


Abstract
Chronic obstructive pulmonary disease (COPD) patients exhibit increased cardiovascular risk, even after controlling for smoking. Inflammation may underlie this observation. Methods: We measured vascular inflammation in both COPD patients and controls using 18F-FDG PET/CT. Aortic inflammation was expressed as the target-to-background ratio (TBR) of the standardized uptake value in 7 COPD patients, 5 metabolic syndrome patients, and 7 ex-smokers. Results: Abdominal aortic mean TBR (±SD) was greater in COPD patients than in ex-smoker controls (1.60 ± 0.13 vs. 1.34 ± 0.15, P = 0.0001). Aortic arch and abdominal aorta mean TBRs were higher in metabolic syndrome patients than in COPD patients (aortic arch, 1.80 ± 0.18 vs. 1.53 ± 0.18, P = 0.001, and abdominal aorta, 1.71 ± 0.14 vs. 1.60 ± 0.13, P = 0.001). Conclusion: COPD patients exhibited aortic inflammation that fell between the aortic inflammation exhibited by ex-smokers and that by metabolic syndrome patients. This may in part explain the increased risk of cardiovascular disease in COPD patients.
Subjects with chronic obstructive pulmonary disease (COPD) are at increased risk of cardiovascular disease (1). In parallel, in the general population, there is evidence that both the rate of decline of lung function and the other markers of airway obstruction are predictive of cardiovascular risk independent of smoking history (2).
Several cardiovascular risk factors occur in COPD, including systemic inflammation, characterized by increased circulating levels of interleukin-6 and C-reactive protein; insulin resistance; and greater arterial stiffness (3–6). Sabit et al. reported greater arterial stiffness in patients with COPD and described a direct relationship between arterial stiffness and circulating interleukin-6 levels (6).
Given the potential for therapeutic intervention, the role of inflammation in explaining this excessive cardiovascular risk warrants exploration. In this study, we quantified arterial inflammation noninvasively using 18F-FDG PET (7,8). There is evidence that arterial 18F-FDG uptake is due to accumulation by activated endothelial cells and macrophages in the vessel wall (9). 18F-FDG PET can track reductions in arterial inflammation after statin therapy and risk factor reduction (10,11).
We hypothesized that patients with COPD would have more arterial inflammation than controls. To test this hypothesis, we measured arterial inflammation in male ex-smokers with COPD and in male ex-smokers without COPD (negative controls). The metabolic syndrome is associated with excessive cardiovascular risk and is known to cause increased arterial inflammation on 18F-FDG PET (9,12). Therefore, we also enrolled men with the metabolic syndrome to act as positive controls for the study.
MATERIALS AND METHODS
Participants
Seven male ex-smokers with COPD (Global Initiative in Chronic Obstructive Lung Disease [GOLD] criteria), 7 men with 2 or more components of the metabolic syndrome (International Diabetes Federation criteria), and 7 male ex-smokers free from COPD were recruited.
The sample size was limited by the Administration of Radioactive Substances Advisory Committee because of radiation exposure constraints in volunteers. The study was approved by the South East Wales Research Ethics committee. Written informed consent was obtained from all participants.
Exclusion criteria were known cardiovascular disease, diabetes mellitus, malignancy, vasculitis, inflammatory arthritis, and renal impairment or the use of maintenance oral glucocorticoids, statins, or other antiinflammatory therapies. All patients were clinically stable for at least 4 wk before study entry and had received no change in therapy during this period.
18F-FDG PET/CT
Imaging was performed using a PET/CT system (Discovery ST; GE Healthcare), after the patients had fasted for 6 h. All subjects had a fasting glucose level less than 7 mmol/L at the time of imaging. Approximately 270 MBq of 18F-FDG was injected intravenously, and subjects rested in a quiet room for 90 min to allow 18F-FDG uptake. Aortic PET was then performed over 30 min (2-dimensional mode, 3 bed positions of 10 min each, and ordered-subset maximization expectation reconstruction, using CT for localization and attenuation correction of PET data). Carotid imaging was performed at a single bed position, with an emission time of 15 min, in 3-dimensional mode with Fourier rebinning iterative reconstruction, again after a localizing CT scan. No CT contrast was administered.
