


Abstract
Oncologic 18F-FDG PET/CT is rapidly gaining acceptance in clinical practice. However, the referring physician’s attitude toward the usefulness of this diagnostic modality is unknown. This survey was undertaken to collect information regarding the current perspective of referring physicians on oncologic PET/CT. Methods: We conducted a prospective worldwide, Web-based survey of physicians who manage cancer patients. A total of 963 referring physicians completed a 20-question survey focused on their experience with oncologic 18F-FDG PET/CT. Attention was directed toward their confidence about indications, their satisfaction with related educational resources, the quality of interaction with interpreting physicians, and practical problems encountered. The respondents included oncologists (38.5%, n = 371), hematologists (16.4%, n = 158), radiation oncologists (9.0%, n = 87), surgeons (30.3%, n = 292), and other physicians (5.7%, n = 55). Results: Only 25.2% of respondents considered the oncologic 18F-FDG PET/CT indications to be well established and defined. Frequent uncertainty about the need for a PET scan was indicated by 62.3% of the respondents. High cost and overinterpretation of findings were the most commonly reported concerns (47.0% and 40.9%, respectively). The experience and skill level of the interpreting physician was considered very important by 96.8% of the surveyed physicians. Conclusion: Referring physicians expressed considerable uncertainty about the appropriate use of oncologic PET/CT. Additional major concerns are procedure costs and quality of interpretation. The responses suggest a strong need for efforts to educate referring and interpreting physicians about the appropriate use of 18F-FDG PET/CT in oncology.
A growing body of evidence supporting the usefulness of PET/CT in oncology has resulted in an increasing clinical use of this technology. However, a lack of consistent national and international guidelines for the appropriate use of PET/CT with regard to clinical indications, imaging protocols, and image interpretation might have led to uncertainty on the side of referring clinicians about the best use of PET/CT.
Two recent surveys have evaluated national and international practice patterns of PET operations (1,2). However, there is a need to evaluate the referring physicians’ perceptions about the strengths and weaknesses of this imaging modality.
We therefore initiated a Web-based survey to document and explore the referring physician’s experience with PET/CT. Such surveys are now common in health care research and are especially important when addressing topics that are difficult to assess using other approaches (3–5).
The Web-based approach was selected because of its significant advantage for systematic data sampling, wide distribution, and ease of computerized data analysis (6,7). Web-based questionnaires have the capacity to provide valuable quantitative and qualitative scientific information and are fully capable of providing reliable data collection (8–10).
The current survey was designed to assess the referring physician’s perception of the use of PET/CT.
MATERIALS AND METHODS
This Web-based survey addressed physicians who manage oncologic patients. It was initiated in June 2011 through a request for participation that was e-mailed to corresponding authors of major clinical oncologic journals. Their e-mail addresses were harvested from their publications listed in PubMed. The e-mail invitation was addressed only to physicians involved in the care of cancer patients.
A Web link was provided for direct, single-click access to the survey, which consisted of 20 multiple-choice questions and an open text field for general comments. The survey was constructed using a commercially available questionnaire platform (SurveyMonkey; http://www.surveymonkey.com/). The questions were developed by multiinstitutional PET/CT experts (the authors) with 2–11 y of clinical experience with PET/CT.
The survey inquired about clinician’s perceptions and experience regarding indications for oncologic PET/CT (satisfaction with available resources, confidence when referring a patient), the quality and value of communication with interpreting physicians, the quality of PET/CT reports, and key problems encountered with this imaging modality. The questions were sequenced in such a way that the clinical flow was followed (from deciding on ordering to using the results of PET/CT). Finally, the survey included some demographic questions.
The questions of the survey were as follows:
Do you feel that the indications for oncologic PET/CT are well established and defined in medicine?
Are updates on the indications for oncologic PET/CT easily accessible to referring physicians?
How often do you think that referring physicians are uncertain about the actual need for a PET/CT scan?
When uncertain about ordering a PET/CT scan, consultation with an imaging expert (nuclear medicine physician, radiologist) is … . (choices were given on how helpful such a consultation is considered).
Considering the clinical value of PET/CT, how important do you think it is for the interpreting physician to have an accurate and detailed clinical history available?
On the PET/CT reports, how important is the differential diagnosis of the PET/CT abnormalities?
Regarding the differential in PET/CT reports, you prefer … . (choices were given on the preferable extent of the differential).
How critical is the experience and skill level of the interpreting physician?
Do you read the entire description of findings (apart from the final impression) in a PET/CT report?
How important is it for you to have images available for personal review?
Do you feel that important technical terms (e.g., attenuation artifact or SUV) have been adequately explained and are clear to you?
Are you satisfied overall with the PET/CT reports that you receive?
How often do you think that there is a need to contact the interpreting physician to discuss the results?
Are you satisfied overall with the accessibility that you have to PET/CT experts (nuclear medicine physicians, nuclear radiologists)?
When you do contact a PET/CT expert regarding PET/CT studies, how often are you satisfied with the communication?
Do you think that more interaction between the referring and the interpreting physicians would benefit patients?
