


See page 1923
The use of nuclear medicine imaging and CT has grown dramatically over the last several decades. In the Unites States, the annual number of nuclear medicine procedures increased 3-fold (from 7 to 20 million) and the annual number of CT procedures 20-fold (from 3 to 60 million) between 1985 and 2005 (1). As a result of this increased medical exposure of the population, the average (i.e., per-capita) annual background dose in the Unites States has nearly doubled, from 3.0 to 5.6 mSv (2). There has been increasing societal concern over the potential public health impact—namely, an increased risk of cancer—associated with this dramatic increase in exposure from diagnostic imaging.
Brenner and Hall, for example, have estimated that as much as 2% of all cancers in the United States may be attributable to CT irradiation (3). Although nuclear medicine diagnostic procedures are not performed as frequently as CT scans and the organ absorbed doses are generally not as high, the effective dose, and therefore the overall radiogenic cancer risk per procedure, are comparable (4). Radiogenic cancer risks vary with sex and, in particular, age at exposure, with children at markedly greater risk than adults. For example, the lifetime attributable risk (LAR) of a radiation-induced cancer is approximately 20%/Sv at 10 y of age but only about 7%/Sv at 40 y of age (5). Therefore, the management of radiation doses associated with diagnostic imaging in pediatric patients is a particular and persisting concern.
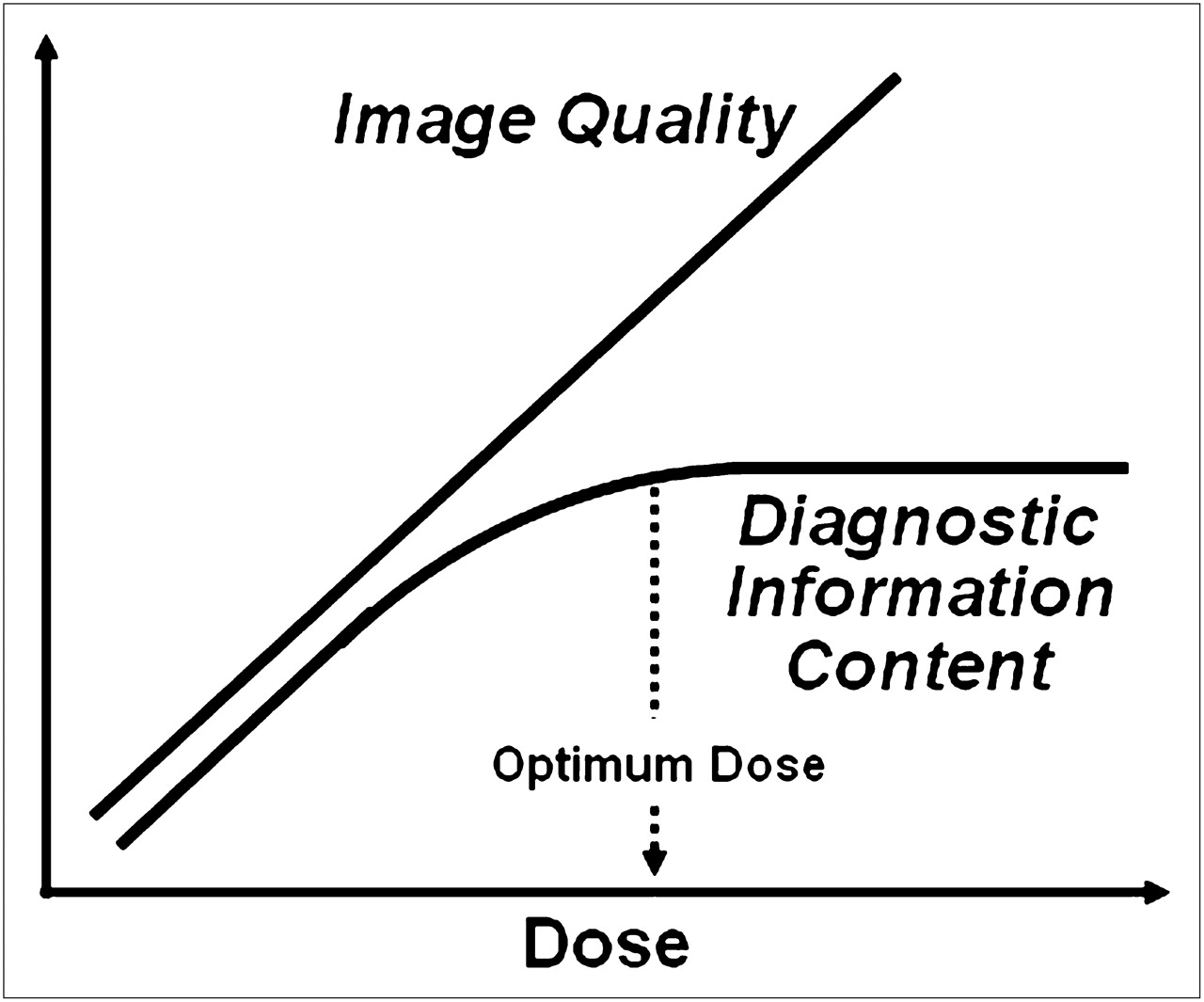
As illustrated in Figure 1, for any radiologic procedure, the image quality—the aesthetics of the study, if you will—improves progressively with patient dose (6). In the case of nuclear medicine, for example, as the administered activity is increased and more photons emanate from the patient and strike the imaging detector, the quantum mottle in the resulting image is reduced, and the image appears smoother and more visually aesthetic. More importantly, diagnostic information content (e.g., lesion detectability) increases as well with increasing dose—but only to a certain point. Although image aesthetics will continue to improve with increasing dose, the optimum patient dose is reached once all of the diagnostic information technically derivable from a particular study has been obtained. Increasing the administered activity and therefore the dose further yields no additional information and thus unnecessarily increases the radiogenic cancer risk to the patient. The optimum-dose concept is the basis of minimizing the risk associated with diagnostic imaging and of the Image Gently campaign currently being promoted