Vascular PET image analysis was performed on a Xeleris 2.0 workstation (GE Healthcare), using validated, reproducible methods (7). Briefly, the aorta was divided into ascending, arch, descending, and abdominal segments using anatomic landmarks derived from the CT scan. Arterial 18F-FDG uptake was quantified by drawing circular regions of interest around each artery on every slice of the coregistered transaxial PET/CT images. A single reader performed the analysis under the direct supervision of another reader, and reproducibility between the two was high (intraclass correlation coefficient > 0.9).
Mean and maximum body weight–corrected standardized uptake values (SUVs) were calculated from the pixel activity within each region of interest. SUVs were normalized to blood 18F-FDG activity by dividing the average SUV by either the inferior vena cava or the internal jugular vein to produce a blood-corrected artery SUV, known as the arterial target-to-background ratio (TBR) (7).
Physiologic Measurements
Subjects’ height and weight were measured to determine body mass index.
Spirometry (Vitalograph Alpha) was performed to determine forced expiratory volume in the first second, forced vital capacity, and the ratio of forced expiratory volume in the first second to forced vital capacity, according to a standardized protocol.
Hemodynamic Measurements
Supine blood pressure measurements were obtained using a validated oscillometric technique (MX2 Basic; Omron Corp.). Radial artery waveforms were recorded with a high-fidelity micromanometer (Millar Instruments). Pulse-wave analysis (Sphygmocor; AtCor Medical) generated a corresponding central waveform, using a validated transfer function. The augmentation index, a validated marker of pulse-wave reflection that correlates with cardiovascular risk, was calculated as the difference between the second and first systolic peaks as a percentage of pulse pressure, and in all cases, the index was corrected to a heart rate of 75 beats per minute. Aortic pulse-wave velocity (aPWV) was measured with the same device by sequentially recording electrocardiogram-gated carotid and femoral artery waveforms. Wave transit time was calculated by the system software, using the R wave of a simultaneously recorded electrocardiogram as a reference. The aPWV was determined by dividing the distance between the 2 recording sites by the wave transit time·
Laboratory Measurements
Near-patient capillary fasting lipid and glucose was measured (Cholestech LDX system; Cholestech Corp.). Venous blood samples were taken for serum interleukin-6 measurement by enzyme-linked immunosorbent assay (R&D Systems) (3).
Statistical Analysis
Statistical analysis was performed using SPSS (version 15; SPSS Inc.). Data are presented as the arithmetic mean ± SD. Smoking history is expressed in pack-years as the median and range. Log10 transformations were performed on interleukin-6 because of the positively skewed distribution, and the geometric mean is presented. The 1-way ANOVA was used for comparisons among the 3 groups. When a probability value under 0.05 was found for the overall comparison, Tukey posttest analysis was performed between individual groups. Statistical significance was set at the 5% level.
RESULTS
Two metabolic syndrome patients withdrew from the study due to claustrophobia; they were excluded from further analysis. Therefore, data from 7 ex-smokers, 7 COPD patients, and 5 metabolic syndrome patients were included in the final analysis.
The average administered dose of 18F-FDG was 285 MBq. Neither the administered dose nor the 18F-FDG circulation time of 90 min differed among the 3 patient groups. The baseline characteristics of the patients are presented in Table 1.
Baseline Characteristics
COPD severity was assessed using the GOLD criteria. One patient had GOLD II, 5 had GOLD III, and 1 had GOLD IV airway obstruction. None had evidence of cor pulmonale or met the criteria for long-term oxygen therapy. Three subjects were using combination inhaled corticosteroid–long-acting β2 agonists. Individual spirometry results were within normal limits in both control groups.
