


Abstract
Radioimmunotherapy is approved by the Food and Drug Administration for CD20 antigen–positive follicular and transformed non-Hodgkin lymphoma. The goal of this study was to obtain the opinion of hematologists and medical oncologists about CD20-directed radioimmunotherapy in the United States. Methods: An e-mail–based survey with 8 questions was sent to 4,239 oncologists and hematologists throughout the United States. Results: Two hundred sixteen (5.0%) oncologists and hematologists responded to our survey. One hundred fifty-seven (72.7%) said they had referred patients with non-Hodgkin lymphoma for radioimmunotherapy in the last 24 mo. Different types of practices had significantly different concerns regarding this treatment. Compared with referring physicians from academic centers, those from nonacademic centers reported significantly higher concerns about the lack of a site to which to refer patients for treatment (P < 0.01), the lack of interest by nuclear physicians in this type of treatment (P < 0.01), and a referral process that they felt was too complicated (P < 0.01). They were also more concerned about an economically adverse effect on their own practices if they referred patients for radioimmunotherapy (P < 0.01). Referring physicians who perceived consolidation as a possible indication for radioimmunotherapy had significantly fewer concerns about an adverse effect on their own practice (P < 0.01) and about nonradioactive alternatives (P < 0.01). Seventy-nine (36.6%) responders thought radioimmunotherapy would probably grow in importance, and 52 (24.1%) responders thought it would definitely grow in importance. However, the group with a positive outlook about the future of radioimmunotherapy predicted a higher growth of radioimmunotherapy if they could administer it in their own offices (P < 0.05). Conclusion: Radioimmunotherapy was generally viewed positively by referring physicians. However, in addition to scientific concerns, barriers to the use of radioimmunotherapy included difficulty in referral, perceptions of a high cost of the treatment, concerns about negative financial outcomes related to referral, and an opinion that the treatment would be used more if given by medical oncologists in their own offices. For the growth of radioimmunotherapy, it appears crucial not only to demonstrate the treatment's safety and efficacy but also to streamline the referral process, to enhance collaboration between specialists, and—it appears—to develop economic incentives for the referring physician.
The radiolabeled monoclonal antibodies 90Y-ibritumomab tiuxetan (Zevalin; Spectrum Pharmaceuticals) and 131I-tositumomab (Bexxar; GlaxoSmithKline) are approved for the treatment of patients with follicular and transformed non-Hodgkin lymphoma (NHL) who failed to respond to or relapsed after prior therapies, including rituximab (Rituxan; Biogen Idec/Genentech) and standard chemotherapy. Recently, 90Y-ibritumomab tiuxetan was approved by the Food and Drug Administration (FDA) as a part of the initial therapy of follicular NHL in the United States.
Proof of concept of 131I bound to anti-CD20 antibodies in patients with relapsed CD20-positive follicular lymphoma (FL) was published in the early 1990s (1). These initial exciting data were confirmed in a phase II trial by the same group and in multicenter studies. 131I anti-CD20 antibodies produced a high overall response rate, and approximately one third of patients had a complete remission despite having chemotherapy-refractory low-grade or transformed low-grade NHL or having experienced a relapse earlier after chemotherapy (2). In untreated patients with advanced-stage FL, 131I-tositumomab showed an overall response rate of 95%, with a rate of complete remission of 74%. In this study, the 5-y progression-free survival was 59%, the toxicity was moderate myelosuppression, and no cases of myelodysplastic syndrome (MDS) or acute leukemia had been observed at the time of the report (3).
Several studies have now reported the benefit of 90Y-ibritumomab tiuxetan in relapsed or refractory CD20-positive FL (4–6). A recent large, prospective phase III trial investigated 90Y-ibritumomab tiuxetan in the setting of consolidation of first-line therapy and showed high efficacy with no unexpected toxicities (7). This study led to the approval of 90Y-ibritumomab tiuxetan for consolidation treatment as a part of first-line therapy in both Europe and now the United States. Other anti-CD20 radiopharmaceuticals, including 131I-rituximab, have shown benefit in relapsed or refractory indolent NHL, with a high overall response rate of 76% (8).
Despite these reports of efficacy and the reasonable safety of 90Y-ibritumomab tiuxetan and 131I-tositumomab, as well as FDA and European Medicines Agency (EMEA) approvals, these treatments appear to be used much less frequently than alternative nonradioactive treatments. The reasons for this low use of CD20-directed radioimmunotherapies are unclear. A front-page article in The New York Times (9) discussed innovative treatments, market factors, and health politics in the choices of treatment for NHL. This article claimed that in the United States the options for drugs to treat cancer, such as radioimmunotherapy, are limited by market forces (9). A further reason for possible underuse was believed to be related to relatively low reimbursement (of the cost of both the drug and the treating physicians) for the administration of these radioimmunotherapeutics (10). Other concerns included the wide range of nonradioactive alternative treatments for CD20-positive lymphomas, possible unexpected late side effects of radioimmunotherapy, and a complicated patient-referral process. Few objective data are available, however, on how oncologists choose to use, or not to use, radioimmunotherapy in patients with NHL.