by many agencies and professional organizations (7–10). For all diagnostic procedures, the study parameters should be judiciously selected to deliver the minimum radiation dose consistent with yielding the clinical information being sought. The current computer simulation study by Sgouros et al. (11) is a rigorously elegant case study of how this may be accomplished in the context of nuclear medicine.

Optimum-dose concept. Stylized graft illustrating relationship among image quality, diagnostic information content, and patient dose for diagnostic imaging procedures. (Reprinted with permission of (6).)
In this study, pharmacokinetic modeling and state-of-the-art pediatric nonuniform rational B-spline (NURBS)–based anatomic phantoms of 10-y-old girls were used to simulate SPECT images of the renal agent 99mTc-dimercaptosuccinic acid (DMSA). Importantly, 2 different anatomic phantoms of 10-y-old girls were considered; the 2 phantoms had the same body mass (32 kg) but different body morphometry, short and stout (125 cm tall) versus tall and lean (147 cm tall). The fidelity of this analysis to actual clinical imaging is remarkable and distinguishes it from other such analyses. Different administered activities (25%, 50%, 75%, 100%, 125%, and 150% of the standard mass–based administered activity of 1.85 MBq/kg), 2.2-cm lesions with different target-to-background activity concentration ratios and at different intrarenal locations, and 50 random variations of lesion uptake for each location were considered. The simulated projection image data were scaled to yield the counts that would be obtained using a dual-detector γ-camera system with low-energy high-resolution collimation (system sensitivity, 85.6 cps/MBq of 99mTc) and a 30-min acquisition and with incorporation of the effects of scatter, attenuation, and detector response. The NURBS phantoms were also used to calculate 99mTc S factors by separate energy spectrum–weighted Monte Carlo simulations for the particulate and photon radiations. Channelized Hotelling observer methodology was used in a receiver-operating-characteristic analysis of lesion detectabilityin the simulated reconstructed images. The MIRD Committee formalism and the foregoing 99mTc-DMSA pharmacokinetics and 99mTc S factors were used to calculate the mean organ-absorbed doses to the 2 pediatric phantoms. The absorbed doses thus calculated ranged from 3.9 × 10−5 (salivary glands) to 7.4 × 10−2 (liver) mGy/MBq in the short, stout phantom and 1.1 × 10−4 (salivary glands) to 5.4 × 10−2 (liver) mGy/MBq in the tall, lean phantom. Organ-absorbed doses were then converted to LARs of cancer using BEIR VII age- and sex-specific risk factors (5).
