


Abstract
Glucagon-like peptide-1 (GLP-1) receptor imaging is superior to somatostatin receptor subtype 2 (sst2) imaging in localizing benign insulinomas. Here, the role of GLP-1 and sst2 receptor imaging in the management of malignant insulinoma patients was investigated. Methods: Eleven patients with malignant insulinoma were prospectively included. 111In-[Lys40(Ahx-diethylenetriaminepentaacetic acid [DTPA])NH2]-exendin-4 SPECT/CT, 68Ga- DOTATATE PET/CT, and in vitro receptor autoradiography were performed to assess the receptor status and to evaluate the detection rate. Results: GLP-1 receptor targeting was positive in 4 of 11 patients, and sst2 receptor expression was positive in 8 of 11. In only 1 patient were both receptors expressed. In 1 patient, GLP-1 receptor imaging was the only method that successfully localized the primary tumor in the pancreas. In 3 patients with sst2-expressing tumors, DOTATATE radiotherapy was effectively applied. Conclusion: As opposed to benign insulinomas, malignant insulinomas often lack GLP-1 receptors. Conversely, malignant insulinomas often express sst2, which can be targeted therapeutically.
- insulinoma
- glucagon-like peptide-1 receptor targeting
- somatostatin receptor subtype 2 targeting
- peptide receptor radionuclide therapy
Insulinomas are rare neuroendocrine tumors, with an incidence of 0.4 per 100,000 people per year, arising from β-cells located in the islets of Langerhans (1). Insulinomas are usually benign but can be malignant in about 5%–15% of patients (2,3).
Insulinomas can become life-threatening if they cannot be removed surgically. In cases of malignant insulinoma, complete resection of all tumors is difficult and prognosis remains relatively poor, with a 5-y survival of 55.6% and 10-y survival of 29% (2,4,5). Most of these patients have lymph node or liver metastases, and only rarely is there involvement of other sites such as bone. Accurate assessment of the extent of the disease is important, especially because preoperative localization of all lesions facilitates surgery (6,7).
Recently, in vitro and in vivo studies have shown that glucagon-like peptide-1 (GLP-1) receptors are expressed in high density in almost all benign insulinomas (8). Consequently, GLP-1 receptor–specific radioligands have been developed and evaluated in animal models (9,10) and in humans (11–13). Treatment studies in an animal tumor model using therapeutic doses of radiolabeled GLP-1 receptor agonist have shown the potential of GLP-1 receptor targeting as a therapeutic approach (14). Although therapeutic targeting of somatostatin receptor subtype 2 (sst2) is an established method to treat patients with gastroenteropancreatic neuroendocrine tumors (15), the use of sst2 receptor–targeted radiotherapy has been only anecdotal in malignant insulinomas (15,16).
Thus, establishing the incidence and density of peptide receptor status in vivo in patients with malignant insulinomas should improve the assessment of the extent of disease and allow the formulation of a targeted therapeutic approach. However, neither the incidence nor the density of GLP-1 and sst2 receptors is known in malignant insulinomas.
Therefore, we aimed at prospectively evaluating GLP-1 and sst2 receptor status in vitro or in vivo in 11 patients with clinical and biochemical evidence of endogenous hyperinsulinemic hypoglycemia and radiologic features of malignant insulinoma.
MATERIALS AND METHODS
Patients and Study Design
Patients with biochemical or clinical evidence for endogenous hyperinsulinemic hypoglycemia and CT findings suggestive of malignancy were eligible for this study. The total cohort consisted of 11 patients. Eight consecutive patients (4 women and 4 men) were prospectively recruited at 3 tertiary referral centers (University College Hospital London, University Hospital Basel, and University Hospital Freiburg). All patients underwent GLP-1 receptor imaging; additional sst2 receptor imaging was performed in 6 of these patients. GLP-1 receptor SPECT/CT scans (radiotracer, 111In-labeled [Lys40(Ahx-DTPA)NH2]-exendin-4, where DTPA is diethylenetriaminepentaacetic acid) and sst2 receptor PET/CT scans (radiotracer, 68Ga-DOTATATE) were obtained at the 3 centers using identical labeling and imaging protocols. In 4 patients (patients 1, 2, 5, and 6), fresh-frozen tumor tissue was available for quantitative assessment of GLP-1 and sst2 receptor density by in vitro receptor autoradiography (17,18). In 3 additional patients (patients 8, 9, and 11), the GLP-1 and sst2 receptor status was evaluated by in vitro autoradiography only. The diagnosis was confirmed by histologic assessment of tumor samples in all patients.
