


Abstract
Serotonin is a modulatory neurotransmitter in the human brain that regulates mood, anger, reward, aggression, and appetite and plays a central role in brain development. These effects are mediated through the interaction of serotonin with at least 15 different receptor molecules. Through the development and careful characterization of novel radiotracers, we have been able to visualize and quantify in vivo many of the key molecular sites—including serotonin receptors, reuptake transporters, and enzymes—responsible for serotonin metabolism. The clinical goals of serotonin imaging are to aid in determining the pathophysiology of brain disorders, to determine novel therapeutic strategies, to predict treatment, to estimate risk, and to determine individualized dosing strategies. Despite the contradictory results of early studies, the field as a whole has made significant progress on nearly all of these fronts, and advances in methodology suggest paths toward coherence. Through concerted, directed, and cooperative efforts, the routine use of serotonin imaging in the clinic will most likely be achieved in the next decade.
Serotonin is a modulatory neurotransmitter in the human brain that regulates mood, anger, reward, aggression, and appetite and plays a central role in brain development (1). Discovered in 1948, serotonin has subsequently been found to act on 15 receptors grouped into 7 families distributed throughout the body (2). It acts on a variety of cognitive and emotional processes and has been implicated in a variety of neurologic and psychiatric disorders including Alzheimer's disease, epilepsy, major depression, bipolar disorder, and schizophrenia (3).
MOLECULAR IMAGING WITH PET
Recent years have seen a dramatic expansion of the tools available to study the molecular basis of neuropsychiatric disorders. Early studies mapped the electrical activity of the cortex using multiple electrodes across the scalp. Blood flow and then glucose metabolism studies using a variety of PET and SPECT tracers followed. These experiments helped localize pathophysiologic brain regions in disorders. Since then, several laboratories have been engaged in the creation and dissemination of highly specific and selective radioactively labeled molecules. The most commonly used radioactive atoms that are attached to these tracer molecules are 11C and 18F. 11C has a short half-life of approximately 20 min, which allows multiple studies in the same day. 18F has a longer half-life of nearly 2 h, allowing shipment of tracers over considerable distances to imaging centers that do not have a cyclotron for producing the radiolabels.
Developing suitable radiotracers for use in human studies is a time-consuming and error-prone process. After a target has been determined, a lead compound must be identified that has high affinity and selectivity for the target and is amenable to having a synthetic production scheme that allows for the rapid incorporation of the radioactive atom. The radiotracer must be able to pass the blood–brain barrier and have both sufficient affinity for the target and a suitable number of target sites in large enough areas of the brain to be detectable. Ideally, the radiotracer is not a substrate for p-glycoproteins, endogenous molecules that actively remove the radiotracer and prevent significant accumulation of tracer in the brain. The radiotracer should have measurable nonspecific binding but also a high ratio of specific binding to nonspecific binding. Specific binding refers to the labeling of the target of interest with the radiotracer. Nonspecific binding describes the binding of the tracer to everything in the field of view that is not the target, such as plasma membranes and other proteins. The radiotracer should not have a metabolic pathway resulting in radioactively labeled metabolites that have affinity for the target and that cross the blood–brain barrier. The radiotracer should also be safe to use in rodents, nonhuman primates, and humans and must have a biodistribution and dosimetry profile amenable to injection into human beings. The process of developing a radiotracer can therefore take years only to be foiled by the last step. The careful characterization of a tracer typically includes 4 steps. First, the reproducibility of binding of the compound must be determined by injecting the tracer on at least 2 occasions and quantifying uptake; acceptable reproducibility is approximately 10%. Second, the tracer must be determined to have stable and reproducible outcome measures that can be obtained within a scan duration of 2 h or less for 11C compounds. Third, the optimal modeling strategy for the tracer must be determined, and finally, the presence or absence of a suitable reference region (region of brain without the target) must be validated.
The last step is critical. If there is a region in the brain that is devoid of the target of interest, we can get an accurate measure of the amount of tracer that is nonspecifically bound. Specific binding then is calculated by taking the total binding in a region with the target of interest and subtracting the nonspecific binding, as we assume that all regions have the same degree of nonspecific binding. Currently, the only way to quantify nonspecific binding is by measuring the amount of nonmetabolized radiotracer in the blood. This measurement requires placement of an arterial line and subsequent analysis of multiple small aliquots of blood. If the reference region is invariant between a study population and a control population, then an arterial blood–derived input function is no longer needed and subsequent studies are much easier to perform and analyze. Most studies are done using reference region approaches, which require the following 3 assumptions. It is often inferred, first, that the differences between groups being compared or differences between pre- and posttreatment studies are due to changes in the total number of receptors and not due to differences in the nonspecifically bound tracer; second, that reference tissue methods mathematically return results comparable to those from arterial line modeling; and third, that there truly is no detectable specific binding in the reference region. There are several examples of violations of these assumptions in the literature, with effects ranging from minor to complete reversals of reported pathophysiologic findings.
