


Abstract
The purpose of this study was to investigate the effect of total prostate-specific antigen (PSA) at the time of 11C-choline PET/CT (trigger PSA), PSA velocity (PSAvel), and PSA doubling time (PSAdt) on 11C-choline PET/CT detection rate in patients treated with radical prostatectomy for prostate cancer, who showed biochemical failure during follow-up. Methods: A total of 190 patients treated with radical prostatectomy for prostate cancer who showed an increase in PSA (mean, 4.2; median, 2.1; range, 0.2–25.4 ng/mL) were retrospectively enrolled. All patients were studied with 11C-choline PET/CT. Patients were grouped according to trigger PSA (PSA ≤ 1 ng/mL, 1 < PSA ≤ 2 ng/mL, 2 < PSA ≤ 5 ng/mL, and PSA > 5 ng/mL). In 106 patients, data were available for calculation of PSAvel and PSAdt. Logistic regression analysis was used to determine whether there was a relationship between PSA levels and PSA kinetics and the rate of detection of relapse using PET. Results: 11C-choline PET/CT detected disease relapse in 74 of 190 patients (38.9%). The detection rate of 11C-choline PET/CT was 19%, 25%, 41%, and 67% in the 4 subgroups—PSA ≤ 1 ng/mL (51 patients), 1 < PSA ≤ 2 ng/mL (39 patients), 2 < PSA ≤ 5 ng/mL (51 patients), and PSA > 5 ng/mL (49 patients)—respectively. Trigger PSA values were statistically different between PET-positive patients (median PSA, 4.0 ng/mL) and PET-negative patients (median PSA, 1.4 ng/mL) (P = 0.0001). Receiver-operating-characteristic analysis showed an optimal cutoff point for trigger PSA of 2.43 ng/mL (area under the curve, 0.76). In 106 patients, PSAdt and PSAvel values were statistically different between patients with PET-positive and -negative scan findings (P = 0.04 and P = 0.03). The 11C-choline PET/CT detection rate was 12%, 34%, 42%, and 70%, respectively, in patients with PSAvel < 1 ng/mL/y (33 patients), 1 < PSAvel ≤ 2 ng/mL/y (26 patients), 2 < PSAvel ≤ 5 ng/mL/y (19 patients), and PSAvel > 5 ng/mL/y (28 patients). The 11C-choline PET/CT detection rate was 20%, 40%, 48%, and 60%, respectively, in patients with PSAdt > 6 mo (45 patients), 4 < PSAdt ≤ 6 mo (20 patients), 2 < PSAdt ≤ 4 mo (31 patients), and PSAdt ≤ 2 mo (10 patients). There was no statistical difference between PET-positive and -negative scan detection rates according to the Gleason score, pT and N status, patient age, or duration between surgery and biochemical relapse. Trigger PSA and PSAvel were found to be independent predictive factors for a PET-positive result (P = 0.002; P = 0.04) and PSAdt was found to be an independent factor only in patients with trigger PSA less than 2 ng/mL (P = 0.05) using multivariate analysis. Conclusion: The 11C-choline PET/CT detection rate is influenced by trigger PSA, PSAdt, and PSAvel. This finding could be used to improve the selection of patients for scanning by reducing the number of false-negative scans and increasing the detection rate of disease in patients with early relapse and potentially curative disease.
Prostate cancer (PC) is one of the most common cancers in men, and the incidence has dramatically increased in the last few years. Currently, PC is the second most common cause of cancer death in men over the age of 50 y. Within the European Union, the incidence rate is 78.9 per 100,000 per year, and the mortality rate is 30.6 per 100,000 per year (1).
Tumor recurrence is common: Relapse after primary therapy occurs (within 10 y) in 20%−30% of patients who have undergone prostatectomy (2,3) and (within 5 y) in up to 53% after external-beam radiotherapy (4). During follow-up, the monitoring of prostate-specific antigen (PSA) levels is the most useful marker for the presence of recurrent disease (5). When biochemical relapse occurs, it is crucial to discriminate between single or multiple lesions, local relapse, or distant metastatic disease to choose the appropriate treatment (1,2).
In patients with biochemical relapse, the accuracy of conventional imaging techniques (transrectal ultrasound [TRUS], CT, MRI, and bone scintigraphy [BS]) is limited. The sensitivity of CT and MRI ranges between 30% and 80% for the detection of lymph node metastases in staging the disease (6–8), but it is much lower in restaging as reported in a recently published large study (9). CT has a limited role in local recurrence (10,11), whereas endorectal-coil MRI has revealed promising results (12,13). In the detection of local relapse, TRUS has a sensitivity between 25% and 54% but is lower at PSA values less than 1 ng/mL (14). Skeletal metastases are rarely detected by bone scanning in men with PSA levels lower than 10 ng/mL (15,16). In recent years, PET (PET/CT) with 11C-choline has emerged as a promising molecular imaging tool for the detection of PC recurrences in patients with biochemical relapse. Even though the detection rate for recurrence with 11C-choline PET/CT decreases at lower levels of PSA, overall the technique remains more sensitive than conventional imaging modalities (17–22).
11C-choline is a substrate for the synthesis of phosphatidylcholine, which is the major phospholipid in the cell membrane (23). Choline kinase activity is substantially upregulated in tumor cells (24,25). The uptake of 11C-choline seems to be mediated by a selective choline transporter and can be affected by chemotherapy and antiandrogen treatment as shown by a recently published in vitro study by Müller et al. (26).
The rationale for our study is based on the fact that PSA levels should reflect or be proportional to the size and the metabolic activity of prostatic metastases (1–3). Moreover, it is known that rapid change in PSA kinetics, either before or after treatment, is an indicator of poor prognosis after surgery or radiation therapy (27–29). Therefore, it is possible that 11C-choline PET/CT is more likely to be positive not only in patients with high levels of trigger PSA but also in patients with faster changes in PSA kinetics. It may be possible to select a population of patients with a high probability of 11C-choline PET/CT positivity on the basis of trigger PSA levels and PSA kinetic values. This combination may reduce the high false-negative rate of 11C-choline PET results reported in the literature.
