


Abstract
A significant antitumor effect was previously observed with radioimmunotherapy using anti–carcinoembryonic antigen 131I-F6 monoclonal antibody in medullary thyroid cancer–bearing nude mice. Nevertheless, no complete response was observed. As seen with chemotherapy, drugs targeting the tumor microenvironment might improve radioimmunotherapy efficacy. This study evaluated the toxicity and efficacy of combining radioimmunotherapy with thalidomide or a cyclopeptidic vascular endothelial growth inhibitor (CBOP11) in mice grafted with the TT human medullary thyroid cancer cell line. Methods: Six to 10 nude mice treated with 92.5 MBq of 131I-F6 in association with 200 mg/kg/d of oral thalidomide during 20 d by force-feeding or 0.45 mg/kg/d of CBOP11 during 25 d using subcutaneous minipumps were compared with control mice receiving either treatment or naked F6 or nonspecific 131I-734. Combined therapies included 131I-F6 at day 0 followed by thalidomide between days 20 and 40, thalidomide between days 0 and 20 followed by 131I-F6 at day 25, 131I-F6 at day 0 and CBOP11 between days 0 and 25, CBOP11 between days 0 and 25 followed by 131I-F6 at day 25, and 131I-F6 at day 0 followed by CBOP11 between days 20 and 45. Animal weight, hematologic toxicity, tumor volume, and serum calcitonin were monitored for the following 3 mo. Improvement of 125I-F6 tumor biodistribution by antiangiogenic drug was studied after pretreatment by thalidomide. Follow-up of the tumor after combined antiangiogenic and radioimmunotherapy therapies was performed by histology studies. Results: Combined associations, as compared with radioimmunotherapy alone, increased leukopenia but not thrombocytopenia. Tumor volume–quadrupling time (TVQT) was 22.8 ± 3.3 d in the control group, 29.9 ± 3.6 d in the group treated with thalidomide, 34.6 ± 4.4 d in the group treated with CBOP11, and 51.0 ± 2.8 d after radioimmunotherapy alone. As compared with radioimmunotherapy, TVQT was significantly longer (P < 0.01) after thalidomide followed by radioimmunotherapy (69.83 ± 3.9), CBOP11 followed by radioimmunotherapy (71.3 ± 6.1), and CBOP11–radioimmunotherapy in concomitance (64.2 ± 6.1). Nevertheless, TVQT was not increased after radioimmunotherapy followed by thalidomide (48.8 ± 4) and radioimmunotherapy followed by CBOP11 (56.8 ± 4.8). Surprisingly, pretreatment by CBOP11 or thalidomide sensitized larger tumors (>300 mm3) to radioimmunotherapy. Change in calcitonin levels confirmed morphologic tumor response. Tumor uptake 24 h after injection of 125I-F6 was 4.5 ± 0.6 percentage injected dose per gram (%ID/g) without pretreatment and 8.7 ± 1.3 %ID/g with pretreatment by thalidomide. An increase of the antitumor effect observed using the antiangiogenic drug combined with radioimmunotherapy was correlated with a decrease of blood vessels shown by von Willebrand immunostaining. Conclusion: Pretreatment with antiangiogenic therapies improved radioimmunotherapy efficacy, with acceptable toxicity. Future investigations will be performed to understand how antiangiogenic agents sensitize large tumors to radioimmunotherapy.
- radioimmunotherapy
- antiangiogenic therapy
- medullary thyroid cancer
- thalidomide
- vascular endothelial growth inhibitor
Radioimmunotherapy is a validated therapeutic modality for the treatment of non-Hodgkin lymphoma. Several clinical studies have shown high response rates for both myeloablative and nonmyeloablative activities in patients with recurrent or refractory lymphoma (1,2). For more radiation-resistant solid tumors requiring higher tumor absorbed dose, radioimmunotherapy efficacy is actually restricted to residual disease stages or indolent type of carcinoma, with repeated courses of radioimmunotherapy or with therapy combining radioimmunotherapy and radiosensitizing chemotherapeutic agents (3–6).
Angiogenesis (sprouting of new microvasculature from existing blood vessels) is critical to sustain the nutrient and oxygen supply during tumor growth and metastatic spreading of most malignant neoplasms (7,8). In the absence of angiogenesis, tumors cannot grow beyond 1–2 mm because diffusion of oxygen and nutrients limits their size. Direct correlations between density of microvessels, metastases, and survival of patients have been shown (9–11). Moreover, our recent works showed that tumor regression after external high-dose radiotherapy is dependent on endothelial apoptosis and tumor vasculature necrosis (12). Then, pharmacologic inhibition of tumor endothelium growth combined with radioimmunotherapy against tumor cells will target different cellular components and may benefit the treatment of solid tumors.
