


Abstract
Postmortem binding studies have established that the concentration of α4β2-nicotinic acetylcholine receptors (α4β2-nAChR) is reduced in advanced Alzheimer disease (AD). However, the status of this receptor in mild or prodromal AD has remained the subject of controversy. Methods: We compared α4β2-nAChR availability in 8 brain regions of living human subjects who had AD and mild cognitive impairment (MCI) with that in age-matched healthy control subjects by using the ligand 123I-5-IA-85380 (123I-5-IA) and SPECT. All subjects (n = 32) were nonsmokers; they were administered 123I-5-IA as a bolus plus a constant infusion and imaged 6–8 h later under equilibrium conditions. The effect of diagnosis on regional α4β2-nAChR availability (regional brain activity/total parent concentration in plasma, proportional to the binding potential) was analyzed using multivariate analysis of covariance, controlling for the effects of age and sex. Results: Despite a significant overall effect of diagnostic group on mean α4β2-nAChR availability, univariate analyses revealed no group differences for any brain region analyzed. An exploratory analysis of the relationship between regional α4β2-nAChR availability and neuropsychologic variables yielded several plausible correlations. However, after Bonferroni adjustment, only the correlation between the anterior cingulate and the Trail Making Test, Part B, in the healthy control subjects remained significant. Conclusion: These results are consistent with several postmortem and in vivo studies suggesting the preservation of nAChRs during the prodromal and early stages of AD. They support the interpretation that nAChR and other cholinergic reductions in AD are late-stage phenomena.
The cholinergic hypothesis of Alzheimer disease (AD) holds that the degeneration of neurons in the basal forebrain and the associated loss of cholinergic neurotransmission in the cerebral cortex and hippocampus contribute significantly to cognitive deterioration in AD (1). Numerous studies have demonstrated reductions in the expression of cholinergic markers in postmortem AD brains, including choline acetyltransferase (2–4), acetylcholinesterase (3), and both muscarinic (5) and nicotinic (2,6–11) acetylcholine receptors (nAChRs). These decrements have been shown to correlate broadly with the cognitive impairments observed in AD when the full severity range is considered (3,4,7).
Of the various cholinergic markers that have been investigated in AD, nAChRs have been among the most consistently implicated. Postmortem binding studies have indicated that α4β2-nAChR is the nicotinic receptor subtype that is most profoundly affected by AD (reviewed in (9)), with reductions of up to 50% in the neocortex, entorhinal cortex, and hippocampus (2,6–11). Decreases in regional nAChR expression have been shown to correlate with declines in cognitive function (7). Evidence has accumulated that cholinergic changes, including reductions in nAChR (7,11), may be a late-stage phenomenon in AD (3,4,12). However, it remains uncertain whether the nAChR deficits occur at an early or a preclinical stage of the disease.
Although a wealth of literature supports the loss of nicotinic function in AD, a comparative paucity of research has addressed the role of nAChRs in the prodromal state of amnestic mild cognitive impairment (MCI). Current conceptions of MCI suggest that it represents a transitional stage between the cognitive changes associated with normal aging and the earliest presentations of probable AD (13). Longitudinal studies have indicated that individuals with MCI decline to AD at a rate of 12% per year and at a rate of up to 80% after 6 y of follow-up (13). If MCI represents prodromal AD, then nAChR abnormalities in MCI could provide an important biomarker at the earliest stage of the disease.
With the advent of functional brain imaging methodologies—specifically, PET and SPECT—it has become possible to study the effects of AD and MCI on nAChRs in living subjects. Initial attempts to image the nAChR in AD with 11C-nicotine demonstrated significant reductions in nAChR (14,15), which correlated with impaired cognitive function (16). However, studies with 11C-nicotine were hampered by high nonspecific binding, rapid metabolism and washout from the brain, and dependence on regional cerebral blood flow.
The search for new nicotinic ligands yielded 3-[2(S)-2-azetidinylmethoxy]pyridine (A-85380), an α4β2-specific compound (17), which was subsequently radiolabeled with 18F (18) and 123I (19) for in vivo nAChR imaging. The resulting ligand, 123I-5-IA-85380 (123I-5-IA), exhibited many properties necessary for the in vivo imaging of α4β2-nAChR with SPECT, including high affinity (dissociation constant, 11 pM), rapid entry into the brain, low nonspecific binding, and minimal toxicity (20).
We demonstrated the feasibility and reproducibility of equilibrium imaging of α4β2-nAChRs by using a paradigm consisting of a bolus plus a constant infusion of 123I-5-IA (21). This paradigm is ideally suited for the 13.2-h half-life of 123I and permits simpler modeling of tracers that lack a suitable reference region (devoid of receptors). We also recently reported significant reductions in α4β2-nAChR in various brain regions across the normal life span (22,23). Several in vivo studies have thus far used A-85380 derivatives to investigate α4β2-nAChR binding in AD or MCI (24–27), with mixed results (reviewed in the “Discussion” section).
