


Abstract
Dynamic nuclear polarization (DNP) is an emerging technique for dramatically increasing the sensitivity of magnetic resonance spectroscopy (MRS). This review evaluates the potential strengths and weaknesses of DNP-enhanced 13C magnetic resonance spectroscopic imaging (DNP-MRSI) as a clinical imaging technique in comparison to PET. The major advantage of MRS is chemical shift, which enables the injected molecule to be observed separately from its metabolites, whereas the major advantage of PET is its high sensitivity. Factors such as spatial and temporal resolution and potential risks and costs of the two techniques will be discussed. PET tracers and 13C-labeled molecules that can be used in oncology will be reviewed with reference to the biologic processes they detect. Because DNP-MRSI and PET are, in principle, similar techniques for assessing tumor metabolism, the experiences gained during the development of PET may help to accelerate translation of DNP-MRSI into routine patient imaging.
PET techniques for imaging tumor metabolism have assisted the development of new drugs and been used to stage tumors and assess treatment response. Although used in a similar way, magnetic resonance spectroscopy (MRS) has not been widely adopted in the clinic, partly because of its poor sensitivity and other factors, such as interpretation. Dynamic nuclear polarization, or DNP (1), is a new technique that addresses this problem by significantly increasing the signal-to-noise ratio. Briefly, 13C-labeled molecules, doped with small quantities of a stable radical, are cooled to approximately 1 K in a magnetic field; microwave irradiation transfers polarization from the fully polarized electron spins on the radical to the 13C nuclei. The sample is then rapidly dissolved using a hot pressurized solution, which can be injected into an animal (or human) in a separate imaging magnet. The increase in signal-to-noise ratio with DNP-MRS is between 104 and 105 (Supplemental Fig. 1; supplemental materials are available online only at http://jnm.snmjournals.org), allowing detection not only of the substrate and products but also of their spatial distribution using spectroscopic imaging (MRSI) (Fig. 1). The technique has been used to image 13C-containing metabolites in tumors, cardiac tissue, and brain (2).
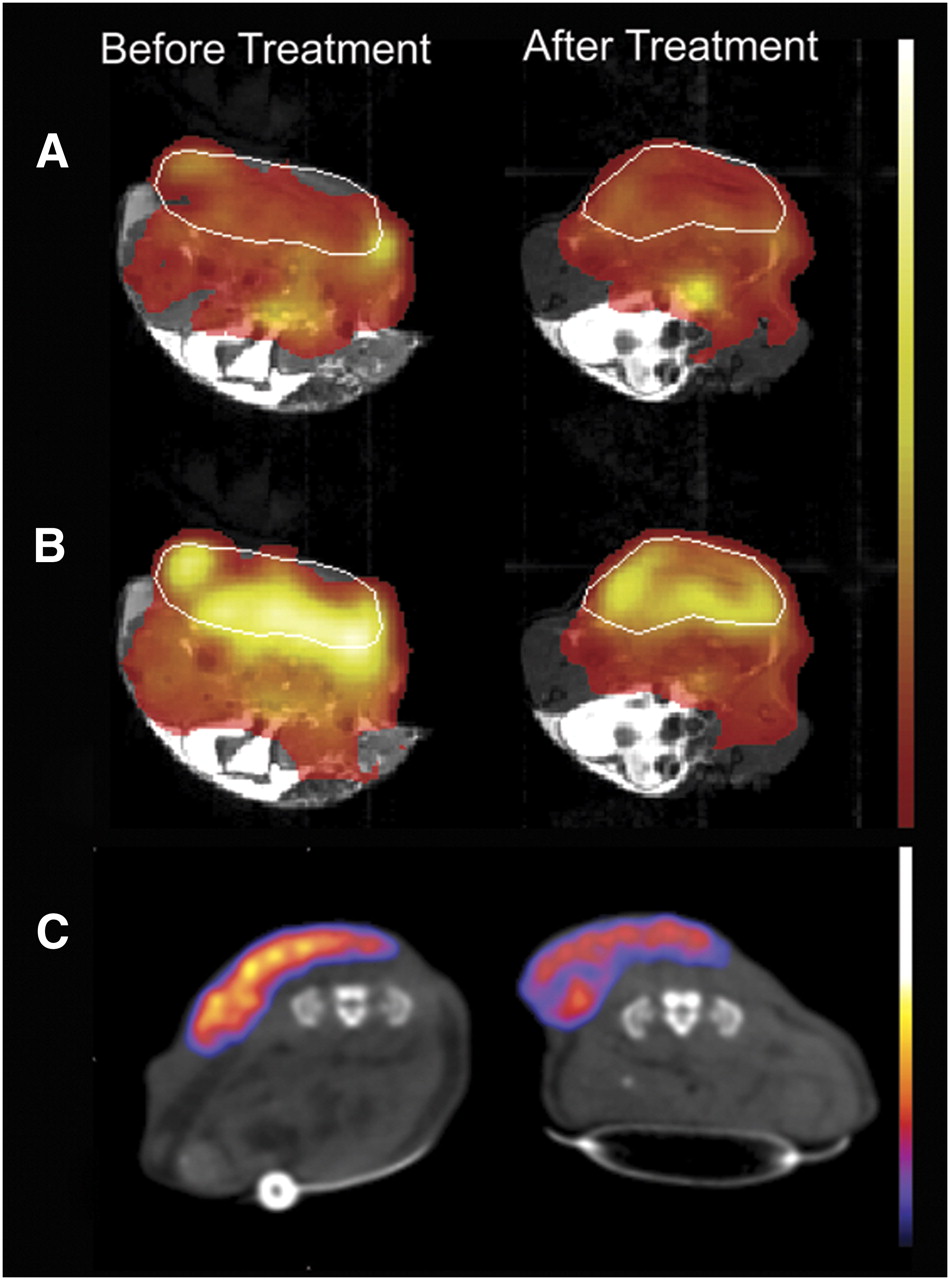
Comparison of [1-13C]pyruvate DNP-MRS and 18FDG PET in a murine lymphoma model. (A) Spatial distribution of injected hyperpolarized [1-13C]pyruvate before and 24 h after treatment of tumor-bearing animal with etoposide. Images were acquired from the same animal. Color maps of hyperpolarized [1-13C]pyruvate distribution are superimposed on gray-scale 1H-MR images and have been normalized to mean pyruvate signal in tumor. Tumor margins are highlighted with a white line. (B) Spatial distribution of hyperpolarized [1-13C]lactate produced from injected hyperpolarized [1-13C]pyruvate. Images are displayed using same scale as for pyruvate. (Reprinted with permission from (6).) (C) PET images acquired between 80 and 90 min after injection of 7 MBq of 18F-FDG. Images were acquired before and after treatment, and color maps have been superimposed over gray-scale CT images. PET and DNP images were acquired from different animals.