The aim of this study was to evaluate the detection rate of whole-body 11C-choline PET/CT for metastatic disease relative to PSA kinetics (expressed as PSA velocity and PSA doubling time) in the restaging of patients with biochemical relapse after radical prostatectomy.
MATERIALS AND METHODS
Patient Population
The study was performed according to the declaration of Helsinki and to national regulations. All patients gave informed consent to participate and for the anonymous publication of data.
A total of 190 consecutive patients (mean age, 68 y; range, 54–83 y) previously treated with radical prostatectomy, with or without pelvic lymph node dissection, and with biochemical recurrence of PC were included in this retrospective study.
The mean free serum PSA level at the time of PET/CT scan (trigger PSA) was 4.2 ng/mL, and median value was 2.1 (range, 0.2–25.4 ng/mL). Pathologic TNM staging was evaluated according to the criteria of the American Joint Committee on Cancer, and histologic grade was evaluated using the Gleason scoring system. Patient population characteristics are summarized in Table 1. All patients underwent 11C-choline PET/CT. None of the patients was receiving any treatment for PC at the time of 11C-choline PET/CT investigation; 169 patients were never treated with hormonal therapy or had not received any treatment within the 6 mo before the scan. Twenty-one patients received their last hormonal treatment between 3 and 6 mo before the 11C-choline PET/CT scan.
Patient Population Characteristics
In 130 patients, BS performed within 3 mo before the PET/CT study was available at the time of reporting. Eighty-four patients had an abdominal CT or MRI scan before the PET/CT scan. On the basis of PSA levels at the time of the PET/CT scan, patients were divided into 4 subgroups: PSA ≤ 1 ng/mL, 1 < PSA ≤ 2 ng/mL, 2 < PSA ≤ 5 ng/mL, and PSA > 5 ng/mL. In 106 patients, data about PSA velocity (PSAvel) and PSA doubling time (PSAdt) were available. Only patients who were able to provide at least 2 PSA measurements after PSA progression (i.e., at least 3 PSA values) were included. None of these patients had any hormonal treatment in the 12 mo before the 11C-choline PET/CT scan.
Radiopharmaceuticals
11C-choline was synthesized according to the solid-phase method, essentially as described by Pascali et al. (30), in a modified commercial synthesis module (TRACERlab; GE Healthcare).
Imaging Protocol
All PET/CT scans were obtained with the Discovery LS (GE Healthcare), a dedicated PET/CT scanner comprising an ADVANCE Nxi PET scanner and a LightSpeed DS multislice CT tomograph. The patients fasted for at least 6 h before PET and received an intravenous injection of 11C-choline (370–555 MBq). The PET/CT scan started 5 min after the injection (according to the 11C-choline kinetic results of previous studies (18,19)), and emission data were acquired at 5–6 bed positions from the mid thigh to the base of the skull, taking 5 min for each position. Patients were asked to void immediately before being scanned, to minimize the presence of tracer in the urinary pathways, and the scan started from the pelvis. The CT parameters were 120 kVp, 60 mA, 0.8 s per tube rotation, slice thickness of 5 mm, pitch of 1.5, and table speed of 30 mm/rotation. CT images were used both for attenuation correction of emission data and for image fusion.
Image Analysis
All PET images were analyzed with dedicated software (eNTEGRA; GE Healthcare), which allowed the review of PET, CT, and fused-imaging data. PET images were first assessed visually, using transaxial, sagittal, and coronal displays, and interpreted by the consensus of 2 experienced nuclear medicine physicians aware of the clinical data. Images were visually interpreted: Any focal uptake of 11C-choline that was higher than the surrounding background was considered suggestive of malignancy. Maximum standardized uptake value (SUVmax) was measured and considered, but no absolute cutoff value was used for the diagnosis. PET/CT findings were considered to be positive if they were confirmed by any one of the following: positive biopsy (only in the case of local relapse) or confirmation of the same lesion by any imaging procedure that had been performed within 6 mo of the PET/CT scan, including BS, TRUS, CT, or MRI. Finally, positive lesions showing a normalization of 11C-choline uptake in a subsequent scan after systemic therapy or positive lesions that were confirmed in a successive scan with the development of further lesions were also considered to be positive.
Data Analysis
The variation of PSA levels was evaluated before the PET/CT study, using at least 2 measurements obtained after the initial PSA level (which had to be >0.2 ng/mL). PSAvel was calculated according to the following formula: (PSA2 − PSA1/time) + (PSA3 − PSA2/time)/2 (31). PSAdt was calculated using the natural logarithm of the first and last PSA and the months between these 2 records. Then the natural logarithm of 2 was divided by the ratio of the difference in transformed PSA to the time between them (32).
The receiver-operating-characteristic (ROC) curve was generated by plotting sensitivity versus 1 − specificity (MedCalc 7.0; MedCalc Software) and was assessed to find the best cutoff point for PSA to predict positive PET/CT scan results. Univariate and multivariate logistic regression analysis (MedCalc 7.0) was performed to assess the influence of various factors (trigger PSA, PSAvel, PSAdt, age, Gleason score, pT and N initial stage, and time elapsed between surgical intervention and PSA progression) on 11C-choline PET/CT detection rate.
RESULTS
The following are trigger PSA values: PSA ≤ 1 ng/mL in 51 patients, 1 < PSA ≤ 2 ng/mL in 39 patients, 2 < PSA ≤ 5 ng/mL in 51 patients, and PSA > 5 ng/mL in 49 patients.