The primary aim of the present study was to compare α4β2-nAChR availability in patients who had probable AD and MCI with that in age-matched healthy control (HC) subjects by use of 123I-5-IA and SPECT. A secondary, exploratory objective was to determine whether regional α4β2-nAChR availability was related to neuropsychologic function.
MATERIALS AND METHODS
Human Subjects
The study sample consisted of 12 subjects with probable AD (age, 75.0 ± 9.0 y [mean ± SD]), 10 subjects with MCI (73.8 ± 6.0 y), and 10 age-matched HC subjects (73.8 ± 8.3 y). All subjects were of European American descent and were nonsmokers. On the basis of responses to a smoking history questionnaire, 18 of the 32 subjects were never-smokers (<100 lifetime cigarettes). Six subjects with AD, 5 subjects with MCI, and 3 subjects with HC were former smokers but had not smoked for ≥20 y. Urine cotinine levels were not determined. All female subjects were postmenopausal. The demographic and cognitive characteristics of the study participants are shown in Table 1.
Subject Characteristics
Screening Procedures and Neuropsychologic Assessment
Screening procedures included a medical history, physical and neurologic examinations, electrocardiography, serum chemistries, thyroid function studies, complete blood count, urinalysis, and urine toxicology screen. Subjects were also assessed with the Mini-Mental State Examination (MMSE) (28), NYU Paragraph (Guild Memory Test word paragraph) (29), Clinical Dementia Rating Scale (CDR) (30), and Cornell Scale for Depression in Dementia (CSDD) (31). Subjects were excluded for significant medical, psychiatric, or neurologic conditions that could contribute to cognitive impairment. No subject was taking psychotropic medications or drugs known to affect the brain's cholinergic system within 4 wk of screening. In particular, none of the subjects with AD was taking a cholinesterase inhibitor or memantine. Subjects were also excluded if they had a modified Hachinski Ischemic Score (32) of greater than 4 or a CSDD score of greater than 12.
Patients with AD were required to meet standard diagnostic criteria for probable AD (33) and to have a CDR score of ≥0.5 and an MMSE score of ≤26. Subjects with MCI were required to meet standard research diagnostic criteria for amnestic MCI (13), including performance on the NYU Paragraph that fell 1.5 SDs below the mean of age-matched and education-adjusted normative data. They were also required to have a CDR score of 0.5 and an MMSE score of ≥24. HC subjects were required to have memory scores within the reference range for age, a CDR score of 0, and an MMSE score of >26. All subjects (or their responsible next of kin) signed informed consent forms approved by the Yale University School of Medicine Human Investigation Committee.
An array of neuropsychologic tests was chosen to assess a broad range of cognitive functions, including attention, memory, executive function, processing speed, language, and verbal and semantic fluencies. On the day of the SPECT scan, the subjects underwent a comprehensive neuropsychologic evaluation that included the tests shown in Tables 1 and 2. The reading subtest of the Wide-Range Achievement Test, third edition, and the Stroop Test could not be administered to one AD subject because of reading impairment.
Neuropsychologic Measures
123I-5-IA SPECT Studies
Subjects were imaged with SPECT and 123I-5-IA administered as a bolus plus a constant infusion as described previously (21). In brief, subjects received a potassium iodide (0.8 g)–saturated solution before radiotracer administration. 123I-5-IA was synthesized as previously described (34) and administered as a bolus (159 ± 11 MBq) and a continuous infusion (22 ± 0 MBq/h) at a bolus-to-infusion ratio of 7.0 h for 8 h. The total administered dose was 363 ± 26 MBq. When this paradigm is used, 123I-5-IA reaches equilibrium binding in the brain by 6–8 h (21).
Three consecutive 30-min emission scans and one 15-min simultaneous transmission and emission protocol scan were acquired between 6 and 8 h with a Picker PRISM 3000XP (n = 29) or 3000XP2 (n = 3) camera equipped with a low-energy, ultra-high-resolution fanbeam collimator (photopeak window, 159 keV ± 10%; matrix, 128 × 128). The difference in sensitivity between the 2 cameras has been found to be less than 2.5% (4 MBq of the 123I source at the center of rotation of each camera). To control for day-to-day variations in camera sensitivity, we measured a 57Co-distributed source with each experiment. The axial resolution (full width at half maximum) was 12.2 mm, measured with a 123I line source in water in a cylindric phantom. Plasma samples were collected before radiotracer injection and at the beginning and end of emission scans to quantify the total parent concentration and the free fraction (percentage) of the parent tracer in plasma (fP) (34).
