


Abstract
Breast cancer is the most common non-skin type of cancer and the second leading cause of cancer mortality in women. Advances in diagnosis and treatment have led to declines in mortality, despite an increase in breast cancer incidence. An advancing array of both local and systemic therapy options has led to increasingly individualized treatment. Imaging plays a key role in detecting breast cancer and directing its therapy. This continuing education article provides a comprehensive review of current and future radiotracer imaging methods applied to breast cancer, in the context of breast cancer management strategies and other nonnuclear imaging methods. Part 1 of the review provided an overview of clinical and biologic considerations in breast cancer and covered radionuclide imaging for detection and staging. Part 2 covers radionuclide imaging of breast cancer response to therapy, other clinical indications for radionuclide breast cancer imaging, and future directions, including molecular imaging.
Breast cancer is the most common non-skin type of cancer and the second leading cause of cancer mortality in women (1). Although its incidence continues to rise, mortality has declined over the past several years (1,2). The decline has been attributed to both early diagnosis and more effective treatment (2). Advances in molecular cancer biology have led to an increased understanding of the biologic factors that contribute to breast cancer pathogenesis and progression. This understanding has already led to new and effective treatments (3), and new targeted therapies continue to be developed and tested (4). Advances in breast cancer molecular biology have also yielded improvements in diagnosis through molecular pathology and molecular imaging (5,6).
Part 1 of this review provided an overview of breast cancer clinical features and biology and reviewed radionuclide imaging for breast cancer detection and staging. Part 2 reviews applications to therapeutic monitoring and other indications such as toxicity monitoring, followed by highlights of future directions, including that of molecular imaging.
RESPONSE TO THERAPY
Overview
A wide range of systemic therapy options for breast cancer exists, and breast cancer is one of the more responsive solid tumors (7). Therefore, the evaluation of response to therapy is an important diagnostic need for breast cancer. Systemic therapy is given in 1 of the 3 following clinical settings: adjuvant (after completion of definitive locoregional surgery to treat residual or metastatic microscopic disease), neoadjuvant (primary systemic therapy given before definitive local surgery), or metastatic (systemic therapy of stage IV disease).
For adjuvant therapy, there should be no residual macroscopic disease after surgery and, therefore, imaging is not helpful for response monitoring, except for restaging when recurrence is suspected. In the neoadjuvant and metastatic settings, imaging plays an important role in evaluating the success of therapy. Size-based criteria using anatomic imaging (mammography or ultrasound in the breast, CT or MRI elsewhere) have traditionally been used to measure response but have some significant limitations in both the neoadjuvant and the metastatic settings (8,9). Functional imaging overcomes many of these limitations and may, therefore, play an increasingly significant role in breast cancer response evaluation.
Neoadjuvant Therapy.
Neoadjuvant (preoperative) systemic therapy has become the standard treatment for patients with locally advanced breast cancer, which is defined as primary breast cancer exceeding 5 cm, fixed axillary lymph nodes, or skin or chest wall invasion (10). Neoadjuvant therapy is increasingly used in patients with operable breast cancer (11). Most neoadjuvant therapy studies have tested cytotoxic chemotherapy regimens; however, neoadjuvant endocrine therapy has been studied (12), and the addition of agents such as trastuzumab to chemotherapy regimens for HER2-overexpressing tumors has increased response rates considerably in appropriately selected patients (13). Although neoadjuvant therapy, compared with similar adjuvant therapy, has not been shown to improve survival it does improve surgical options and provide prognostic information (11). Studies have demonstrated that the extent of residual breast and axillary disease after treatment is prognostic for both disease-free survival and overall survival (8,14,15). Patients demonstrating complete pathologic response (pCR) (defined as no residual invasive tumor on histopathology at posttherapy surgery), compared with patients without pCR, have improved long-term outcome (8,15). One of the primary aims of neoadjuvant therapy is, therefore, to assess the response of the primary tumor to the treatment regimen (16). Sized-based approaches for response evaluation, for example, physical examination and mammography, have not performed well in this setting and have trouble distinguishing pCR from other responses (8,9). This is, therefore, a role in which functional imaging may be particularly helpful.
Studies of 18F-FDG PET comprise the largest body of work on radiotracer imaging for response evaluation to neoadjuvant breast cancer treatment (17–19). Some of the earliest work using 18F-FDG to monitor cancer response was done in this clinical setting (20,21). Serial 18F-FDG PET has been widely studied as a method for assessing tumor response to neoadjuvant chemotherapy, using a comparison to histopathology assessment of response from the postsurgery specimen as the gold standard (17,22). In these studies, 18F-FDG PET scans were obtained before therapy and then at 2 or more time points (early [after a single cycle of therapy], mid-therapy, and after therapy) during the course of neoadjuvant therapy (Fig. 1). The pretherapy scan serves as the baseline to assess future changes in the level of 18F-FDG uptake but is also important in defining the extent of disease that may affect postsurgical treatment, such as radiation therapy, by demonstrating occult nodal or distant metastatic disease (23,24).