In general, what is (are) the main problem(s) that you encounter with oncologic PET/CT as an imaging modality?
What is your specialty?
For how many years have you been practicing your specialty?
For approximately how long has PET or PET/CT been available for your patients?
A reminder to complete the survey was e-mailed within 7–33 d. Repeat responses were prevented by a software program denying access to recipients who had already completed the survey. Data collection was completed 8 wk after the distribution of the reminder e-mail. Responses from physicians not involved in cancer care were excluded.
The collected data were analyzed quantitatively by the creation of appropriate cross tabulations. The results are discussed, and their implementations are analyzed.
RESULTS
A total of 19,053 invitations for participation in the survey were delivered. Of the recipients, 242 declared noneligibility or refused participation. A reminder invitation by e-mail was sent to the remaining 18,811.
Of the 981 recipients who completed the questionnaire, 18 were not eligible for inclusion in the analysis. Of those, 6 were radiologists, 4 were nuclear medicine physicians, and 8 were not practicing physicians or did not indicate their specialty. Thus, a total of 963 of the addressees who completed the survey were included in the analysis.
Demographics
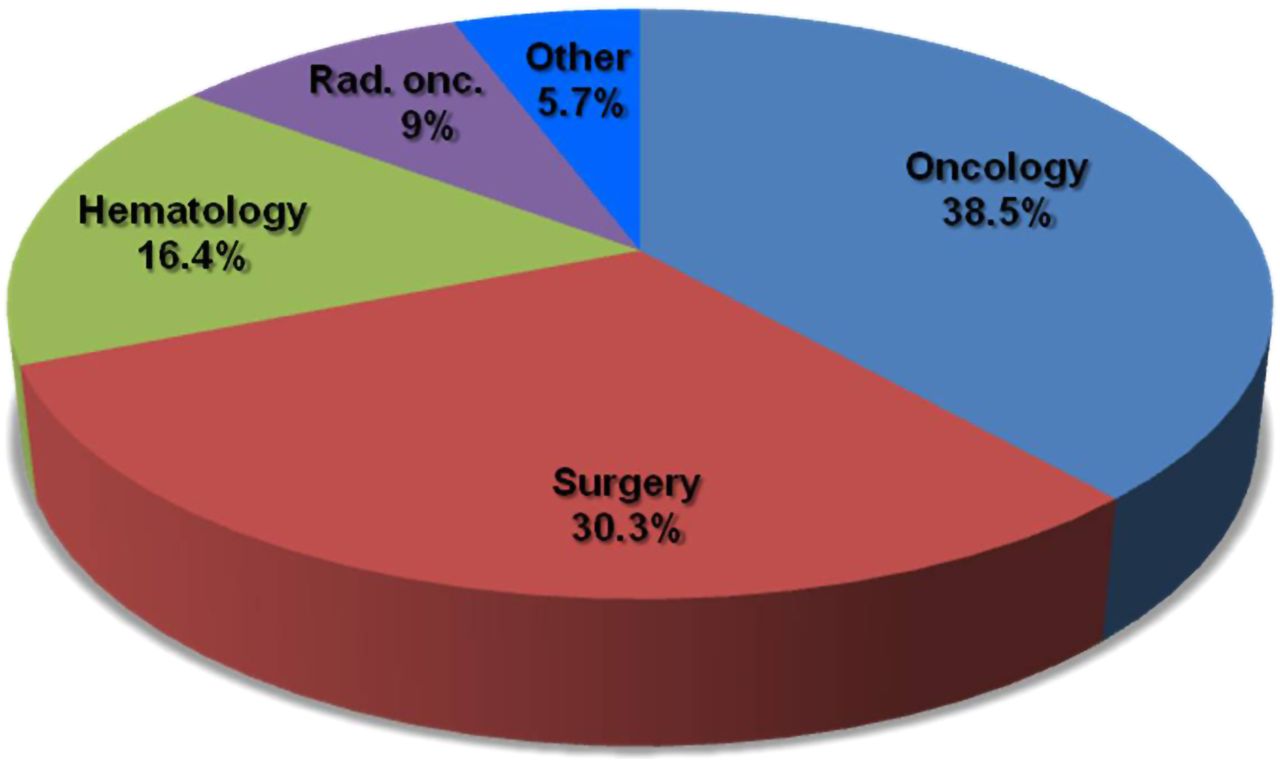
Of the 963 eligible participants, 38.5% (371) were oncologists, 30.3% (292) were surgeons, 16.4% (158) were hematologists, and 9.0% (87) were radiation oncologists. The remaining 5.7% (55) had various backgrounds, including 7 internists, 6 pulmonologists, 6 endocrinologists, 5 gastroenterologists, 5 infectious disease specialists, 4 dermatologists, 4 primary care or general practice physicians, 3 geriatric specialists, 2 intensivists, 2 pediatricians, 2 neurologists, 2 palliative medicine physicians, 2 pathologists, 2 with no specialty, 1 rheumatologist, 1 public health specialist, and 1 oral medicine specialist. Figure 1 provides a summary of the participants’ specialties.