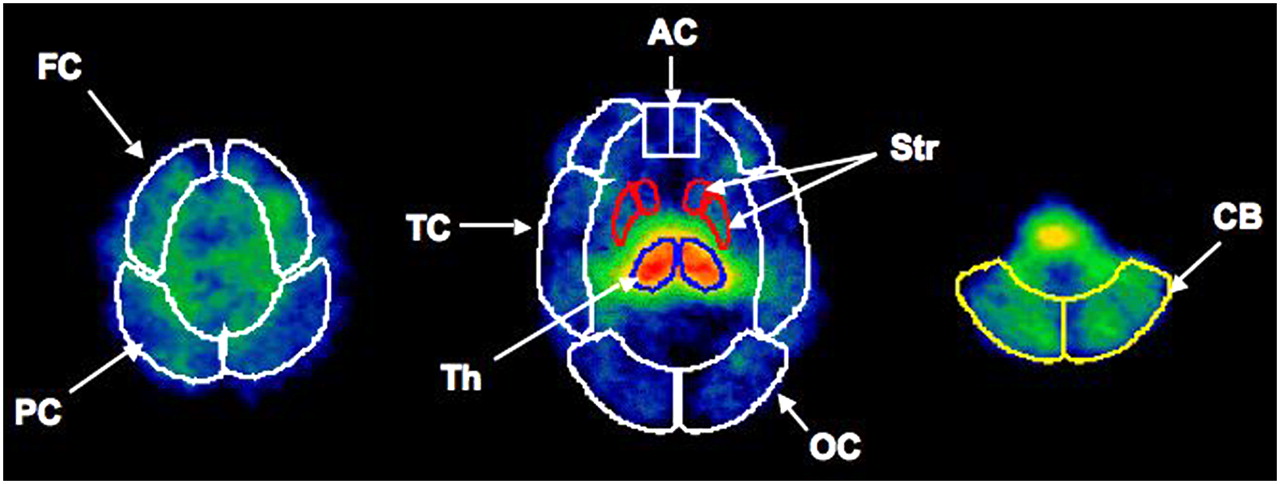
SPECT emission images were reconstructed and analyzed as previously described, including nonuniform attenuation correction (21,23). Sagittal MR images were obtained with a 1.5-T GE Healthcare Signa camera with spoiled gradient recalled echo sequences (echo time, 5 ms; repetition time, 24 ms; number of excitations, 1; matrix, 256 × 192; field of view, 34 cm). The coregistered and reoriented MR image was used to guide the placement of standardized 2-dimensional region-of-interest templates (Fig. 1) (21). No attempt was made to correct for partial-volume effects. The mean from 2 raters who conducted image analyses is reported. Both raters were unaware of subject identity and diagnostic group.

Placement of 2-dimensional standardized regions of interest on 3 representative transverse images of 123I-5-IA uptake. AC = anterior cingulate; CB = cerebellum; FC = frontal cortex; OC = occipital cortex; PC = parietal cortex; Str = striatum; TC = temporal cortex; Th = thalamus.
Statistical Analyses
On the basis of previous postmortem studies (9,35,36), the a priori hypothesis was that α4β2-nAChR availability would be decreased broadly in neocortical brain regions—particularly temporal and frontal but also parietal and occipital cortices—in subjects with AD compared with HC subjects, with receptor availability in subjects with MCI being between those in subjects with AD and HC subjects. Nicotinic receptor–binding studies in the postmortem AD brain have generally shown less consistent findings in subcortical areas, such as the striatum and thalamus, with no changes in the cerebellum (9,35,36). We also conducted an exploratory analysis to determine whether regional α4β2-nAChR availability was correlated with neuropsychologic measures within each subject group.
We previously validated 2 equilibrium outcome measures for 123I-5-IA (21): VT (VT′ in our earlier publications (21–23,37)) is the volume of distribution, which is calculated as the ratio of the regional brain concentration to the total plasma parent concentration; VT/fP (VT in our earlier publications (21–23,37)) is the tissue equilibrium volume of distribution, which is equal to the sum of V2 (nondisplaceable) and V3 (receptor bound) and which is calculated as the ratio of the regional brain concentration to the free plasma parent concentration (total plasma parent concentration × fP). We analyzed VT as the primary outcome measure in the present study because of its greater test–retest reliability. However, we also performed a confirmatory analysis of VT/fP, which has the advantage of not assuming intersubject uniformity of fP.