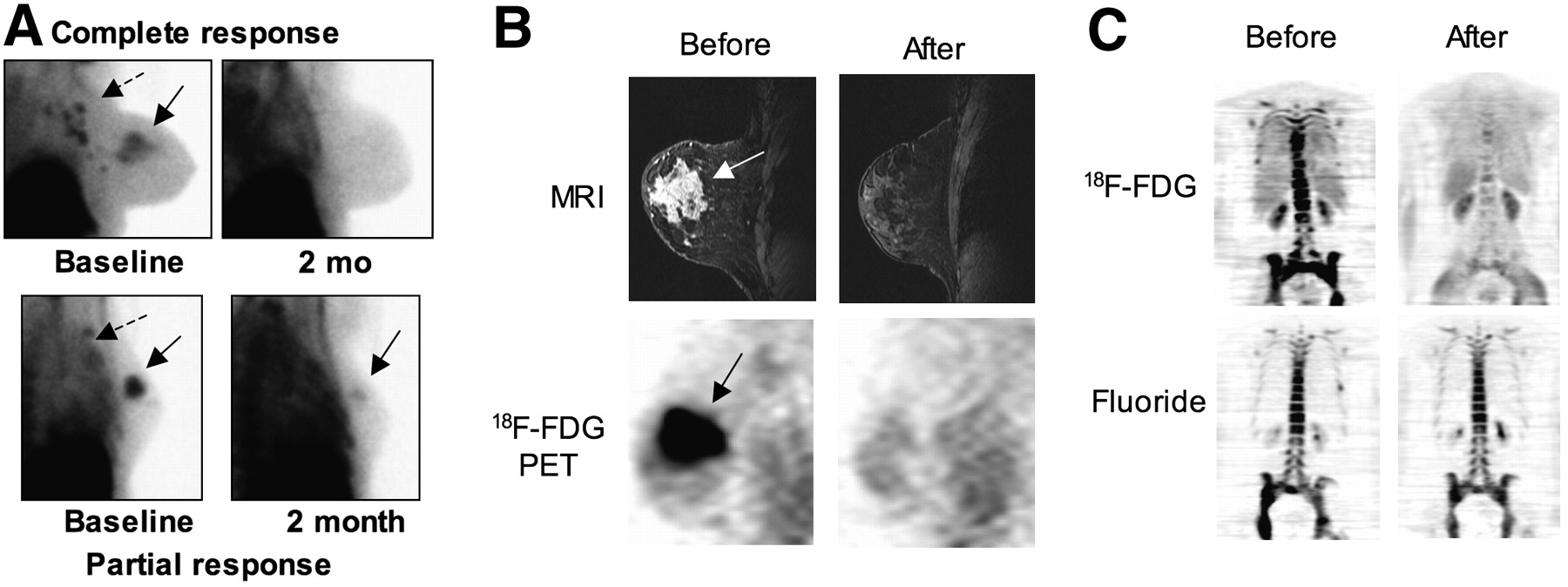
Examples of radiotracer imaging to measure breast cancer response. (A) Prone lateral 99mTc-sestamibi images of patients with locally advanced breast cancer obtained before and after neoadjuvant chemotherapy (left and right columns) for 2 patients (top and bottom row). Primary tumor (solid arrow) and nodal metastases (dashed arrow) are seen. Top patient demonstrated pCR, and bottom patient demonstrated clinical response but had residual tumor at postchemotherapy surgery. (B) Contrast-enhanced breast MR (top) and sagittal 18F-FDG PET images (bottom) of patient with locally advanced breast cancer are shown taken before and after neoadjuvant chemotherapy (left and right columns), focusing on primary tumor (arrow). Patient demonstrated pCR to neoadjuvant chemotherapy as indicated by both MR and PET images after chemotherapy. (Adapted from (31).) (C) Coronal 18F-FDG PET (top) and 18F-fluoride images (bottom) taken before (left) and 4 mo after (right) endocrine therapy of breast cancer widely metastatic to bone with primarily lytic metastases. Patients had excellent clinical response with dramatic reduction in tumor markers and pain. 18F-FDG images show substantial resolution in abnormal uptake. Fluoride images show some change, but to much lesser extent than do 18F-FDG images.
Most studies evaluating 18F-FDG PET to assess response to neoadjuvant therapy have measured change in 18F-FDG uptake at mid-therapy, compared with at baseline, as a measure of response. The results of these studies are summarized in Table 1. One of the earliest studies of 18F-FDG PET to measure response was performed by Wahl et al. (21) and showed significant quantitative differences in the 18F-FDG uptake measured before and after 2 mo of therapy for responders versus nonresponders. Almost all of the subsequent studies reported similar findings and found that a primary tumor 18F-FDG uptake decline by approximately 50% or more was predictive of a good response (17,22). Perhaps more important, lesser declines in 18F-FDG uptake predicted poor response.
Response Evaluation of Breast Cancer Therapy by 18F-FDG PET
Studies evaluating change in 18F-FDG uptake early in the course of therapy suggest that early assessment of response is possible and predictive of subsequent pathologic response (Table 1). Three early studies measuring 18F-FDG uptake after the first cycle of therapy all demonstrated that early 18F-FDG PET predicted final response. In 2 of these, the data suggest that early 18F-FDG PET may demonstrate greater separation between responders and nonresponders than would mid-therapy imaging (21,25,26). More recently, Rousseau et al. (27) found that, using a 60% decrease in baseline SUV as the threshold for response, 18F-FDG PET was 61% sensitive and 96% specific after a single cycle and increased to 89% sensitive and 95% specific after 2 cycles of therapy. Another study by Berriolo-Riedinger reported similar findings (28). These findings suggest that 18F-FDG PET may serve as an early predictor of chemotherapy response and, importantly, as an accurate predictor of lack of response, which is clinically relevant given the increasing number of new medical therapies available for breast cancer.
Studies performed after the completion of chemotherapy have shown that although residual 18F-FDG uptake predicts residual disease, the absence of 18F-FDG uptake is not a reliable indicator of pCR (17,29–31). This is especially true for axillary nodal disease, because the sensitivity for residual microscopic disease after therapy is low. In patients with gross residual disease, posttherapy 18F-FDG PET has been shown to complement MRI to help define the extent of residual breast disease (32). Recent studies have shown that the presence of 18F-FDG uptake after therapy is highly predictive of relapse (33). Therefore, even though 18F-FDG PET may miss small-volume disease after therapy, the presence or absence of 18F-FDG uptake may carry prognostic significance that may be important in directing the intensity of additional therapy and postsurgery surveillance.