Overall, 11C-choline PET/CT detected disease relapse in 74 of 190 patients (38.9%). Median and mean values for trigger PSA at the time of PET investigation were 1.5 and 2.4 ng/mL in 116 PET-negative patients and were 4.2 and 6.7 ng/mL in 74 PET-positive patients (P = 0.0001; Table 2).
Trigger PSA and PSA Kinetics
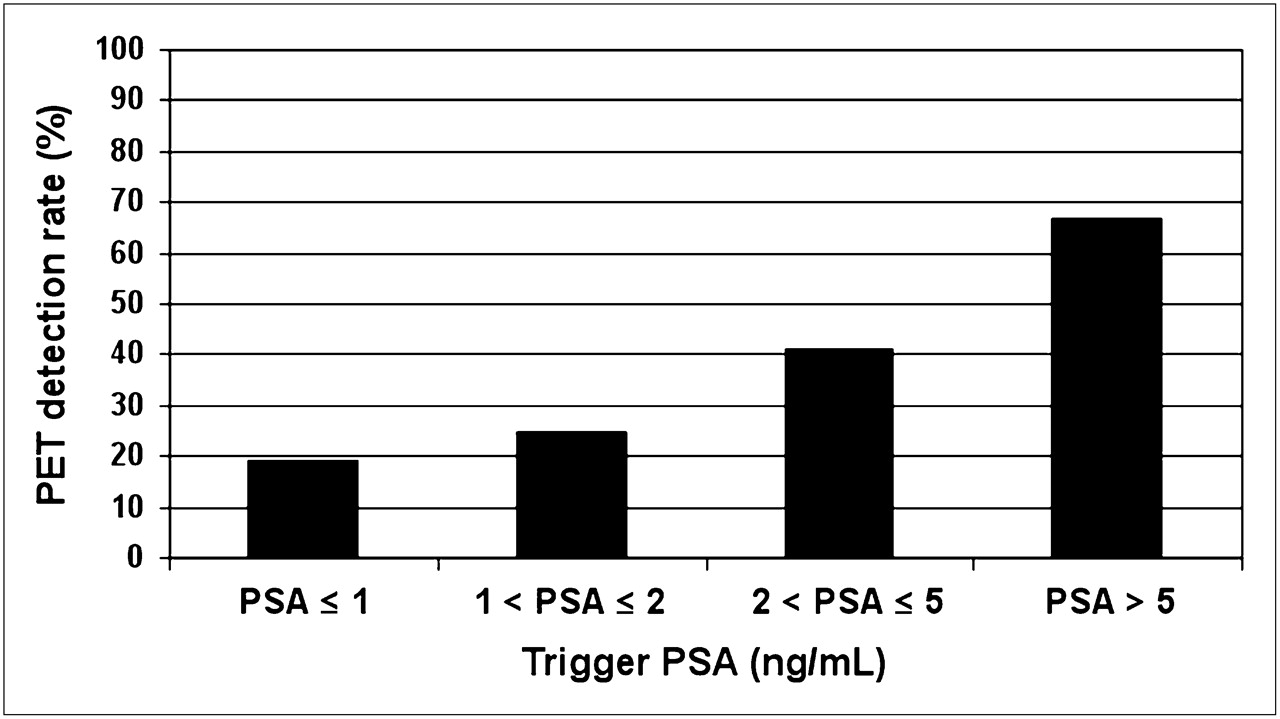
The percentages of positive 11C-choline PET/CT scans were 19% (10/51 patients), 25% (10/39 patients), 41% (21/51 patients), and 67% (33/49 patients) in the subgroups of PSA ≤ 1 ng/mL, 1 < PSA ≤ 2 ng/mL, 2 < PSA ≤ 5 ng/mL, and PSA > 5 ng/mL, respectively (Fig. 1).

Trigger PSA and PET detection rate. Detection rate of 11C-choline PET/CT in 190 patients divided in 4 subgroups on basis of trigger PSA levels at time of PET scan: PSA ≤ 1 ng/mL (51 patients), 1 < PSA ≤ 2 ng/mL (39 patients), 2 < PSA ≤ 5 ng/mL (51 patients), and PSA > 5 ng/mL (49 patients).