Once developed and brought into human use, the radiotracer has to be carefully characterized and validated. Typically, the first studies are done with arterial blood samples drawn and analyzed for quantification of the tracer uptake into the brain. Using compartment models (4), we can calculate the binding potential as the uptake of the tracer in the brain relative to the concentration of the tracer in blood (requiring an arterial line, BPF = Bavail/KD) or relative to binding in a region of the brain that lacks specific binding (BPND = fNDBPF). Bavail is the total number of available target sites, 1/KD is the affinity of the radiotracer to the target, and fND is the free radiotracer in the brain (5).
CURRENT SEROTONIN IMAGING IN NEUROPSYCHIATRIC CONDITIONS
A comprehensive list of all the radioligands that have been through some or all of these steps is beyond the scope of this article. However, within the serotonergic system, excellent radioligands are on the near horizon for several serotonin receptors: 5-hydroxytryptamine subtypes 1A, 2A, 1B, 4, 2C, and 6 (5-HT1A, 5-HT2A, 5-HT1B, 5-HT4, 5-HT2C, and 5-HT6, respectively). There are also several outstanding tracers for the serotonin transporter and the enzyme responsible for the breakdown of serotonin in the brain, monoamine oxidase inhibitor A.
Diagnosis
Although serotonin imaging has many potential clinical uses (Table 1), there are currently no psychiatric or neurologic diseases in which serotonin imaging is used for routine diagnosis. There are several possible reasons for this. First, the magnitude of differences between the study population and healthy control comparison groups is likely small. Second, in studies having statistically significant differences between groups, there may still be considerable overlap between groups, not allowing for a clear diagnostic cutoff. This large variability in binding within groups suggests that there