The study was approved by the local institutional review board of each participating institution, and written informed consent was obtained in accordance with provisions of the Declaration of Helsinki.
Synthesis and Radiolabeling of DTPA-Exendin-4 and DOTATATE
DTPA-exendin-4 (10) and DOTATATE were custom-synthesized by Peptide Specialty Laboratories and Bachem, respectively.
For radiolabeling of DTPA-exendin-4 with 111InCl3, an aliquot of approximately 50 μL (20 μg) of DTPA-exendin-4 was dissolved in 400 μL of ammonium acetate buffer (0.2 M, pH 5.0), incubated with approximately 190 MBq of 111InCl3 (Mallinckrodt) at 90°C for 10 min, and then subjected to quality control by analytic high-performance liquid chromatography (10). The labeling yield of 111In-DTPA-exendin-4 was greater than 98% at a specific activity of 90 GBq/μmol and a radiochemical purity of about 92%.
Approximately 50 μg of DOTATATE was radiolabeled with 600–1,200 MBq of 68Ga with fully automated equipment from Eckert & Ziegler as described before (19). The labeling yield and radiochemical purity of 68Ga-DOTATATE was greater than 97% at a specific activity of 17–34 GBq/μmol.
Imaging and Analysis of Tumor Samples
In all patients, high-speed helical CT scans of the abdomen were obtained less than 6 wk before receptor imaging using a dual-phase, thin-section (0.5-mm collimation) imaging protocol. Usually, 150 mL of nonionic contrast medium were administrated at 4 mL/s, with scan delays of approximately 30 s for the arterial phase and 70 s for the portal phase. Scanning was performed at 120 kV and 100–300 mA.
GLP-1 receptor total-body and SPECT/CT scans were acquired at 4 h and between 2 and 4 d after intravenous injection of 10 ± 2 μg (108–136 MBq) of 111In-DTPA-exendin-4. Imaging was performed with a combined SPECT/CT unit (Symbia T2 [Siemens], Infinia Hawkeye [GE Healthcare], or Bright View XCT [Philips]) equipped with a medium-energy, parallel-hole collimator (12). Blood samples were taken to measure blood glucose levels just before and at 15, 40, 60, 120, 180, and 240 min after injection of 111In-DTPA-exendin-4.
sst2 receptor scans were obtained at 1 h after intravenous injection of 28 ± 8 μg (149–172 MBq) of 68Ga-DOTATATE. Imaging was performed with a combined PET/CT unit (Discovery ST16 [GE Healthcare] Gemini TF64 [Philips]) using a standard protocol (19). Before imaging, patients were asked to stop treatment with long- and short-acting somatostatin analogs.
CT scans were evaluated by experienced radiologists. Two nuclear medicine physicians independently assessed GLP-1 and sst2 receptor scans. The physicians were unaware of patients’ identities, type of scan, or results of other imaging modalities. Afterward, lesion-by-lesion analysis was performed for all tumor foci. Concordant findings on receptor imaging and CT were interpreted as a tumor lesion. In the case of discrepancies between receptor imaging and CT, further evaluation was performed either by histologic assessment or follow-up imaging studies.
RESULTS
GLP-1 and sst Receptor Status in Patients with Malignant Insulinoma
Table 1 summarizes patient characteristics and biochemical evaluation at recruitment.
