


Abstract
Transarterial chemoembolization (TACE) improves survival in patients with hepatocellular carcinoma (HCC) in whom curative therapies are not suitable. The aim of this study was to assess survival differences in patients with hepatic cirrhosis and unresectable HCC treated by 131I-lipiodol versus TACE or transarterial embolization (TAE). Methods: A retrospective study was performed on a cohort of 124 patients undergoing treatment for unresectable HCC between 1997 and 2006. A total of 50 patients (44 men; mean age, 59 y) received 131I-lipiodol (mean sessions per patient, 1.7), and 74 patients (63 men; mean age, 61 y) received TACE/TAE (mean sessions per patient, 1.8). Although no significant difference between the 2 treatment groups with respect to HCC size and clinical staging was observed, a higher proportion of patients with portal vein thrombosis (PVT) was treated with 131I-lipiodol than with TACE/TAE (28% vs. 8%, P = 0.003). Results: Actuarial survival was not significantly different between patients treated with 131I-lipiodol and patients treated with TACE/TAE. Survival at 6 mo, 1 y, 2 y, and 3 y was 86%, 69%, 54%, and 45%, respectively, after 131I-lipiodol, compared with 77%, 62%, 47%, and 43%, respectively, after TACE/TAE. However, patients with PVT survived a mean of 454 d after 131I-lipiodol, compared with a mean of 171 d after TACE/TAE (P = 0.025). In addition, patients with more advanced disease (Barcelona Clinic Liver Cancer stage D) lived on average 363 d after 131I-lipiodol, compared with 36 d after TACE/TAE (P = 0.014). Conclusion: In patients with unresectable HCC, there was no difference in survival between 131I-lipiodol therapy and TACE/TAE treatment. However, in the patients with advanced clinical staging or PVT, there was a significant survival advantage for those treated with 131I-lipiodol.
Hepatocelluar carcinoma (HCC) is the world's fifth most common neoplasm, with its highest incidence in the developing world. It is the third most common cause of cancer death, and its development is related to the incidence of cirrhosis (1). Prognosis depends on the extent of the tumor at diagnosis but also on the extent of liver injury and the presence or absence of portal vein thrombosis (PVT). All of these factors are independent predictors of survival (2).
Curative treatments are normally offered in 40% of patients at most (1); hence, most patients can be given only palliative treatment. At present, the only such treatment that has been shown to improve survival is transarterial chemoembolization (TACE) (3). However, the optimal technique has not been defined, and it has been reported that the use of particles alone (transarterial embolization [TAE]) may give results similar to adding chemotherapy (4). These treatments may have significant morbidity, especially if the patient has little hepatic reserve (3,4). To provide an alternative with potential similar efficacy but reduced morbidity, several groups, including our own, have used radioiodinated poppyseed oil (131I-lipiodol) (3,5–7). The number of published studies remains small, so results concerning the therapeutic use of this agent are heterogeneous and even contradictory (8).
In our center, we have been offering 131I-lipiodol therapy as a routine treatment in unresectable HCC for 10 y. The aim of this study was to evaluate the outcomes of intraarterial 131I-lipiodol, compared with TACE and TAE, in patients with cirrhosis and unresectable HCC. Second, we determined whether there were any specific patient or tumor characteristics that were associated with improved survival.
MATERIALS AND METHODS
Patient Selection
An audit was performed of consecutive patients with cirrhosis and unresectable HCC treated with 131I-lipiodol between January 1997 and March 2006. There were 50 such patients (44 men, 6 women; mean age, 59 y; range, 28–89 y). In addition, data from 74 consecutive patients treated with TACE or TAE between January 1997 and June 2003 were also collected to provide data for comparison with the 131I-lipiodol group (63 men, 11 women; mean age, 61 y; range, 23–84 y).
The diagnosis of HCC was made according to the criteria of the 2000 Barcelona European Association for Study of the Liver consensus conference (9). At baseline (the day of the first session of intraarterial treatment), standard laboratory data and imaging characteristics of the HCC and liver from cross-sectional imaging (CT or MRI) were recorded. The presence of PVT was also noted in the 2 treatment groups. The Child–Pugh, Model for End-Stage Liver Disease (MELD), Cancer Liver Italian Program (CLIP), and Barcelona Clinic Liver Cancer (BCLC) scores were calculated, and the Okuda stage was identified (10–15).
