


Abstract
The prognostic power of myocardial perfusion imaging in patients with ischemic heart disease (IHD) has been demonstrated since planar imaging. We aimed to investigate whether gated SPECT retains this value in current cardiology if compared with a complete diagnostic work-up and with more recent prognostic indicators. Methods: We selected from our database a cohort of 676 consecutive inpatients who underwent a complete diagnostic work-up that included gated SPECT and coronary arteriography for known or suspected IHD. Patients with acute myocardial infarction (MI), previous coronary artery bypass surgery, or overt hyperthyroidism and patients who were undergoing dialysis treatment were excluded. During follow-up (median, 37 mo), 24 patients died from cardiac causes and 19 experienced a nonfatal MI. Results: The following were determined to be independent predictors of event-free survival (cardiac death and nonfatal MI) in the different phases of diagnostic work-up using Cox proportional hazards regression analysis: among clinical variables, a previous MI; among laboratory examinations, serum creatinine and low-density lipoprotein (LDL) and high-density lipoprotein (HDL) cholesterol levels; among electrocardiographic and echocardiographic variables, left ventricular ejection fraction; and among SPECT variables, summed rest score (SRS) and summed difference score (SDS). In addition, a score of coronary stenoses at angiography was an independent predictor. When the above predictors were tested together, SRS (P < 0.0001), SDS (P = 0.0108), and serum creatinine (P = 0.0186) and LDL and HDL cholesterol levels (P = 0.0222) were the final independent predictors of event-free survival. When gated SPECT was added to the clinical, laboratory, electrocardiographic, and echocardiographic variables, the prognostic stratification significantly improved (P < 0.05); when coronary arteriography was added to gated SPECT, prognostic stratification did not further improve (P > 0.25). If the information provided by gated SPECT was made available after clinical, laboratory, electrocardiographic, echocardiographic, and angiographic variables, the prognostic stratification still improved significantly (P < 0.05). In 492 of these patients with ascertained IHD, SRS and SDS were the final independent predictors of survival. Medical treatment and coronary revascularization did not affect the prognostic information of gated SPECT. Conclusion: Myocardial perfusion abnormalities at rest and after stress are still the best predictors of cardiac event–free survival in patients with known or suspected IHD, even when compared with an extensive diagnostic work-up.
The prognostic value of stress testing with myocardial perfusion imaging has been established since the initial studies with 201Tl, in which extent and severity of myocardial hypoperfusion were shown to be independent predictors of prognosis in patients with known or suspected ischemic heart disease (IHD) (1–3). In addition, thallium imaging, compared with clinical and exercise stress test data, provided further prognostic information, and the combination of the above variables provided more prognostic information than did the combination of clinical and angiographic data (4,5).
However, substantial changes in nuclear cardiology have taken place over the past 2 decades, leading to improved techniques. Thus, SPECT has replaced planar imaging (6,7), and technetium-based imaging agents have been largely used as an alternative to 201Tl (8). The addition of gating to myocardial perfusion imaging has further improved diagnostic accuracy (9) and quantitative analysis of digital data (10). Meanwhile, the prognostic power of 2-dimensional echocardiography in IHD patients has been demonstrated both at rest and after stress (11,12). Furthermore, several laboratory examinations were shown to stratify the risk of cardiac patients; these variables included serum creatinine (13), triiodothyronine levels and indicators of a mild thyroid dysfunction (14), serum cholesterol and its fractions (15), C-reactive protein (16), and cardiac peptides (17). In parallel, great changes have also taken place in clinical cardiology, including secondary prevention, improved medical treatment, percutaneous coronary interventions, and surgical procedures. Because of these interventions, the clinical profile of patients with IHD has changed, and commonly treated patients are now older and affected by greater comorbidity than in the past (18).
With these considerations in mind, we sought to investigate whether gated SPECT with technetium-based imaging agents still preserves its prognostic value in current cardiology when compared with a complete diagnostic work-up and with more recent prognostic indicators.