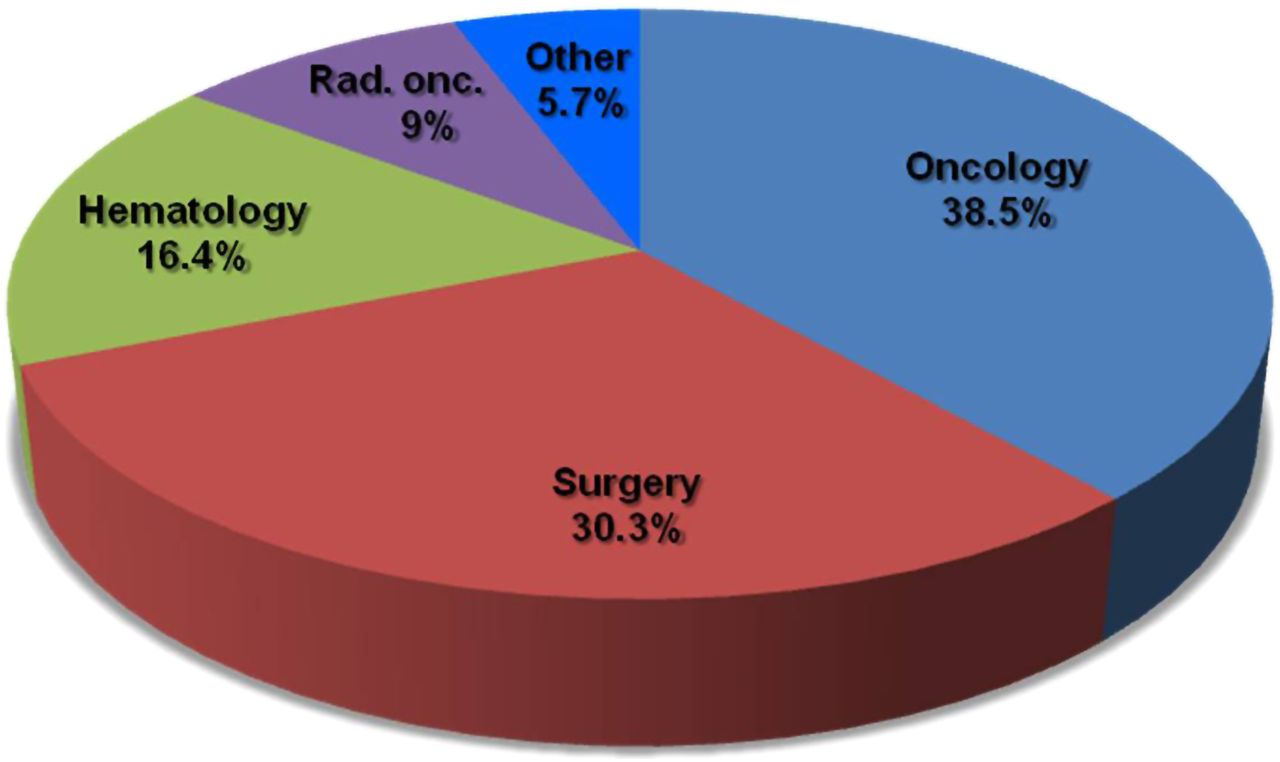
Participants’ specialty (question 18).
Regarding the geographical distribution, 53.1% (511) were from Europe, 32.8% (316) from North America, 10.3% (99) from Asia, 2.0% (19) from Australia and New Zealand, 1.1% (11) from South America, and 0.7% (7) from Africa.
A total of 66.1% of the participants had more than 10 y of experience practicing their specialty, 19.1% had 5–10 y, 11.9% had less than 5 y, and 2.9% were still in training.
PET or PET/CT was available to their patients for more than 5 y in the institutions of 75.6% of the participants. For each question there were a limited number of participants who did not provide a response.
Familiarity with PET Indications
Only 25.2% of the respondents (242/960) felt that indications for PET/CT are well defined and established. Of these, only 3.6% (35/960) were highly confident about indications.
For 48.9% of the respondents (470/961), information about PET/CT indications was only “sometimes” easily accessible to referring physicians, whereas 18.6% (179/961) felt that this information is “very rarely” or “never” easily accessible. Only one third of the respondents (32.4%, 312/961) answered in a positive way (“in most of the cases” or “absolutely” accessible).
Uncertainty about indications always or in most cases was declared by 16.2% of respondents (155/959), whereas 46.1% (442/959) indicated frequent (“in many cases”) uncertainty. Therefore, a total of 62.3% of the respondents indicated at least a frequent uncertainty when deciding about the need for a PET scan. Some uncertainty was declared by 33.1% (317/959), whereas 4.6% (44/959) were only rarely uncertain. No uncertainty was expressed by only a single respondent. The graphs of the participants’ responses to these questions are shown in Figure 2.
