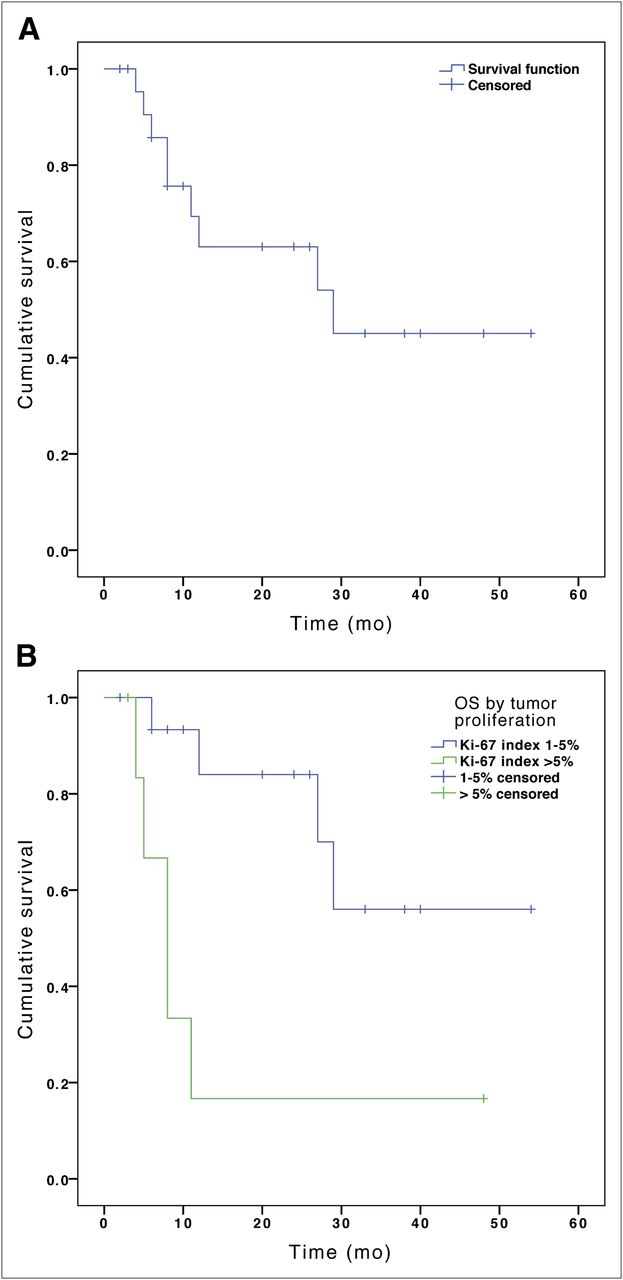
The median OS after implementation of radioembolization (Fig. 2A) was 29 mo (95% CI, 4–54 mo). Median OS from the start of PRRT was 54 mo (95% CI, 47–61 mo). From all investigated baseline factors including age, performance status, tumor type, hepatic tumor load, extrahepatic disease, tumor response, previous cumulative activity of 177Lu-octreotate, and administered 90Y activity per liter of target liver volume, only the tumor proliferation index significantly affected OS (Table 3). Patients with a Ki-67 index of greater than 5% survived a shorter time (median OS of 8 mo; 95% CI, 5–11 mo) than the remaining patients (median OS not reached after 54 mo; P = 0.007); the respective Kaplan–Meier curves are depicted in Figure 2B.