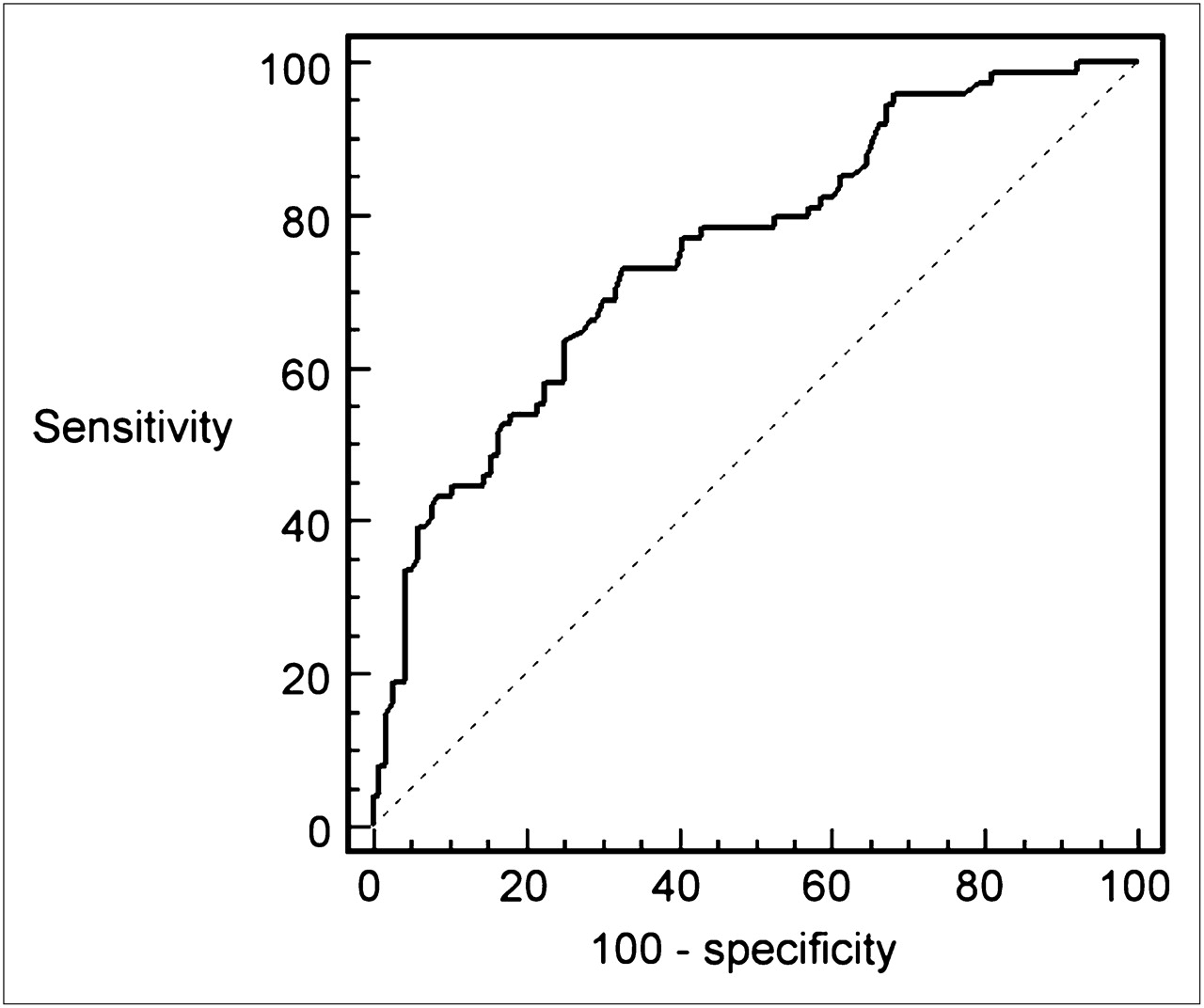
The ROC analysis demonstrated an optimal cutoff value for trigger PSA of 2.43 ng/mL, with an area under the curve (AUC) of 0.76 in the prediction of 11C-choline PET/CT positivity and a sensitivity of 73% and a specificity of 69% (Fig. 2). There were 14 of 52 (26%) PET-positive patients with a trigger PSA below the cutoff of 2.43 ng/mL and 60 of 138 (43%) PET-positive patients with a trigger PSA above the cutoff.

ROC curve of trigger PSA values in 190 patients; optimal cutoff point, 2.43 ng/mL. Area under ROC curve (AUC) = 0.76; SE = 0.037; 95% confidence interval = 0.693–0.816.
In univariate logistic regression analysis, no statistically significant differences were found in the percentage of PET/CT-positive scans according to the Gleason score (using >6 to define a high Gleason score) the pathologic T stage (pT2 vs. pT3/4), the patient age (>65 or <65 y), the duration between surgical intervention and biochemical relapse (<36 or >36 mo), or the presence or absence of lymph node (N) involvement.
Localization of Disease Relapse
11C-choline PET/CT detected 35 patients with lesions located only within bone: 18 of 35 were single lesions, and 17 of 35 were multiple lesions. Twenty patients were found to have lymph node lesions: 11 of 20 were single, and 9 of 20 were multiple. Ten patients had bone and lymph node lesions. Finally, 9 patients presented with other sites of relapse; 5 of these had local recurrence, 3 had pararectal recurrence, and 1 had a lung metastasis.
PET/CT findings were positive for bone lesions in 31 of 130 patients who had a bone scan performed before PET/CT: 22 were negative at BS, and 9 patients had shown a single lesion at BS but multiple bone lesions at PET/CT.
In 84 patients who also underwent CT or MRI, 11C-choline PET/CT had a better detection rate for relapse. 11C-choline PET/CT detected single or multiple sites of relapse in 29 of 84 patients, whereas CT or MRI detected single lesions in only 15 of 84 patients. 11C-choline PET/CT positive findings were validated in the following 6 mo by BS in 17 of 35 patients with bone lesions; CT or MRI in 9 of 20 patients with lymph node lesions and in 1 patient with a lung metastasis; and TRUS and biopsy in 5 patients with local recurrence and in 3 patients with pararectal recurrence. In the remaining 39 patients, a subsequent 11C-choline PET/CT scan confirmed positive findings according to the standard of reference described in the “Materials and Methods” section. There were no false-positive results for 11C-choline PET/CT in our study population.
PSA Kinetics: PSAvel and PSAdt
In 106 patients, data were available to enable calculation of PSA kinetics. PSAvel, expressed in ng/mL/y, and PSAdt, expressed in months, were measured.