Overall survival for each patient was calculated from the date of the patient's first procedure (131I-lipiodol, TACE, or TAE) until death, loss to follow-up or liver transplantation, or status at the time of data collection (March 2006). The mean follow-up data available for the 131I-lipiodol group was 168 d (range, 8–1,054 d) and for the TACE/TAE comparison group 270 d (range, 9–1,703 d).
Before starting treatment with 131I-lipiodol, 3 patients had undergone percutaneous ethanol treatment (PEI), and 9 had received previous TACE treatment (data from these patients were not included in the TACE group). In the patients treated with TAE/TACE, 4 patients had received PEI or radiofrequency ablation.
Treatment
131I-Lipiodol.
After a full diagnostic angiogram to determine the vascular anatomy of the liver and the HCC and the presence or absence of PVT, a slow infusion of 131I-lipiodol (1,000 MBq) was administered under fluoroscopic control, into either the right or the left hepatic artery, depending on the site of the tumor. In patients with extensive bilateral disease, the 131I-lipiodol was infused into the common hepatic artery distal to the gastroduodenal artery. Care was taken to ensure that the rate of infusion did not cause reflux and result in retrograde flow down the gastroduodenal artery. The procedure was performed under light benzodiazepine sedation, and opiate pain relief was administered 2 min before the 131I-lipiodol infusion. All radioactive lines were disposed of as required by radiation safety rules, and the patient was taken from the radiography area to a shielded room for 3–4 d before being discharged. At 48 h, a whole-body 131I-lipiodol scan was obtained to confirm tumor uptake, and a CT scan was normally obtained at day 10.
TAE/TACE.
TAE or TACE treatment was also performed under light sedation. As described above, the site of the tumor and the presence of PVT were identified. Embolization was performed using polyvinyl alcohol particles (Ivalon) (diameter, 150–500 μm) under fluoroscopic guidance until flow was stopped. If the disease was bilateral, the dominant side (normally the right) was treated first and, if appropriate, the contralateral side was treated about 6–8 wk later. For those patients receiving TACE, cisplatin was injected before the particles in the last 9 patients of this group, and 22 received epirubicin dissolved in lipiodol. When cisplatin was used, the patients were hydrated in advance and given mannitol to induce diuresis before the procedure. Opiate analgesia was administered just before the procedure and for 24 h afterward. The patient was discharged the next day if there were no complications.
Treatment Schedule.
In the 131I-lipiodol group, 32 patients received a single treatment session, 10 patients received 2 treatment sessions, and 8 patients received 3 or more treatment sessions. The minimal retreatment interval was 6 wk (although 3 mo was the usual interval), so that the mean treatment sessions for those receiving 131I-lipiodol was 1.7 (range, 1–6). In the TACE/TAE group, 45 patients received 1 treatment session, 13 received 2 treatment sessions, and 16 received 3 or more sessions. The mean number of treatments in this group was 1.8 (range, 1–6).
Tumor Response.
One month after each session of treatment, the patients underwent CT to evaluate tumor response. Further sessions of the same treatment were offered to the patient for the following reasons: if appreciable tumor response or symptomatic relief had been obtained from the previous session and if the treatment had been well tolerated and the patient's overall condition and liver function were deemed satisfactory.
Clinical, biochemical, and radiologic data were collected after the last session of intraarterial treatment or after 3 sessions of treatment.
Tumor response was evaluated on the basis of the number of HCC nodules (reduced disease, at least 1 nodule less; stable disease, same number of nodules; and progressive disease, at least 1 new nodule), size of largest HCC nodule (reduced disease, main nodule diameter reduced more than 5 mm; stable disease, main nodule diameter ± 5 mm; and progressive disease, main nodule diameter increased more than 5 mm), and α-fetoprotein values (reduced disease, reduced more than 200 ng/mL; stable disease, ±200 ng/mL; and progressive disease, increased more than 200 ng/mL).
Statistical Analysis.
Data were analyzed using a statistical analysis package (social sciences, version 11.0 for Windows; SSPS Inc.). Pearson, χ2, and Mann–Whitney U tests using this software were applied to compare categoric and continuous variables in the 2 treatment groups (significance level of P < 0.05).
Actuarial survival data were plotted using Kaplan–Meier curves, with the time zero being the date of the first 131I-lipiodol or TACE/TAE therapy session.
Variables were evaluated in a univariate analysis to test their association with tumor response and death; those with a significance level of P less than 0.1 were then entered into a multivariate analysis by linear regression.