The goal of this study was to survey referring oncologists for their opinion about CD20-directed radioimmunotherapy in the United States.
MATERIALS AND METHODS
We developed an 8-question survey (Fig. 1), and after testing it in a pilot setting at our own center, used it to systematically question medical oncologists and hematologists about their perception of radioimmunotherapy in NHL. The survey assessed the process of deciding on whether to treat NHL patients with radioimmunotherapy. General perceptions regarding the treatment in the broad areas of evidence-based efficacy, alternative therapeutic options, and logistic barriers to use were explored. Questions about practice-specific and societal economic factors—particularly emphasizing possible concerns about this form of therapy that might detract from its use—were included. To increase the response rate, the questions were kept brief so that the survey could be completed within 10 min.

The survey (square boxes represent multiple answers possible; circles represent only 1 answer possible; items marked with * are required).
SurveyGizmo (Widgix, LLC), an e-mail–based tool drawing on the databases of medical oncologists and hematologists, was used to distribute the survey. Most of the questions were multiple-choice; some had a free-text option. One question about a PET facility in the oncologists' or hematologists' office was not used for this survey and will be reported elsewhere. The Institutional Review Board of the Johns Hopkins University approved the study protocol. Potential responders were informed of the principal investigator's name but were not told whether the principal investigator had any financial interest in either of these forms of therapy. We calculated means and SD. For the multivariate analyses, logistic regression or proportional odds models were fitted for binary or ordered categoric response variables, and linear regression models were fitted for physician concern variables. These models will adjust for potential confounding covariates such as geographics and practice type.
RESULTS
Demographic Characteristics of Study Participants
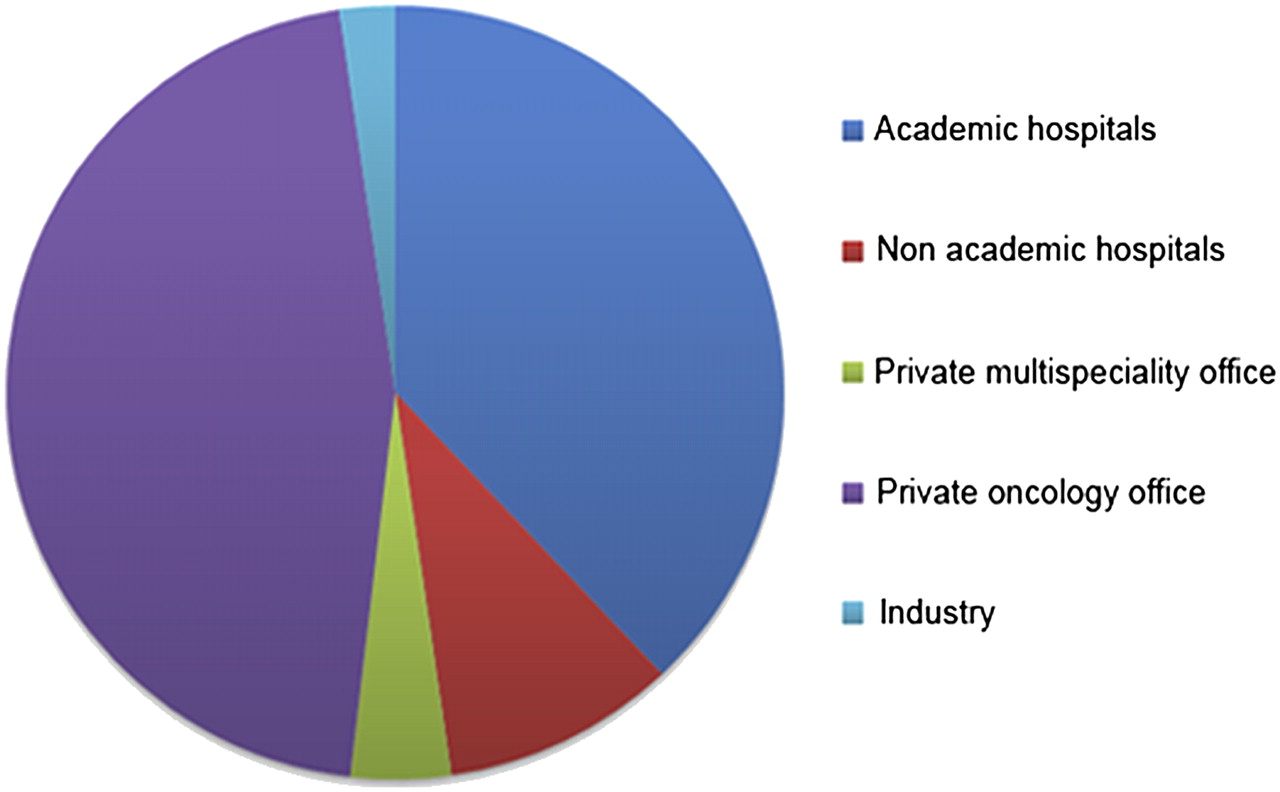
We e-mailed 4,239 surveys. The names and addresses of the recipients were culled from a combination of databases, and we received 216 (5.0%) completed responses. The survey was resent twice at intervals of 7 d if there was no response and was closed after 31 d. A map of the geographic location of the responders is provided in Figure 2. Responders specified their predominant practice location: 82 (38%) worked in university hospitals, 21 (9.7%) in nonuniversity hospitals, 9 (4.2%) in private multispecialty offices, 99 (45.8%) in private oncology offices, and 5 (2.3%) in industry. Our survey allowed only 1 selection for the major type of practice (Fig. 3).