Medullary thyroid carcinoma (MTC) is a neuroendocrine tumor representing about 10% of all thyroid cancers. Because an MTC tumor expresses and secretes carcinoembryonic antigen (CEA), it constitutes a potential application for radioimmunotherapy with anti-CEA antibodies (13). Our group demonstrated the efficacy of radioimmunotherapy in the treatment of MTC in animal model or in phase I/II clinical trials (14–17). Nevertheless, radioimmunotherapy efficacy must be improved, in particular in cases of aggressive forms of carcinoma or large tumor masses. Moreover, MTC appeared a good model to study combinations of antiangiogenic treatment and radioimmunotherapy, because of the sensitivity of neuroendocrine tumors to the antiangiogenic treatments (18).
The purpose of the present study was to assess the efficacy and toxicity of combined antiangiogenic therapy and anti-CEA radioimmunotherapy in nude mice grafted with a human MTC cell line. Two different antiangiogenic drugs have been evaluated: thalidomide—which induces apoptosis of endothelial cells—and a cyclopeptidic vascular endothelial growth inhibitor (VEGF)—CBOP11—which inhibits VEGF-induced endothelial cell proliferation (19,20). A significant part of the study focused on the determination of the best relative timing for radioimmunotherapy and antiangiogenic treatment.
MATERIALS AND METHODS
Cell Line
The TT line of human MTC obtained from the American Type Culture Collection for use in this study expresses CEA on its cell membrane and secretes calcitonin. It was cultured as adherent-cell monolayers in RPMI medium (Gibco BRL) to which was added 10% fetal calf serum (Gibco BRL), 1% glutamine (l-glutamine, 200 mM; Gibco BRL), and 1% antibiotic (penicillin, 100 U/mL, and streptomycin, 100 U/mL; Gibco BRL).
Animal Model
Nude mice more than 10 wk old were purchased from Janvier. Mice were housed at the animal core facility of the Cancer Research Center. This facility is approved by the French Association for Accreditation of Laboratory Animal Care and is maintained in accordance with the regulations and standards of INSERM and the French Department of Agriculture. Mice were grafted subcutaneously in the right flank with 106 TT cells in 0.3 mL of sterile normal saline solution. The animals were housed in aseptic conditions. Lugol's solution (0.1%) was added to drinking water (1 mL/100 mL) the week before and then 2 wk after the injection of the radioiodinated monoclonal antibody (mAb).
Antibody, Labeling, and Controls
The reference antibody was an anti-CEA F(ab′)2 fragment designated F6. This mouse IgG1 antibody, used as the F(ab′)2 fragment, was purchased from Immunotech SA. The F(ab′)2 fragment of nonspecific 734 antibody (Immunotech SA) was used as control. The antibody was labeled using IODO-GEN (Pierce) as described by Fraker et al. (21). The specific activity of the 131I-radiolabeled antibody, measured using an ionization chamber (Medi-202; Medisystème), ranged from 180 to 350 MBq/mg for the different preparations. The radiochemical purity, as determined by instant thin-layer chromatography (ITLC) on ITLC–silica gel paper (Gelman), was always above 98%. The immunoreactivity, assessed using antiidiotype antibody 44-12-13 (kindly provided by Immunotech SA), was 85%−96%.
Experimental Radioimmunotherapy and Antiangiogenic Treatment
Groups of 6–12 mice each were studied. The different treatment procedures are summarized in Figure 1. A group with an initial tumor volume of 101 ± 32 mm was injected with 92.5 MBq (250 μg) of 131I-F6 fragment. mAb diluted in 0.2 mL of sterile normal saline solution was injected into the lateral tail vein. The maximal tolerated dose of radioimmunotherapy, determined in a preliminary study, was 92.5 MBq (Françoise Kraeber-Bodéré, unpublished data, 1999). Two antiangiogenic agents were used in this study. Thalidomide was suspended in hydroxy-propyl-methyl-cellulose E4 M premium grade 2910 (Colorcon). CBOP11, an antagonist of VEGF, was diluted in normal saline solution. Two groups were treated with 200 mg/kg/d of thalidomide during 20 d by force-feeding or with 0.45 mg/kg/d of CBOP11 during 25 d using a subcutaneous 2004 Alzet osmotic minipump (Zilberberg JBC 2003). Initial tumor volumes in these groups were, respectively, 99 ± 58 and 92 ± 38 mm. Combined therapies included 131I-F6 at day 0 followed by thalidomide between days 20 and 40, thalidomide between days 0 and 20 followed by 131I-F6 radioimmunotherapy at day 25, 131I-F6 at day 0 and CBOP11 between days 0 and 25, CBOP11 between days 0 and 25 followed by 131I-F6 radioimmunotherapy at day 25, and finally 131I-F6 at day 0 followed by CBOP11 between days 20 and 45. Initial tumor volumes in these groups were, respectively, 78 ± 36, 87 ± 49, 108 ± 56, 102 ± 35, and 88 ± 31 mm. The treatment group including injection of 131I-F6 at day 0 in parallel with thalidomide between days 0 and 20 was