Sestamibi imaging has also been used to assess response in the neoadjuvant setting (34,35). Studies have shown the ability of serial sestamibi imaging to discern pCR from other responses (34,35). The use of tumor uptake indices for evaluating changes in sestamibi uptake may be especially useful in this setting (36). Some comparisons of sestamibi and 18F-FDG PET to measure response have shown sestamibi to be similarly, and perhaps more, predictive of pathologic response (37). More recent studies have shown that, although sestamibi uptake after therapy may underestimate tumor extent (38), changes in sestamibi uptake with treatment and residual uptake after therapy predict relapse and survival (39). Comparative studies of sestamibi and PET blood flow measurements (40) suggest that the correspondence between sestamibi uptake and tumor blood flow may be the basis for response evaluation, and the similarity of sestamibi outcome data and PET blood flow data (39,41) supports this premise. Some studies have shown that serial sestamibi can measure response early after the start of treatment (42); however, some other studies have not supported these findings (43). Despite these successes, serial sestamibi imaging has not seen widespread use in the neoadjuvant setting; the infrequent use of sestamibi may be because, of the radiotracer methods, 18F-FDG PET also provides staging information (which is important for many neoadjuvantly treated breast cancer patients).
Studies have also investigated sestamibi uptake and washout as a predictor of multidrug resistance mediated by P-glycoprotein (44). Some studies have shown that the rate of sestamibi washout before therapy, as an index of multidrug resistance, is predictive of response (45,46). Other studies have not supported the predictive value of sestamibi uptake indices (47,48). Some of the difference may be because both delivery (i.e., tumor blood flow) and retention contribute to sestamibi uptake and washout and may confound interpretation of sestamibi images for predicting drug transport (40). Ongoing work with PET probes of P-glycoprotein function in breast cancer may help in this regard (49,50).
Other functional imaging modalities have been used to evaluate breast cancer response in the neoadjuvant setting, including PET with other radiopharmaceuticals, Doppler ultrasound (51), breast MRI, breast magnetic resonance spectroscopy (MRS) (52,53), and optical imaging (54). Among these functional imaging modalities, contrast-enhanced MRI is the most widely used in clinical practice (55). Studies have shown that MRI, 18F-FDG PET, and sestamibi are similarly accurate in measuring response; however, MRI provides a detailed anatomic picture of the extent of disease, important for surgical planning after therapy (55). Some studies also suggest that changes in MRI provide prognostic information similar to that provided by 18F-FDG PET and sestamibi (56). Preliminary studies combining MRI and 18F-FDG PET have been promising in predicting response and delineating the extent of residual disease (32,57). Data suggest a correspondence between MRI and PET measures of tumor perfusion but not 18F-FDG PET measures of metabolism (58), and studies suggest that the 2 modalities provide complementary information on tumor biology (57). MRS has demonstrated an ability to measure early response to therapy (59) similar to that of 18F-FDG PET (60).
A particularly intriguing application of 18F-FDG to breast cancer treatment is as a pharmacodynamic measure of response for targeted therapy, to help predict the efficacy of targeted therapy. 18F-FDG PET may provide an early indication of biologic changes in response to targeted therapy that may indicate that the chosen drug has successfully hit the target and, perhaps more important, indicate when the targeted therapy has not impacted the cancer. Dehdashti et al. used 18F-FDG PET as an early indicator of the effect of endocrine therapy (61,62). In these studies, serial 18F-FDG PET showed that an increase in uptake in response to an estrogen receptor (ER) agonist, either the agonist flare of tamoxifen (62) or an estradiol challenge (61), predicted response and time to progression. Early studies also support the ability of serial 18F-FDG PET to measure response to lapatinib, a HER2-targeted agent (63). These studies indicate a potential of PET to identify early response to targeted therapy and merit further study.
Metastatic Disease.
Radiotracer imaging methods have also been used to evaluate the response of stage IV, metastatic breast cancer (MBC), to therapy; however, fewer studies have been performed in this area than in others. The standard approach for response evaluation for MBC relies on changes in tumor size, typically using standard criteria such as Response Evaluation Criteria in Solid Tumors (RECIST) (64,65) and anatomic imaging, mostly CT. This approach works well for some sites of metastatic disease such as the liver and lungs. However, for other sites of disease, size-based criteria are problematic. This is true for regional nodal disease, in which the often small size of the lesion and tissue distortion from prior surgery or radiotherapy can make size-based response assessment challenging. Bone, a common site of breast cancer metastases, poses particular challenges (66). These are areas in which functional radionuclide imaging can provide clinically relevant and important data for response assessment.
Although other radiotracer imaging approaches have been useful for evaluating primary tumor response, only 18F-FDG PET has seen widespread use for response evaluation of MBC. Several relatively small studies have been conducted evaluating serial 18F-FDG PET for measuring MBC response to treatment. Most studies showed, similar to neoadjuvant therapy, that response is accompanied by substantial drops in 18F-FDG uptake, typically 40%−50% or more from the pretherapy baselines (67–69). Some studies suggested that imaging as early as after 1 cycle of chemotherapy could predict response (69), akin to the neoadjuvant therapy setting. However, other studies have not shown similar accuracy for early repeated 18F-FDG PET (67). The level of 18F-FDG uptake after therapy has also been shown to be predictive. The study by Cachin et al. (70), similar to findings in the neoadjuvant setting, showed that the persistence of 18F-FDG uptake after therapy for patients undergoing high-dose chemotherapy predicted a significantly poorer outcome than did absence of abnormal uptake after therapy (i.e., for those patients who achieved a complete metabolic response).