Geographic locations of responders (Yahoo! MapMaker for Excel, version 1.02; Microsoft).
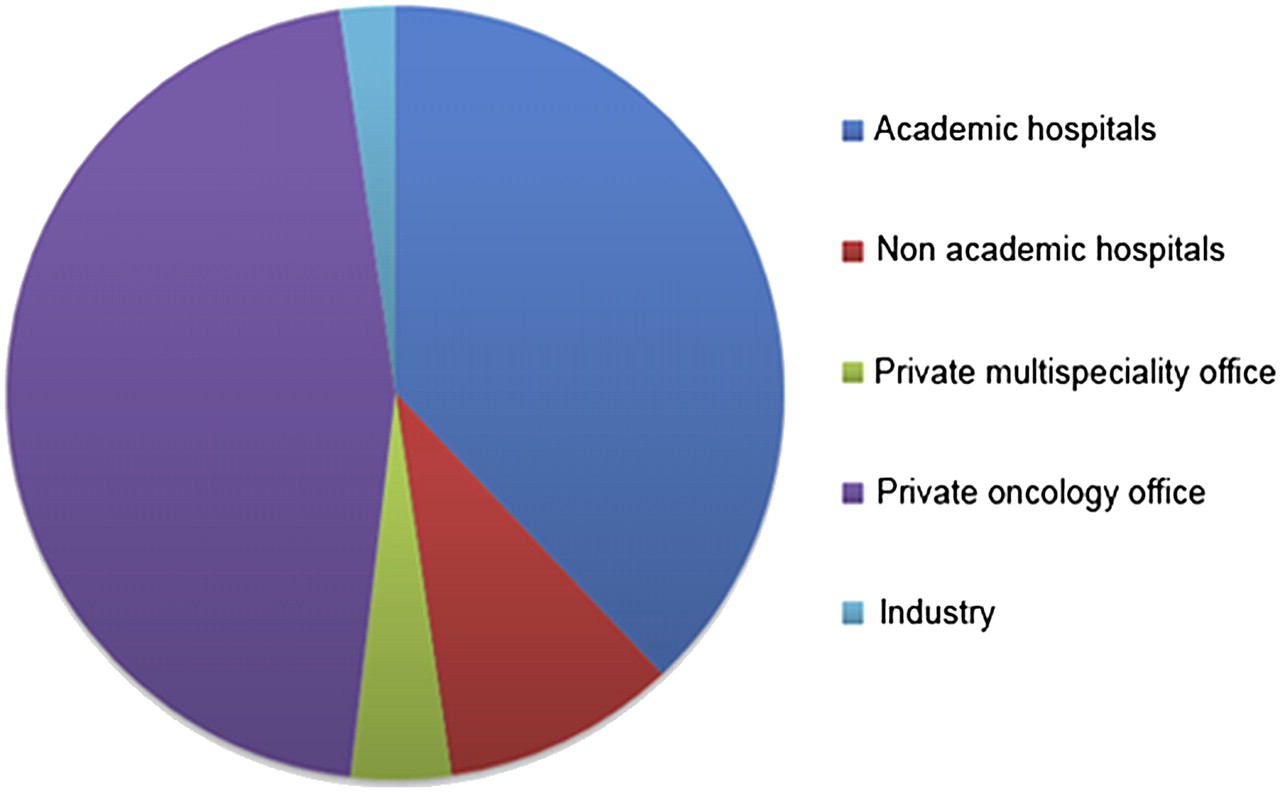
Practice types: academic hospitals, 38%; nonacademic hospitals, 9.7%; private multispecialty offices, 4.2%; private oncology offices, 45.8%; and industry, 2.3%.