are many biologic covariates of interest that we have not yet determined, such as sex, genetic polymorphisms, and epigenetic regulation. Third, findings of serotonergic abnormalities are often not replicated between groups (3), as there are methodologic differences in choice of ligands, modeling methods, reference regions, study populations, and other variables. Fourth, our imaging technology, both image acquisition and analysis, is rapidly improving; currently, there is no universally accepted technology or methodology.
Overview of Potential Clinical Uses of Serotonin Imaging
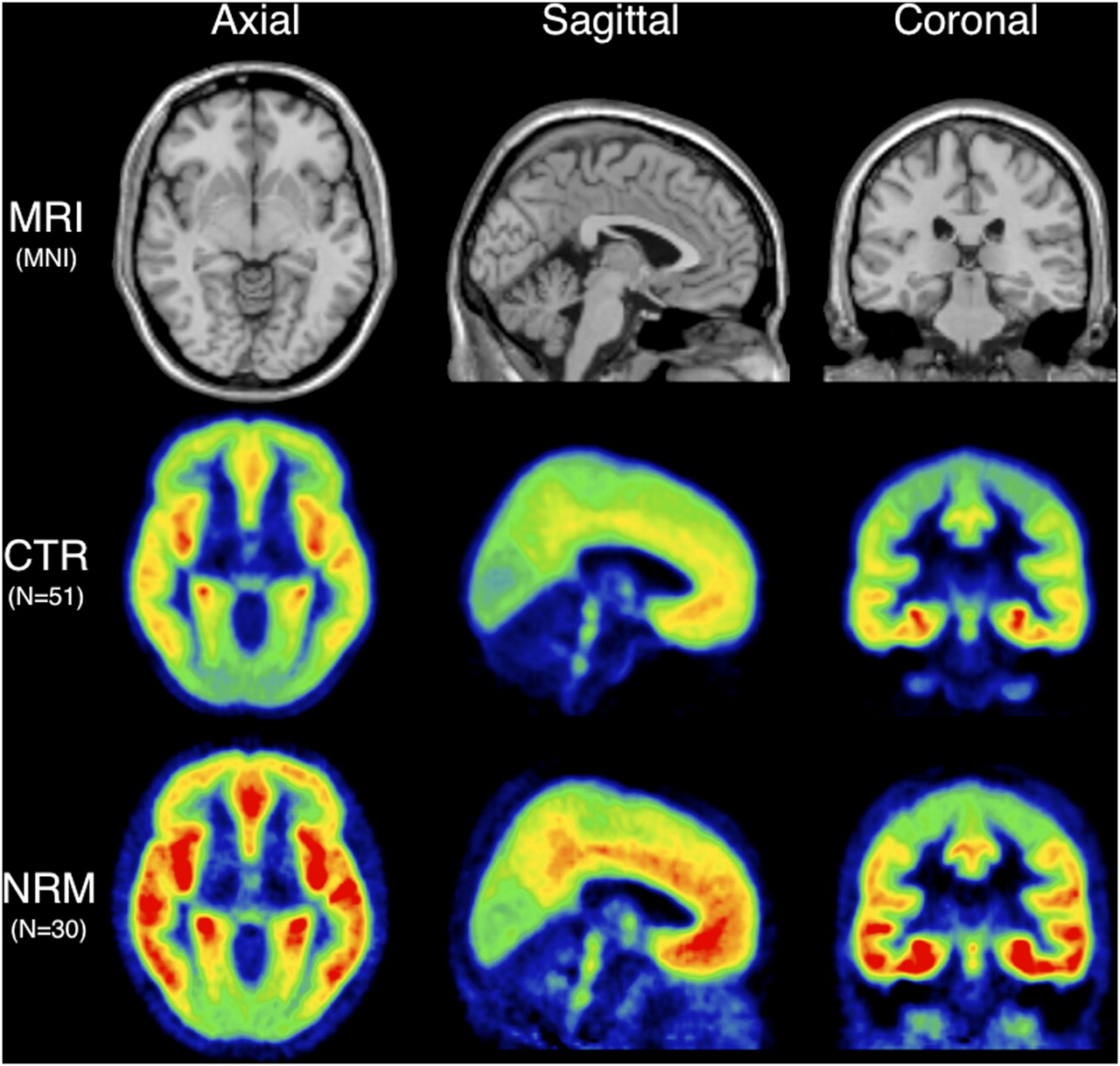
An example of evolving methodology is the 5-HT1A receptor in major depressive disorder. Several years ago, Pike et al. developed a highly selective and specific 5-HT1A radioligand that was lauded for its extremely low nonspecific binding, 11C-WAY-100635 (6). As there are virtually no 5-HT1A receptors in the cerebellum, groups assumed that using a reference tissue method with the cerebellum as the reference region would be justified. Early reports suggested that there was widespread reduction of 5-HT1A receptors in depressed subjects, compared with controls (7,8). Subsequently, it was shown that the few 5-HT1A receptors in certain regions of the cerebellum were quantifiable. If studies are done not with the reference region approaches, which express binding relative to binding in the reference region, but with full quantification, which expresses binding relative to plasma measures, the depressed subjects in fact have higher 5-HT1A binding than do controls (Fig. 1) (9). This is due to small but statistically significant differences in specific binding in the reference region. This finding has now been replicated in a novel cohort (10). Additionally, the findings of other groups can be replicated if certain assumptions regarding reference region and outcome measure are made (9).