technically infeasible to handle, because of the incapacity to force-feed the highly radioactive mice the first 7 d after the radioimmunotherapy. Two control groups were treated with 92.5 MBq of nonspecific 131I-734 and 250 μg of naked F6. The initial volumes of these 2 groups were, respectively, 113 ± 55 and 228 ± 94 mm. In all these treated groups, the initial tumor volume used as a reference to compare the efficacy of the different therapy protocols was the volume determined at the beginning of the first treatment. Another group with large tumors (383 ± 142 mm) was also treated by radioimmunotherapy alone (92.5 MBq) and compared with the 2 groups treated by radioimmunotherapy with similar tumor volume but pretreated by the 2 antiangiogenic agents. In these 2 groups, tumor volumes after thalidomide or CBOP11 were, respectively, 502 ± 201 and 466 ± 231 mm when radioimmunotherapy was administered. Finally, a control group of 12 mice received no treatment. Tumor length, width, and thickness were measured with a sliding caliper twice weekly for 150 d. Tumor volume was calculated according to the formula volume = length × width × thickness × 0.5. All animals were weighed on the day of injection and then twice a week for 90 d. Biologic monitoring was performed on a blood sample drawn from the inner border of the eye. The parameters used to evaluate the toxicity of each type of treatment were maximal weight loss and variation in the number of leukocytes and platelets measured on day 0, 15, 30, 45 and 60. The parameters used to evaluate the efficacy of each type of treatment were tumor volume–quadrupling time (TVQT) or tumor volume–doubling time (TVDT) and the variation in serum calcitonin concentration measured by radioimmunoassay on days 0, 30, 60, and 90 (calcitonin immunoradiometric assay; CIS Bio International). Data are expressed as the ratio between calcitonin serum level at a given time after treatment initiation and the value measured just before treatment.

Treatment timeline. RIT = radioimmunotherapy.
Biodistribution Study
In the aim to understand the mechanisms underlying the effect of pretreatment using an antiangiogenic agent, biodistribution studies were compared in mice injected with 125I-F6 (37 kBq, 30 μg) with oral pretreatment using thalidomide (thalidomide between days 0 and 20 followed by 125I-F6 at day 25). Biodistribution was assessed at 24 and 72 h (3 mice per time point). Tumor and organs were removed and weighed, and then the radioactivity was counted by a γ-counter. The results were expressed as percentage injected dose per gram (%ID/g).
Histologic Study
Histologic analysis of tumors treated with radioimmunotherapy or antiangiogenic drugs was performed at 15, 30, 45, and more than 60 d to establish overall tumor morphology and specific markers of antitumor efficacy. After tumors were harvested, they were fixed in 4% formol, embedded in paraffin, and cut into 4-μm sections. Degree of cellular pleomorphism was studied by hemalum–eosin–safranin staining, and necrosis was estimated by cell size and density, the nucleocytoplasmic ratio, the appearance of chromatin, and the size of nucleoli. Cellular reactivity with anti-CEA mAb was studied by an indirect immunoperoxidase staining. Tumor cell proliferation was assessed by hybridization with Ki67 antibody (MIB-1 clone; Dako). Degree of tumor cell proliferation after treatment was estimated in function of the tumor proliferation without treatment. Endothelium vasculature was detected with a brown biotin staining after hybridization with anti–von Willebrand factor (polyclonal antirabbit; Dako) and counterstaining with hematoxylin. Degree of tumor vasculature regression after treatment, as compared with the tumor vasculature without treatment, was estimated by brown vessels counting on the different fields (original magnification, ×200).
Statistical Analysis
Because of the limited number of animals, the means for the quantitative variables of the different groups were compared using nonparametric tests (the Mann–Whitney U test for comparison of 2 groups and the Kruskall–Wallis test for comparison of more than 2 groups). P values of 0.05 or less were considered significant. BMDP Statistical Software, version 7.0 (Statistical Solutions Ltd.), was used for the analysis.
RESULTS
Treatment Toxicity
No significant weight loss was observed in mice treated with the different therapies (<8% in all treated groups vs. control). In untreated controls, the mean leukocyte concentration was 2,700/mm3 (range, 800–7,000/mm3) and that of platelets 1.4 106/mm3 (range, 0.57–2.7 106/mm3). Toxicity on leukocytes and platelets was expressed as the percentage of the concentration relative to basal value (Table 1). Percentages between 70% and 130% were considered normal. When a significant decrease of blood counts was observed at day 60, additional counting was performed at day 75.