MATERIALS AND METHODS
Patients
Starting in 2000, we adopted a fully computerized clinical report that allowed handling and recording of the clinical and administrative data of all patients admitted. From this database, we retrospectively selected a group of consecutive patients admitted for known or suspected IHD who had undergone a complete diagnostic work-up that included stress/rest myocardial perfusion imaging and coronary arteriography. Patients with acute or recent ST segment elevation myocardial infarction (MI), previous coronary artery bypass graft surgery, chronic renal failure under dialysis treatment, or primary overt hyperthyroidism (free triiodothyronine level > 420 pg/dL or free thyroxine level > 1.85 ng/dL, with an undetectable thyrotropin level) were excluded from the study. Thus, a study cohort of 676 patients was selected; patient characteristics are shown in Tables 1 and 2.
Clinical Characteristics of Patients (n = 676)
Angiographic and Scintigraphic Characteristics of Patients (n = 676)
At hospital discharge, 492 of these patients (73%) were affected by IHD. In 479 patients, the diagnosis was based on the angiographic evidence of coronary stenoses in at least 1 of the major coronary arteries or secondary branches. In 13 patients with normal coronary arteries, the diagnosis was based on the evidence of a previous MI (documented by clinical records, 8 patients) or on the recording of electrocardiographic patterns of Prinzmetal angina (collected during hospitalization, 5 patients). The 184 patients with normal coronary arteries in whom the suspicion of IHD was not confirmed were affected by dilated cardiomyopathy or myocarditis (60 patients), syndrome X (77 patients), or valvular heart disease (8 patients). The remaining 39 subjects were unaffected by disease.
Diagnostic Work-up
The diagnostic work-up included clinical evaluation, laboratory tests, 12-lead electrocardiography (ECG), 2-dimensional echocardiography, stress/rest gated SPECT, and coronary arteriography. Gated SPECT was performed before coronary arteriography in 623 patients (92%) and after arteriography in the remaining 53 patients (8%). The time interval between gated SPECT and coronary angiography was 11 ± 4 d (range, 1–19 d). Patients experiencing cardiac events during this time were excluded from the study.
Clinical Examination.
The clinical variables explored were patient age, sex, and history of angina (at rest, on effort, or mixed); previous MI; and cardiovascular risk factors. The latter included having a family history of premature IHD (before age 55 y if male, 65 y if female), diabetes mellitus (fasting glucose levels ≥ 126 mg/dL on 2 occasions or need for oral hypoglycemic or insulin agents) (19), arterial hypertension (systolic blood pressure ≥ 140 mm Hg, diastolic blood pressure > 90 mm Hg, or use of an antihypertensive drug) (20), hypercholesterolemia (total cholesterol ≥ 200 mg/dL or use of a lipid-lowering drug) (21), hypertriglyceridemia (triglycerides ≥ 150 mg/dL), and obesity (body mass index ≥ 30 kg/m2) (22) and being a current or former smoker (within the last year).
Laboratory Examinations.
The laboratory variables explored were erythrocyte sedimentation rate; fasting glucose, serum creatinine, total cholesterol, and high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol levels; triglycerides; lipoprotein (a); thyrotropin; free triiodothyronine; free thyroxine; C-reactive protein; and fibrinogen.
Electrocardiographic Data.
The electrocardiographic variables examined were 12-lead ECG results (normal or abnormal), bicycle exercise stress test results (negative or positive, if ST segment depression ≥ 0.15 mV), having undergone or not the exercise stress test, and maximal workload on effort (watts).
Echocardiographic Data.
Two-dimensional echocardiographic variables were left ventricular ejection fraction (LVEF), left ventricular (LV) end-diastolic diameter, wall motion score index, and end-diastolic thickness of the interventricular septum and posterior wall. LVEF was measured by the single-plane Simpson rule; in the case of geometrically distorted ventricles or LV regional wall motion abnormalities, the EF was measured by the biplane Simpson rule.
Gated SPECT.