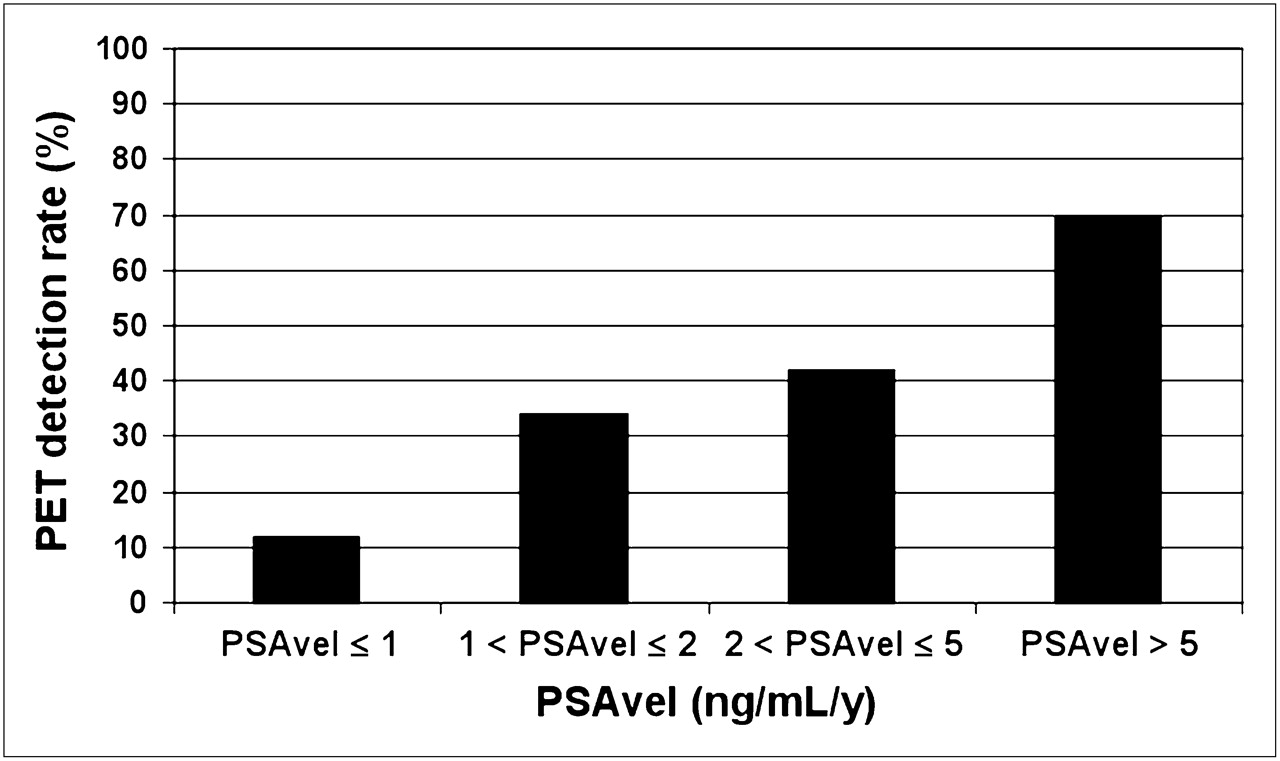
PSAvel ranged between 0.03 and 49 ng/mL/y. The differences in PSAvel values between the 2 groups of PET-positive and PET-negative patients (41 and 65 patients, respectively) were statistically significant. Median and mean values of PSAvel in PET-positive patients were 3.4 and 9.0 ng/mL/y (SD 11) versus median and mean values of 1.0 and 3.2 ng/mL/y in PET-negative patients (P = 0.03) (Table 2). The detection rates of 11C-choline PET/CT were 12%, 34%, 42%, and 70% in patients with PSAvel values of, respectively, less than 1 ng/mL/y (33 patients), 1–2 ng/mL/y (26 patients), 2–5 ng/mL/y (19 patients), and greater than 5 ng/mL/y (28 patients) (Fig. 3). ROC analysis showed an optimal cutoff point for PSAvel of 1.1 ng/mL/y (AUC, 0.75). Only 5 of 39 patients (13%) with a PSAvel less than 1.1/ng/mL/y were PET-positive, compared with 36 of 67 (54%) who were PET-positive with PSAvel greater than or equal to 1.1 ng/mL/y (Table 3).

PSAvel and PET detection rate. Detection rate of 11C-choline PET/CT in 4 groups of PSAvel values: PSAvel ≤ 1 ng/mL/y (33 patients), 1 < PSAvel ≤ 2 ng/mL/y (26 patients), 2 < PSAvel ≤ 5 ng/mL/y (19 patients), and PSAvel > 5 ng/mL/y (28 patients).
PET/CT Detection Rate for Cutoffs Determined by ROC Curve Analysis
PSAdt values ranged between 0.34 and 46 mo. There was a significant difference in the median and mean PSAdt between PET-positive and -negative patients. The median and mean PSAdt values were 3.9 and 6.2 mo, respectively, for PET-positive patients versus 6.2 and 10.1 mo, respectively, for PET-negative patients (P = 0.04) (Table 2).