The first clinical trial of DNP-MRS is ongoing and is exploring the metabolism of hyperpolarized pyruvate in human prostate cancer. Consequently, it is important to consider what role it might play in the diagnosis and management of cancer patients, and its advantages compared with PET (Supplemental Fig. 1C shows a schematic of a clinical device (3)). The physical principles of the technique and its biomedical applications have been reviewed recently (2,4). Here, we compare the strengths and weaknesses of PET, DNP-MRS, and DNP-MRSI (Table 1).
PET Tracers and DNP-Polarized Molecules with Clinical Imaging Potential in Oncology
SENSITIVITY
Sensitivity depends on many factors, including specific activity of the PET probe and concentration of the hyperpolarized substrate. However, despite the large increase in sensitivity afforded by DNP-MRS, PET is still much more sensitive; PET tracers can be detected in the nano- to picomolar range (5), whereas DNP-MRS sensitivity is still in the millimolar range. Therefore, hyperpolarized molecules are injected at concentrations that greatly exceed physiologic levels (e.g., 15–28 μmoles of pyruvate in mouse models (6,7)), whereas PET-labeled molecules can be administered at concentrations unlikely to perturb normal metabolism. An exception is hyperpolarized bicarbonate, which is already present at high concentrations in vivo (8); the ratio of hyperpolarized bicarbonate to carbon dioxide can be used to determine tissue extracellular pH.
MULTIPARAMETRIC DETECTION
The key advantage of DNP-MRS is that both the injected substrate and its metabolic products can be detected, allowing real-time observation of multiple metabolites. In addition, multiple hyperpolarized molecules can be detected simultaneously, allowing several metabolic pathways to be probed in conjunction with a marker of blood flow (9,10). In contrast, PET measures perfusion and accumulation of a tracer and does not differentiate between metabolites containing the radiolabel.
RANGE OF TRACERS AND TIMING OF ACQUISITION
For DNP-MRS, several requirements must be fulfilled for detection of metabolism in vivo (2); the 13C-labeled molecule must be very soluble and there should be minimal spin–spin coupling to maximize polarization lifetime. Typically, this means the 13C label must be in a carbonyl or carboxyl group. Nevertheless, polarization half-lives are typically only 10–30 s, and consequently, substrate injection and subsequent imaging must be accomplished within a few minutes. This requirement limits usable substrates to those that show relatively rapid metabolism, with hyperpolarized [1-13C]pyruvate being the lead clinical candidate (4). Despite the restrictions for successful DNP-MRS, there are several promising 13C-labeled molecules (Table 1). In contrast, there is a wide range of PET tracers, extending from labeled metabolites, such as 18F-FDG, to labeled drugs (which are not in routine clinical use). Furthermore, although positron-emitting isotopes have relatively short half-lives, which limit human applications (18F = 109.7 min; 11C = 20.4 min; 15O = 2.04 min, 13N = 9.97 min), these half-lives are much longer than those for hyperpolarization and therefore can be used to probe slower metabolism.