Univariate Analysis of Potential Factors Contributing to OS
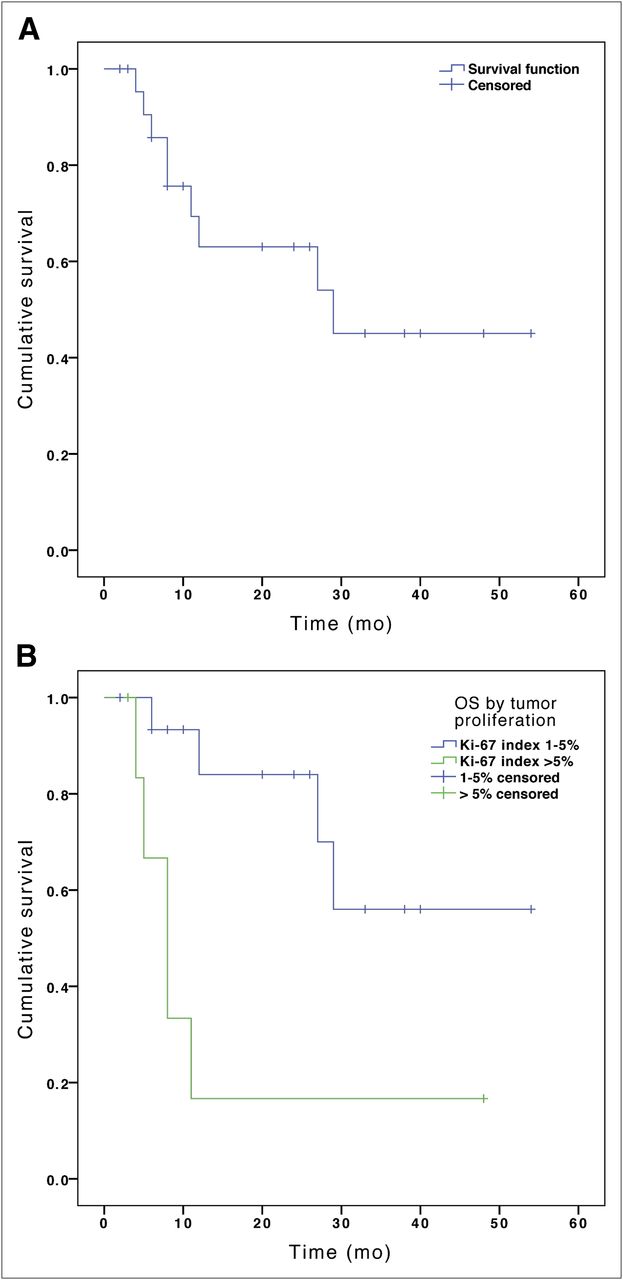
Cumulative survival after radioembolization illustrated by Kaplan–Meier curves. Median OS of entire cohort (A) was 29 mo (95% CI, 4–54 mo). When stratified by tumor proliferation index (B), median OS was 8 mo (95% CI, 5–11) in patients with index greater than 5%, whereas for Ki-67 of 5% or less, median OS was not reached after 54 mo (P = 0.007).
DISCUSSION
Our retrospective study indicates that 90Y-RE is a safe option in patients with a history of previous PRRT. The proposed restriction of 90Y-RE after hepatic radiation exposure such as external-beam therapy (23,24) does not seem to apply for this kind of internal radiation. The absence of any observed serious toxicity despite pretreatment with high applied total activities in our cohort disputes a major impact of the internally induced radiation dose and its significance for patient selection.
There is a substantial database demonstrating the efficacy of radioembolization in hepatic NET as found by prospective and retrospective studies (14–21). Most reported median OS rates range between 25 and 36 mo from treatment (14,16,18,19,21), median OS was not reached in 2 other reports after a median follow-up of 13–17 mo (17,20), and 1 large retrospective multicenter evaluation yielded an extraordinarily long median OS of 70 mo (15). Reported symptomatic and biochemical response rates were in the range of 75%–95% (17,19–21) and 45%–67% (17,19,20), respectively. Reported toxicities of clinical relevance were limited (grades 3–4, <15%) and mostly transient.
Patients with a history of previous internal radiation therapies such as PRRT, however, were rare (n = 4) in these reported series covering overall more than 300 NET patients (15–18,20,21). Our study confirms efficacy of 90Y-RE even in this advanced-metastatic patient group comprising exclusively individuals with reprogression or uncontrolled disease after systemic PRRT. Although radiologic response after 3 mo was less frequent (overall response rate, 30%) than in most series with PRRT-naïve patients (overall response rate, 50%–64%) (15–17,19,21), response is in line with a solid recent single-center report (20) stating a similar response rate of 22.5%.
The OS from the start of 90Y-RE observed in our cohort (median OS, 29 mo) appears to be in the lower range of the major NET radioembolization study outcomes (reported median OS, 25–36 mo). The potential negative selection bias should be kept in mind, because patients with a well-preserved somatostatin-receptor status and good outcome after PRRT would have been retreated with PRRT in our institution; so these individuals with relapsing and refractory disease obviously comprise a negatively selected cohort. Nevertheless, when calculated from the start of PRRT, the median OS in our series reaches 54 mo (95% CI, 47–61 mo). The only predictor of survival in this small cohort was the tumor proliferation index Ki-67 (Fig. 2B), whereas the other baseline factors, including age, performance status, tumor type, hepatic tumor load, presence of extrahepatic disease, tumor response, and previous cumulative activity of 177Lu-octreotate, did not affect survival in the univariate analysis. Remission status after 90Y-RE had only a mild predictive trend, with a median OS not reached after 41 mo in patients experiencing a partial response as opposed to a median OS of 12 mo for the remaining patients (with stable or progressive disease). The lack of significance might be explained by the group of stable-disease patients for whom NETs with a less overt tendency toward morphologic response (i.e., tumor shrinkage) were likely to be less rapidly proliferating and of the G1–G2 carcinoid type. A group of patients with this type of NETs had a potentially better long-term prognosis than those with responsive but higher proliferating tumors. However, the validity of the entire parameter exploration is obviously limited by the small patient number and considerable amount of variables.