The effect of diagnosis (HC, MCI, and AD) on regional α4β2-nAChR availability (VT and VT/fP, average values at 6–8 h) in 8 brain regions was determined by multivariate analysis of covariance (MANCOVA), controlling for age and sex. Age was included in the model because α4β2-nAChR availability has been shown to decline significantly with age in the same 8 brain regions (23). The Pearson r was used to examine the relationship between regional α4β2-nAChR availability (VT) and neuropsychologic measures. Given the exploratory nature of this analysis, no correction for multiple comparisons was applied. However, the effect of Bonferroni adjustment was considered. Group differences in neuropsychologic measures were analyzed by analysis of covariance (ANCOVA), with age, sex, and education entered into the model as covariates. Group differences in demographic and cognitive characteristics were analyzed by ANOVA or the χ2 test. All statistical analyses were performed with SPSS (SPSS Inc.) and included 2-tailed tests of significance.
RESULTS
Subject Characteristics
Table 1 summarizes the characteristics of each diagnostic group with regard to demographics and cognitive function. HC subjects, subjects with MCI, and subjects with AD did not differ with respect to age (F2,29 = 0.23; P = 0.79), sex (χ2 = 2.13; P = 0.34), education (F2,29 = 2.36; P = 0.11), or Wide-Range Achievement Test, third edition, reading subtest standard score (F2,28 = 1.40; P = 0.26) as an estimate of premorbid intelligence. In contrast, in measures of global function and cognitive performance, the 3 groups differed significantly, as shown in Table 1. Impairments in subjects with AD spanned a range of mild to moderate severity, as evidenced by MMSE (20.4 ± 5.9) and CDR (1.00 ± 0.52) scores. However, the majority of impairments were of mild (CDR score, 1; n = 6) or very mild (CDR score, 0.5; n = 4) severity. Although no subject had clinically important depressive symptoms, there was a significant effect of group on the CSDD score (F2,29 = 4.49; P = 0.020), in that patients with AD scored nominally higher (2.3 ± 2.9) than HC subjects (0.0 ± 0.0).
Table 2 shows the results obtained from the larger neuropsychologic battery, organized to reflect the various cognitive domains assessed. Group comparisons of neuropsychologic measures were done with raw scores and ANCOVA analyses, controlling for age, sex, and education. All tests in the battery demonstrated significant effects of diagnostic group, with arithmetic differences generally following the pattern of HC > MCI > AD; however, the statistical significance of post hoc pairwise comparisons varied considerably, as shown in Table 2. The results of these analyses broadly supported the previous construct of amnestic MCI (13) as involving objective memory impairment but normal general cognitive function. All 4 memory measures revealed significant differences between subjects with MCI and HC subjects, but only 1 of 8 nonmemory tests (category fluency) revealed such a difference.
Effect of AD and MCI on Regional α4β2-nAChR Availability
The primary outcome measure (VT) assumed that fP does not vary as a function of diagnostic group (HC, MCI, and AD). Indeed, ANOVA analyses revealed no group differences in fP (HC, 33.3% ± 2.5%; MCI, 32.2% ± 5.4%; AD, 33.3% ± 4.2%; F2,29 = 0.12; P = 0.89), total plasma parent concentration (HC, 0.38 ± 0.10 kBq/mL; MCI, 0.42 ± 0.10 kBq/mL; AD, 0.44 ± 0.13 kBq/mL; F = 0.44; P = 0.65), or free plasma parent concentration (F = 0.47; P = 0.63).