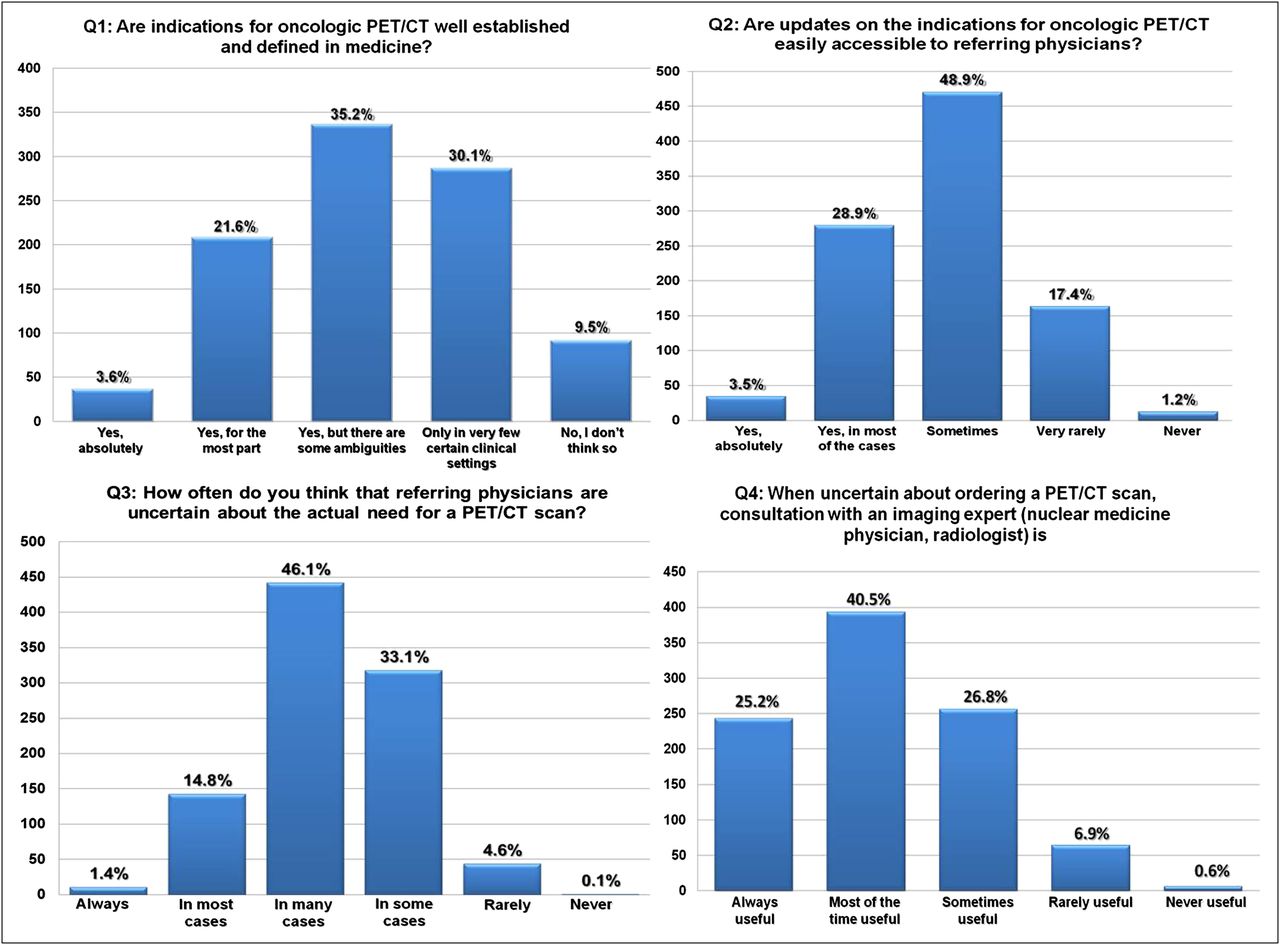
Responses to survey questions 1 through 4.
Communication with Interpreting Physician
Consultation with an imaging expert in cases of uncertainty before ordering a PET scan (question 4, Fig. 2) was considered useful always or most of the time by 65.7% of the respondents (25.2% and 40.5%, respectively), sometimes useful by 26.8%, and rarely or never useful by 7.5% (6.9% and 0.6%, respectively).
Regarding the clinical importance of providing an accurate and detailed history to the interpreting physician (question 5, Fig. 3), 69.0% ranked it of highest importance (essential), and 21.6% evaluated it as very important. These add up to a significant 90.6%.

Responses to survey questions 5 through 8.