Referral Frequencies and Indications
Twenty-one (9.7%) responders saw radioimmunotherapy with 131I-tositumomab or 90Y-ibritumomab tiuxetan as a possible first-line indication, and 111 (51.4%) would refer NHL patients for second-line treatment. One hundred thirty-eight (63.9%) saw this treatment as third-line treatment, and 71 (32.9%) would use it later than third-line treatment. Nine (4.2%) thought radioimmunotherapy with 131I-tositumomab or 90Y-ibritumomab tiuxetan was only investigational at this time. Three (1.38%, 2 from academia and 1 from a nonacademic hospital) stated they would never refer a patient with NHL for radioimmunotherapy. Fifty-four (25%) stated they would refer patients for consolidation after immunochemotherapy. This survey was completed just before U.S. FDA approval of 90Y-ibritumomab tiuxetan as a part of first-line treatment. Figure 4 reports the physician's perceived indications for 131I-tositumomab or 90Y-ibritumomab tiuxetan in patients with NHL.

Preferred indications (%) for use of 131I-tositumomab or 90Y-ibritumomab tiuxetan. Blue = physicians who did treat NHL patients with 131I-tositumomab or 90Y-ibritumomab tiuxetan in last 24 mo (n = 157); red = physicians who did not (n = 59).
Concerns About Anti-CD20 Radioimmunotherapy
The surveyed population rated their concerns about radioimmunotherapy for NHL from 1 (no concern) to 5 (major concern). Nine factors were rated. In decreasing order of concern, these were as follows: (1) 131I-tositumomab or 90Y-ibritumomab tiuxetan theoretically may cause bone marrow damage preventing further therapy (autologous stem cell transplantation) (mean rating, 3.16 ± 0.09). (2) There