Blood Cell Variations at Different Days After Treatment
No significant leukopenia was observed after thalidomide treatment. After radioimmunotherapy alone and CBOP11, the leukopenia nadir was observed at day 15 with, respectively, 41% ± 21% and 41% ± 25% of initial concentration, and the concentration was restored by day 30. In the group treated by thalidomide followed by radioimmunotherapy, the nadir was observed at day 45 (26% ± 26%), and leukocyte counts were restored at day 60; in the group treated by radioimmunotherapy followed by thalidomide, the nadir was observed at day 15 (34% ± 24%), with recovery at day 30. This leukopenia was related to radioimmunotherapy. In the group treated by CBOP11 followed by radioimmunotherapy, the nadir was observed at day 30 (41% ± 19%), with recovery at day 75; in the group treated by radioimmunotherapy and CBOP11 in concomitance, the nadir was observed at day 15 (29% ± 27%), with recovery at day 45. In the group injected by radioimmunotherapy followed by CBOP11, leukopenia was observed at day 15 (43% ± 22%), with recovery at day 45.
A moderate thrombocytopenia was observed at day 15 after radioimmunotherapy; radioimmunotherapy followed by thalidomide, and radioimmunotherapy followed by CBOP11 (Table 1). Platelet counts were restored at day 30. In the other groups, no thrombocytopenia was observed. A significant increase of platelet concentration was noted after radioimmunotherapy (days 45 and 60), thalidomide followed by radioimmunotherapy (day 30), CBOP11 followed by radioimmunotherapy (day 30), and radioimmunotherapy and CBOP11 in concomitance (days 45 and 60).
After reaching the nadir, hematopoiesis was restored spontaneously in all groups of mice. Two animal deaths (days 20 and 52 after injection of 131I-734) were recorded during the monitoring period. The death occurring at day 20 was related to leukopenia; the one that occurred on day 52 was related to infection (as verified by histologic study at autopsy).
Efficacy of Combination of Thalidomide and 131I-F6
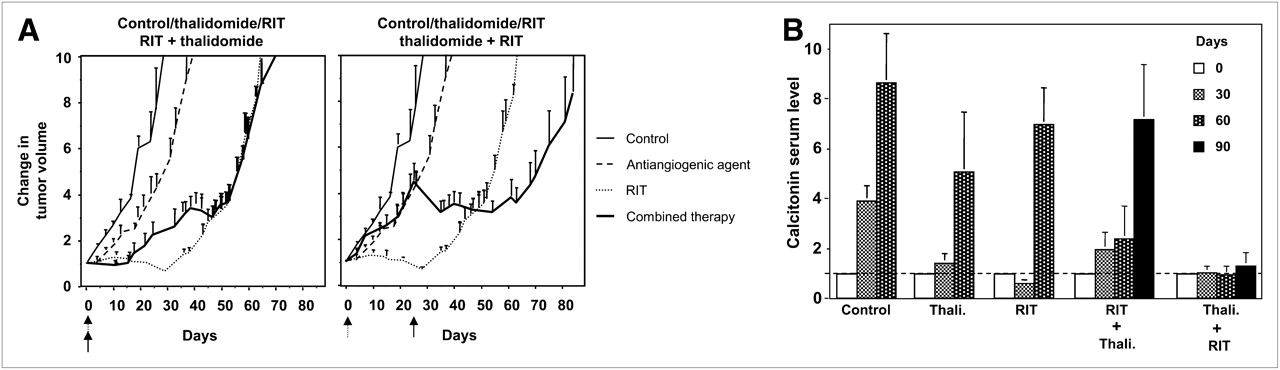
Thalidomide and 131I-F6 were evaluated as single-modality therapeutic agents and in combination (Fig. 2A). Supplemental Figure 1 (supplemental materials are available online only at http://jnm.snmjournals.org) shows the TT tumor growth curves in the control groups. A rapid tumor growth was observed in the 3 control groups. Therapeutic efficacy of the different treatments was compared using TVQT measurement (t = 0 was considered at the beginning of the first treatment of the protocol). TVQT was 22.8 ± 3.3 d in the nontreated control group, 29.9 ± 3.6 d in the group treated with thalidomide, and 51.0 ± 2.8 d after radioimmunotherapy alone (Supplemental Fig. 2). As compared with the radioimmunotherapy value, TVQT was significantly longer (P < 0.01) after thalidomide followed by radioimmunotherapy (74.1 ± 5.2). Nevertheless, TVQT was not increased after radioimmunotherapy followed by thalidomide (54.5 ± 6.8). Changes in calcitonin concentrations were parallel to those in tumor volumes (Fig. 2B). In the control group, the ratio of calcitonin concentration to pretreatment value increased rapidly and correlated to tumor size. This ratio was 4.09 ± 1.46 at day 30. Radioimmunotherapy had a strong biologic effect, with a ratio of 0.59 ± 0.31 at day 30. Using thalidomide alone, a moderate effect was observed, with a ratio of 1.39 ± 0.93 at day 30. Thalidomide followed by radioimmunotherapy allowed a prolonged biologic effect, with ratios of 1.04 ± 0.9, 1.02 ± 0.69, and 1.3 ± 0.63 at days 30, 60, and 90, respectively. Radioimmunotherapy followed by thalidomide slightly delayed the increase of calcitonin concentrations, as compared with the group treated only by radioimmunotherapy. TVDT (t = 0 was considered to be the time of the radioimmunotherapy injection) was calculated to assess the sensitization of radioimmunotherapy effects by the antiangiogenic drugs (Supplemental Fig. 2). Only pretreatment by thalidomide prolonged the tumor response to radioimmunotherapy (TVDT = 54.8 ± 3.7), as compared with radioimmunotherapy alone (TVDT = 42.3 ± 2.8, P = 0.02).