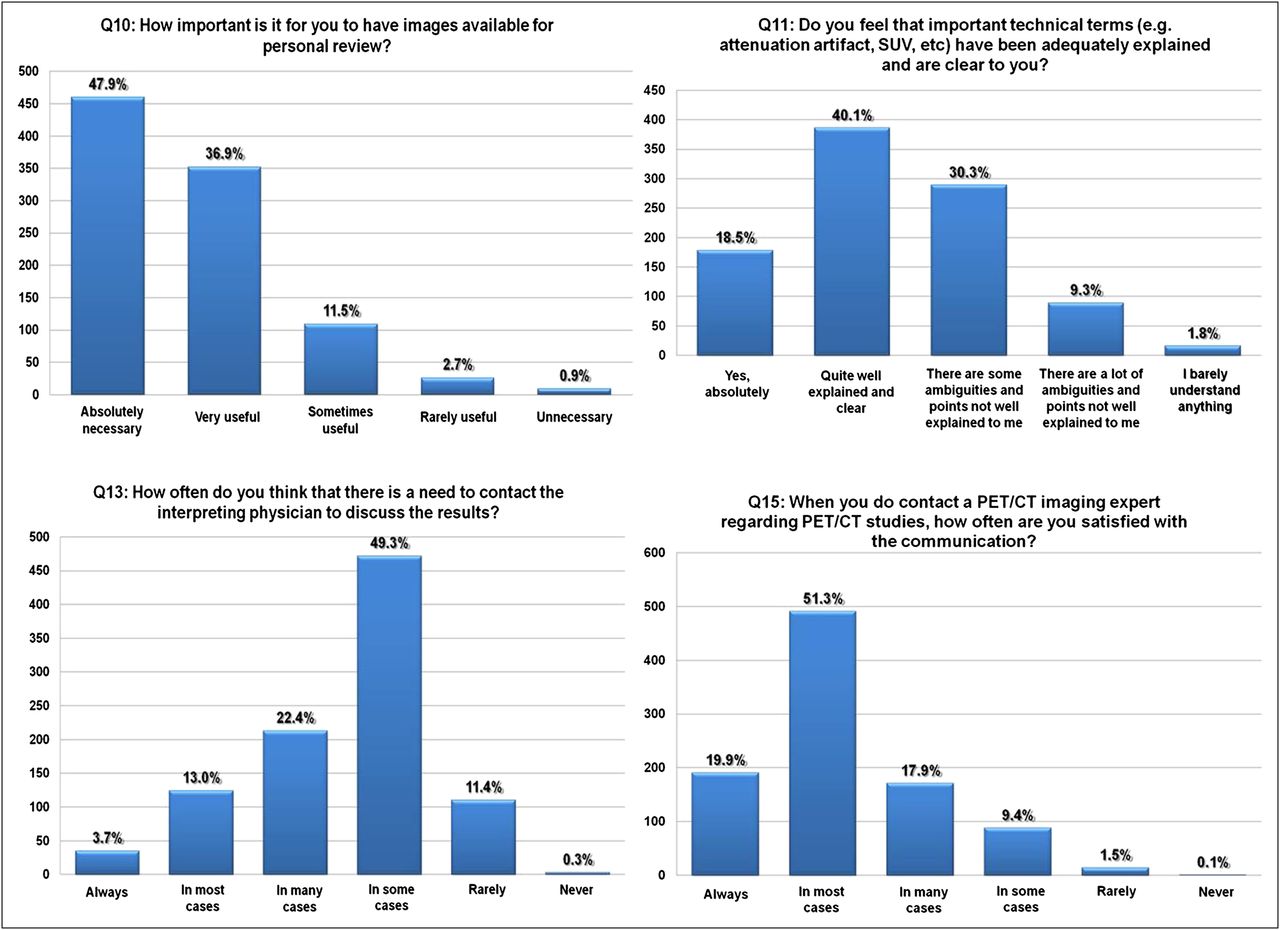
Contact with the imaging expert was also considered important after receiving the report; the need for discussing results with an imaging expert (question 13, Fig. 4) was uncommon in only 11.7% (rarely, 11.4%; never, 0.3%). A sporadic need to discuss the results with the interpreting physician was reported by 49.3%, whereas 39.1% reported at least a frequent necessity for discussion.
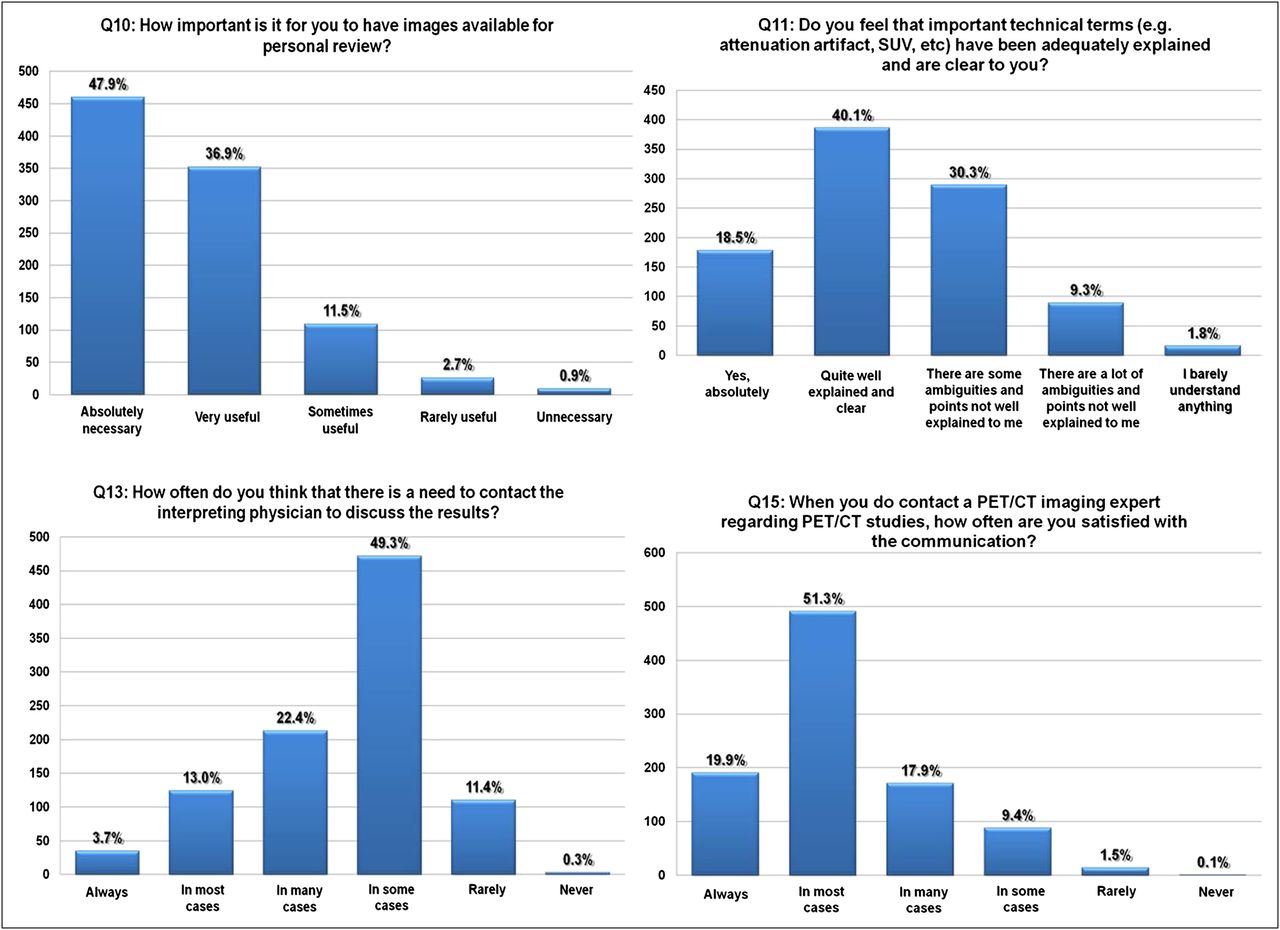
Responses to survey questions 10, 11, 13, and 15.
The accessibility of imaging experts for consultation was deemed satisfactory; only 8.6% of respondents were not satisfied with how available imaging experts are, whereas 91.4% were fully (68.4%) or somewhat (23.0%) satisfied. Regarding their satisfaction with the quality of this contact (question 15, Fig. 4), only 1.6% was rarely or never satisfied. The rest expressed their frequent (89%) or partial (9.4%) satisfaction. Nevertheless, 96.3% of the respondents agreed that even more interaction between referring and interpreting physicians would benefit patients (question 16).
Quality of Reports
A differential diagnosis for PET/CT abnormalities on the report (question 6, Fig. 3) was considered important (absolutely important, extremely important, or very useful) by 86.0%. Only 1.9% considered a differential diagnosis rarely useful (1.7%) or unnecessary (0.2%).