might be unexpected late side effects of 131I-tositumomab or 90Y-ibritumomab tiuxetan (MDS) (mean rating, 3.04 ± 0.08). (3) There are too many effective nonradioactive treatment alternatives for NHL (mean rating, 3.0 ± 0.09). (4) 131I-tositumomab or 90Y-ibritumomab tiuxetan treatment is too expensive (mean rating, 2.96 ± 0.10). (5) Referring patients for 131I-tositumomab or 90Y-ibritumomab tiuxetan is too complicated (mean rating, 2.50 ± 0.10). (6) Nuclear physicians are not too interested in treating patients with 131I-tositumomab or 90Y-ibritumomab tiuxetan (mean rating, 2.44 ± 0.10). (7) 131I-tositumomab or 90Y-ibritumomab tiuxetan treatment does not have enough reported randomized studies (mean rating, 2.38 ± 0.09). (8) There is no treatment site of 131I-tositumomab or 90Y-ibritumomab tiuxetan that is convenient for my patients (mean rating, 2.12 ± 0.10). (9) It is or would be economically adverse for my practice to use 131I-tositumomab or 90Y-ibritumomab tiuxetan (mean rating, 2.05 ± 0.09).
Predicted Growth of Radioimmunotherapy for NHL
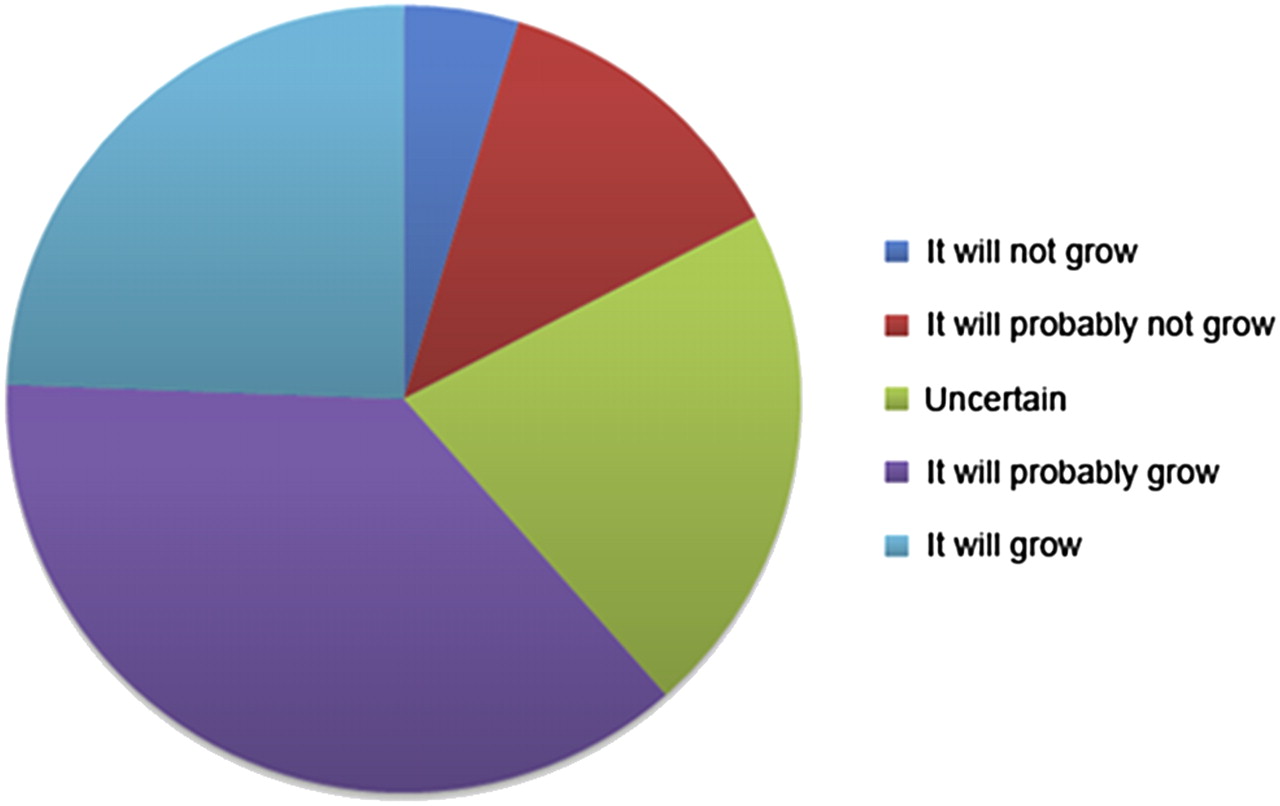
Ten (4.62%) responders thought radioimmunotherapy for NHL would definitely not grow in the future, 27 (12.5%) thought it would probably not grow, 46 (21.3%) were uncertain about the future growth, 79 (36.5%) thought it would probably grow, and 52 (24.1%) thought it would definitely grow (Fig. 5).
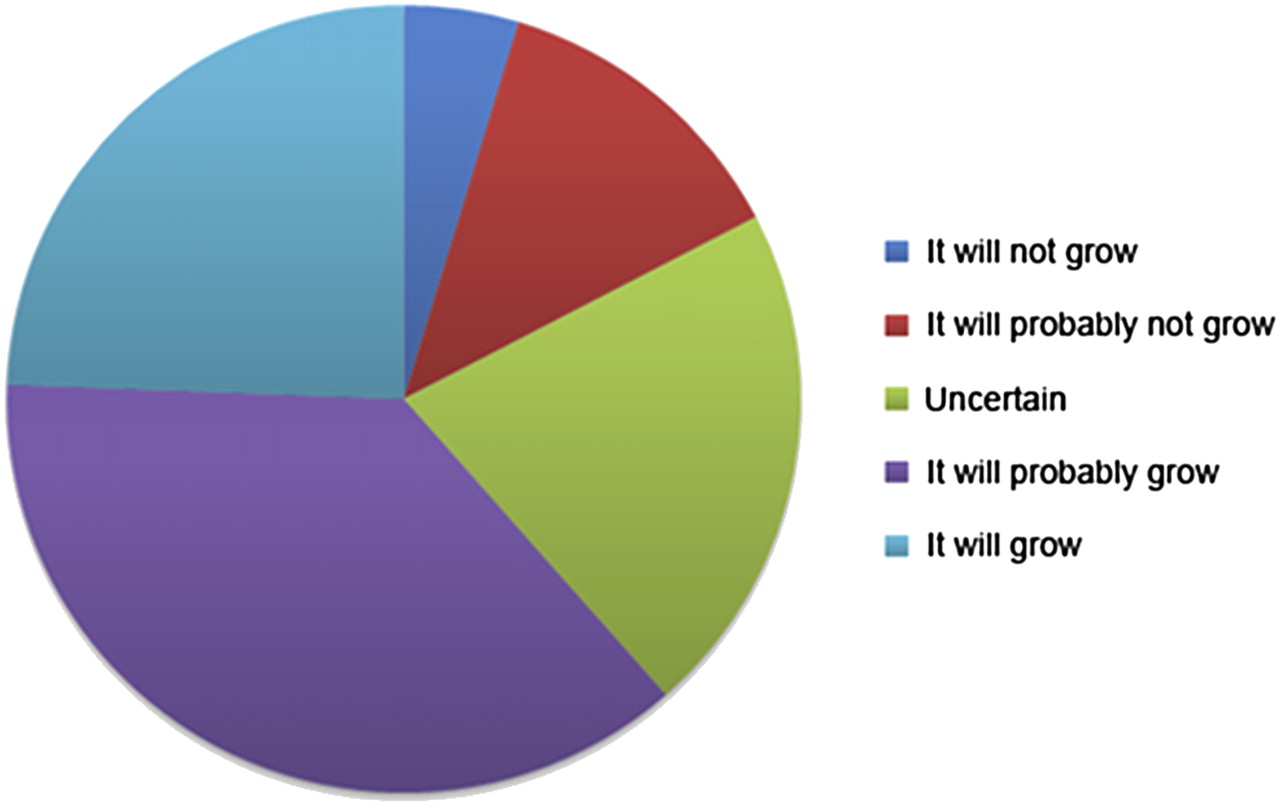
Predicted future growth of 131I-tositumomab or 90Y-ibritumomab tiuxetan radioimmunotherapy for NHL: It will not grow, 4.62%; it will probably not grow, 12.5%; uncertain, 21.3%; it will probably grow, 35.6%; and it will grow, 24.1%.