Efficacy of combination of thalidomide and 131I-F6 radioimmunotherapy. (A) Changes in TT tumor volume in treated mice and controls. Graphs show relative tumor volume (ratio of tumor volume to initial size before treatment) as function of time. Tumor volume in control group and group treated by thalidomide or radioimmunotherapy alone are shown in background in gray for comparison with combined therapy. Arrows show day of radioimmunotherapy injection. (B) Changes in calcitonin concentration (pg/mL) in treated mice and controls. Graphs show relative calcitonin concentration (ratio of calcitonin concentration to initial concentration before treatment) as function of time. RIT = radioimmunotherapy; Thali = thalidomide.
Efficacy of Combination of CBOP11 and 131I-F6
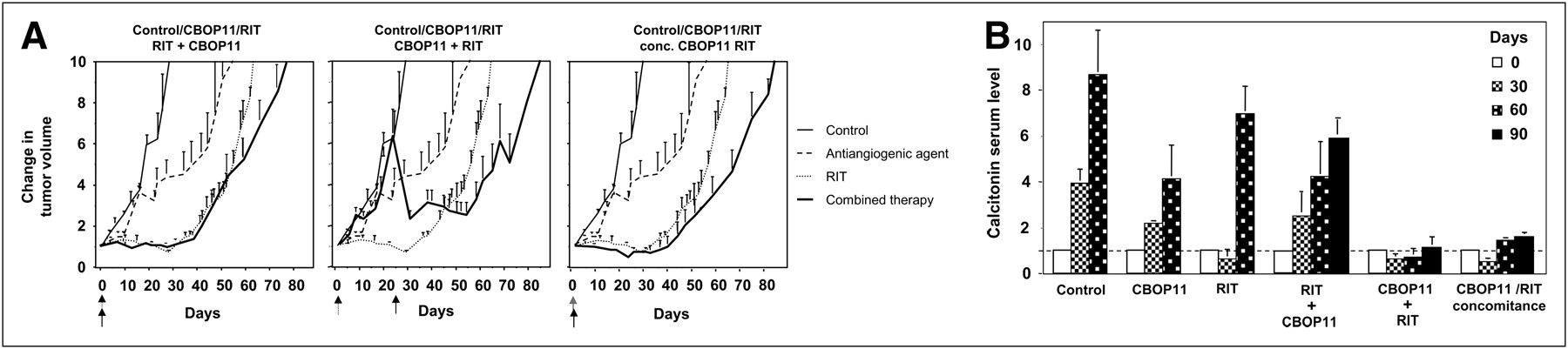
CBOP11 and 131I-F6 were evaluated as single-modality therapeutic agents and in combination (Figs. 3A and 3B). TVQT was 34.6 ± 4.4 d in the group treated with CBOP11 alone (Supplemental Fig. 2). As compared with the radioimmunotherapy value (51.0 ± 2.8 d), TVQT was significantly longer after CBOP11 followed by radioimmunotherapy (74.0 ± 13.1) and CBOP11 and radioimmunotherapy in concomitance (60.2 ± 4.7) (P < 0.01). TVQT was not increased when CBOP11 was given after radioimmunotherapy (56.8 ± 4.8). Changes in calcitonin concentrations were parallel to those in tumor volume (Fig. 3B). Using CBOP11 alone, we observed a small effect, with a ratio of 2.07 ± 1.17 at day 30. Treatments using CBOP11 followed by radioimmunotherapy or combined with radioimmunotherapy achieved a prolonged biologic effect. Ratios at day 90 were 1.54 ± 0.29 and 1.88 ± 0.12, respectively. When radioimmunotherapy was followed by CBOP11, a slight effect was observed, with a ratio at day 60 of 4.15 ± 1.71. TVDT was calculated to assess the sensitization of radioimmunotherapy effects by CBOP11 (Supplemental Fig. 2). Pretreatment and concomitant treatment by CBOP11 prolonged the tumor response to radioimmunotherapy (TVDT = 53.3 ± 3.1 and 49.7 ± 5, respectively) as compared with radioimmunotherapy alone (TVDT = 42.3 ± 2.8, with significant difference only for the first combination, P = 0.03 and 0.12, respectively).