An extensive, complete, and detailed differential diagnosis (question 7, Fig. 3) was preferred by 31.4%, whereas 66.0% preferred only the clinically relevant differential diagnosis. Only 2.6% of the respondents considered a differential diagnosis irrelevant. Rather than reading only the final impression, 60.5% of the participants always read the entire report (question 9). Only 1.3% rarely or never read the entire report.
The experience and skill level of the interpreting physician (question 8, Fig. 3) was rated as being of high importance and significance; 96.8% considered this factor to be either absolutely critical (52.7%) or very important (44.1%). “Somewhat important” was selected by only 3.1%, “not that important” by 0.2%, and “not important at all” by none.
The terms and expressions used in PET reports were absolutely (18.5%) or quite (40.1%) familiar to 58.6% of respondents (question 11, Fig. 4). However, 30.3% reported ambiguity, poor explanations, and lack of familiarity with the report terminology, and 11.1% expressed a very low level of comprehension.
A strong desire for having access to the PET/CT images was expressed by 84.8% of surveyed physicians (question 10, Fig. 4). More specifically, 47.9% deemed this access as absolutely necessary and 36.9% as very useful. Only 3.6% thought that being provided with images was rarely useful (2.7%) or unnecessary (0.9%).
The overall satisfaction with PET/CT reports (question 12) was reasonably high, with 66.2% of the participants being satisfied either always (4.4%) or in most cases (61.8%). Only 1.4% of the participants declared that they were rarely satisfied.