A particularly vexing clinical problem for breast cancer clinicians is the evaluation of response of bone metastases (66). The size of many bony lesions is difficult to estimate and may not necessarily change with response. Bone metastases are, therefore, not considered evaluable for response by RECIST criteria (64). Bone scintigraphy continues to be an excellent tool for bone metastasis detection but is problematic for response evaluation. Changes in the bone scan significantly lag bone metastasis response and may even transiently worsen or “flare” in response to successful therapy (71,72). The flare phenomenon has been attributed to an increased uptake of diphosphonates that accompanies healing of the surrounding bone as the tumor is successfully treated, particularly for more lytic metastases (66). On the basis of molecular analyses, approximately 80% of bone metastases are primarily lytic (73). Even in the absence of an overt worsening or flare, the healing response likely contributes to the lag in bone scan changes after successful treatment. Fluoride PET, because it images bone metastases through a mechanism similar to bone scintigraphy, may yield comparable results. Preliminary results support this premise. A fluoride PET flare response has been reported (74), and early studies suggested that although fluoride PET provided quantitative information and interesting insights into physiologic changes in response to treatment, uptake did not change significantly with treatment (75).
The differences seen between bone scintigraphy and 18F-FDG PET for bone metastases (76) led some investigators to hypothesize that 18F-FDG PET might provide a useful and accurate means for assessing bone metastasis response. Specifically, although imaging such as CT, MRI, and bone scintigraphy rely on changes in the normal bone to identify tumors, 18F-FDG PET might image hypermetabolism in the tumor itself and therefore provide useful information. Early studies supported this hypothesis. Stafford et al. (77) showed that changes in PET uptake correlated with the clinical assessment of response in bone-dominant MBC and, furthermore, that changes in 18F-FDG uptake correlated with changes in breast cancer tumor markers, which are used clinically to assess bone metastasis response. A follow-up report (78) showed that changes in 18F-FDG uptake predicted time to progression, a more robust clinical endpoint than response, and that the level of 18F-FDG predicted the likelihood of a skeletal event, perhaps as an index of the lytic nature of the bony lesions. Recent studies using 18F-FDG PET/CT showed similar findings and also showed that correlative changes in CT—in particular, increased sclerosis associated with response to treatment—could provide important complementary information to PET (79,80). The study by Tateishi et al. (80) also showed that both metabolic and structural changes on 18F-FDG PET/CT predicted bone metastasis time to progression. In interpreting 18F-PET studies to evaluate bone metastasis response, it is important to recognize that although an absence of uptake after therapy indicates a good response to treatment and favorable prediction for time to progression, it does not indicate an absence of disease. Examples showed that disease recurrence on PET occurred in sites of previously noted disease shortly after changing therapy, despite an absence of uptake before changing therapy (77). Nevertheless, the application of 18F-FDG PET/CT to bone metastasis response represents an important and clinically relevant application to breast cancer that is currently underutilized.
Some other newer imaging methods have also shown promise for evaluating breast cancer bone metastasis response. Early studies of diffusion MRI have shown promise as a method for response evaluation (81). Prospective, multicenter clinical trials are needed for 18F-FDG PET/CT or diffusion MRI to validate their efficacy as methods for evalzuating bone metastasis response, enable their more widespread clinical trial participation, and improve clinical management for patients with bone-dominant breast cancer.
OTHER INDICATIONS AND FUTURE DIRECTIONS
Toxicity Monitoring
Methods commonly used in nuclear medicine play a role in toxicity monitoring for breast cancer patients. Some chemotherapy agents (e.g., doxorubicin) and, more recently, some targeted biologic agents such as trastuzumab can have significant cardiac toxicity (82). Periodic measurement of ejection fraction is needed to screen for cardiotoxicity in advance of overt symptoms of heart failure, especially for drugs such as doxorubicin, in which dysfunction is typically not reversible (82). Both radionuclide ventriculogram and echocardiography are used for the measurement of ejection fraction for monitoring cardiotoxicity. Studies suggest that radionuclide ventriculography is less operator-dependent and more precise and therefore able to detect small decrements more reliably (83). Echocardiography involves neither radiation nor the need for blood labeling and injection. In practice, both methods are used, with the choice largely depending on institutional preference.
Osteoporosis is an increasingly common consequence of breast cancer systemic treatments, especially the aromatase inhibitors (84). Bisphosphonates are increasingly used to prevent osteoporosis in many patients, to limit progression in patients with bone metastases, and possibly as adjuvant therapy in patients with high-risk, nonmetastatic disease (85). Monitoring bone mineral density as an index of treatment effect on normal bone is important and is commonly performed using dual-energy x-ray absorptiometry (85).
Prognostic Indicators
Predicting tumor behavior, and in particular the likelihood of cancer relapse or progression, is an increasingly important part of directing breast cancer therapy and is traditionally done by in vitro assay of tumor biopsy material. Early data suggest that parameters from radiotracer imaging may also carry prognostic information for breast cancer. Oshida (86) showed that the level of uptake in the primary tumor was predictive of disease-free survival. Other studies showed that the patterns of perfusion, measured by PET or MRI, and kinetics of 18F-FDG uptake were prognostically significant (41,57,87). Although it is unlikely that one would perform MRI or PET solely to gather prognostic information, such information may be readily available from scans obtained for staging or response evaluation and, therefore, merits further investigation.
Future Directions: Molecular Imaging
As breast cancer treatment becomes increasingly targeted and individualized, demands on breast cancer diagnosis to help direct the therapeutic approach will increase. The imaging approaches in current clinical use for diagnosing and staging breast cancer—mammography, ultrasound, contrast-enhanced MRI, CT, bone scanning, and 18F-FDG PET/CT—provide important information on disease extent and response to treatment but are relatively nonspecific. More specific functional and molecular imaging methods, discussed below, are poised to provide the kind of diagnostic data that are needed to help take advantage of progress in our understanding of breast cancer biology and new therapeutic options. Selected examples of molecular and functional approaches include tumor perfusion and angiogenesis imaging, tumor receptor imaging, and novel approaches to early response to treatment imaging.