Clinical Characteristics and Biochemical Evaluation of 11 Patients with Hypoglycemic Episodes and CT Findings Suggesting Malignant Insulinoma
GLP-1 and sst2 receptor imaging or in vitro receptor autoradiography of resected tumor samples was performed to test the GLP-1 and sst receptor status in malignant insulinoma (Table 2). GLP-1 receptors were expressed in the tumors of 4 patients (36%), whereas sst2 receptors were found in the tumors of 8 patients (73%). Importantly, only patient 1 expressed both receptors in the primary tumor and 1 locoregional lymph node metastasis, indicating similar receptor biology in the primary tumor and the single metastasis. All other patients showed overexpression of only 1 type of receptor (Table 2; Figs. 1 and 2). Moreover, GLP-1 receptor imaging detected all tumor lesions in GLP-1 receptor–positive tumors (16/16), whereas sst2 receptor imaging picked up all tumor lesions in sst2 receptor–positive tumors (35/35), resulting in a sensitivity of 100% when the 2 imaging methods were combined (Supplemental Table 1; supplemental materials are available online only at http://jnm.snmjournals.org). CT, by contrast, identified 42 of 51 tumor lesions (82%). In patients for whom both in vitro autoradiography and imaging studies were performed, an excellent correlation was found between in vitro and in vivo studies (Table 2; Figs. 1 and 2).