Proposed risk factors for the development of serious toxicity after radioembolization are previous chemo- or intraarterial therapy, young age, and high applied activities relative to the targeted liver volume (7,9,10). In our cohort, serious toxicity (grade 4) did not occur, despite the frequency of advanced liver infiltration (>50% tumor load in 47.8% of patients), high activities per target liver tissue (mean, 1.8 GBq/L of target liver volume; 56.5% of patients with >1.5 GBq/L of target volume), and preexposure to internal radiation. In addition, 10 of 23 patients (53.5%) were pretreated with systemic or transarterial chemotherapy. One explanation for the lack of toxicity may be the hypervascular nature of NET, leading to pronounced preferential tumor-targeted flow and microsphere accumulation with sparing of healthy liver tissue. Our data suggest that 90Y-RE is a safe option in NET patients even after treatment with PRRT.
Hepatic radiation exposure in PRRT has generally not been seen as a concern for liver function (1,31,32). Reported absorbed doses of healthy liver tissue were mainly in the range of 0.1–0.3 Gy/GBq for 177Lu-based PRRT (33–35) and 0.5–1.0 Gy/GBq for 90Y-based PRRT (36–38). For our cohort, the cumulative organ dose to the healthy liver is estimated to be in the range of 2–12 Gy. To allow the addition of the 177Lu-octreotate– and 90Y-RE–associated doses, the biologic equivalent dose formalism would have to be used and respective values calculated (39,40), possibly allowing future toxicity prediction in multiple repeated PRRT or radioembolization treatment settings if a database for dose–toxicity relations were established for both treatment modalities. We speculate that the minor toxicologic relevance of liver-absorbed doses by 177Lu-based PRRT should translate well to 90Y-based PRRT, which will presumably be supported by future safety data.
The preferable treatment sequence (PRRT followed by 90Y-RE vs. 90Y-RE followed by PRRT) remains a matter of discussion. One may argue that liver-directed treatment such as 90Y-RE should be performed as long as tumor involvement is liver-dominant and PRRT is kept in reserve for later stages with more widespread disease. The argument for the reverse sequence is that radioembolization works also in less differentiated NET, whereas effective PRRT depends on pronounced somatostatin receptor overexpression subjected to a potential decline during the course of tumor disease. The ease of use and absence of risk of serious toxicity make PRRT the first-choice modality in somatostatin receptor–positive NET that is uncontrolled or progressive under somatostatin analog treatment, but there certainly is a need for individualized treatment, discussion, and decision making based on various factors, including the patient’s preference.
The retrospective nature of this study is an obvious limitation for estimating efficacy and toxicity. However, these initial results provide the first evidence of safety for 90Y radioembolization in patients with a history of PRRT. Prospective trials evaluating the benefit and safety of this sequence would be desirable to confirm these preliminary data. Also, the clinical benefit would be better determined using standardized quality-of-life assessment tools, such as the QoL-C30 or other NET-specific questionnaires. Another limitation is the absence of dosimetric data involved in this analysis. The establishment of a dose–toxicity relationship based on the healthy liver-absorbed dose from PRRT and radioembolization would be highly desirable, but with the lack of toxicity observed in our cohort this aim seems to be difficult to achieve.
CONCLUSION
90Y-RE is safe in patients with advanced liver-dominant NET and a history of internal radiation exposure by PRRT. 90Y-RE can be effective in inducing clinical, biochemical, and morphologic response even after the failure of potent systemic radiopeptide treatment. The lack of relevant liver toxicity despite high applied 90Y activities and considerable previous cumulative activities of 177Lu-octreotate is noteworthy and disputes internal radiation exposure by PRRT as a toxicity risk factor in subsequent radioembolization. The observed outcome in this significantly pretreated and negatively preselected population with overall advanced disease (>50% hepatic tumor burden in almost half of the patients) shows that radioembolization may clearly provide a salvage option for developed resistance to receptor-mediated internal radiation and suggests that PRRT be given before 90Y-RE as a feasible sequence.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 17, 2012.
- © 2012 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication April 20, 2012.
- Accepted for publication June 25, 2012.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Role of Adding Somatostatin Analogues to Peptide Receptor Radionuclide Therapy as a Combination and Maintenance Therapy
- Pitfalls in the response evaluation after peptide receptor radionuclide therapy with [177Lu-DOTA0,Tyr3]octreotate
- GEP-NETS UPDATE: Radionuclide therapy in neuroendocrine tumors
- The Efficacy of Hepatic 90Y Resin Radioembolization for Metastatic Neuroendocrine Tumors: A Meta-Analysis