RESULTS
131I-Lipiodol Versus TACE/TAE
Before treatment, there were no significant differences between the 2 treatment groups (Tables 1 and 2) with respect to all factors, including sex; age; cause of the underlying cirrhosis; and the Child–Pugh, MELD, CLIP, and BCLC scores. However, there was a significantly greater number of patients with PVT treated with 131I-lipiodol than with TACE/TAE (P = 0.003). Within the group of patients selected for treatment with 131I-lipiodol, 22% were staged as Okuda III, compared with only 8% staged as Okuda III treated with TCAE/TAE (P = 0.02). There was also a significantly longer duration of disease from diagnosis to treatment in the group treated with 131I-lipiodol, with a median of 143 d (compared with 35 d for TACE/TAE [P < 0.0001]).
Patient Characteristics at Baseline: 131I-Lipiodol Group Versus TACE/TAE Group
Patient Characteristics at Baseline: TACE Group Versus TAE Group
At the end of the follow-up period, 13 of 50 patients (26%) treated with 131I-lipiodol had died and 3 patients (6%) had undergone a liver transplant, compared with 32 of 74 patients (43%) in the TACE/TAE group who had died and 10 patients who had undergone a liver transplant (13%). Although the death rate in the TACE/TAE group was almost 50% greater than that in the group treated with 131I-lipiodol, this result failed to reach statistical significance, even when correcting for survival from the date of diagnosis and not from the date of treatment. The median overall survival after the first treatment was 624 d (95% confidence interval, 0–1,316 d) for patients given 131I-lipiodol, which was similar to the 638 d (95% confidence interval, 85–1191 d) recorded for those patients treated with TACE/TAE. The actuarial survival rates show that the initial better survival of patients treated with 131I-lipiodol is not apparent at the 3-y mark (Fig. 1). For the 131I-lipiodol group, the overall survival at 6 mo, 1 y, 2 y, and 3 y was 86%, 69%, 54%, and 45%, respectively, compared with 77%, 62%, 47%, and 43%, respectively, in the TACE/TAE group.