Problems Encountered
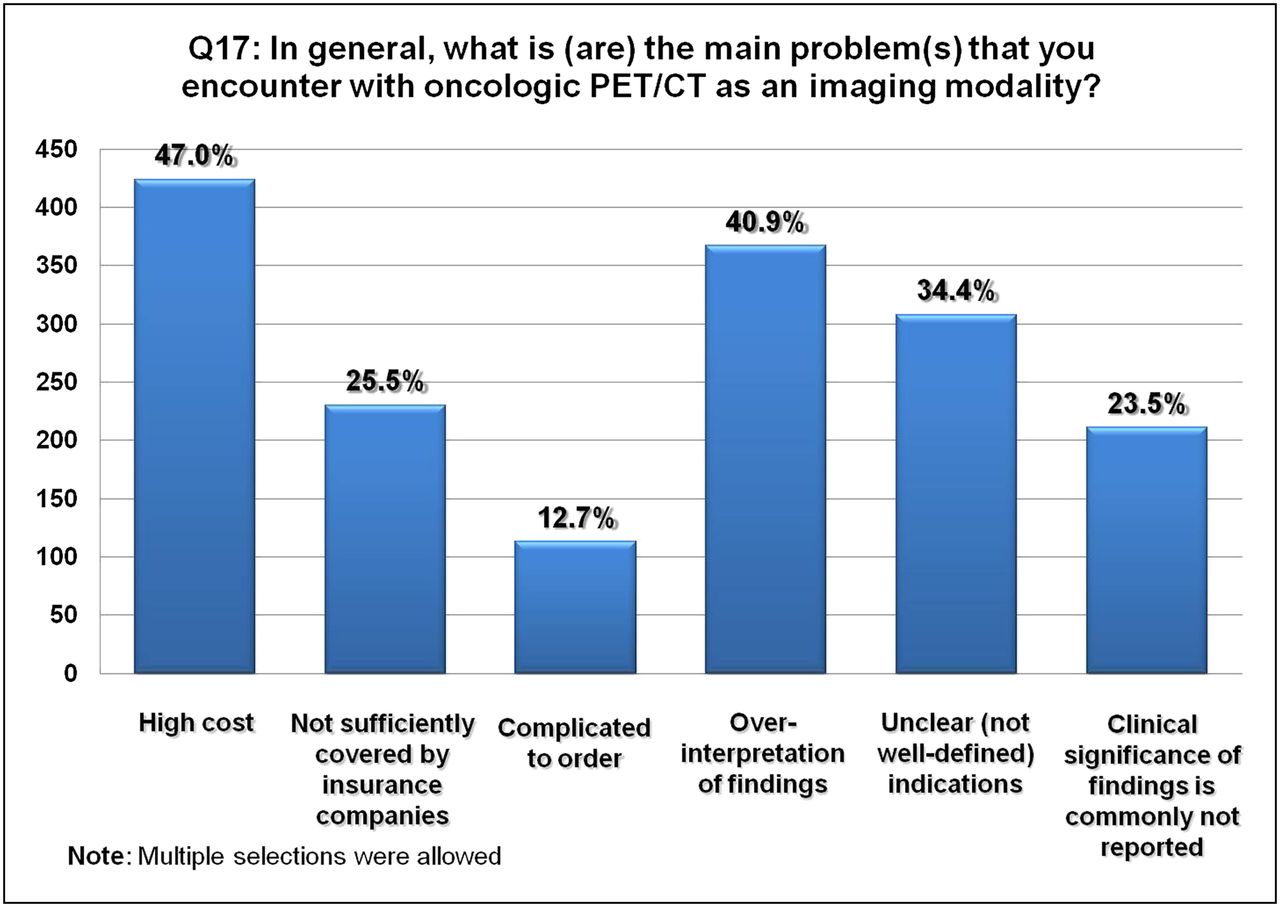
Almost half the participants (47.0%) raised concerns about the high cost of PET/CT (question 17, Fig. 5). Overinterpretation of image findings was another important concern for 40.9% of the participants. This concern was expressed at a similar frequency across all referring specialties with the exception of radiation oncologists, who expressed a somewhat higher degree of concern (48.1%, vs. 40.2% for the other specialties).

Responses to survey question 17.
Unclear indications for PET/CT were perceived to be a problem by 34.4% of respondents, whereas 25.5% considered insufficient insurance coverage as an impediment, and 23.5% indicated concern about the fact that the clinical significance of PET/CT findings was commonly not reported. The most common optional free-text responses had to do with concerns about the limited availability (n = 24) and the ambiguity of the reported results (n = 15).
DISCUSSION
The aim of this survey was to gather information on potential dysfunctions encountered in the clinical use of 18F-FDG PET/CT in oncology. The documentation and communication of the anecdotal experience of the clinicians are of paramount importance for achieving a satisfactory comprehension of the dysfunctions and for addressing practical shortcomings and are a requisite for improving the effectiveness and functional output of this diagnostic tool.
The most significant finding from our results is the prevailing uncertainty of the referring physicians about the appropriate use of PET/CT in oncology. On one hand, most do not consider the indications for oncologic 18F-FDG PET/CT to be well established in medicine (question 1, Fig. 2), and on the other hand, physicians are frequently uncertain about when to order an examination (question 3, Fig. 2). To make this issue even more complicated, almost two thirds of referring physicians report difficulties in accessing updates on indications for oncologic PET/CT (question 2, Fig. 2). This problem is of high significance considering the dynamic evolution and adoption of indications in oncologic PET/CT as a result of the extensive research and large volume of publications in this field. The rapid influx of evidence-based updates on indications should ideally be accompanied by a substantial updating capacity, should somebody wish this influx to result in a proportional clinical impact.