Gated SPECT was performed with a double-head γ-camera (E. Cam; Siemens Medical Solutions, and Millennium MC; GE Healthcare) equipped with a high-resolution collimator. A protocol consisting of a 64 × 64 matrix, 32 projections per head, 40-s projections, and 8 frames per cycle was applied, with appropriate energy photopeaks. All studies were reconstructed using a 2-dimensional Butterworth filter, with an order of 2.5 (99mTc-tetrofosmin) and a cutoff frequency of 0.3 cycles per pixel (99mTc); projections were reconstructed into transaxial images using filtered backprojection with a ramp filter. No attenuation or scatter correction was used.
Each patient underwent stress/rest gated SPECT according to a single-day protocol. A total of 539 patients (80%) underwent exercise stress testing, and 137 patients (20%) underwent a dipyridamole stress test. Bicycle exercise stress tests (stepwise increments of 25 W every 2 min) or dipyridamole stress tests (0.56 mg/kg intravenously over 4 min) were chosen on the basis of the patient's ability to exercise and after evaluation of medical treatment. Of the 539 patients submitted to exercise stress testing, 387 reached 85% of the maximal predicted heart rate, 58 reached from 80% to 85% of the maximal predicted heart rate, and the remaining 94 patients did not reach the target heart rate and were injected for significant ST segment depression (69 patients) or ventricular arrhythmias (25 patients). In every patient, standard protocols for the injection of 99mTc-tetrofosmin (370 MBq for stress imaging and 740 MBq for rest imaging) were used both during stress and at rest. Images were acquired from 15 to 45 min after the stress and from 30 to 45 min after the rest injections. All patients with previous MI were subjected to baseline tracer injection after sublingual administration of nitrates. Adverse events were defined according to international guidelines.
LV regional wall motion and thickening were quantitatively analyzed at rest and after stress using a previously validated software program (Quantitative Gated SPECT; Cedars Sinai) that provided scores of regional wall motion (0, normal; 5, dyskinetic) and thickening (0, normal; 3, absent thickening) according to a 17-segment polar map (23). In every patient, Quantitative Gated SPECT and Quantitative Perfusion SPECT programs were used both at rest and after stress after qualitative analysis of reconstructed images. In 6% of patients (mainly those with low EF and dominance of myocardial necrosis), LV contours were manually adjusted. By adding the 17-segment scores, summed stress scores (SSS) and summed rest scores (SRS) were automatically calculated. The summed difference score (SDS), indicating the extent of reversible perfusion defects, was obtained by calculating the differences between the SSS and the SRS (24). Regional wall motion analysis by Quantitative Perfusion SPECT was used to identify attenuation artifacts in patients with fixed positive defects at rest and after stress. The variables derived from gated SPECT were LVEF, summed motion, and thickening scores at rest; LVEF, summed motion, and thickening scores after stress; and SRS, SSS, and SDS.
Coronary Arteriography.
Angiographic images (Judkins technique) were qualitatively analyzed. The variables explored were the presence of a stenosis (>50% luminal diameter reduction) in the main coronary arteries and a semiquantitative score of the extent of coronary lesions. To derive this score, the location of coronary stenoses was categorized as proximal, middle, or distal for left anterior descending artery and as proximal or distal for left circumflex and right coronary arteries. If a vessel presented more than 1 stenosis, only the most severe was considered; eventual downstream lesions were ignored. A score was assigned to each stenosis on the basis of the extent of the perfusion territory according to a 17-segment model (25). Specifically, scores of 7, 5, and 3 were assigned to proximal, middle, and distal left anterior descending artery stenoses, and scores of 5 and 3 were assigned to proximal and distal left circumflex and right coronary artery stenoses. A score of 12 was assigned to left main stenoses; in this case, left anterior descending or left circumflex stenoses were ignored. The final score (ranging from 0 to 17) was obtained by summation. The same score was also obtained using a 70% coronary stenosis threshold.