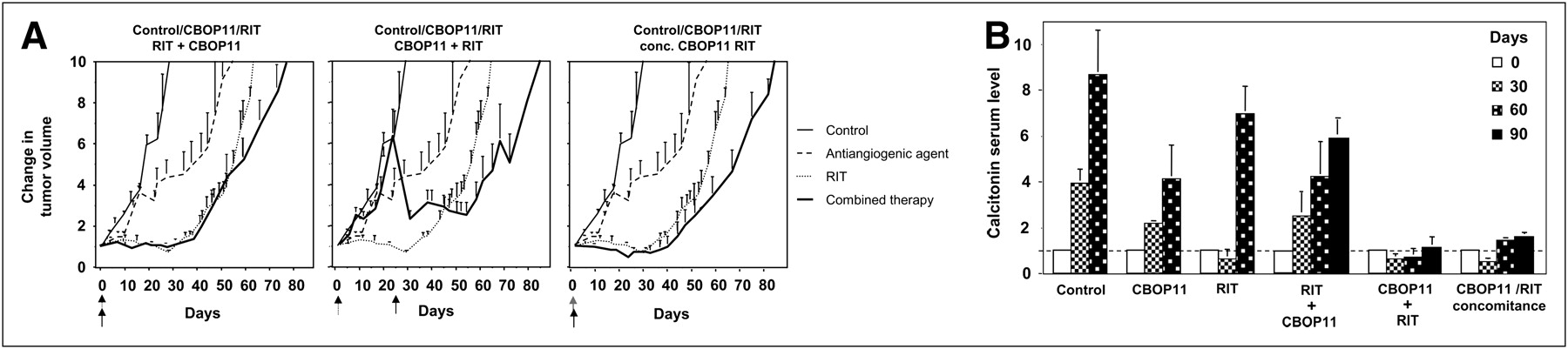
Efficacy of combination of CBOP11 and 131I-F6 radioimmunotherapy. (A) Changes in TT tumor size in treated mice and controls. Graphs show relative tumor volume (ratio of tumor volume to initial size before treatment) as function of time. Tumor volume in control group and group treated by radioimmunotherapy alone are shown in background in gray for comparison with combined therapy. Arrows show day of radioimmunotherapy injection. (B) Changes in calcitonin concentration (pg/mL) in treated mice and controls. Graphs show relative calcitonin concentration (ratio of calcitonin concentration to initial concentration before treatment) as function of time. Conc = concomitance; RIT = radioimmunotherapy.
Efficacy of Combination of Antiangiogenic Treatment and 131I-F6 on Large Tumors
Figures 4A and 4B show the growth curves and change in calcitonin levels of TT large tumors (>300 mm3), respectively. Day 0 represents the day of radioimmunotherapy administration. Pretreatment by CBOP11 or thalidomide sensitized large tumor to radioimmunotherapy. TVDT of large tumors untreated or treated by radioimmunotherapy were, respectively, 12.2 ± 6.37 and 25.5 ± 6.13. The value was significantly increased when radioimmunotherapy followed thalidomide (57.66 ± 10.6) and CBOP11 (59.4 ± 2.51) (P < 0.01 vs. radioimmunotherapy). Change in calcitonin levels confirmed morphologic tumor response. Ratios at day 60 were 3.75 ± 1.1 in the control group, 4.80 ± 1.15 in the group treated by radioimmunotherapy, 1.10 ± 0.30 in the group pretreated by thalidomide, and 1.85 ± 0.20 in the group pretreated by CBOP11.

Efficacy of combination of antiangiogenic treatment and 131I-F6 radioimmunotherapy on large tumors. (A) Changes in TT tumor size in treated mice and controls. Graphs show relative tumor volume (ratio of tumor volume to initial size before radioimmunotherapy) as function of time. (B) Changes in calcitonin concentration (pg/mL) in treated mice and controls. Graphs show relative calcitonin concentration (ratio of calcitonin concentration to initial concentration before radioimmunotherapy) as function of time. In A (arrow) and B, day 0 represents day of radioimmunotherapy administration. RIT = radioimmunotherapy; Thali = thalidomide.