Tumor Perfusion and Angiogenesis Imaging.
Tumor vascularity has been recognized as being important in cancer growth and metastasis and in the systemic delivery of therapeutic agents (88). Antiangiogenic agents such as bevacizumab are now used as part of U.S. Food and Drug Administration–approved breast cancer treatments (89). For these reasons, the ability to image and quantify tumor perfusion and neovasculature is a clinically important need (90). Tumor perfusion is one of the earliest physiologic properties to be measured, and advances in methodology have led to increasingly quantitative approaches. The most physiologically robust and quantitative measures of tumor blood flow use freely diffusible imaging probes. With this approach, blood flow can be inferred from the time course of probe uptake and washout using methods developed and validated for measuring cerebral blood flow (91). One example is the use of 15O-water to measure tumor blood flow by PET, which yields measures of tumor blood flow in mL/min/g (92). 15O-water PET has been shown to yield reliable estimates of tumor blood flow for breast cancer (92,93). Recent studies have shown that serial measures of breast cancer perfusion by water PET in the neoadjuvant setting are highly predictive of response and survival (41,94).
Some studies have suggested that dynamic 18F-FDG PET and kinetic analysis may yield estimates of tumor perfusion, inferred from the 18F-FDG delivery (K1) kinetic parameter, comparable to 15O-water PET (95–97). Studies have shown that this parameter is predictive of response (96), and recent studies have suggested that changes in 18F-FDG K1 with therapy in the neoadjuvant setting are comparable to changes in perfusion from 15O-water in ability to predict response and survival (41). Thus, it may be possible to obtain information from dynamic 18F-FDG PET on both tumor perfusion and metabolism that is clinically predictive. This approach, therefore, merits further investigation.
Perhaps the mostly widely used approach to measure tumor perfusion in clinical practice is dynamic contrast-enhanced (DCE) MRI. Considerable effort has been devoted to the quantification of tumor perfusion and tumor capillary permeability using radiographic and MRI contrast agents (98,99). These agents have somewhat limited permeability across capillaries; therefore, their in vivo kinetics is dependent on both blood flow and capillary permeability. Increasingly sophisticated image acquisition and analysis methods—for breast DCE MRI, in particular—have led to the ability to measure regional breast cancer perfusion and capillary permeability in both animal models and patients (100). These methods have been applied in early trials of antiangiogenic breast cancer therapy and have yielded insights into the nature of response (101). Standardized methods for DCE MRI for clinical trials have been proposed (102).
Other approaches to measuring breast cancer perfusion include Doppler ultrasound (51) and optical imaging (54).