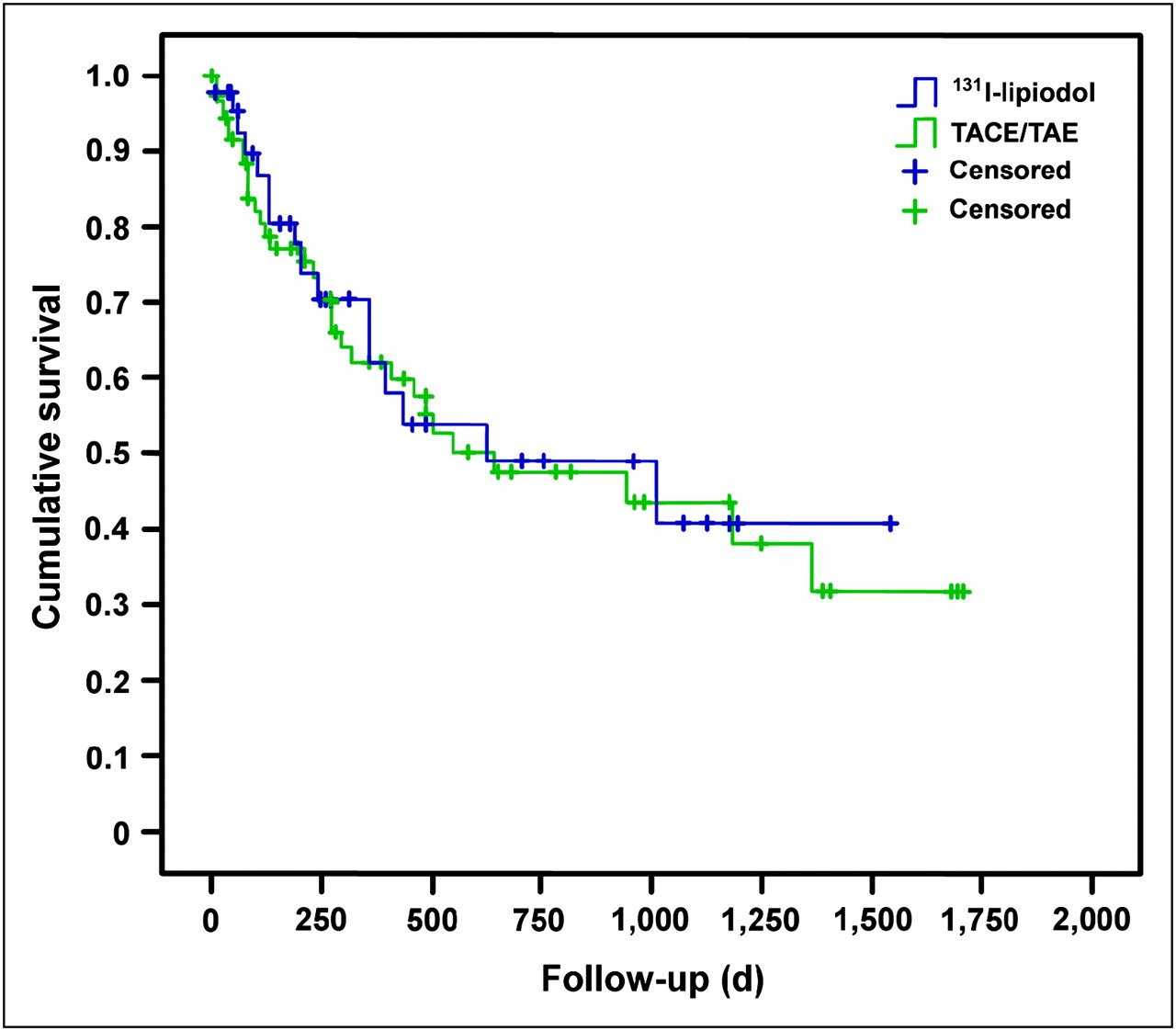
Survival curves in 131I-lipiodol group, compared with TACE/TAE group.
Factors Affecting Survival
When comparing the patients in whom only 131I-lipiodol (38 patients) or only TACE/TAE (70 patients) had been the first therapy for HCC, there was again no significant difference in survival.
Those patients with Child–Pugh score A disease treated with 131I-lipiodol had a mean overall survival of 1,111 d (±145), compared with 898 d (±127) if treated with TACE/TAE. This difference was not significant and neither was survival in Child–Pugh score B patients, in whom the mean overall survival was 407 d (±75) for those patients treated with 131I-lipiodol and 879 d (±156) for those treated with TACE/TAE.
There was, however, a significantly improved survival rate (P = 0.014) in those patients with the most advanced disease treated with 131I-lipiodol. In the patients with Child–Pugh score C disease, the mean survival rate in those patients (n = 5) treated with 131I-lipiodol was 393 d (±0), compared with 36 d (±18) in 3 patients treated with TACE/TAE. However, the number of patients with such extensive disease was small (n = 8).
PVT
A total of 20 patients had PVT at the time of therapy. Of those patients, 14 were treated with 131I-lipiodol and the mean overall survival was 454 d (±127), which was significantly longer (P = 0.025) than the 171 d (±117) in the 6 patients treated with TACE/TAE (Figs. 2 and 3). Patients with PVT treated with 131I-lipiodol had better survival than did patients treated with TACE/TAE, even when 2 patients in the131I-lipiodol group who had initial treatment with PEI or TACE were excluded from the analysis (12 vs. 6; P = 0.029). PVT itself had no affect on overall survival in those patients receiving treatment with 131I-lipiodol but was associated with significantly reduced survival in patients treated with TACE/TAE (P = 0.0002).