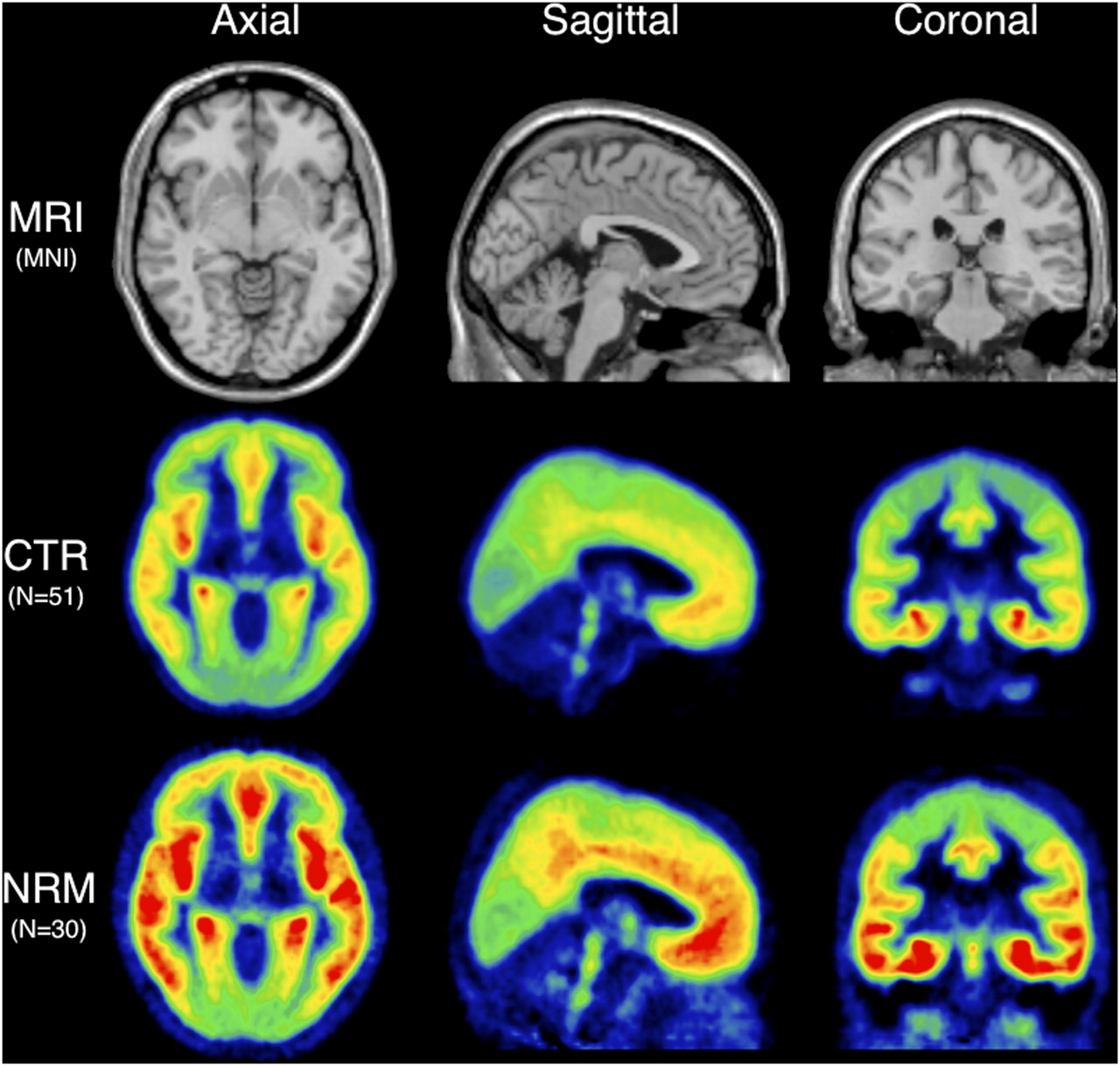
Example of using 5-HT1A imaging for diagnosis. Not recently medicated (NRM) depressed subjects show much higher 5-HT1A binding potential than do healthy volunteers (CTR).
Perhaps one of the largest differences ever described in depression is the 34% higher expression of monoamine oxidase A in several brain regions of depressed subjects (11), a finding that has recently been replicated (12). Monoamine oxidase A is the enzyme responsible for the degradation of monoamines such as serotonin and a target of a large class of antidepressants. With large differences such as this, we will soon be able to use this measure as a diagnostic test.
For many neurologic and psychiatric disorders, there are tremendous barriers toward treatment, namely stigma. We believe that by demonstrating that these illnesses are not choices, but biologic medical illnesses just like diabetes and hypertension, we will reduce the barriers.
Treatment Planning
In a naturalistic study, higher 5-HT1A binding was associated with a lack of response to antidepressant treatment (13). If this finding is replicated in a prospective study, it suggests that PET could be used to help determine whether subjects are likely to respond to medication or should seek alternative treatments such as psychotherapy, electroconvulsive therapy, or transcranial magnetic stimulation. Since there is virtually nothing to guide a physician in selecting the first line of antidepressant therapy and most medications require at least 4–6 wk to determine efficacy and often require a trial of a second medication, imaging that predicts the most efficacious treatment modality for an individual would have a significant impact on the treatment of major depressive disorder.
Imaging studies in temporal lobe epilepsy, using an 18F-fluorinated 5-HT1A antagonist radiotracer, have shown that decreased 5-HT1A binding in the hippocampus, amygdala, and temporal pole predicted a good response to anterior temporal lobectomy (14). Given the risk and side effects of such an invasive procedure, the ramifications of this imaging capacity are profound and extremely encouraging.