This concern is not new. Manning et al. identified with their study several inconsistencies in the standardized algorithm for the use of PET/CT in different cancer types among 3 primary sources of information: the National Comprehensive Cancer Network guidelines, an extensive review of the pertinent published literature, and the actual clinical practices of referring physicians (11). The authors also indicated that according to their clinical experience many physicians remain somewhat unsure about specifically when to use the test in assessments of patients.
In our study, a potential bias could arise from the fact that participants were selected through their publications in medical journals and that therefore the study population presumably had a more academic orientation than do community clinicians who manage oncologic patients. Because academically oriented physicians generally have better access to scientific publications (including updated guidelines), we suspect that the average referring physician, having even more limited access to literature, would be even less informed about the indications for PET/CT. Acceptance of such a bias amplifies the magnitude of the problem and should alert both scientific communities of clinicians and imaging specialists to the need for increased consensus in the issuance of guidelines for more efficient and educative multidisciplinary interaction.
Another clinically significant finding is the obvious concern of referring physicians about overinterpretation in oncologic PET/CT as expressed by the responses to question 17 (Fig. 5). This concern can presumably be explained by the known variations in increased 18F-FDG uptake by many benign, physiologic processes and conditions (4,12–14). This observation is also significant because it expresses the concerns of the referring physicians for frequent up-staging of oncologic patients with 18F-FDG PET/CT, with the consequent changes in patient management. Also, this finding is in accordance with the importance that referring physicians ascribed to the experience and skill level of the interpreting physician (question 8, Fig. 3).
This point requires the attention of the interpreting physicians in order to improve their specificity while keeping the impact on sensitivity minimal. At the same time, the referring physician should exert every possible effort to help eliminate this problem by providing the appropriate feedback to interpreting physicians whenever such cases of overinterpretation come to their attention. Interestingly, the concern about overinterpretation was expressed similarly by all specialties, with an apparent predominance from radiation oncologists (48.1%, vs. 40.2% in other specialties). This difference is likely due to the nature of their practice (targeted therapy).
The degree of satisfaction with the PET/CT reports (question 12) was quite high; 66.2% declared most frequently satisfied. Nevertheless, this percentage might be an overestimation because the diagnostic centers that support the average community referring physician are expected to be less up to date in equipment, protocols, and staff training than are the academic centers from which many of our respondents presumably originate. This speculation is amplified by the findings of Coleman et al. (15), who found—on the basis of analysis of National Oncologic PET Registry data—that more than 40% of the PET reports did not include critical elements.
Several other interesting points arise from the results of the questionnaire, knowledge of which might be useful to both referring and interpreting physicians. One such point is the apparent need to provide a differential diagnosis for the reported PET/CT abnormalities, as 86% of the referring physicians considered it at least very useful to have a differential diagnosis (question 6, Fig. 3). It seems that the extent of the provided differential needs to be tailored to the specific preference of the referring physician, as two thirds of the referring physicians appeared to prefer a clinically meaningful differential and the other one third to be in favor of a detailed and complete differential (question 7, Fig. 3). There is, in general, a strong belief that more interaction between referring and interpreting physicians would benefit patients, as was reflected by the 96.3% of the respondents who answered positively to question 16. This message needs to be conveyed in both directions with the hope that a greater multidisciplinary exchange of knowledge will be pursued.
Web-based questionnaires are potentially limited in their validity as a result of selective nonresponse and the unknown reliability of the respondents (10). However, selective nonresponse bias is of concern mainly in surveys of the general population rather than in surveys of medical practitioners (16). Furthermore, in our study we could not assume any reasonable mechanism that could lead to selective nonresponse.
Our relatively low response rate (5.2%) has 2 simultaneous potential explanations; the first is the low response rate that Web-based surveys generally have (17,18), and the second is that a presumed considerable number of the recipients of our request either had a nonclinical medical specialty or were scientists performing research in the field of oncology and therefore not eligible for participation. The reliability of the data provided by respondents can be assumed to be at least reasonable since all recipients of our invitation have published in peer-reviewed scientific journals and therefore presumptively have already been evaluated by the scientific community as a reliable and trusted source through the peer review process.
The physicians who participated in this study practice in a variety of countries with different health care systems, different reimbursement and insurance coverage policies, and different protocols for oncologic PET/CT. Therefore, our observations should not be generalized or used to describe the situation in any particular country or health care system.
CONCLUSION
There is a remarkable degree of skepticism and confusion among clinicians over the indications for the appropriate use of oncologic PET/CT. The functional use of the emerging scientific evidence for the clinical utility of PET/CT in oncology is limited. Interpretation of oncologic PET/CT by imaging specialists needs to become more conservative, moving toward the direction of clinically appropriate specificity. The perceived high cost of PET/CT continues to be a major limiting factor for the wider use of this imaging technology.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 23, 2012.
- © 2012 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 20, 2011.
- Accepted for publication May 2, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}