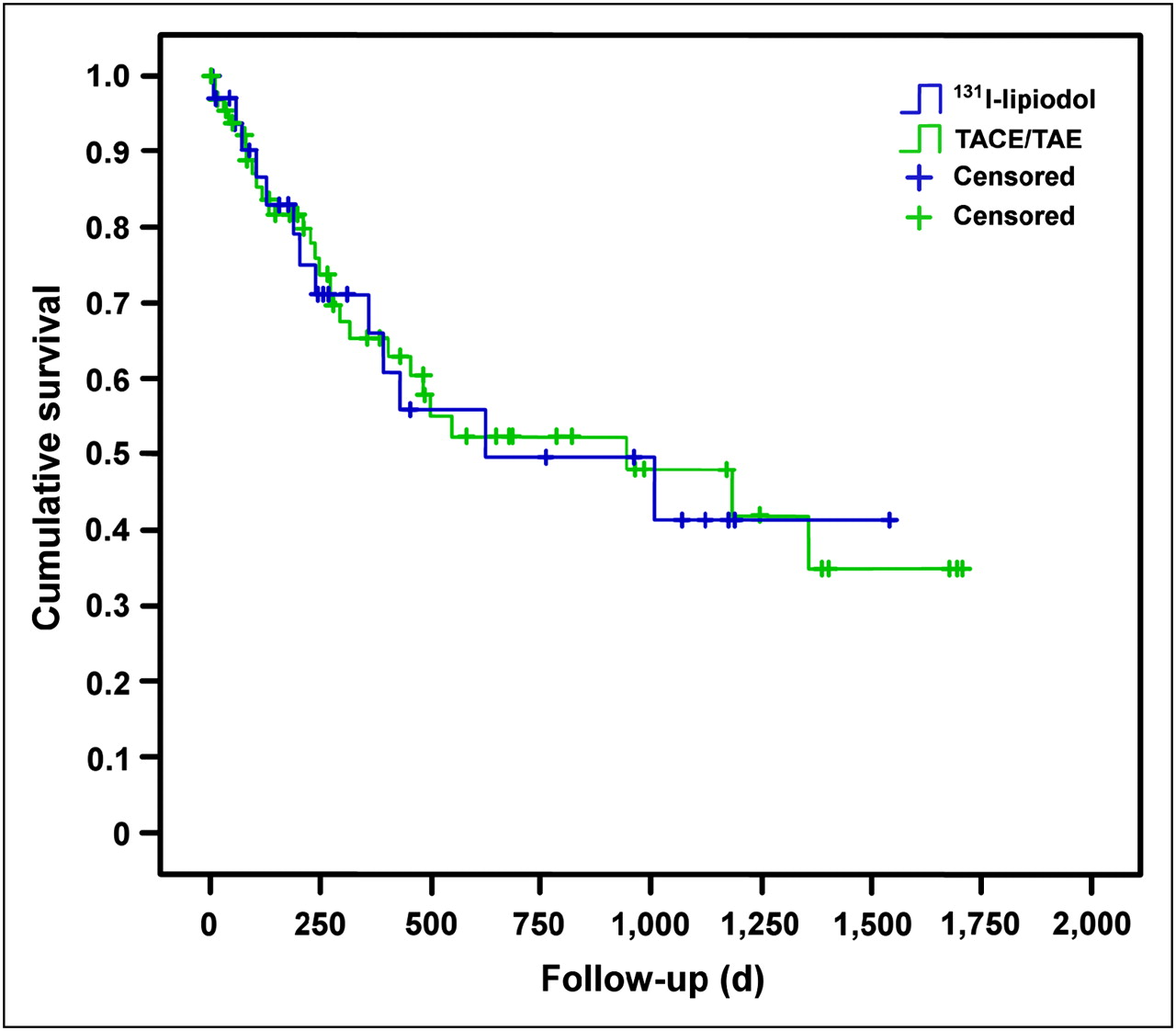
Survival curves in patients with patent portal vein in 131I-lipiodol group, compared with TACE/TAE group.

Survival curve in patients with PVT in 131I-lipiodol group, compared with TACE/TAE group (log rank P = 0.0255).
BCLC Staging
There was no significant difference in survival in patients with BCLC stage A and B between the 2 forms of treatment. In patients with BCLC stage A, the 1-y overall survival rate for the 131I-lipiodol-treated group was 88% (±8%) and for the TACE/TAE-treated group it was 77% (±9%). In patients with BCLC stage B, the survival rate was 31% (±17%) if patients were treated with 131I-lipiodol and 58% (±8%) if patients were treated with TACE/TAE.
There were only 8 patients with advanced disease (BCLC stage D); 5 of these patients were treated with 131I-lipidol and had a mean survival of 393 d (±56), which was significantly greater (P = 0.014) than the mean survival of 36 d (±18) in those patients treated with TACE/TAE (Table 3). However, because of small patient numbers, the confidence interval of this difference is large.
Percentage Mean Survival Rates at 6 Months, 1 Year, and 2 Years in 2 Groups
Size of Tumor
There was no significant difference in tumor size in the 2 treatment groups, and overall there was a tumor size reduction in 63% of patients, size stability in 28%, and progressive disease in 9%. The number of HCC nodules was reduced in 30%, was stable in 39%, and was increased in 31%. There was evidence of biologic response in terms of reduced α-fetoprotein levels in 16% of patients, the levels were stable in 39% of patients, and the levels progressed in 21% of patients. There was no difference in the 2 groups. The Child–Pugh score remained unchanged in 69% of all patients, was worse in 26%, and was improved in only 6 patients (5%).