Predicted Growth of Approved Radioimmunotherapy in Responder's Own Office
Ninety-three (43.1%) responders felt that radioimmunotherapy with 131I-tositumomab or 90Y-ibritumomab tiuxetan would grow in importance if they could give it in their own practice. One hundred twenty-three (56.9%) responders felt this would not affect use of the treatment in their practice.
Further Comments from Responders
This free-text field was open for further comments. Forty-six (21.3%) responders added one or more specific comments. The comments could be categorized easily as medical, scientific, logistic, or economic. Nine comments raised medical concerns: the referring physicians were concerned about possible prolonged myelosuppression and MDS after radioimmunotherapy. Eleven comments pointed toward a lack of randomized trials comparing radioimmunotherapy with conventional treatment. Logistic concerns were raised in 13 comments. Several comments specifically pointed out the complicated referral process and their nuclear physicians' lack of interest in using radioimmunotherapy. Further logistic concerns included losing the patient after referral to an academic medical institution. Thirteen responders expressed economic concerns. They reported the possibility that their practice would not be reimbursed because their patients were referred to another site for radioimmunotherapy. They also agreed that if regulations allowed them to administer 90Y-ibritumomab tiuxetan or 131I-tositumomab within their own practice, their use of this therapy would increase. Further concerns were expressed about reduced reimbursement for standard treatments if the oncologists were to send patients out of their practices for radioimmunotherapy.
Emerging Patterns After Subgroup Analysis
Referral Frequency, by Type of Practice
There was no significant difference in practice type among responders who had referred a patient for radioimmunotherapy (academia vs. nonacademia, P = 0.78; hospitals vs. private practice, P = 0.43). However, the referral frequency was significantly higher in hospitals than in private oncology or multispecialty practices (P < 0.01).
Referral Indication, by Type of Practice
No significant difference between 1 particular line of treatment and a responder's type of practice was observed. Also, responders who saw consolidation as a possible indication after chemoimmunotherapy for their patients with NHL did not significantly differ in their type of practice.
Concerns About Anti-CD20 Radioimmunotherapy
Responders not in academia were more concerned than those in academia about access to a treatment site (P < 0.01), lack of interest by nuclear physicians in these treatments (P < 0.01), a referral process that is too complicated (P < 0.01), and the economic adversity of referring patients for radioimmunotherapy (P < 0.01) (Table 1).
Concerns About Treatment of NHL Patients with 90Y-Ibritumomab Tiuxetan or 131I-Tositumomab
Responders from private practices had more concerns than did responders from hospitals about possible MDS (P < 0.1) after radioimmunotherapy, bone marrow damage preventing further therapy (P < 0.05), lack of a treatment site for patients with NHL (P < 0.01), lack of interest by nuclear physicians (P < 0.1), and a referral process that was too complicated (P < 0.01).
The only significant concern of the subgroup who had referred patients in the last 24 mo was the perception that the higher expense of 90Y-ibritumomab tiuxetan and 131I-tositumomab is associated with lower use (P < 0.05).
Responders who would not refer NHL patients for first- or second-line treatment with 131I-tositumomab or 90Y-ibritumomab tiuxetan tended to believe other nonradioactive treatment alternatives were available (P < 0.1). Physicians favoring early-line treatment did not significantly differ from other physicians in medical or scientific, logistic, or economic concerns. Responders who viewed consolidation as a less appropriate indication for radioimmunotherapy had significantly more concerns about nonradioactive treatment alternatives (P = 0.02), bone marrow damage preventing further therapy (P = 0.02), and the occurrence of later MDS (P = 0.05). However, the most significant concern in this group, which did not consider consolidation to be an indication for radioimmunotherapy, was a perceived adverse economic effect on their own practice from the use of radioimmunotherapy for consolidation (P < 0.01).