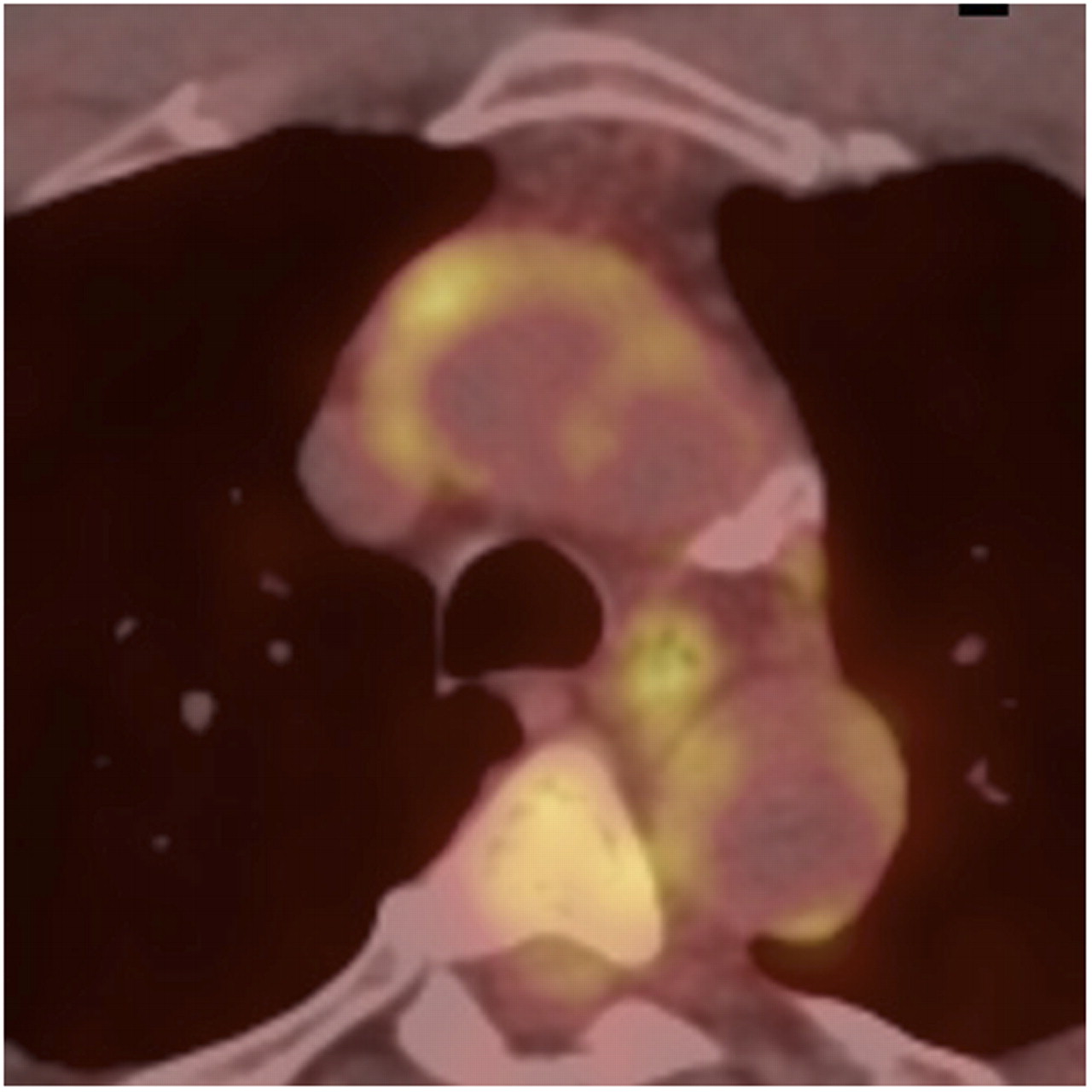
Figure 1 shows an aortic PET/CT image. Both mean and maximum TBRs were greater in the abdominal aorta of COPD patients than ex-smoker controls (mean ± SD, 1.60 ± 0.13 vs. 1.34 ± 0.15, P = 0.0001, and maximum ± SD, 2.14 ± 0.16 vs. 1.83 ± 0.20, P = 0.0001; Figs. 2 and 3).