Comparison of Imaging Results, Receptor Autoradiography Results, and Immunohistochemical Results
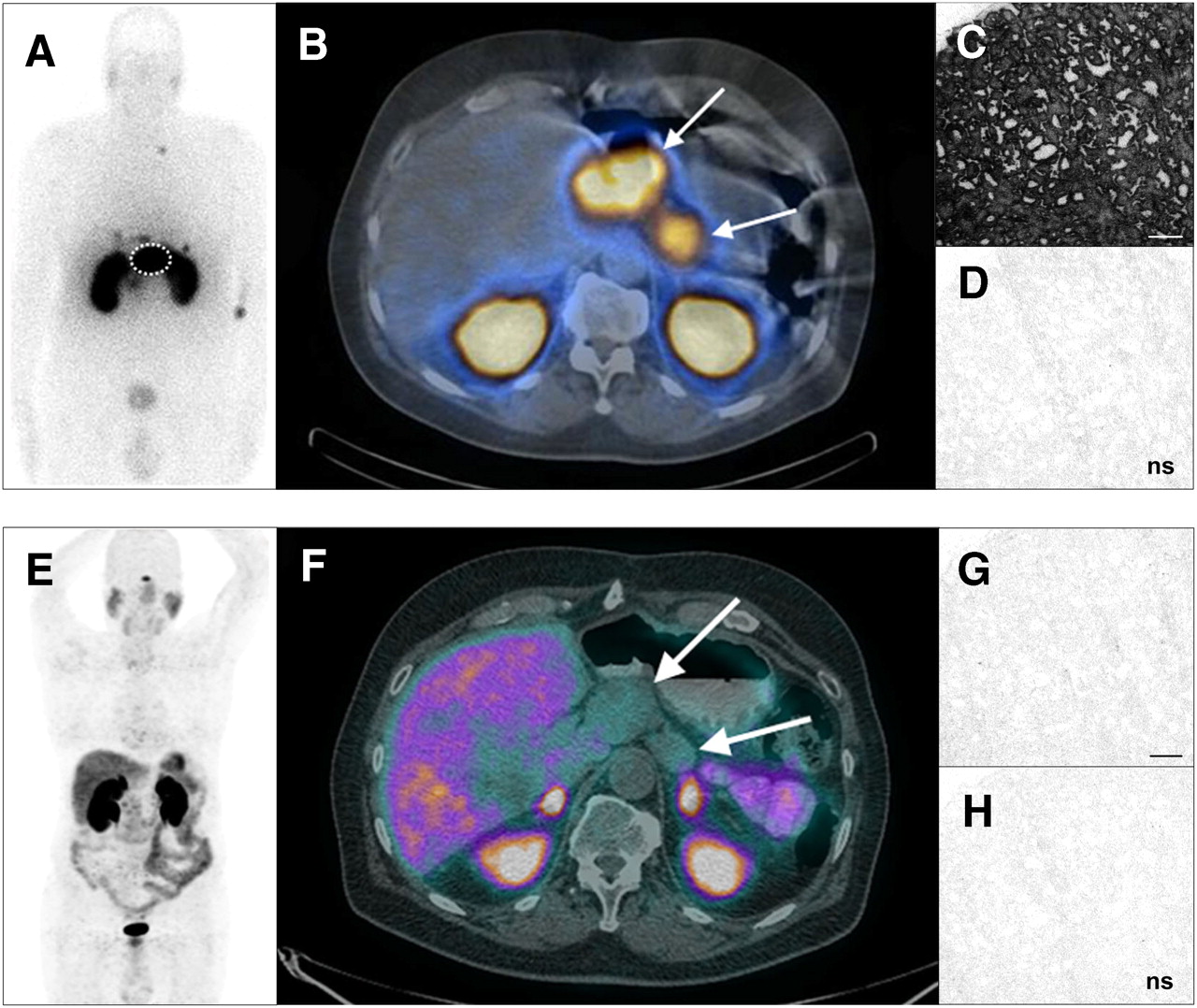
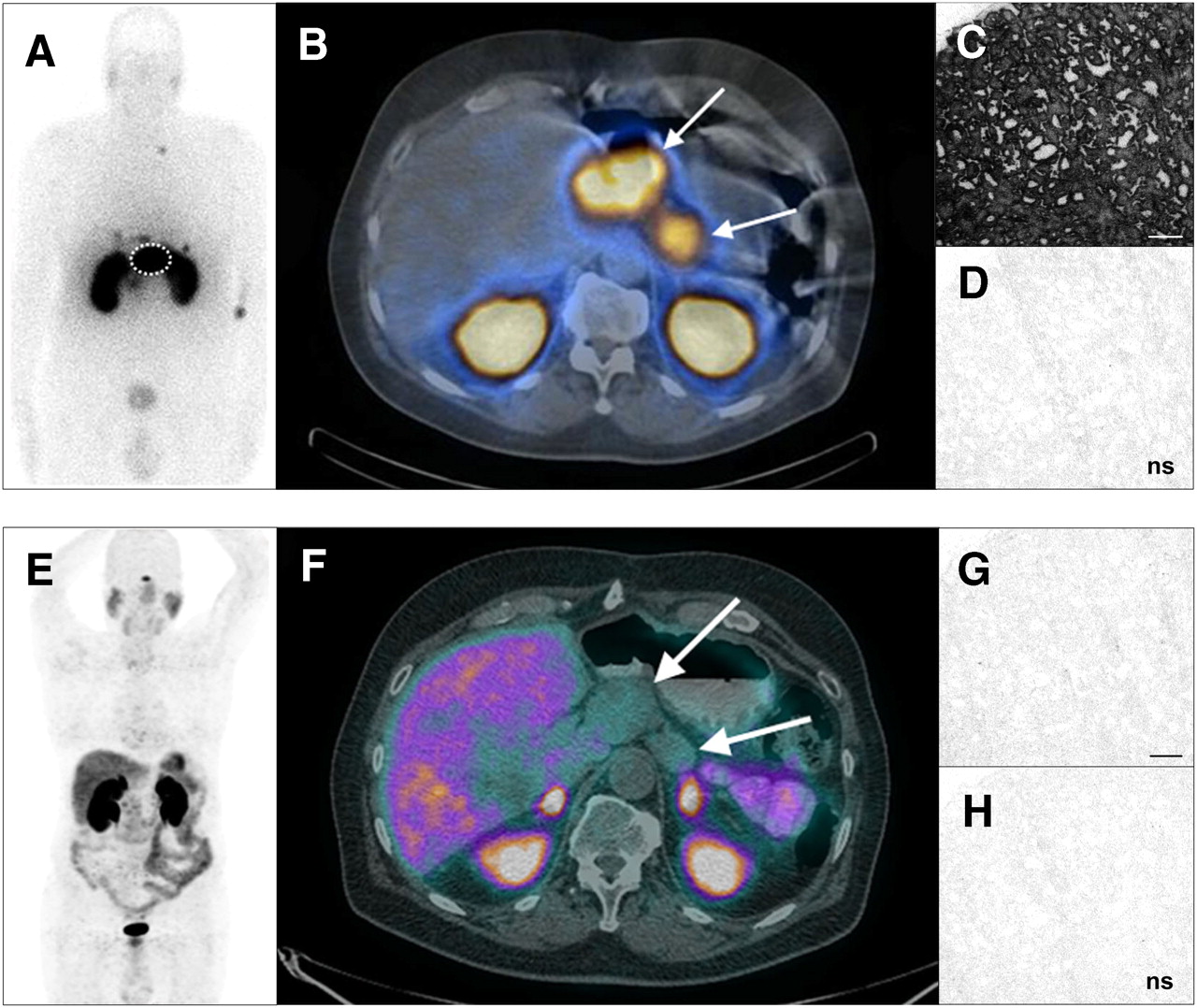
Example of GLP-1 receptor–positive and sst2 receptor–negative malignant insulinoma (patient 2). GLP-1 receptor scintigraphy (A) and SPECT/CT (B) were performed 4 h after injection of 111In-DTPA-exendin-4 (109 MBq), and sst2 receptor PET/CT (E and F) was performed 1 h after injection of 68Ga-DOTATATE (149 MBq). Tumor tissue samples from same patient were used for in vitro GLP-1 (C and D) and sst2 receptor (G and H) quantification. There is focal 111In-DTPA-exendin-4 uptake in 2 liver lesions, 1 cardiophrenic lesion, 1 left retroclavicular lymph node, and 1 retrosternal lymph node (A). Moreover, dotted circle in A and arrows in B show 2 large 111In-DTPA-exendin-4–avid lymph nodes adjacent to stomach. sst2 receptor whole-body PET (E) shows normal 68Ga-DOTATATE distribution even in large lymph nodes adjacent to stomach (arrows, F). There is excellent correlation between peptide receptor imaging and in vitro receptor quantification: autoradiograms show strongly positive specific binding of 125I-GLP-1 (7-36) amide in whole tumor (C), whereas 125I-[Tyr3]-octreotide shows only nonspecific binding (G). Autoradiograms show nonspecific binding of 125I-GLP-1 (7-36) amide (D) and 125I-[Tyr3]-octreotide (H) in presence of 100 nM GLP-1 (7-36) amide and 100 nM octreotide, respectively. Bar = 1 mm.