Biodistribution Study
Tumor uptake was, respectively, 4.5 ± 0.6 %ID/g and 2.7 ± 1.1 %ID/g at 24 and 72 h after the injection of 125I-F6 without pretreatment by thalidomide and, respectively, 8.7 ± 1.3 %ID/g and 2.9 ± 0.7 %ID/g at 24 and 72 h after the injection of 125I-F6 with pretreatment by thalidomide. In the group injected with 125I-F6 alone, uptake for tumor-to-blood, -liver, and -kidney ratios were, respectively, 1.3 ± 0.3, 7.4 ± 3.2 and 4.4 ± 2.0 at 24 h and, respectively, 7.4 ± 2.1, 36.9 ± 7.5 and 24.7 ± 4.4 at 72 h. In the group pretreated by thalidomide, uptake for tumor-to-blood, -liver, and -kidney ratios were, respectively, 2.2 ± 0.1, 11.9 ± 0.9 and 7.5 ± 1.1 at 24 h and, respectively, 10.3 ± 1.7, 34.3 ± 4.5 and 29.8 ± 3.1 at 72 h.
Histologic Study
Tumor proliferation was microscopically comparable in the different samples obtained from growing tumors, consisting of a dense growth of large cells with a high nucleocytoplasmic ratio. The large nuclei displayed regular borders, fine chromatin, and small nucleoli. Proliferation took the form of rows and lobules separated by a thin fibrovascular stroma. Control tumor obtained from untreated mice was characterized by the presence of 5%−20% of necrosis. MIB-1 labeled 40%−50% of nuclei, and 100% of the cells expressed CEA in all assessed treated tumors.
After radioimmunotherapy, tumor necrosis was evaluated at 10% of tumor at day 15, 40%−50% at day 30, and 20% at days 45 and more than 60. So, the maximal value was observed at day 30. The values were not higher than the control tumor at the other days. After CBOP11, maximal necrosis was observed at day 15 with 40% of tumor and decreased at day 30 (30%), t day 45 (5%), and at more than 60 d (Supplemental Fig. 3). After radioimmunotherapy–CBOP11 concomitant treatment, large necrosis was prolonged to day 45 (40%), suggesting a prolonged efficacy of the combined treatment.
A direct impact on tumor development can explain better the tumor control by antiangiogenic drugs before the radioimmunotherapy protocol. Vasculature was detected by the clone on paraffin sections. As compared with untreated tumor, vasculature regression was estimated at 20% 15 d after treatment either by CBOP11 or radioimmunotherapy (Fig. 5). Concomitant treatment improved vasculature regression, which was estimated at 70% at day 15.

von Willebrand factor (VWF) immunostaining of TT xenograft treated by CBOP11. Hybridization with anti-VWF polyclonal antibody shows vasculature as function of treatment by radioimmunotherapy or CBOP11. (×200; windows, ×400). Arrows showed different endothelial cells stained in brown by biotin-labeled immunoperoxidase.
DISCUSSION
Angiogenesis is a complex and coordinated process, requiring several signaling steps. VEGFs and their receptors are key molecules in the regulation of vessel growth (22). Thalidomide is postulated to have antiangiogenic activity through its ability to interfere with the VEGF and basic fibroblast growth factor pathways (19,23,24). Thalidomide induces a regulation of VEGF receptors mediated by ceramides and antagonized by sphingosine-1-phosphate (22). CBOP11 encompasses residues 79–93 of VEGF, which are involved in the interaction with VEGF receptor-2 (20). CBOP11 inhibits VEGF binding to endothelial cells, endothelial cell proliferation, migration, and signaling induced by VEGF.
The present study established the benefits of the combination of radioimmunotherapy with antiangiogenic agents in MTC. The 2 antiangiogenic agents thalidomide and CBOP11 sensitized tumors to radioimmunotherapy when drugs were administered before or in concomitance with radioimmunotherapy. Surprisingly, antiangiogenic therapy improved the effect of radioimmunotherapy on large tumors. Moreover, although the combination of radioimmunotherapy with antiangiogenic agents induced a prolonged biologic response, with stabilization of calcitonin secretion, a recurrence of tumor growth was observed. Despite no clear explanation, this observation may be understood by the relapse of less differentiated cells, or because thalidomide and radioimmunotherapy affect the tumor microenvironment (such as hypoxia or acidic area), which may influence in return the calcitonin secretion.