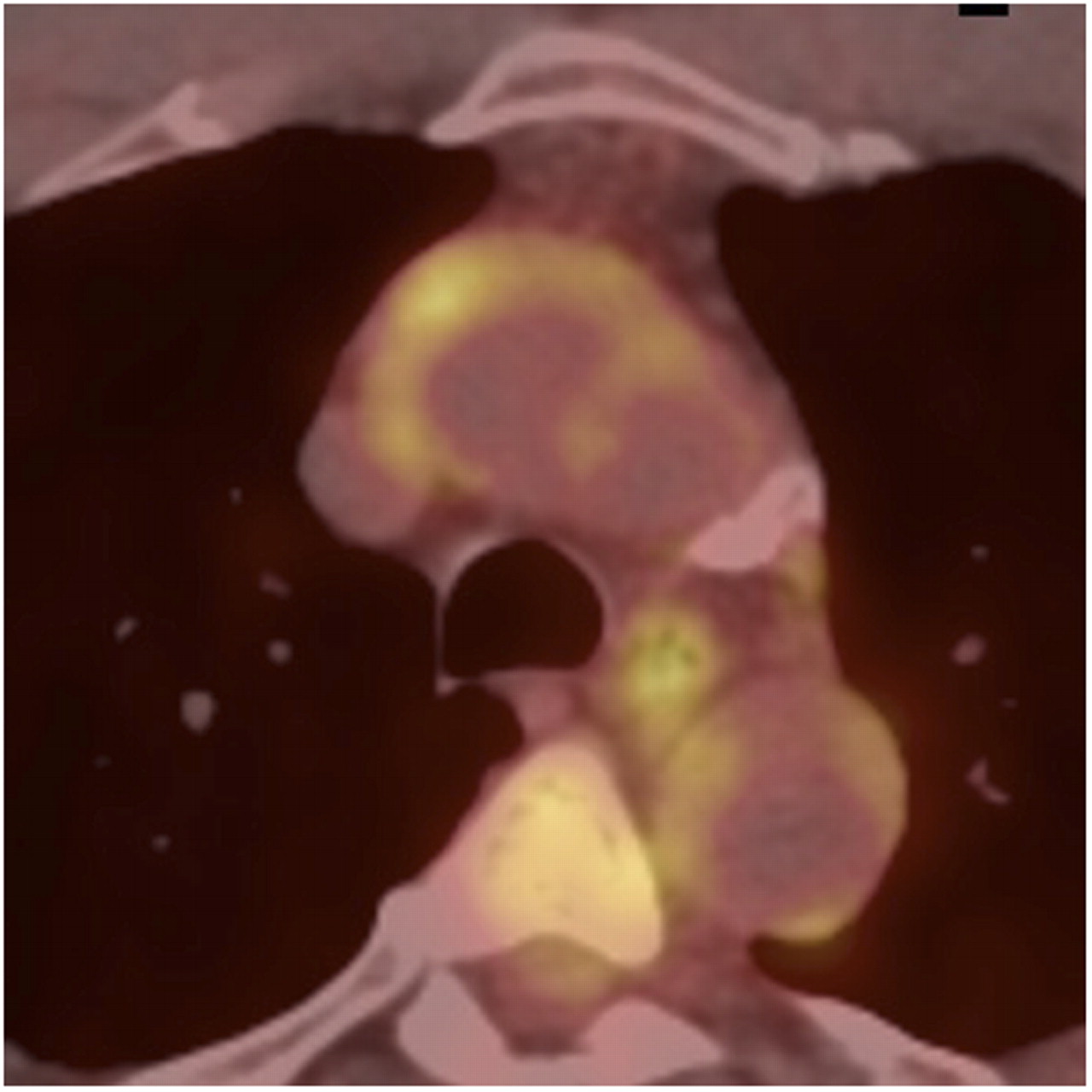
Fused 18F-FDG PET/CT image of aortic arch. Calcium is seen in wall of vessel; also seen is 18F-FDG uptake (golden color), especially in anterior aspect of ascending aorta.

Mean 18F-FDG TBR. *P < 0.05, compared with ex-smokers.