Although tumor perfusion imaging measures the physiologic consequences of angiogenesis, perfusion is not specific to tumor neovessels and is influenced by physiologic parameters not necessarily related to tumor angiogenesis (88). Targeted imaging probes can noninvasively and specifically assess tumor neovasculature. PET probes based on labeled peptides that bind specifically to integrins expressed in neovessels have been studied in animals and tested in humans (103). MRI probes have been developed and are at an earlier stage of testing (98). Such agents may be especially helpful for therapies directed at tumor neovasculature, such as bevacizumab.
The combination of tumor perfusion and metabolism imaging may yield further insights. Studies have shown that unlike in normal tissues, the relationship between breast cancer metabolism and perfusion measured by 18F-FDG and water PET (Fig. 2) or by PET and MRI (57,96,97,104,105) varies considerably. Studies have shown that the relationship between metabolism and perfusion is predictive of therapeutic response and patient outcome (41,57,105). An imbalance between metabolism and perfusion, indicated by high metabolism relative to perfusion, is associated with poor response and early relapse. More study of the biologic mechanism underlying these findings may yield insight into these striking results.
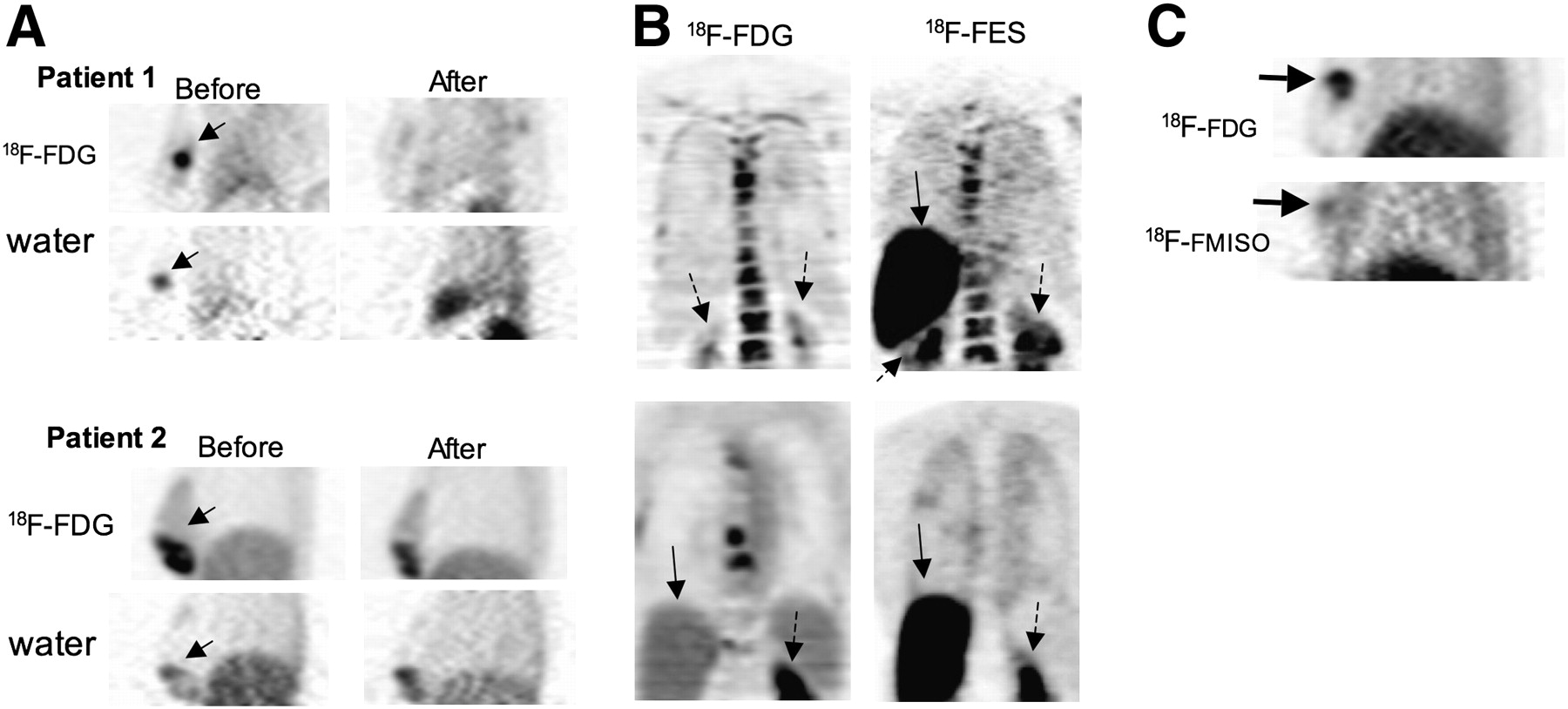
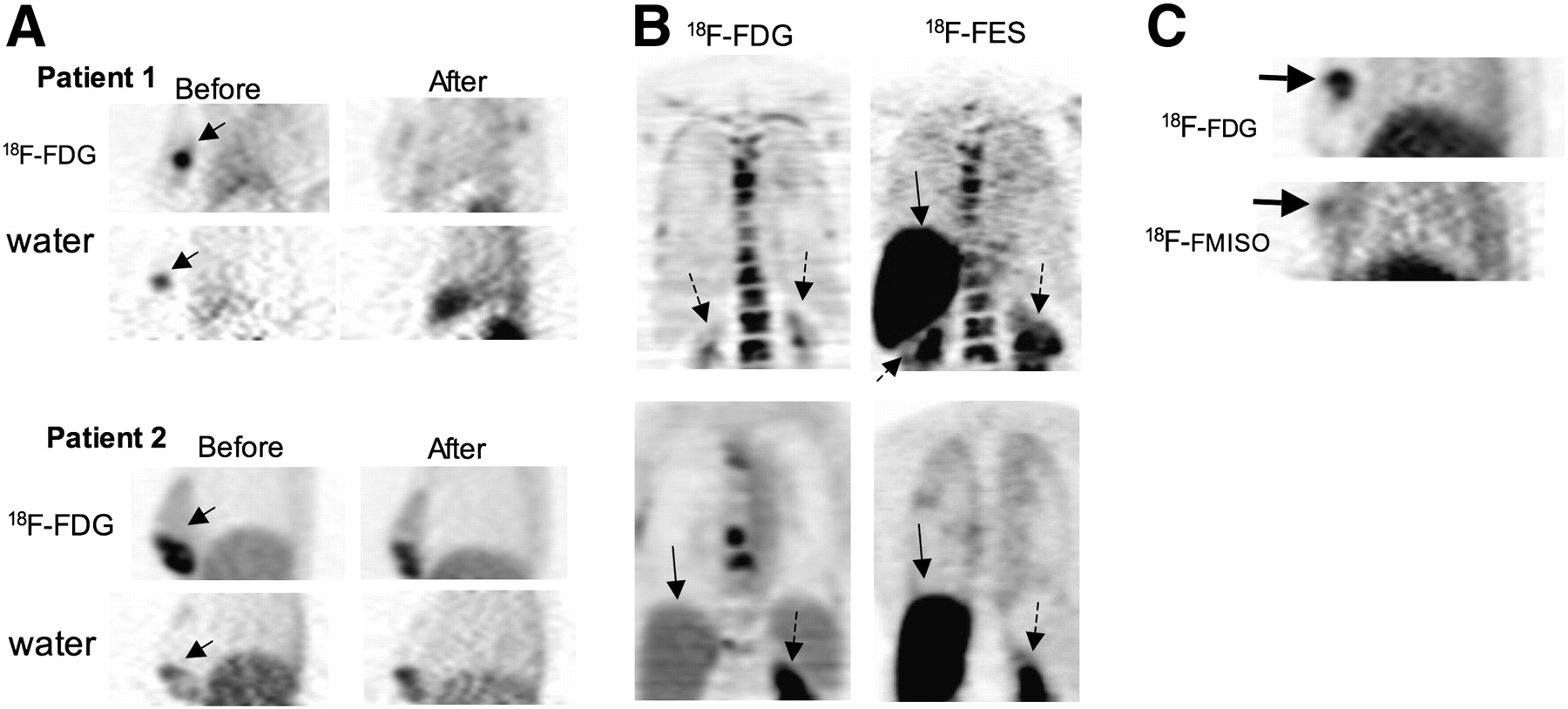
Examples of functional and molecular imaging of breast cancer. (A) Sagittal PET images are shown for 2 patients with breast cancer, imaged before and after neoadjuvant chemotherapy using 18F-FDG PET to measure tumor metabolism (top rows) and 15O-water PET to measure tumor perfusion (bottom rows). Patient 1 demonstrated pCR to chemotherapy, and patient 2 had significant residual disease at posttreatment surgery. Of interest, pretherapy metabolism and perfusion were well matched for patient 1, whereas metabolism and perfusion were both globally and regionally mismatched for patient 2, who had a poor response. (B) Coronal images are shown for 2 patients using 18F-FDG PET to identify active disease and 18F-FES to indicate ER expression. Both patients had extensive bony metastases arising from an ER-positive primary tumor. However, whereas 18F-FES PET showed that the patient had preserved ER expression in metastases, the absence of uptake for the patient in the bottom row suggests loss of ER expression. The patient in the top row responded to endocrine therapy; the patient in the bottom row did not. Normal liver (solid arrow) and kidney (dashed arrow) are indicated. (C) Sagittal images are shown from patient with locally advanced breast cancer (arrows) for 18F-FDG PET and 18F-fluoromisonidazole to indicate tumor hypoxia. Images suggested that inner core of the breast lesion was hypoxic. Patient demonstrated substantial clinical response to chemotherapy, but macroscopic viable tumor was found at postchemotherapy surgery. 18F-MISO = 18F-fluoromisonidazole.