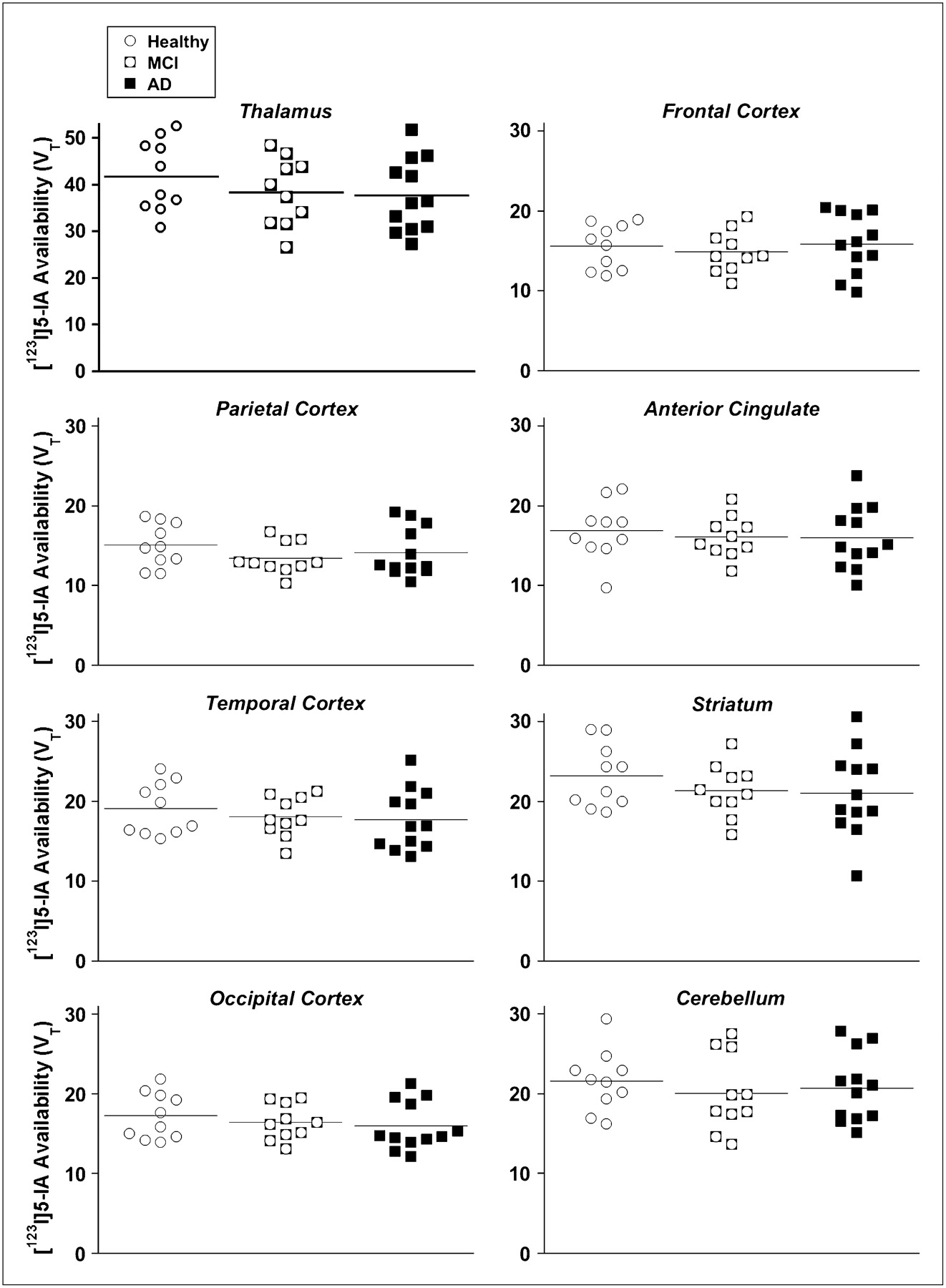
Mean values for regional α4β2-nAChR availability (VT) are shown in Table 3 and graphically depicted in Figure 2. MANCOVA results indicated a significant overall effect of diagnostic group on mean VT (Wilks Λ test: F16,40 = 2.25; P = 0.019). However, counter to the previously mentioned hypothesis, univariate analyses revealed no significant regional differences among the subject groups for any of the 8 regions, including the 4 neocortical regions. Neither age (F8,20 = 2.16; P = 0.078) nor sex (F8,20 = 0.62; P = 0.76) was significant in the MANCOVA model. In a confirmatory analysis of the alternate outcome measure (VT/fP), MANCOVA results again indicated a significant overall effect of diagnostic group on mean α4β2-nAChR availability (Wilks Λ test: F16,40 = 2.22; P = 0.021). However, univariate analyses again revealed no significant regional differences among the subject groups for any of the 8 regions (data not shown).