Oncologists who predicted an increase in the importance of 131I-tositumomab or 90Y-ibritumomab tiuxetan use in their own office, should regulations allow it, had significantly more concerns about the lack of a treatment site (P < 0.01), the lack of interest by nuclear physicians (P < 0.01), a referral process that was too complicated (P < 0.01), and an adverse economic effect on their practice if they referred patients for radioimmunotherapy (P < 0.01).
Responders who thought radioimmunotherapy for NHL would probably or definitely grow in importance had significantly fewer concerns (or interests) than other responders about nonradioactive treatment alternatives (P < 0.01), bone marrow damage (P < 0.01), a perceived high price of 90Y-ibritumomab tiuxetan or 131I-tositumomab (P = 0.03), the lack of randomized trials (P = 0.01), and late side effects such as MDS (P = 0.01).
Predicted Growth
Seventy-nine responders thought radioimmunotherapy with 90Y-ibritumomab tiuxetan or 131I-tositumomab would probably grow, and 52 responders thought it would definitely grow in importance. However, the optimistic responders could not be significantly assigned to a single practice type. The only additional significant factor by subgroup analysis was that responders who thought this treatment would grow saw greater growth if they could apply the treatment in their own offices (P < 0.05).
DISCUSSION
131I-tositumomab and 90Y-ibritumomab tiuxetan radioimmunotherapy is FDA-approved for follicular and secondary transformed lymphoma after first-line therapy, and as of September 2009, 90Y-ibritumomab tiuxetan is FDA-approved as part of first-line therapy in both the United States and Europe. Despite the increasing evidence of efficacy and the relatively low reported toxicity, this relatively new form of treatment is not as extensively used as other therapies for lymphoma. This study is the first, to our knowledge, to analyze medical oncologists' perceptions and use of radioimmunotherapy with 131I-tositumomab or 90Y-ibritumomab tiuxetan in the United States. Our goal was to identify the challenges that need to be overcome to increase the use of radioimmunotherapy. Although new cancer therapies are typically more expensive than therapies using older drugs, determining how oncologists select therapies for their patients could add information to the health care debate.
Only 5.0% of the invited oncologists answered this survey. This number appears low but is in the expected range for e-mail–based surveys (11). Radioimmunotherapy is certainly used by our group of responders: 157 (72.7%) had referred patients with NHL for radioimmunotherapy with 131I-tositumomab or 90Y-ibritumomab tiuxetan in the past 24 mo. However, there may be a bias because our responders may be more interested than the nonresponders in this form of treatment. More than 60% of the responders saw 90Y-ibritumomab tiuxetan or 131I-tositumomab as a suitable second- or first-line treatment for patients with NHL. An even a larger group saw radioimmunotherapy for later indications as third-line (n = 138) or even post–third-line therapy (n = 71), and their only significant concern was the availability of nonradioactive alternative treatments.
There are several agents for second-line treatment of FL. Retreatment with rituximab shows an overall response of 40%, with 11% complete remissions (12). Rituximab, combined with cyclophosphamide, doxorubicin, vincristine, and prednisone, demonstrates a 30% complete response rate (13). Overall, there is a broad variety of choice in the treatment of lymphoma, and this might be one of the most important hurdles for the future of radioimmunotherapy (14–18).
Fifty-four (25%) responders would refer patients for radioimmunotherapy for consolidation after immunochemotherapy. This indication recently received regulatory approval in Europe and the United States for marketing. These responders did not significantly differ from the others in type of practice.
A recent randomized multicenter phase III trial (FIT Trial (6)) investigated 90Y-ibritumomab tiuxetan as first-line consolidation therapy. 90Y-ibritumomab tiuxetan was given as a single therapeutic dose in patients with advanced (stage III or IV) FL who achieved a partial or complete remission after receiving various induction chemotherapy regimens. In 414 patients, the results showed a significantly prolonged median progression-free survival, from 13.3 to 36.5 mo. However, in the small subgroup of patients receiving previous rituximab therapy, the prolongation of progression-free survival was not significant.
The nonradioactive alternative is prolonged rituximab maintenance. This treatment was recently analyzed in a large systematic review, and a higher rate of severe infections was observed. The result was a black-box warning issued by the FDA regarding long-term use of rituximab because of the occurrence of progressive multifocal leukoencephalopathy (19). However, superior rates of overall survival were found for patients with relapsed disease (hazard ratio, 0.58; confidence interval, 0.42–0.79), but the survival benefit was not consistent for patients after first-line treatment (20).