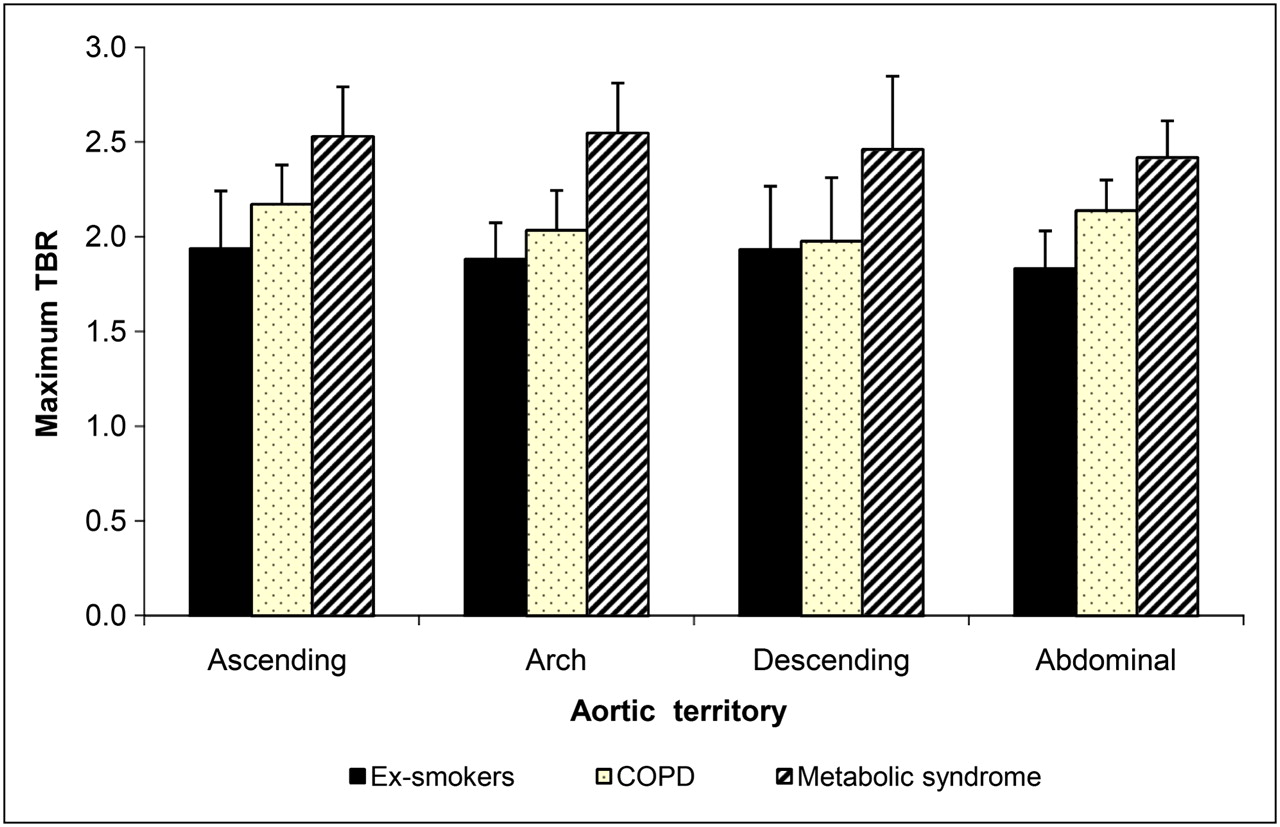
Maximum 18F-FDG TBR. *P < 0.05, compared with ex-smokers.
Aortic arch and abdominal aorta TBRs were greater in the metabolic syndrome group than in the COPD group (Figs. 2 and 3). Compared with ex-smokers, the metabolic syndrome patients had greater mean and maximum aortic TBRs in all territories (Figs. 2 and 3).
No significant difference was observed in carotid artery mean or maximum TBR among the 3 groups (Figs. 2 and 3).
No significant differences were noted in the venous blood 18F-FDG values among the 3 groups (1.01 ± 0.10 in the COPD group, 1.09 ± 0.09 in ex-smokers, and 0.95 ± 0.14 in the metabolic syndrome group; P = 0.115).
Blood pressure and augmentation index were not different among the 3 groups. The aPWV was greater in patients with COPD (10.6 ± 2.8 ms−1) than in ex-smoker controls (8.2 ± 1.7 ms−1) and subjects with metabolic syndrome (9.4 ± 1.5 ms−1), but this difference did not reach significance (P = 0.28). Similarly, interleukin-6 levels did not differ among the 3 groups (Table 1).