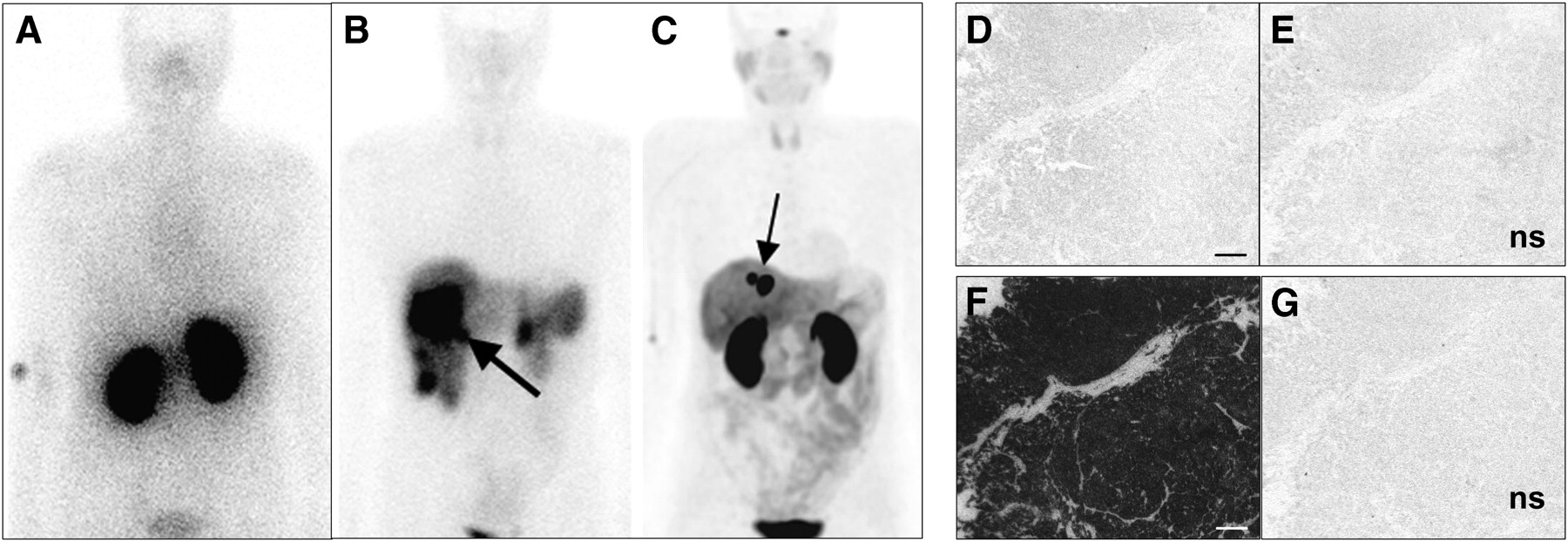
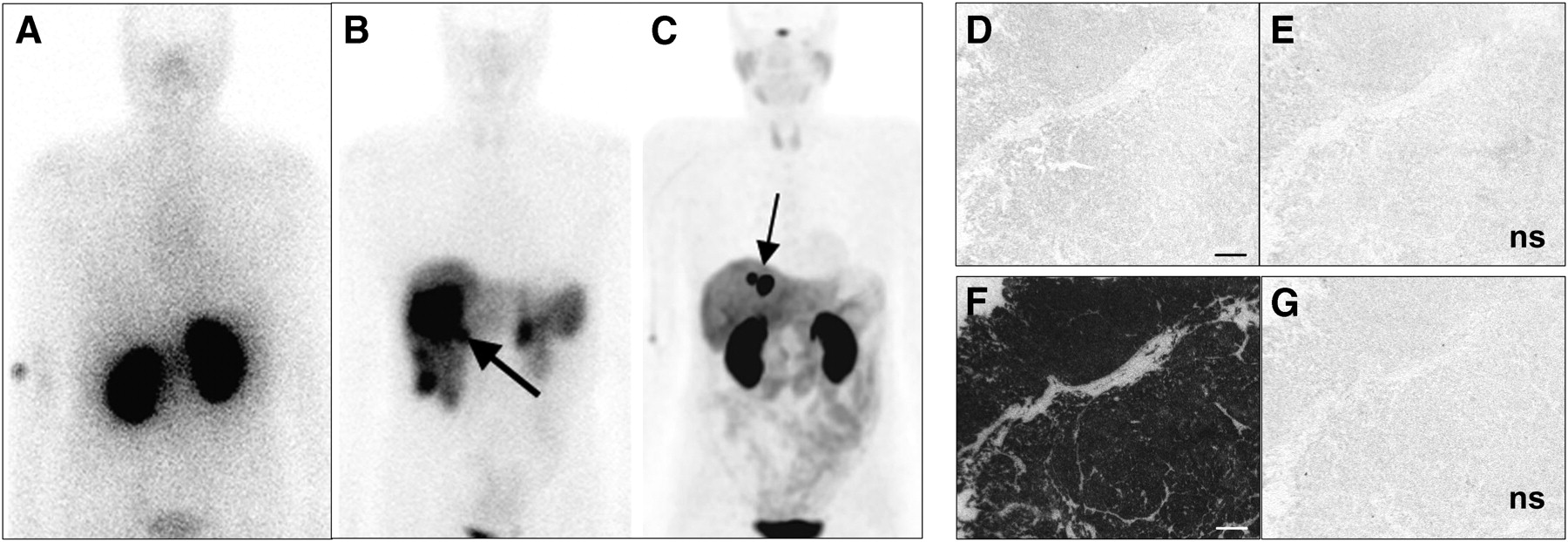
Example of GLP-1 receptor–negative and sst2 receptor–positive malignant insulinoma (patient 6). Baseline GLP-1 receptor (A) and sst2 receptor scintigraphy (B) were performed 4 h after injection of 111In-DTPA-exendin-4 (124 MBq) and 99mTc-tektrotyd (669 MBq), and posttreatment sst2 receptor PET (C) was performed 1 h after injection of 68Ga-DOTATATE (165 MBq). Tumor tissue samples from same patient were used for in vitro GLP-1 (D and E) and sst2 receptor (F and G) quantification. sst2 receptor scintigraphy shows intense 99mTc-tektrotyd uptake in tail of pancreas and in multiple liver lesions (B). Arrow shows large 99mTc-tektrotyd–avid lesion in right liver lobe (B). GLP-1 receptor whole-body scan shows normal 111In-DTPA-exendin-4 distribution, even in large liver lesion (A). After distal pancreatectomy, right hemihepatectomy, and PRRT good partial remission was achieved, with residual disease in only 2 liver lesions, with maximal diameter of 1.3 cm (arrow, C). Correlation is excellent between peptide receptor imaging and in vitro receptor quantification: autoradiograms show strongly positive specific binding of 125I-[Tyr3]-octreotide in whole tumor (F), whereas 125I-GLP-1 (7–36) amide shows only nonspecific binding (D). Autoradiograms show nonspecific binding of 125I-GLP-1 (7-36) amide (E) and 125I-[Tyr3]-octreotide (G) in presence of 100 nM GLP-1 (7-36) amide and 100 nM octreotide, respectively. Bar = 1 mm.