Tumor Receptor Imaging.
The ability to measure the expression of specific proteins that are gene products associated with breast cancer has led to important advances in breast cancer treatment. The ability to image tumor receptors and proteins involved in extracellular signaling is particularly relevant to breast cancer treatment and includes the expression of ERs, a target for endocrine therapy (106), and HER2, also increasingly a target of tumor-specific treatment (3). Tumor receptors are measured by in vitro assay of biopsy material (107). Complementary advantages of imaging to measure receptor expression include its noninvasiveness, the ability to measure receptor expression in the entire disease burden (and thus the ability to avoid sampling error that can occur with heterogeneous receptor expression), and the potential for serial studies of in vivo drug effects on the target. A practical consideration is that imaging can assess receptor expression at sites that are challenging to sample and assay, for example, bone metastases, in which decalcification can make assay of tumor gene products challenging.
The imaging of tumor receptors poses some unique challenges (108). Even small molar quantities of the imaging agent may saturate the receptor and limit the ability to visualize receptor expression (109,110); thus, molecular imaging of tumor receptors has been most successful to date with radionuclide imaging, PET, and SPECT, with which it is possible to generate images with nanomolar or picomolar amounts of the imaging probe. For larger molecules, such as peptides and monoclonal antibodies, other labels suitable for optical imaging, MRI, and ultrasound imaging are possible (108); however, for small-molecule receptor imaging agents, such as labeled steroids for steroid receptors, radionuclide imaging appears to be the only feasible approach.
The most work to date for breast cancer tumor receptor imaging has been done for steroid receptors (108,111). Considerable efforts have gone into the development of radiopharmaceuticals for ER imaging (108,111). Although a variety of ER imaging agents have been tested, and continue to be developed and tested, the most successful ER imaging radiopharmaceutical to date is 16-α-18F-fluoro-17-β-estradiol (18F-FES) (110). This radiopharmaceutical can be synthesized with sufficient specific activity that high-quality patient images can be made with injections of less than 5 μg of FES (Fig. 2). Regional estrogen binding is readily quantified by FES PET, and FES uptake has been validated as a measure of ER expression in breast tumors against ER expression assay of tissue samples by radioligand binding (112) and immunohistochemistry (113). FES uptake is readily visualized and quantified in primary and metastatic breast cancer (114) and can identify heterogeneous ER expression, for example, loss of ER expression in metastases arising from ER-expressing primary tumors (114,115). The level of FES uptake has been shown to be predictive of response to endocrine therapy (62,115), including heavily pretreated patients. Serial FES PET can also measure the pharmacodynamic effect of drugs on estradiol binding to the ER, yielding insights into determinants of drug efficacy (108).
Somatostatin receptor imaging of breast cancer using labeled peptides has also been studied (116,117). Although not a direct target or breast cancer therapy, somatostatin receptor expression measured by the uptake of labeled probes has been shown to be predictive of response to ER-directed therapy (117). A variety of other receptor agents has also been tested (108).
HER2 (ErbB2) expression in breast cancer has become an important indicator of prognosis and an increasingly important target for therapy (118). Recent efforts have focused on imaging HER2 expression in breast cancer. The most success and largest number of studies to date used imaging probes based on immune recognition to image HER2 expression. Specific imaging probes based on radiolabeled antibodies or fragments, or novel constructs such as affibodies, have shown success in early studies (108). Studies using a 68Ga-labeled F(ab′)2 fragment of trastuzumab (119) demonstrated the feasibility of measuring regional HER2 expression in murine animal models. The imaging results nicely demonstrated alterations in HER2 expression accompanying experimental therapy using heat shock protein 90–directed agents (geldamycin analogs) to disrupt protein chaperoning and reduce HER2 expression (119). Studies using 131I- or 111In-labeled trastuzumab have demonstrated the ability to image tumor expression of HER2 and tumor and normal tissue accumulation of trastuzumab (120,121), although there has been some controversy about the significance of uptake in normal tissues prone to trastuzumab toxicity, such as the heart (120,121). Promising early patient studies have also been presented for 89Zr-labeled trastuzumab (122).
Early Response Imaging.
Studies of 18F-FDG PET have shown that tumor glycolysis declines early in the course of treatment (25–27), providing a means for early response assessment. However, other pathways more closely tied to cellular growth and death may provide even earlier and more specific indications of therapeutic response. Imaging targets include protein and membrane lipid synthesis, cellular proliferation, and cell death or apoptosis.
Several methods have addressed tumor biosynthesis as an indicator of tumor growth, with approaches targeted to protein synthesis and membrane synthesis. The uptake of labeled amino acids, such as 11C-methionine, has been shown to correlate with tumor growth, and changes in uptake provide an early indication of breast cancer response to therapy (123). This approach, however, is limited by the complex nature of amino acid metabolism pathways, making it difficult to measure protein synthetic rate versus amino acid transport and metabolism (124). Artificial amino acids have also been tested as indicators of amino acid transport (125).