Similar to the 5-HT1A system, higher 5-HT2A seems to predict poorer response to treatment (15). Using 18F-fluoroethylspiperone, a nonselective 5-HT2A and dopamine D2 receptor antagonist, depressed subjects with higher binding were less likely to respond to treatment with paroxetine.
Therapeutic Drug Levels
Perhaps one of the most valuable current uses of PET technology is determining the in vivo brain occupancy of a putative pharmaceutical at the target of interest, that is, when developing a pharmaceutical treatment for depression. Literature suggests (16) that roughly 80% of the serotonin transporters have to be occupied by an antidepressant in vivo in humans to be useful. If the maximum tolerated dose is known, then a very small PET study (∼10 subjects) can determine whether the desired occupancy is achieved at the tolerable dose. If so, then we can proceed to full clinical trials. If not, we have saved millions of dollars and a failed trial for subjects who have serious debilitation and life-threatening illness. Currently, there is no other method available for the in vivo determination of receptor occupancy in humans; it is unique to molecular imaging.
Clozapine is one of the most successful treatments for schizophrenia to date. Unlike other antipsychotics, its blockade of dopamine receptors is modest. It has a broad spectrum of activity including antagonism of most 5-HT2A receptors (17). In designing pharmaceuticals to maximize the beneficial effects of clozapine while removing the serious side effects such as agranulocytosis, one might design other antagonists with high 5-HT2A antagonism. Surprisingly, occupancy imaging of a newer atypical antipsychotic showed it possessed only a moderate degree of 5-HT2A antagonism (18).
Although the widespread use of PET as a clinical tool to determine in vivo brain occupancy for individual patients is unlikely, it might be used to establish a plasma level and brain occupancy relationship. If this were demonstrated, then clinicians would be able to estimate brain occupancy based on a simple blood sample.
Suicide Risk Assessment
Currently, there are no in vivo PET serotonergic markers associated with increased risk for suicide; this is a major deficiency. A tremendous amount of literature, including postmortem 5-HT receptor binding studies, has associated suicide risk with differences in the serotonergic system. Greater investigation in this area is clearly needed, as this is an urgent public health problem.
FUTURE DIRECTIONS
Diagnosis
To resolve the many discrepant studies between groups, there needs to be a consensus on how initial studies in patient populations should be performed. Although costly and somewhat burdensome, large multicenter studies with arterial blood sampling should be performed initially. This way, all outcome measures are available. All practitioners and researchers alike ultimately want to extend imaging technology to the largest group of patients with the least risk and discomfort. With a full dataset, we can carefully evaluate exactly which steps can be sacrificed without compromising the full capacity of the tracer. Multicenter studies are also essential for sufficient sample size. As we learn progressively more about genetic and epigenetic modulation of protein expression in the brain, we will need large sample sizes to see the effects of the various polymorphisms in a statistically robust way. In addition, several groups are working on mathematic techniques of recreating the arterial input function using just the brain data. With large comprehensive datasets, these methods can be put to the test and used in future studies.
Treatment Planning
The applications of this technology are not only in diagnosing subjects but also in planning treatment. Whether it helps when choosing one class of medication over another or even medication versus therapy, this is a need that radiotracer imaging can fill. To achieve this, we need to do blinded, prospective treatment studies in subjects who have pretreatment imaging. However, for this technology to be widely disseminated, we need to be able to have fluorinated tracers that can be distributed widely and methodology that can be easily applied or processed at a central location. Advances in Alzheimer's disease diagnosis provide an excellent example of the fusion of both these tracks. Although early studies were performed with 11C-Pittsburgh compound B, several groups have developed fluorinated compounds. Also, there are now fully automated methods for the analysis and diagnosis based on 11C-Pittsburgh compound B images (19).
CONCLUSION
Molecular imaging of the serotonergic system is not yet in use in clinical practice. Several issues have to be addressed first. It is reasonable to expect significant advances in the next decade. The advances that will be necessary for the widespread application of molecular imaging include careful characterization of the new radiotracers, careful application of modeling techniques, the use of PET in large multicenter trials, the standardization and automation of image-processing techniques, and the development of statistical algorithms that can use voxels as predictors of response to treatment for risk stratification. Several groups are working intensely in all of these areas, and we have every reason to be hopeful that our current research tools will soon be clinical tools.
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication February 10, 2010.
- Accepted for publication May 27, 2010.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.