TACE Versus TAE
Overall, 31 patients received TACE and 43 received TAE; the choice of treatment was related to the availability of the treatment. There was no significant difference in outcomes between TACE and TAE; overall survival at 6 mo, 1 y, and 2 y was 75% (±8%), 61% (±10%), and 44% (±11%), respectively, for TACE and 79% (±7%), 63% (±8%), and 50% (±9%), respectively, for TAE.
Prognostic Factors Affecting Survival
Independent of the type of treatment used, univariate analysis of various risk factors showed that pretherapy risk factors predicting an adverse outcome (death) included increasing number of tumor nodules (P = 0.07), increasing size of largest nodule (P = 0.012), and Okuda stage (P = 0.012). There was a nonsignificant trend for improved survival (P = 0.065) for those patients treated with 131I-lipiodol, considering that those treated with 131I-lipiodol had larger tumors with a poorer prognosis.
Multivariate analysis showed that the only independent factor adversely affecting survival, independent of the type of therapy, was the size of the largest nodule at imaging.
DISCUSSION
This retrospective review confirms that 131I-lipiodol therapy in patients with cirrhosis and HCC has an efficacy similar to that of TACE/TAE therapy. This finding is comparable to that of the 2 prospective randomized controlled trials that show a similar efficacy for the 2 treatment modalities (4,7) (however, the efficacy result was found for a consecutive series of patients selected solely on the feasibility of treating HCC with transarterial techniques). Therefore, there appears to be a survival benefit for 131I-lipiodol in those patients with more advanced disease, for example, in those with Okuda stage III disease or BCLC stage D. In PVT patients, there also appeared to be a significant improvement in survival for patients receiving 131I-lipiodol. These patients lived almost a year longer on average than those treated with TACE or TAE. It is known from published literature that there is an improved survival rate for those treated with 131I-lipiodol, compared with the survival rate for those receiving medical support (6). The analysis of outcomes in our cohort suggests that 131I-lipiodol may have advantages in patients with advanced disease or PVT, whereas TACE/TAE may be deleterious given the short survival times after this therapy in this subgroup.
Other radionuclide therapies have also been reported to be effective therapies for HCC, including the use of 90Y intraarterial radiotherapy, also known as radioembolization (radio refers to the radiation exposure to the tissue and embolization refers to the microembolic effect). There are currently 2 commercially available 90Y microspheres: TheraSphere (MDS Nordion) is a minimally embolic device consisting of small (20–30 μm) glass spheres, with a higher specific activity (2,500 Bq) and a lower number of spheres (1.2 million microspheres/3 GBq); conversely, a selective internal radiation (SIR) sphere is moderately embolic, consisting of 20- to 60-μm resin spheres, with a lower specific activity (50 Bq) and a greater number of spheres (∼40–80 million microspheres/3 GBq). These spheres, similar to 131I-lipiodol, are infused into the hepatic artery; as they are particles, however, only 1 lobe at a time can be embolized. Thus, for bilobar disease 2 separate treatment sessions are needed, whereas with 131I-lipiodol a single infusion into the common hepatic artery beyond the gastroduodenal artery will result in tumor uptake in both lobes. In addition, the mechanism of action of 131I-lipiodol, which involves direct uptake into tumor cells, results in a higher tumor radiation dose than do the methods requiring embolization of radioactive particles (9). In a prospective phase 2 study of 65 patients with biopsy-proven HCC, the administration of TheraSpheres (5–10 GBq) resulted in a survival time of between 8 and 12 mo for Okuda stage I or II patients (10). Keppke et al. (11) reported a median survival of 660 d in 42 patients with Okuda stage I treated with TheraSpheres. Young et al. (12) observed a significant mean cumulative radiation dose of 390 Gy and 196 Gy tolerated by Okuda stage I and II patients, respectively, before the occurrence of toxicity. Kulik et al. (13) showed complete necrosis of HCC nodules (demonstrated on liver explants) in 14 of 21 patients (66%) treated with TheraSpheres and subsequently bridged to liver transplantation.
In a recent study in which 5 patients with unresectable HCC were treated with SIR spheres, all had an initial reduction in α-fetoprotein, which was sustained in 4 patients (14). Sangro et al. (15) achieved partial response or stable disease (response evaluation criteria in solid tumors [RECIST]) in 88% of 24 HCC patients with Child–Pugh score A treated with SIR spheres.