IMAGE ANALYSIS
Quantitative analysis of both PET and DNP-MRS generally requires pharmacokinetic modeling (6,11,12). A key difference with DNP-MRS is that the lifetime of the label depends on various factors, such as the presence of paramagnetic centers. Consequently, it is difficult to derive absolute concentrations of the labeled molecules and thus to measure real fluxes (in mM/s); in most cases only rate constants for label flux are reported. Quantitative PET kinetic modeling can be simplified by correcting tracer concentration for injected dose and patient weight to produce a semiquantitative standardized uptake value. Similar approaches may be needed for clinical analysis of hyperpolarized substrate kinetics.
TEMPORAL AND SPATIAL RESOLUTION
Preclinically, the in-plane resolution of both techniques is comparable (~1 mm), but PET can achieve an isotropic image resolution of about 1 mm, whereas DNP-MRSI often uses a thicker slice to improve signal-to-noise ratio (e.g., ∼5 mm). However, DNP-MRSI can be acquired much more rapidly (<1 s) (4) and thus could be acquired within a single breath-hold, reducing motion artifacts. Clinically, the spatial resolution of PET is about 5 mm, and although the resolution of clinical DNP-MRSI is not yet known, with dedicated coils and pulse sequences, similar or better resolution should be achievable. PET can provide whole-body coverage, whereas DNP-MRSI is currently acquired over a limited field of view.
IMAGE COREGISTRATION
PET usually uses CT for anatomic coregistration. Although CT acquisition is rapid and relatively inexpensive, it results in additional radiation exposure and has reduced soft-tissue contrast when compared with 1H-MRI. Administration of contrast medium greatly improves anatomic resolution but can complicate attenuation correction, although this effect is small. The recent introduction of combined PET/MRI will improve anatomic image contrast while providing further complementary information on tissue biology. For example, diffusion-weighted imaging may indicate whether reduced 18F-FDG uptake was due to changed metabolism or a reduction in tumor cellularity. Hyperpolarized 13C-MRSI will be performed in conjunction with 1H-MRI, allowing diffusion-weighted imaging and other MR methods to be combined in the same patient examination.
RISKS
Current evidence suggests that the combined detriment from exposure to PET/CT radiation, due to excess cancer and heritable effects, is about 5% per sievert (13). Although these risks are small, they become important when multiple investigations are undertaken (e.g., to determine therapy response) and when children and women of reproductive age are imaged. The risks from MRI are largely secondary to the presence of ferromagnetic material inside or outside the patient. Magnetic fields per se, 13C-enrichment, and hyperpolarization have no known biologic risks. However, although most hyperpolarized molecules are endogenous, they are injected at a high concentration and possible effects will need to be evaluated in dose-limiting toxicity studies.
COST AND AVAILABILITY
PET with 18F-labeled molecules is widely available, and even many smaller hospitals have access to mobile PET scanners. Local 68Ga generation may become available over the next few years. Few hospitals have an on-site cyclotron to enable the use of 11C- and 15O-labeled probes. Currently, clinical DNP-MRS is a research tool at a single site; however, since most hospitals in developed countries have access to MRI, and a sterile-use hyperpolarizer for potential clinical use has been described recently, the technique could become more widely applied (3) (Supplemental Fig. 1C). Although the running costs for DNP-MRS are currently unknown, it seems likely that they will be no more than for PET and could become cheaper as DNP-MRS becomes more widely available and the manufacturing of 13C-labeled molecules increases.
CONCLUSION
There are a range of labeled molecules for probing tumor biology with PET and DNP-MRS (Table 1). However, PET is already established as a clinical tool and if DNP-MRS is to be adopted, it must provide complementary and clinically useful information. For example, DNP-MRS may provide additional patient information that could be used in conjunction with other imaging tests to assist in diagnosis and patient management. Furthermore, the quantitative information that DNP-MRS provides is of direct biologic relevance and could help further our understanding of tumor biology and accelerate new drug development.
Given the stringent requirements for a hyperpolarized molecule to be used in vivo, it is likely that only a limited number will be available for use in patients. Similarly, although there is a large number of PET probes, many centers use only one routinely: 18F-FDG. Thus, the number of available tracers is not critical to success but rather the efficacy and biologic relevance of those that are available. The current leading DNP molecule is [1-13C]pyruvate, and future research will determine whether it becomes the 18F-FDG equivalent for DNP-MRS. It is likely to be used initially as an early treatment response marker and will have to demonstrate additional efficacy compared with that provided by 18F-FDG. A second candidate molecule for clinical use is [1,4-13C2]fumarate, which has shown promise for detecting cell death.
The DNP-MRS community can learn from previous work undertaken in translating PET tracers to the clinic: the production of clinical-grade tracers, data modeling, and biologic validation are just a few examples of where the two techniques overlap. It has taken several decades for PET to gain widespread clinical acceptance, and studying the problems experienced with PET might help accelerate translation of DNP-MRSI into a routine clinical imaging tool.
Acknowledgments
We acknowledge Cancer Research U.K., the Leukemia and Lymphoma Society, the Wellcome Trust, the National Institute for Health Research Cambridge Biomedical Research Centre, and GE Healthcare for support. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 17, 2011.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication June 16, 2011.
- Accepted for publication July 21, 2011.





{kind=link}