Benefits from associating radioimmunotherapy with antiangiogenic agents were reported in human colon cancer xenografts (23–25). Thalidomide associated with the 131I-labeled antiglycoprotein mAb A7 more efficiently inhibited tumor growth than did the monotherapy (23). Immunohistochemistry revealed that microvessel number decreased within tumors treated with thalidomide and that combined therapy further reduced the microvessel number. Moreover, in an animal model of liver metastases, this group assessed antiangiogenic therapy with 2-methoxyestradiol and radioimmunotherapy using the same mAb (25). All nontreated mice died by 31 d after cell inoculation. Monotherapy comprising 2-methoxyestradiol resulted in slightly better survival. Radioimmunotherapy displayed a marked therapeutic effect. The combined regimen demonstrated superior survival in comparison to monotherapy. Another team assessed the cyclic Arg-Gly-Asp peptide cilengitide (EMD 121974), which targets the αvβ3 integrin receptor expressed on neovasculature, combined with systemic radioimmunotherapy in an aggressive human breast cancer model having mutant p53 and expressing bcl-2 (26). Cilengitide combined with radioimmunotherapy significantly increased therapeutic efficacy and apoptosis, when compared with single-modality therapy.
Neuroendocrine tumors are characterized by abundant vasculature and high levels of VEGF expression and are, therefore, potentially susceptible to therapeutic strategies targeting angiogenic pathways (27). Bevacizumab, a mAb-targeting VEGF, and SU11248, a small-molecule tyrosine kinase inhibitor targeting the VEGF receptor, have both recently been shown to have single-agent activity in neuroendocrine tumors (28,29). Moreover, thalidomide was associated with apparent disease stabilization in a small phase II study of patients with metastatic neuroendocrine tumors (30). Angiogenesis probably plays an important prognostic role in MTC. Indeed, a pathology study assessing 53 MTC patients observed that the number of newly formed vessels was significantly associated with poor prognosis (31). All patients who died of the disease showed a microvessel count higher than 30, which resulted in a high statistical difference, compared with living patients (P = 0.00098). Multiple logistic regression analysis showed that microvessel count together with pTNM (P = 0.026) were statistically significant prognostic factors. Moreover, encouraging evidence of antitumor activity has been reported in patients with metastatic hereditary MTC using vandetanib, a multitargeted kinase inhibitor exhibiting potent activity against VEGF receptor-2 kinase insert domain-containing receptor and, to a lesser extent, epidermal growth factor receptor and RET kinase (32).
The clinical application of the combination of radioimmunotherapy and antiangiogenic therapy might be promising only if acceptable toxicity is observed. In addition to teratogenicity, thalidomide induces side effects including somnolence, constipation, skin rashes, orthostatic hypotension, nausea, neuropathy, and neutropenia (33). The clinical toxicity of CBOP11 is unknown, but our results revealed CBOP11-induced leukopenia. Toxicity of radioimmunotherapy is essentially hematologic too. No additional toxicity was observed in the association cilengitide–radioimmunotherapy (26). Similar to the results reported by Kinuya et al., our study showed that the combined regimens, as compared with radioimmunotherapy alone, delayed recovery of the leukocyte concentration (25). Interestingly, hematologic toxicity was higher in the group showing an increased antitumor effect. Indeed, groups showing tumor efficacy were associated with leukopenia and increase of platelets. The combined therapy may target hematologic stem cells such as endothelial progenitors involved in hematopoiesis and tumor development. Platelet increase may repair vessel damage induced by antiangiogenic agents and ionizing radiation.
As reported for combination of radioimmunotherapy and chemotherapy (34), the timing of association appeared determinant. Our study demonstrated no benefit of antiangiogenic therapy given after radioimmunotherapy. Burke et al. already showed a significant decrease of microvessel density after radioimmunotherapy, compared with untreated mice (26). The fact that radioimmunotherapy modulated tumor vasculature might explain why therapy with antiangiogenic agents before radioimmunotherapy was superior to that after radioimmunotherapy. In our experiments, the biodistribution study showed that a pretreatment by thalidomide increased radioactivity tumor uptake, allowing increased tumor absorbed dose. However, tumor uptake was increased only at the 24-h time point, probably reflecting the enhanced tumor perfusion. As previously explained with external radiotherapy, antiangiogenic agents normalize tumor vascularization, improve perfusion, reduce hypoxia, and increase radiosensitivity (35). Despite a lack of specific prolonged high tumor uptake, increase of radioimmunotherapy efficacy by antiangiogenic agents might be explained by the enhanced tumor cell radiosensitivity. Moreover, VEGF and basic fibroblast growth factor are cytokines known to optimize the survival of endothelial cells under stress exposure. By inhibiting these endothelial survival pathways, antiangiogenic agents could sensitize endothelial cells to radiation delivered by radioimmunotherapy, increase death of endothelial cells, and reduce tumor growth (36).
CONCLUSION
Pretreatment with thalidomide and CBOP11 improved radioimmunotherapy efficacy in MTC, with acceptable toxicity. Antiangiogenic therapy restored the effect of radioimmunotherapy on large tumors. Future investigations will be performed to understand how antiangiogenic agents enhance radioimmunotherapy efficacy.
Acknowledgments
We thank the ARC for financial support.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 14, 2009.
- Accepted for publication December 23, 2009.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.