Comparison of Biochemical Results and Peptide Receptor Expression
About 40 min after the injection of 111In-DTPA-exendin-4 (10 ± 2 μg), blood sugar dropped by 1.1–3.3 mmol/L in patients with GLP-1 receptor–positive malignant insulinoma and by 0.5–0.6 mmol/L in patients with GLP-1 receptor–negative malignant insulinoma (Table 2). No further side effects were observed.
Biochemical results at the end of the fasting test showed a tendency for lower insulin concentrations in patients with GLP-1 receptor–positive and sst2 receptor–negative tumors (3.0–80 mU/L) than in those with sst2 receptor–positive and GLP-1 receptor–negative tumors (20–143 mU/L) (Table 1).
Clinical Course After Imaging
Treatments and clinical course after imaging are summarized in Table 1. Four patients (patients 1, 5, 10, and 11) with limited disease (locoregional lymph node metastases or single liver lesion) were treated with curative-intent surgery. Three of these patients were tumor free at the end of the study. In patient 1, GLP-1 receptor imaging was the only diagnostic method that could successfully localize the insulinoma in the pancreas and was therefore a decisive factor for patient management. Two patients with extensive disease (patients 2 and 6) received aggressive debulking surgery, and 3 patients (patients 3, 4, and 6) with positive 68Ga-DOTATATE PET findings were treated with 1–3 cycles of peptide receptor radionuclide therapy (PRRT) using 90Y-DOTATATE or 177Lu-DOTATATE to control hypoglycemia and tumor growth. In patients 3 and 6, a partial response and normalization of blood glucose were achieved after treatment with 90Y-DOTATATE and 177Lu-DOTATATE, and patient 4 showed stable disease until termination of the study.
DISCUSSION
This is the first report, to our knowledge, that evaluates GLP-1 and sst2 receptor targeting and status in vitro or in vivo in patients with malignant insulinoma. The main findings of this study are that malignant insulinomas do not always express GLP-1 receptor, express sst2 receptors more often than GLP-1 receptor, and always express 1 of the 2 receptors.
The present study shows that, in contrast to benign insulinomas (8,12), only a low percentage of the malignant insulinomas (36%) expressed GLP-1 receptors. However, somatostatin receptor scintigraphy, reported previously to have a low detection rate of less than 20% in benign insulinomas (20), was positive in 73% of malignant insulinomas in the present study. Concomitant GLP-1 and sst2 receptor expression was discovered in only 1 patient. Importantly, all tumors in all patients could be localized with the combination of the 2 peptide receptor imaging methods.