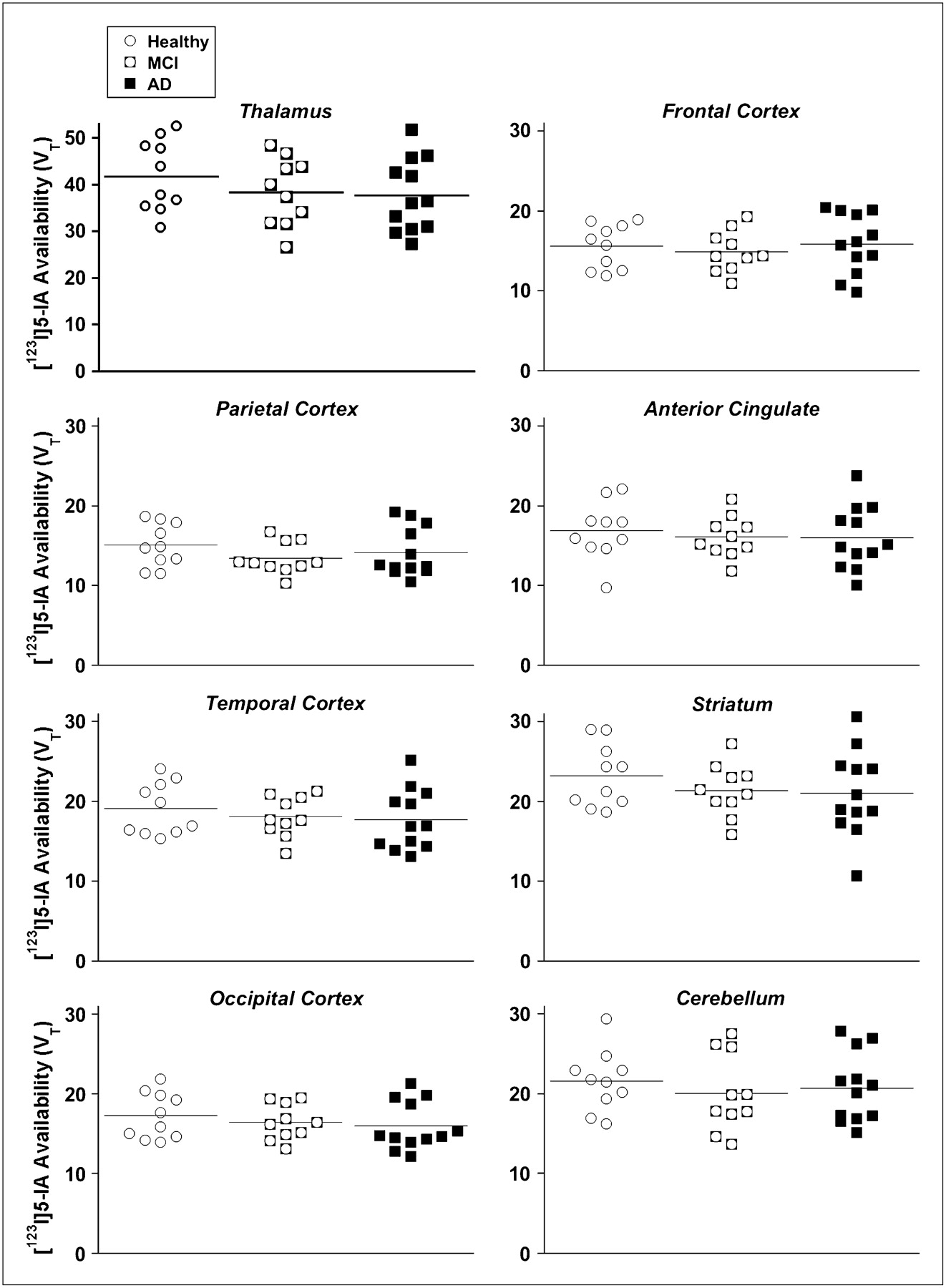
Regional nAChR availability (VT) in 8 brain regions as measured with 123I-5-IA and SPECT in older HC subjects (n = 10), subjects with amnestic MCI (n = 10), and subjects with probable AD (n = 12). MANCOVA results indicated significant overall effect of diagnostic group on mean nAChR availability (Wilks Λ test: F16,40 = 2.25; P = 0.019). However, univariate analyses revealed no significant differences among subject groups for any region.
Effect of Diagnostic Group on Regional α4β2-nAChR Availability (VT)
Relationship Between Regional α4β2-nAChR Availability and Neuropsychologic Measures
An exploratory analysis of the relationship between α4β2-nAChR availability (VT) in 6 brain regions (eliminating the cerebellum and the striatum) and performance on 10 neuropsychologic measures for each of the diagnostic groups is shown in Table 4. Significant (P < 0.05) correlations were consistently in the predicted direction (greater α4β2-nAChR availability correlating with better task performance). After Bonferroni adjustment (α = 0.05/162, or 0.00031), only the correlation between the Trail Making Test, Part B, and the anterior cingulate in the HC group (r = 0.91) remained significant (P = 0.00029). The HC group accounted for the majority of significant correlations between neuropsychologic measures and regional α4β2-nAChR availability (VT). Because of limitations in spatial resolution with SPECT, we did not attempt to measure 123I-5-IA availability in medial temporal lobe structures, including the hippocampal formation and the entorhinal cortex, for correlations with measures of episodic memory.
Correlations Between Neuropsychologic Measures and Regional nAChR Availability
DISCUSSION
The present study failed to demonstrate reductions in regional α4β2-nAChR availability in subjects with mild to moderate AD or amnestic MCI compared with age-matched HC subjects. α4β2-nAChR availability did not differ among diagnostic groups in any of the 8 brain regions investigated. An exploratory analysis of the relationship between regional α4β2-nAChR availability and neuropsychologic variables yielded several plausible correlations. However, after Bonferroni adjustment, only the correlation between the anterior cingulate and the Trail Making Test, Part B, in the HC group remained significant.