Importantly, the same diagnostic performance—in terms of identifying the intrarenal defects—could be achieved in the tall, thin patient with only one-half of the standard mass–based administered activity (MBq/kg) used for the short, stout patient. The difference in diagnostic information content between the 2 image sets was due to a combination of 10% more photons escaping, a 10% smaller average radius of the γ-camera orbit, and a 10% lower scatter-to-primary photon ratio for the tall, lean patient than for the short, stout patient. This combination resulted in slightly lower quantum mottle (noise), sharper spatial resolution, and higher contrast, respectively—and better diagnostic performance per unit administered activity—for the taller patient. For 99mTc-DMSA renal imaging of children, therefore, the optimum administered activity (MBq/kg) and resulting radiation doses (mSv/MBq) are considerably lower for tall, lean patients than for short, stout patients of the same body mass. Specifically, the diagnostic information content of 99mTc-DMSA renal imaging was optimized with an administered activity of 59 MBq in a short, stout 10-y-old girl but with only 30 MBq in a tall, lean 10-y-old girl, resulting in a LAR of cancer of 0.006% for the short, stout patient but only 0.002% for the tall, lean patient. Similar LARs were obtained on the basis of the effective dose and the overall radiation detriment factor in ICRP 103 (12). First-order metrics of body morphometry such as body mass and body surface area are thus inadequate for optimum scaling of administered activities among patients.
The diagnostic information content of a procedure must, of course, not be compromised in a misguided attempt to minimize patient radiation dose. A suboptimal procedure (e.g., with an inadequate administered activity) not only compromises patient management by failing to disclose the information being sought but also may ultimately increase the patient's radiation exposure by requiring a repeated, properly performed study to obtain the needed information. Given the possibility of performing such suboptimal procedures in the interest of dose reduction, rigorous validation of diagnostic protocols designed to reduce patient exposure are therefore required before they are recommended for standard practice. In the current virtual-reality study by Sgouros et al. (11), such validation was accomplished by remarkably realistic computer simulation of SPECT studies over a range of administered activities in combination with comparison of diagnostic information content of the resulting images using receiver operating characteristics. Alternatively, such an analysis could be performed empirically—that is, in the context of a traditional clinical trial in which different patient strata are administered different activities of a radiopharmaceutical and the diagnostic accuracy correlated with the administered activity. In addition to practical limitations such as time and cost, patient-to-patient variations in the location and extent of defects and body morphometry and the absence of an unambiguous reference standard (i.e., ground truth diagnosis) may confound interpretation of the results and thus derivation of an optimum administered activity. Further, ethical considerations, especially in children, may make such a study unacceptable to institutional reviews boards and prospective subjects or their parents.
With persisting concerns regarding radiation risks of diagnostic imaging procedures, the virtual-reality approach of Sgouros et al. (11) can yield computationally validated “isoradiation risk”–administered activity guidelines for pediatric and other patients that account for differences in body morphometry and body mass among patients—all while circumventing the burdens and limitations of traditional clinical trials. With the rigor achieved in the current study, virtual reality is indeed better than the real thing.
Footnotes
Published online Nov. 11, 2011.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication October 24, 2011.
- Accepted for publication October 26, 2011.





{kind=link}