We observed the interplay of potential competing medical and economic interests in our survey. The responders who would consolidate had significantly fewer concerns about nonradioactive alternatives (P = 0.02) than those who would not consolidate, but these responders also perceived an adverse economic effect on their own practice (P < 0.01).
The future growth of radioimmunotherapy with 131I-tositumomab or 90Y-ibritumomab tiuxetan was judged to be positive by most of our responders. There was no single type of practice in which most of the responders had a positive outlook about the future growth of radioimmunotherapy. However, logistic regression did show that positive responders thought radioimmunotherapy for NHL would grow even more if it could be given in their own practice (P = 0.03). Responders who thought that referring patients away from their practice for treatment would be economically adverse to their practice also thought radioimmunotherapy would grow more if it could be given in their own practice (P < 0.01). This response clearly showed a high economic stake affecting perceptions about radioimmunotherapy use, which is a factor in the perception of growth for the future of radioimmunotherapy therapy.
In the free-text field a responder wrote, “These drugs are of great value in patients with lymphoma but will never be used in the number of patients that could benefit because of present logistic and regulatory restrictions. If the drug could be easily ordered or even administered by medical oncologists, this would improve the situation greatly.” The effects that beneficiaries and generous reimbursement have on the choice of cancer treatment have been discussed previously (21,22).
Responders not from academia were significantly more concerned than those from academia that referral of patients for radioimmunotherapy would have an adverse economic effect on their practice (P < 0.01). One responder wrote, “This treatment is underutilized and difficult to arrange at tertiary centers, I believe, in large part because of the reimbursement reward to practicing oncologists and the need to involve and educate nuclear medicine physicians.” This comment and others clearly demonstrate the importance of logistic and economic factors affecting the availability of radioimmunotherapy for NHL.
The nonacademic responders were significantly more concerned about the lack of a treatment site, the lack of interest by nuclear physicians, and a referral process that was too complicated.
The only significant concern in the group that did not treat any NHL patients within the past 24 mo was the high price of 131I-tositumomab and 90Y-ibritumomab tiuxetan. Currently, Medicare reimburses hospitals about $16,000 for each treatment with radioimmunotherapy (23). The cost for combined chemoimmunotherapy with cyclophosphamide, doxorubicin, vincristine, and prednisone and rituximab is about $17,000 (24), making the price for these second-line treatments comparable. The reimbursement practice by Medicare for 90Y-ibritumomab tiuxetan and 131I-tositumomab has been questioned, and hospitals administering radioimmunotherapy to patients with NHL may lose about $10,000 per treatment (25). This might be one of several explanations of why some hospitals stopped providing radioimmunotherapy for patients with NHL.
CONCLUSION
Overall, we see a positive perception for radioimmunotherapy in this population of referring U.S. oncologists. Our data indicate that economic and logistic effects on the oncologists' practice are important. Some fear that by referring a patient away from their practice for radioimmunotherapy, they may lose that patient. Others fear the loss of revenue from treatments at their own site resulting from referral to other sites for this treatment. This could be one of several reasons why radioimmunotherapy is not more widely used. Of course, in an ideal world, the choice of cancer treatment for a specific patient should be based on the most effective therapy for that patient, and perhaps on its cost-effectiveness, without any influence from its profitability to the treating physician.
It seems crucial for the future of radioimmunotherapy not only to demonstrate that the treatment process is safe and efficacious but also to streamline the process to provide easy referrals and better collaboration among specialists and to ensure that appropriate safeguards are developed so that the economic concerns of the referring physician are not a significant factor in their choice of cancer treatment for patients with lymphoma.
Acknowledgments
We thank Dr. Richard F. Ambinder for his kind support. Dr. Richard L. Wahl is one of the inventors of anti-CD20 radioimmunotherapy and receives payments from the University of Michigan as part of a patent licensing agreement related to royalties from the U.S. sales of the radioimmunotherapy agents 131I-tositumomab and 90Y-ibritumomab tiuxetan. This arrangement has been disclosed to and is managed by the JHU COI committee.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 25, 2009.
- Accepted for publication February 3, 2010.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Current Landscape in Clinical Pretargeted Radioimmunoimaging and Therapy
- Proceedings of the Second NCI-SNMMI Workshop on Targeted Radionuclide Therapy
- Advances in the treatment of hematologic malignancies using immunoconjugates
- Targeted Radionuclide Therapy: Proceedings of a Joint Workshop Hosted by the National Cancer Institute and the Society of Nuclear Medicine and Molecular Imaging
- Radioimmunotherapy in Non-Hodgkin Lymphoma: Opinions of Nuclear Medicine Physicians and Radiation Oncologists
- Radioimmunotherapy of relapsed indolent non-Hodgkin lymphoma with 131I-rituximab in routine clinical practice: 10-year single-institution experience of 142 consecutive patients