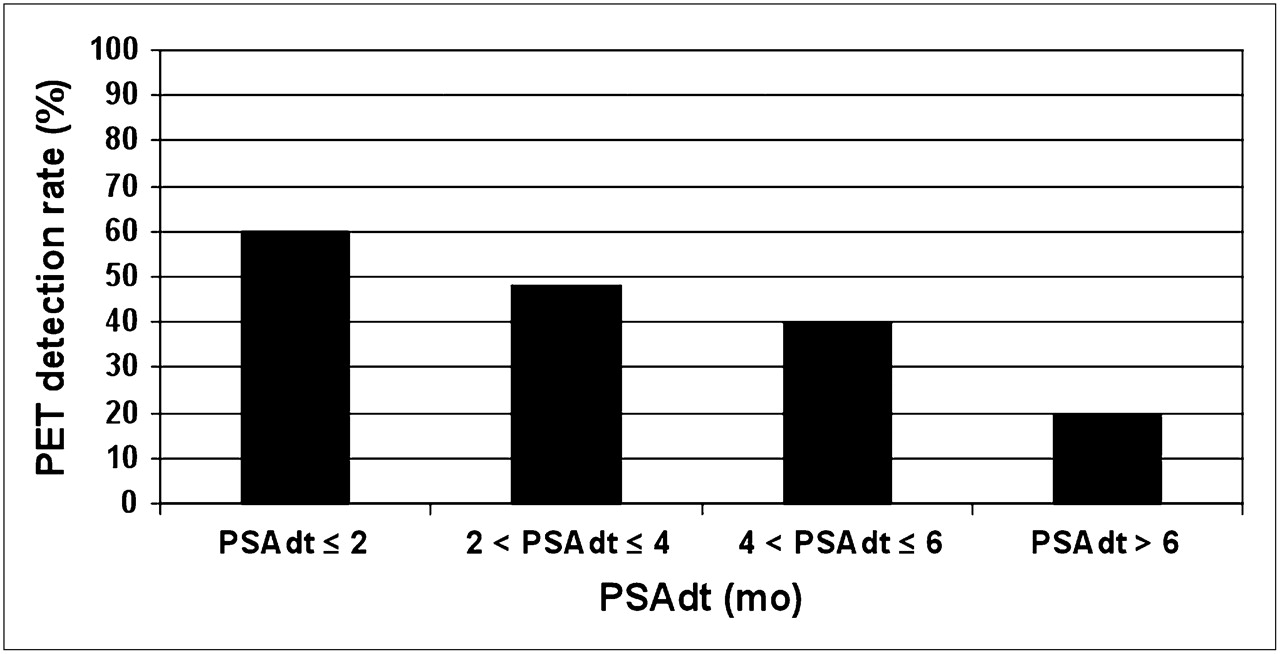
The detection rates of 11C-choline PET/CT were 20%, 40%, 48%, and 60% in patients with PSAdt values of greater than 6 mo (45 patients), 4–6 mo (20 patients), 2–4 mo (31 patients), and less than 2 mo (10 patients), respectively (Fig. 4). ROC analysis showed an optimal cutoff point for PSAdt value of 3.4 mo (AUC, 0.64). A total of 22 of 72 patients (30%) with a PSAdt greater than 3.4 mo were PET-positive, compared with 19 of 34 (56%) who were PET-positive with a PSAdt less than or equal to 3.4 mo (Table 3).

PSAdt and PET detection rate. Detection rate of 11C-choline PET/CT in 4 groups of PSAdt values: PSAdt > 6 mo (45 patients), 4 < PSAdt ≤ 6 mo (20 patients), 2 < PSAdt ≤ 4 mo (31 patients), and PSAdt ≤ 2 mo (10 patients).
In a subgroup of patients with trigger PSA less than 2 ng/mL (60 patients, 15 positive and 45 negative), the difference between the PSAdt values in the 2 groups was statistically significant: PSAdt mean and median values for PET-positive patients were both 5 mo, and PSAdt mean and median values for PET-negative patients were 7.3 and 11.5 mo, respectively (P = 0.05) (Table 2). In these 60 patients with a low pretest probability for PET positivity according to the trigger PSA value, the simple application of the parameter of PSAdt (slower or faster than 3.4 mo) could be used to select a group of patients who were significantly more likely to have disease detected using 11C-choline PET/CT. In fact, in patients with rapidly increasing PSA levels (PSAdt < 3.4 mo), the detection rate was 7 of 17 (41%), whereas in patients with slowly increasing PSA levels (PSAdt > 3.4 mo) the detection rate was 8 of 43 (18%) (Table 3).
Even with an arbitrary PSAdt cutoff point slower or faster than 6 mo (2,3–5), the difference in PET detection rate is evident. In patients with PSAdt less than 6 mo, the detection rate was 11 of 31 (35%), whereas in patients with PSAdt greater than 6 mo, the detection rate was 4 of 29 (14%).
Trigger PSA and PSAvel were found to be independent predictive factors for PET-positive scan findings (P = 0.002; P = 0.04) using multivariate regression analysis. However, PSAdt was found to be an independent factor only in the group of 60 patients with trigger PSA less than 2 ng/mL (P = 0.05), not in the whole population.
DISCUSSION
Recently, there have been several research groups that have investigated the potential use of conventional imaging or PET with 11C- or 18F-choline in PC patients with biochemical failure. Available data suggest a better diagnostic accuracy for PET, but they also suggest a correlation between trigger PSA values and imaging sensitivity.
In a recent study by Choueiri et al. (9) in 292 patients, a significant correlation was found between imaging sensitivity (BS, CT, and MRI) and trigger PSA, PSAdt, and PSAvel. However, conventional imaging in their series detected only 31 (11%) imaging-positive patients, and the mean value of PSA trigger was high at 23 ng/mL. The finding of the study by Choueiri et al. (9) contrasts with the study by Picchio et al. (21) in which the site of recurrence was detected with 11C-choline PET in 47 of 100 patients. The mean trigger PSA value in their population was 6.5 ng/mL. De Jong et al. (22) proved disease relapse in 5 of 13 (38%) patients after radical prostatectomy and 7 of 9 (78%) patients after radiotherapy, but 11C-choline was negative in all patients with PSA less than 5 ng/mL. Similar issues of limited sensitivity of PET/CT for low trigger PSA values have also been identified with 18F-choline. Schmid et al. (33) and Cimitan et al. (17) showed a low detection rate of PET/CT in patients with PSA values lower than 4–5 ng/mL.
Krause et al. (20) have recently shown that 11C-choline PET/CT in 63 patients, with a mean PSA value of 5.9 ng/mL, had an overall detection rate of recurrence of 56%. They also demonstrated a linear relationship between trigger PSA and PET detection rate: PET showed recurrence in 36% of the patients with a PSA value less than 1 ng/mL, in 43% with a PSA value between 1 and 2 ng/mL, in 62% with a PSA value between 2 and 3 ng/mL, and in 73% with a PSA value greater than or equal to 3 ng/mL.
Husarik et al., using 18F-choline PET, had a detection rate of 84% in 68 patients. However, in that population the mean PSA level was 10.8 ng/mL (34). Reske et al., studying 11C-choline PET/CT in a group of 33 patients with histologically proven local relapse, showed a sensitivity of 71% and good specificity, with 12 true-negative scans in 13 control patients (35).