Follow-up
Patients were followed up by periodic examinations in the outpatient setting. In patients who did not attend this program, follow-up data were obtained using written telephone interview (administered to the patient or the patient's family by dedicated personnel) or mail questionnaires. In case of negative answers, the local demographic registry was queried. Cardiac death was defined as death caused by acute MI, death caused by heart failure, or a sudden and unexpected death not related to any possible cause; nonfatal MI was documented by clinical records. The study protocol was approved by the local committee on human research. In addition, patients gave written informed consent to have their clinical data prospectively collected for research purposes.
Statistical Analysis
Continuous variables were expressed as mean ± SD, and categoric variables were expressed as percentages. The primary endpoint was the occurrence of cardiac events, defined as cardiac death or nonfatal acute MI. Predictors of survival were initially identified by univariate analysis performed using the Cox proportional hazards regression model. Categoric variables were included in the model as dummy variables. The independent predictors of survival at each of the different stages of diagnostic work-up were identified using multivariate Cox regression analysis and included all the variables collected at that stage. A backward elimination procedure was used to select the independent variables, that is, those variables resulting in a significant outcome. Once the independent predictors of survival at the different steps of the diagnostic work-up were identified, these predictors were entered into a Cox proportional hazards regression analysis to obtain the final independent predictors of cardiac event–free survival. The incremental prognostic information obtained at each step of the diagnostic process was evaluated by the χ2 improvement.
To assess the prognostic value of the Cox proportional hazards regression models, we used the time-dependent receiver-operating-characteristic (ROC) curve estimation from censored survival data using the nearest-neighbor estimation method (26). The linear prognostic scores obtained from the final Cox models were considered in the analysis. The area under the time-dependent ROC curves (AUC) was used to express the prognostic accuracy of the final Cox models. All statistical tests were 2-tailed; a P value of less than 0.05 was considered significant. Statistical analysis was performed with free and commercially available software (JMP 4.0 [SAS Institute Inc.]; SPSS 10.0 [SPSS Inc.]; R: A Programming Environment for Data Analysis and Graphics, version 2.7.1 [R Foundation for Statistical Computing]; and STATA [StataCorp LP]).