Comparison with In Vivo Imaging Studies
Our results are thus in agreement with those of Ellis et al. (26), who observed no significant reduction in α4β2-nAChR binding, as measured with 2-18F-fluoro-A-85380 (2-18F-FA) and PET, in subjects with early AD compared with age-matched HC subjects. However, our results stand in contrast to those of O'Brien et al. (24), Sabri et al. (25), and Terrière et al. (27), who all found significant reductions in α4β2-nAChR in patients with AD (24,25) or MCI (25,27), as measured with the ligand 123I-5-IA (24,27) or 2-18F-FA (25). Using 123I-5-IA, O'Brien et al. found significant reductions in the activity ratios of the region of interest to cerebellum in the frontal, striatal, right medial temporal, and pontine regions in 16 patients with AD compared with 16 control subjects. Sabri et al. reported significant reductions in the 2-18F-FA binding potential (using the corpus callosum as a reference region) in the hippocampus, caudate, frontal cortex, temporal cortex, posterior cingulate, anterior cingulate, and parietal cortex in 17 patients with moderate to severe AD and 6 subjects with amnestic MCI compared with 10 older HC subjects. That study contained very little subject characterization, including demographics, cognitive or functional status, smoking status, or concomitant medications, thus limiting comparison with other studies. Terrière et al. studied 9 subjects with amnestic MCI and 10 age-matched HC subjects by using 123I-5-IA and statistical parametric mapping analysis with global normalization; the subjects with MCI evidenced discrete reductions in uptake in the medial temporal cortex.
The divergent results among these studies may be related to several factors, including subject differences and outcome measures. Severity level may account for some differences because positive results were obtained in the studies of O'Brien et al. (subjects with somewhat more advanced AD; MMSE score, 17.2 ± 5.7) (24) and Sabri et al. (subjects with moderate to severe AD) (25), whereas negative results were observed in subjects with milder AD in the study of Ellis et al. (MMSE score, 22.5 ± 2.5) (26) and the present study (MMSE score, 20.4 ± 5.9). To be sure, these severity differences were not great and do not explain the discrepant results even in studies of MCI. The finding by Terrière et al. (27) of reduced α4β2-nAChR binding restricted to the medial temporal cortex may be particularly susceptible to partial-volume effects, given that medial temporal lobe structures are also most atrophied in amnestic MCI (37). However, this feature is a limitation of all studies, none of which have corrected for the effects of atrophy. All studies that provided information about the subjects appropriately excluded current smokers. Only O'Brien et al. (24) included subjects taking cholinesterase inhibitors (7/16) in the AD group; however, these authors reported substantially the same results when these subjects were excluded from the analysis. The 2 studies in which gray matter reference regions—either the cerebellum (24) or the whole brain (27)—were used were limited by substantial nicotine-specific binding in these regions (20,21).
Older PET studies with 11C-nicotine had revealed reductions in nAChR-binding sites in subjects with moderate AD (14,15). Significantly lower levels of 11C-nicotine binding were observed in the frontal cortex, temporal cortex, and hippocampus in patients than in these regions in control subjects (14,15). These 11C-nicotine studies were limited by high nonspecific binding, rapid metabolism and washout from the brain, and a strong dependence on cerebral blood flow. Some of these studies involved the use of a dual-tracer model, with the administration of 15O-H2O and 11C-nicotine, to generate a flow-compensated parameter of 11C-nicotine binding (14,15).
Comparison with Postmortem Studies
Our results also disagree with those of the majority of postmortem binding studies of AD, which have consistently revealed that the nAChR subtype is reduced (reviewed in (9)). However, these studies were done largely with autopsy specimens from patients in the terminal stages of the disease (2,6). Studies that have specifically included patients with mild AD (7,10) or MCI (11) are extremely rare and have tended to suggest that reductions in nAChR binding may be restricted to the moderate or even the severe stages of the disease. Perry et al. (7) showed that 3H-epibatidine binding in the temporal cortex was inversely correlated with clinical severity (CDR rating). However, these investigators also observed no discernible decline in nAChR binding in individuals with CDR scores of 0–2, but only in the severe stages of the disease (7). Pimlott et al. (10) reported no significant differences in 125I-5-IA binding in several brain regions, including the caudate, putamen, and insular cortex, between control subjects and patients with mild AD (n = 4); however, the neocortical and medial temporal regions were not examined. Interestingly, the only study of nAChR binding in subjects with MCI found no difference in 3H-epibatidine binding between subjects with no dementia and subjects with MCI (11).