Scattoni et al. (36) also demonstrated good specificity with 11C-choline PET/CT in the restaging of patients with biochemical relapse and lymph node lesions. In this study, specificity was 90%, and the positive predictive value was 86%. All positive findings were histologically confirmed.
There is converging evidence in the literature that PET with radioactively labeled choline derivates has a significantly higher detection rate than conventional imaging, with high specificity and positive predictive value and a relationship between detection rate and trigger PSA values. In our series, the relationship between detection rate and trigger PSA was highly statistically significant (P = 0.0001), using the optimal cutoff point for trigger PSA value of 2.43 ng/mL.
None of the known risk factors (1–3) appears to influence 11C-choline PET/CT sensitivity as much as trigger PSA does. In fact, none of the following factors was found to be statistically significant in a univariate analysis: patient age, duration between surgery and biochemical relapse, Gleason score, and the initial T and N stage.
Overall, in our population, the 11C-choline PET/CT detection rate (38.9%) was substantially lower than that stated in the literature, and this difference is likely due to our patient selection. We did not select patients with a high risk of relapse, because our study was designed to understand the influence of PSA and PSA kinetics on PET detection rate, especially for low trigger PSA levels. However, if we compare the mean PSA values and overall 11C-choline PET detection rate in our patient population (4.2 ng/mL and 38.9%, respectively) with those of 3 large studies—Picchio et al. (6.5 ng/mL and 47%) (21), Krause et al. (5.9 ng/mL and 56%) (20), and Husarik et al. (10.8 ng/mL and 84%) (34)—our overall detection rate is in line with these published results. In patients with low PSA values, our detection rate is lower than that found by Krause et al. (20). In patients with PSA less than 2 ng/mL, their detection rate was 38%; in our study, however, the detection rate was only 22% in patients with low PSA. This difference is not possible to explain and can be solved only by further larger studies.
According to our findings, the analysis of PSA kinetics, using PSAvel and PSAdt as parameters, may be suggested to improve detection rate in patients with biochemical relapse and, thus, to reduce the number of PET-negative studies, especially when PSA is low. Our results showed that the detection rate of 11C-choline PET/CT is significantly higher when PSAvel was greater than 1.1 ng/mL/y or PSAdt was less than 3.4 mo (Fig. 5).
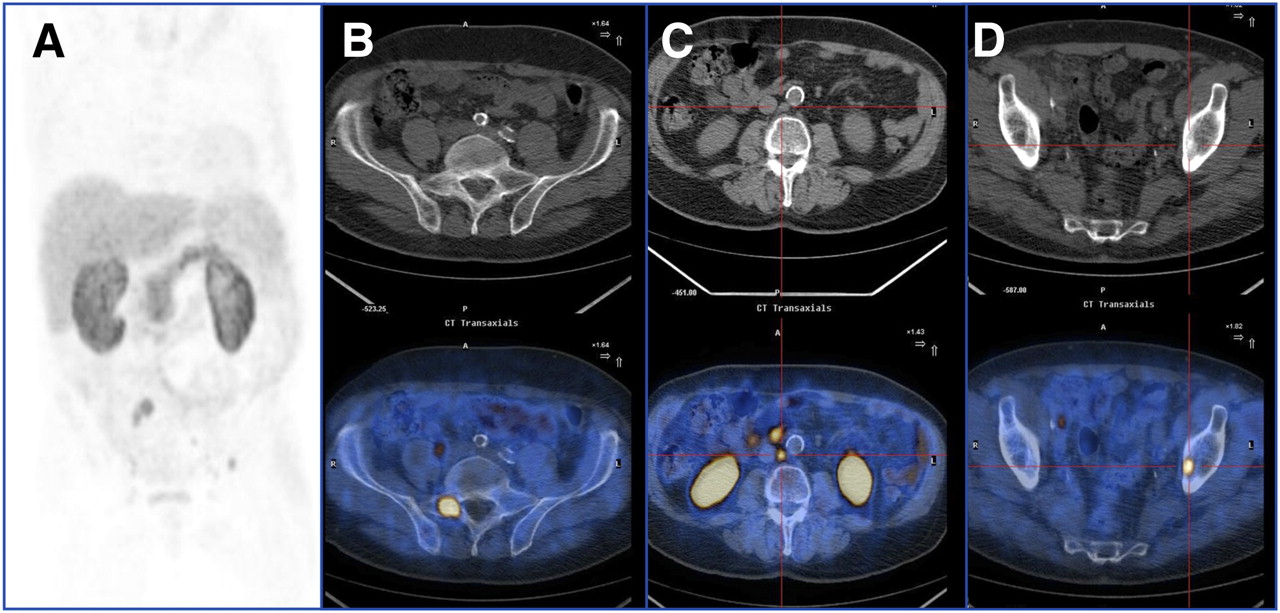
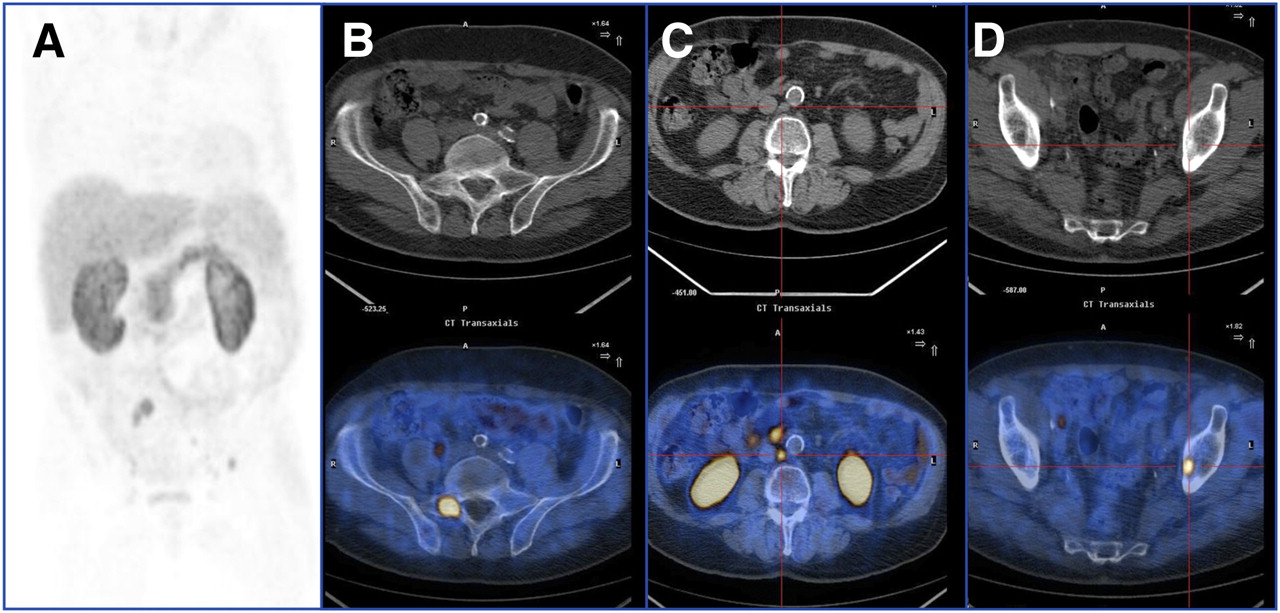
One-year-old patient who underwent surgery (initial staging, pT3b Nx, Mx; Gs 4 + 3) in July 2006. Trigger PSA at time of PET scan was 0.35 ng/mL (February 2007). (A) Maximum-intensity projection. (B) Sacral bone lesion (note large extent and high uptake of lesion [SUVmax, 7.1] without any structural damage on attenuation correction CT, suggestive of fast growing, highly hypermetabolic disease). (C) Positive paraaortic LN (9 mm). (D) Small left pelvic bone hypermetabolic lesion without corresponding findings on CT. PSAdt = 1 mo.