DISCUSSION
In this exploratory prospective imaging study, we found that aortic 18F-FDG uptake was increased in COPD patients, compared with ex-smoker controls. The degree of 18F-FDG uptake was intermediate between the negative control ex-smokers and subjects with metabolic syndrome. On the basis of prior work linking arterial 18F-FDG uptake with vascular inflammation (9), this pilot study provides evidence that, in tandem with a systemic inflammatory state (4), there is increased vascular inflammation in patients with COPD and that this may be a contributing factor to increased cardiovascular risk.
Our results are concordant with published work in which subjects with metabolic syndrome had increased vascular inflammation measured by PET. Age, male sex, and waist circumference were strong predictors of 18F-FDG uptake (9,12). Although arterial 18F-FDG uptake—in terms of both extent throughout the aorta and degree—was less in COPD patients than in the metabolic syndrome group, the uptake remained higher in the COPD group than in the negative control ex-smokers, especially in the abdominal aorta, despite the small patient numbers. Similar trends were seen when carotid artery 18F-FDG uptake was compared across groups, although these trends failed to reach statistical significance in our population. We were also not able to relate arterial 18F-FDG uptake to either circulating inflammatory mediators or aPWV, although larger studies have suggested these relationships (8,9).
Within the vascular wall, the exact site of 18F-FDG accumulation is unclear. From autoradiographic and histologic work, we know that 18F-FDG uptake is correlated with macrophage density but not plaque thickness, surface area, or smooth muscle content (8,7). Two recent studies have linked vascular 18F-FDG uptake with gene expression profiles of inflammation (CD68 messenger RNA) (13,14). There is increasing evidence that vascular 18F-FDG uptake portends future cardiovascular events (15,16). Two comprehensive reviews of 18F-FDG PET of atherosclerosis have recently been published (17,18).
Changes in aortic structure and the presence of vascular inflammation have not been well described in patients with COPD. Pulmonary endothelial dysfunction has, however, been documented (19). Vascular dysfunction is also hypothesized as being a contributor to the increased heterogeneity in regional lung perfusion in COPD patients, compared with controls (20).
There were limitations to our study. It was not possible to match smoking history in our patients with COPD and ex-smoker controls. That said, none of the subjects with metabolic syndrome were smokers, yet this group had the greatest 18F-FDG uptake. In addition, although the number of subjects studied was small, we did show significant differences among the groups in terms of aortic inflammation. Future larger studies, well matched for smoking history, are needed to determine the clinical relevance of these findings in terms of the prediction of cardiovascular events in this high-risk patient group.
CONCLUSION
Our small study suggests that aortic 18F-FDG accumulation is increased in COPD patients. Inflammation of the vascular wall was intermediate between ex-smokers without COPD and patients with established metabolic syndrome. 18F-FDG PET might be useful to test the antiinflammatory effect of future drug therapies in COPD and allow mechanistic evaluation of the increased cardiovascular risk to be explored.
Acknowledgments
We thank Dr. Shamus Linnane, Dr. Barry J. McDonnell, Margarate Munnery, and Julia Howard for their technical support. The study was funded by an unrestricted grant from Schering-Plough, the NIHR Nottingham Respiratory Biomedical Research Unit, the NIHR Cambridge Biomedical Research Centre, and a fellowship from the Association of the British Pharmaceutical Industry.
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication February 4, 2010.
- Accepted for publication July 14, 2010.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Effect of Vegan Fecal Microbiota Transplantation on Carnitine- and Choline-Derived Trimethylamine-N-Oxide Production and Vascular Inflammation in Patients With Metabolic Syndrome
- Psoriasis: More Than Just Skin Deep
- Exercise and cardiovascular benefit in subjects with COPD: the need for randomised trials
- Chronic obstructive pulmonary disease: a modifiable risk factor for cardiovascular disease?
- N-(4-18F-Fluorobenzoyl)Interleukin-2 for PET of Human-Activated T Lymphocytes