Proliferating tumor cells also engage in enhanced lipid biosynthesis to provide the building blocks needed for cellular membranes (126). This process can also be assayed through molecular imaging using several different methods. Spurred by results in brain tumor imaging (127), MRS studies of breast cancer have shown increased choline pool sizes to be a feature of breast malignancy (52,128). Interestingly, changes in the choline concentration measured by MRS early in treatment appear to be a marker for early response to therapy, as early as 24 h after treatment with chemotherapy (59). These exciting early findings are now being tested in a large prospective cooperative group trial. Lipid metabolism can also be studied by PET using either 11C- or 18F-labeled choline or 11C-acetate (129), which enters lipid synthesis from the tricarboxylic acid cycle via fatty acid synthase. Fatty acid synthase has been shown to have increased activity and expression in cancer and may be a target for therapy (130). This approach has shown considerable promise in other tumors such as prostate cancer (131), including therapeutic response (132), but has not been applied to the same extent to breast cancer (133).
Aberrant cellular proliferation is a fundamental property of cancer, including breast cancer (134). Labeled compounds such as 14C- or 3H-thymidine have been an important method for measuring cellular proliferation through tissue sampling, dating back more than 40 years (135). Assay of breast tissue for cellular proliferation, typically by assay of MIB-1 (Ki-67) (136), is routinely performed in many centers. Early work used PET and 11C-thymidine to measure tumor proliferation by imaging, and quantitative imaging approaches were validated against in vitro assay gold standards (137). However, the short half-life of 11C (20 min) and the extensive in vivo metabolism of thymidine limit the feasibility of this approach for both animal and patient imaging. Thymidine analogs labeled with 18F (half-life, 109 min) have been developed and undergone considerable study in recent years (137,138). The most promising of these had been 18F-fluorothymidine (18F-FLT), with notable recent results for both animal and patient breast cancer imaging (139–142). 18F-FLT PET appears especially promising for measuring the early effects of therapy on breast cancer growth, as suggested by recent studies (140,141) that showed the ability of serial 18F-FLT PET to identify early responders, and importantly, nonresponders. This is an exciting area of imaging research and likely to be of clinical importance in the future.
Cell death, or apoptosis, is a fundamental part of normal cellular physiology and an early indicator of therapeutic response (143). Methods for imaging cell death have been investigated. Many of these have been based on an extension of annexin V staining in vitro, which indicates apoptotic cells through binding to phosphatidylserines (144). The molecules are found only on the inner surface of plasma membranes and therefore normally not accessible to annexin V, a peptide, for binding. However, during apoptosis, these molecules are transiently exposed to the extracellular space, allowing binding of annexin (144). The earliest studies used 99mTc-annexin and SPECT to measure apoptosis in animal models and patients (144,145). More recently, methods for annexin-based apoptosis imaging have been developed for PET, MRI, optical imaging, and ultrasound imaging (146). One limitation of this approach has been the transient nature of phosphatidylserine exposure during cell death, resulting in a fairly limited signal for imaging (147). Other approaches targeted to different aspects of the apoptotic cascade are being investigated (146). An alternative but less specific approach has been to use MRI measures of water diffusion through the extracellular space as an indirect measure of tumor cellularity (148,149). Increases in the diffusion coefficient, as an indicator of a decrease in tumor cellularity, have correlated with measures of apoptosis in animal models (148) and response to therapy in early patient studies (81,149). This method has the advantage of being available using existing MRI instrumentation for both animal and patient imaging, without the need for imaging probes, but provides a relatively indirect measure of cell death.
CONCLUSION
Breast cancer is a common disorder in women and a leading cause of death. Imaging plays an important role in the detection, diagnosis, staging, and response evaluation of breast cancer. Radiotracer imaging methods play an important current role in breast cancer staging and response evaluation, including sentinel node lymphatic mapping, bone scintigraphy, and 18F-FDG PET/CT. Ongoing trials of dedicated devices for primary tumor imaging using breast-dedicated PET and SPECT may lead to the increased use for primary tumor diagnosis and determination of the extent of disease in the breast. However, more studies are needed. As breast cancer diagnosis and therapy become increasingly molecular and individualized, molecular breast cancer imaging will play a progressively more important role in breast cancer patient care. Radiotracer molecular imaging methods have already been shown to be accurate and helpful in directing the treatment of breast cancer. Future clinical trials will validate these methods and test their value in directing breast cancer treatment. Current practice and early experimental results suggest that radiotracer imaging will play an increasingly important role in the care of breast cancer patients in the future.
Acknowledgments
We acknowledge the help of Erin Schubert, Lisa Dunnwald, and Lanell Peterson with capturing the images used in the figures and the support of the molecular imaging and breast cancer groups at the University of Washington and Seattle Cancer Care Alliance. This work was supported in part by NIH grants CA42045, CA72064, CA90771, and CA124573.
Footnotes
-
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH MAY 2010.
-
David Mankoff has indicated he receives scientific study/trial support from Pfizer and GE Healthcare. No other potential conflict of interest relevant to this article was reported.
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- Received for publication December 17, 2008.
- Accepted for publication December 29, 2008.
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Bridge Not Too Far: Linking Disciplines Through Molecular Imaging Probes
- Complexity of Response Evaluation During Primary Systemic Therapy of Breast Cancer: Scoring Systems and Beyond-Preliminary Results
- Breast Imaging Devices for Nuclear Medicine
- PET Tumor Metabolism in Locally Advanced Breast Cancer Patients Undergoing Neoadjuvant Chemotherapy: Value of Static versus Kinetic Measures of Fluorodeoxyglucose Uptake
- A Bridge Not Too Far: Linking Disciplines Through Molecular Imaging Probes