This is an initial study demonstrating a significant association between 11C-choline PET detection rate and PSA kinetics. On the basis of our findings, only patients with a high probability of having a positive scan should undergo a 11C-choline PET investigation. This likelihood is increased in patients with a trigger PSA less than 2.4 ng/mL and with PSAdt or PSAvel lower than 3.4 mo or higher than 1 ng/mL/y, respectively, or in patients with an initial trigger PSA higher than 2.4 ng/mL. Using these criteria, we were able to satisfy 2 needs: to reduce the number of inappropriate choline PET/CT scans and to improve the early detection of the site of recurrence soon after biochemical relapse. This should help clinicians in the selection of patients who could benefit the most from this functional imaging method and improve the clinical impact of PET with 11C-choline on patient management.
Despite the above-mentioned good results of choline PET/CT in terms of specificity, the problem of the validation of positive findings is the main limitation of our study. As with many other studies that try to address the same issue, our validation has been based on a longitudinal follow-up of each lesion. Histology would have been preferable but was not feasible because of practical and ethical issues.
CONCLUSION
11C-choline PET/CT plays an emerging and important role in PC because it is a noninvasive test that allows a whole-body examination in 1 step.
Our study demonstrates that 11C-choline PET/CT has a linear relationship with the PSA level (trigger PSA) at the time of PET/CT, with lower detection rates at lower PSA levels. There also appears to be a relationship between the rates of change in PSA, measured by PSA kinetics, and the positivity of the 11C-choline PET. This relationship was true using either PSAdt or PSAvel, particularly when the absolute PSA level was low. The greater the level of PSAdt and PSAvel, the more likely the 11C-choline PET/CT was to be positive. Therefore, the PSA kinetics could be useful in selecting patients for 11C-choline PET scans and reducing the number of negative or inconclusive 11C-choline PET scan findings and, thus, in detecting patients with early relapse who are potentially treatable with curative intent. Further studies will be needed to confirm this hypothesis.
Acknowledgments
We thank Riccardo Schiavina, Gian Carlo Montini, Vincenzo Allegri, and Cinzia Pettinato for their contribution to the release of this work.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication December 22, 2008.
- Accepted for publication May 7, 2009.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 11C-Choline PET/CT in Recurrent Prostate Cancer: Retrospective Analysis in a Large U.S. Patient Series
- What Medical, Urologic, and Radiation Oncologists Want from Molecular Imaging of Prostate Cancer
- 11C- or 18F-Choline PET/CT for Imaging Evaluation of Biochemical Recurrence of Prostate Cancer
- Evaluation of Hybrid 68Ga-PSMA Ligand PET/CT in 248 Patients with Biochemical Recurrence After Radical Prostatectomy
- Early Biochemical Relapse After Radical Prostatectomy: Which Prostate Cancer Patients May Benefit from a Restaging 11C-Choline PET/CT Scan Before Salvage Radiation Therapy?
- PET/MR in Oncology: Non-18F-FDG Tracers for Routine Applications
- 11C-Choline PET/CT Predicts Prostate Cancer-Specific Survival in Patients with Biochemical Failure During Androgen-Deprivation Therapy
- Detection of Recurrent Prostate Cancer After Radical Prostatectomy: Comparison of 11C-Choline PET/CT with Pelvic Multiparametric MR Imaging with Endorectal Coil
- Prostate Cancer: PET with 18F-FDG, 18F- or 11C-Acetate, and 18F- or 11C-Choline
- Reply: Influence of Trigger PSA and PSA Kinetics on 11C-Choline PET/CT Detection Rate in Patients with Biochemical Relapse After Radical Prostatectomy
- Influence of Trigger PSA and PSA Kinetics on 11C-Choline PET/CT Detection Rate in Patients with Biochemical Relapse After Radical Prostatectomy