More broadly, several postmortem investigations have suggested the preservation during the early stages of AD of a range of cholinergic markers, including neocortical acetylcholinesterase activity (3), choline acetyltransferase activity (3,4), and cholinergic neurons in the nucleus basalis of Meynert (12). However, the results of one study have suggested that the early neuropathologic stages of AD may be associated with a loss of neocortical choline acetyltransferase activity (39). Conversely, other studies have reported reductions in the number of neurons in the nucleus basalis containing immunoreactivity for TrkA (40) and the low-affinity p75 neurotrophin receptor (41) in MCI and mild AD. These collective clinicopathologic observations—in conjunction with the results of the present in vivo imaging study—support the interpretation that there may be some phenotypic changes but minimal degeneration of cholinergic basal forebrain neurons in MCI and mild AD. Alternatively, to the extent that neurodegeneration occurs, it may be compensated for by the upregulation of cholinergic markers (4), including nAChRs.
Neuropsychologic Analyses
Our failure to observe reductions in receptor availability in subjects with AD and MCI is more striking in light of the dramatic and expected cognitive differences among our subject groups. For all neuropsychologic and clinical measures obtained (with the exception of the Trail Making Test, Part A), the performance of the MCI group was intermediate between those of the AD group and the HC group. This finding is consistent with the concept of MCI as a transitional stage between normal aging and the onset of AD. The results of these analyses also broadly supported the previous construct of amnestic MCI (13) as involving objective memory impairment but normal general cognitive function. All 4 memory measures revealed significant differences between subjects with MCI and HC subjects, but only 1 of 8 nonmemory tests (Category Fluency) revealed such a difference.
When the relationship between α4β2-nAChR availability and several neuropsychologic variables was explored with (uncorrected) correlational analyses, several plausible correlations emerged—mostly in the HC group. The HC group showed the majority of significant correlations between neuropsychologic measures and regional α4β2-nAChR availability (VT), as performance on both the Trail Making Test, Part B, and the Digit Symbol Test correlated with VT in 4 brain regions (anterior cingulate, frontal cortex, temporal cortex, and thalamus). However, after Bonferroni adjustment, only the correlation between the Trail Making Test, Part B, and VT in the anterior cingulate in the HC group remained significant. Although exploratory, this finding is interesting in light of recent evidence that genetic variations in α4β2-nAChR affect performance on attentional tasks (42) as well as the activation of an attentional network that includes the anterior cingulate (43).
Two other research teams have examined specific neuropsychologic correlations with in vivo nAChR binding in subjects with AD or HC subjects. Kadir et al. (16) found that mean cortical 11C-nicotine binding was correlated with performance on the Digit Symbol Test and the Trail Making Test, Part A—which they grouped as “attention” tests—but not with measures of episodic memory or visuospatial ability in 27 patients with mild AD. Unlike these investigators, we did not find correlations between nAChR availability and the Digit Symbol Test or the Trail Making Test, Part A, in the AD group. Indeed, the only significant correlations in this group involved Category Fluency. However, our results bear some similarity to those of Kadir et al. in that the significant correlations in the HC group included the Trail Making Test, Part A, the Digit Symbol Test, and the Trail Making Test, Part B (which also has strong attentional demands but is thought to require more executive control and set shifting). In their study with 2-18F-FA, Ellis et al. (26) used an extensive neuropsychologic test battery and found that nAChR binding in the frontal cortex in patients with mild AD correlated significantly with performance on a simple reaction time task. After correcting for multiple comparisons, they observed no significant correlations for the HC group. We did not measure simple reaction time for comparison with this finding.
CONCLUSION
The results of the present study failed to demonstrate reductions in regional α4β2-nAChR availability in patients with mild to moderate AD or amnestic MCI compared with age-matched HC subjects. These results are consistent with those of several postmortem and in vivo studies suggesting the preservation of nAChRs during the prodromal and early stages of AD. They support the interpretation that nAChR and other cholinergic reductions in AD are late-stage phenomena.
Acknowledgments
This paper is dedicated to the memory of coauthor Julie Staley. We thank Louis Amici, Jane Bartosik, Gina Morano, Andrea Perez, and Stacey Ross for excellent technical assistance. This research was supported by American Health Assistance Foundation grant A2004-216 as well as the Office of Academic Affiliations, VA Special Mental Illness Research Education and Clinical Centers Fellowship Program in Advanced Psychiatry and Psychology, Department of Veteran Affairs. None of the authors has an actual or potential conflict of interest with this research.
Footnotes
-
↵† Deceased.
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication March 8, 2009.
- Accepted for publication May 12, 2009.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.