However, there are 2 major caveats to the use of these techniques, as they are essentially embolic in nature: severe liver dysfunction and PVT represent theoretic contraindications, as in TACE. In addition, techniques using 90Y-labeled products tend to cost up to 10 times more than do products with 131I-lipiodol. Recently, Kulik et al. (16) reported on the safety of 90Y in 108 patients with or without PVT. In 34 patients with PVT treated with TheraSpheres, increased bilirubin developed in 40%, ascites developed in 18%, and hepatic encephalopathy developed in 4%; median survival was 304 d. The authors concluded that the microembolic effect of TheraSpheres did not increase the risk of liver-adverse events in patients with PVT (because it did not result in macroembolic effect).
However, the BCLC treatment recommendations suggest that these forms of therapies should be only part of clinical trials (17) because it is felt there is no evidence for their efficacy. However, one of the reasons is the limited published experience, given the poor availability of 131I-lipiodol, although it is a licensed product in many European Union countries. The availability and reliability of supply of 131I-lipiodol is an issue, as production at present occurs only in France. This shortage of supply has resulted in only 1–2 centers per European country offering the therapy and some delays in obtaining the 131I-lipiodol and having the trained staff to administer it safely.
As a strategy to deal with this problem, the International Atomic Energy Agency set up a coordinated research project to develop an on-site labeling system using a tungsten or rhenium generator producing 188Re. This radionuclide has a shorter half-life than 131I but similar β-emissions, allowing the administration of higher initial activities. Both initial results and later follow-up data suggest an efficacy rate for 188Re similar to 131I-lipiodol but a lower cost (18). In a series of 185 patients with unresectable HCC treated across 7 developing nations, the mean overall survival was 256 d. Although the number of patients with PVT was not noted, the authors stated that the presence of cirrhosis, CLIP score, and Child–Pugh score were the best predictors of survival.
In our patients, there was no significant difference in overall survival between patients receiving 131I-lipiodol and those undergoing TACE/TAE treatment, although PVT, a known adverse prognostic factor in HCC, was more frequent in the 131I-lipiodol group. Our results in the TACE/TAE group are comparable to those reported in controlled trials; our results are only slightly worse than the survival rates achieved in the trial by Llovet et al. (19), given that HCC-cirrhotic patients had better or similar liver function (only Child A or B) and tumor stage (only Okuda I or II). The post-TACE survival rate in the Llovet study, compared with our study, was 82% versus 61% at 1 y, respectively, and 63% versus 44% at 2 y, respectively. The post-TAE survival rate in the Llovet study, compared with our study, was 75% versus 63% at 1 y, respectively, and 50% versus 50% at 2 y, respectively.
When considering only patients with PVT, our series showed a significant improvement in survival in patients undergoing 131I-lipiodol therapy (n = 14), compared with TACE/TAE therapy (n = 6). 131I-lipiodol therapy also resulted in a significantly better survival rate in advanced HCC (BCLC stage D), although only a few patients (n = 8) were treated. This may be because 131I-lipiodol, compared with TACE/TAE, was better tolerated (less posttreatment liver dysfunction) (5,7).
As expected from previous studies of HCC using either radionuclides or TACE/TAE, the factors affecting prognosis are related to tumor size, tumor recurrence after transplant (20), tumor multifocality (21), and the stage of the tumor and the overall liver reserve as reflected in the CLIP and Child–Pugh scores and Okuda staging (22–25). Our results suggest that 131I-lipiodol has the most advantage as a therapy when these prognostic factors are at their worst.
The evaluation of response to treatment using either RECIST or WHO criteria (26–28) reflects outcomes in HCC partially due to the problem in identifying where there is viable tumor. Criteria such as residual tumor vascularity have been suggested by the European Association for the Study of the Liver in their 2000 recommendations (17). Functional imaging (29) may be an alternative.
CONCLUSION
Our observations in a consecutive cohort of HCC patients treated either with 131I-lipiodol or with TACE/TAE suggest that 131I-lipiodol may be the preferred transarterial therapy in patients with advanced disease; there was increased survival for the 131I-lipiodol group, compared with the TACE/TAE group. However, in groups without PVT or advanced disease, there was no difference in survival.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 24, 2008.
- Accepted for publication February 27, 2009.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.