The results obtained with GLP-1 and sst2 receptor targeting significantly affected clinical management and outcome in 4 of the recruited patients. Indeed, knowing that a given tumor expresses sst2 receptor makes it a potential candidate for targeted radiotherapy with somatostatin analogs. The 3 patients with positive sst2 receptor scan findings and progressive disease were treated with 177Lu-DOTATATE or 90Y-DOTATATE (PRRT). In 2 of these patients (patients 3 and 6), a partial response and normalization of blood glucose were achieved shortly after treatment. The third patient (patient 4) showed no further progression until the end of the study. In 1 patient, GLP-1 receptor scans correctly localized the insulinoma in the pancreas, whereas CT and MRI scans showed evidence for liver and lymph node metastases but were unable to localize the primary tumor. The patient was referred for surgery on the basis of the GLP-1 receptor scan findings and remained tumor-free until the end of the study.
Although it was not possible, for logistic reasons, to perform in vitro and in vivo assessment of GLP-1 and sst2 receptor status in all patients, our data indicate an excellent correlation between in vivo and in vitro receptor data. The in vitro data indicate that there is an absence of the gray zone of mild to moderate receptor expression that could make in vivo assessment of receptor expression by PET and SPECT challenging. All tumors studied by autoradiography either demonstrated high density receptor expression or were completely negative. Therefore, the in vitro and in vivo data can be used interchangeably.
CONCLUSION
Our data indicate that, in contrast to benign insulinomas, malignant insulinomas often lack GLP-1 receptors but express sst2 receptors more often. This observation is clinically relevant for 2 reasons. First, if a malignant insulinoma is suspected using biochemical investigations and conventional imaging, sst2 receptor imaging can be recommended for presurgical staging and potentially PRRT. Second, a scan negative for GLP-1 receptors may potentially indicate malignant insulinoma.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
This work was supported in part by the Novartis Foundation, the Swiss National Science Foundation (PASMP3-123269), an Oncosuisse grant (no. OCS-02259-08), a proportion of funding from the Department of Health's NIHR Biomedical Research Centre's funding scheme, and from the King's College London and UCL Comprehensive Cancer Imaging Centre CR-U.K. and EPSRC, in association with the MRC and DoH (England). No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication November 8, 2010.
- Accepted for publication March 16, 2011.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Peptide Receptor Radionuclide Therapy Is Effective for Clinical Control of Symptomatic Metastatic Insulinoma: A Long-Term Retrospective Analysis
- Glucagon-like Peptide-1 Receptor as Emerging Target: Will It Make It to the Clinic?
- Succinylated Gelatin Improves the Theranostic Potential of Radiolabeled Exendin-4 in Insulinoma Patients
- Molecular imaging in the investigation of hypoglycaemic syndromes and their management
- A New Theranostic Paradigm for Advanced Thyroid Cancer
- Medical management of secretory syndromes related to gastroenteropancreatic neuroendocrine tumours
- Glucagon-Like Peptide-1 Receptor PET/CT with 68Ga-NOTA-Exendin-4 for Detecting Localized Insulinoma: A Prospective Cohort Study
- Triple-Peptide Receptor Targeting In Vitro Allows Detection of All Tested Gut and Bronchial NETs
- Hallmarks of gastrointestinal neuroendocrine tumours: implications for treatment
- GLP-1 Provoked Severe Hypoglycemia in an Individual With Type 2 Diabetes and a Benign Insulinoma
- The Human GLP-1 Analogs Liraglutide and Semaglutide: Absence of Histopathological Effects on the Pancreas in Nonhuman Primates
- GEP-NETS update: Functional localisation and scintigraphy in neuroendocrine tumours of the gastrointestinal tract and pancreas (GEP-NETs)
- MANAGEMENT OF ENDOCRINE DISEASE: A clinical update on tumor-induced hypoglycemia
- Radiopeptide Imaging and Therapy in Europe