RESULTS
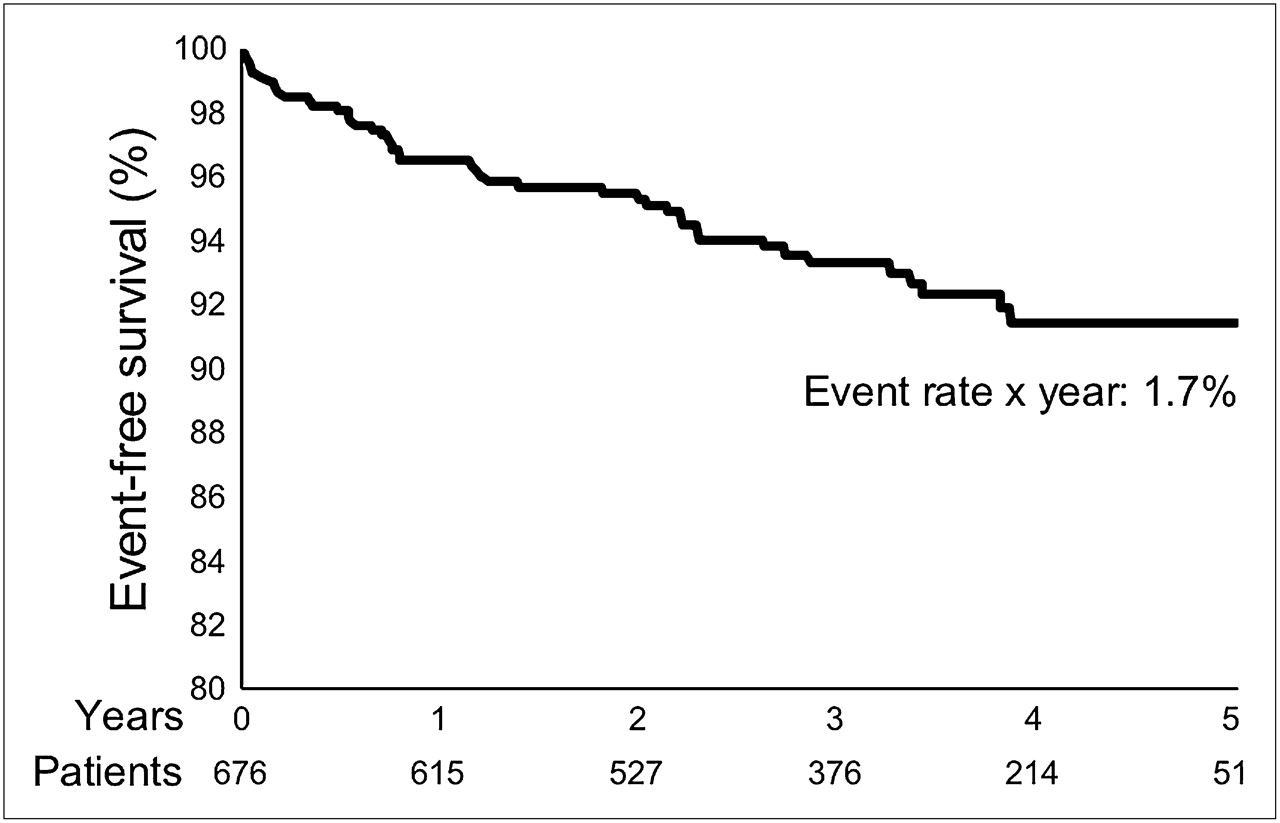
During follow-up (median, 37 mo), 59 of 676 patients died (24 from cardiac causes) and 19 experienced a nonfatal MI. A plot of cardiac event–free survival (cardiac death and nonfatal MI) is shown in Figure 1. The annual all-cause mortality rate was 2.4%, and the annual rate of cardiac events was 1.7%.

Event-free survival (cardiac death and nonfatal MI) in patients with known or suspected IHD.
Predictors of Cardiac Event–Free Survival
As shown in Table 3, several variables were significant predictors of cardiac event–free survival at univariate analysis. Multivariate Cox regression analysis determined that the following variables were independent predictors at the different stages of diagnostic work-up: among clinical data, a previous MI; among laboratory tests, serum creatinine and the ratio between LDL and HDL cholesterol levels; among electrocardiographic and echocardiographic variables, LVEF; among the variables extracted from gated SPECT, SRS and SDS; and among angiographic variables, the score of the extent of coronary stenoses (Table 4). When all the above predictors were evaluated together (Table 5), only SRS and SDS, serum creatinine, and LDL/HDL cholesterol levels were (in descending order of significance) the final independent predictors of cardiac event–free survival (global χ2 = 38.84, P < 0.0001). An SRS value greater than or equal to 4 identified patients at risk of cardiac events, with a sensitivity of 48% and a specificity of 70%. An SDS value greater than or equal to 6 identified patients at risk, with a sensitivity of 48% and a specificity of 75%.
Significant Predictors of Event-Free Survival Using Univariate Analysis
Independent Predictors of Event-Free Survival Using Multivariate Analysis at Each Stage of Diagnostic Work-up
Final, Independent Predictors of Event-Free Survival Using Multivariate Analysis, Considering All Stages of Diagnostic Work-up
In the 492 patients in whom the diagnosis of IHD was ascertained, SRS (hazard ratio [HR], 1.20; 95% confidence interval [CI], 1.12–1.28; χ2 = 26.67; P < 0.0001) and SDS (HR, 1.15; 95% CI, 1.04–1.28; χ2 = 7.30; P = 0.0069) were the only final independent predictors of survival (global χ2 = 27.72, P < 0.0001). The AUC showed a good prognostic value for the 2 final Cox models (AUC = 0.75 for total patients [95% CI, 0.68–0.82] and AUC = 0.73 for patient with ascertained IHD [95% CI, 0.65–0.82]).
Incremental Prognostic Value
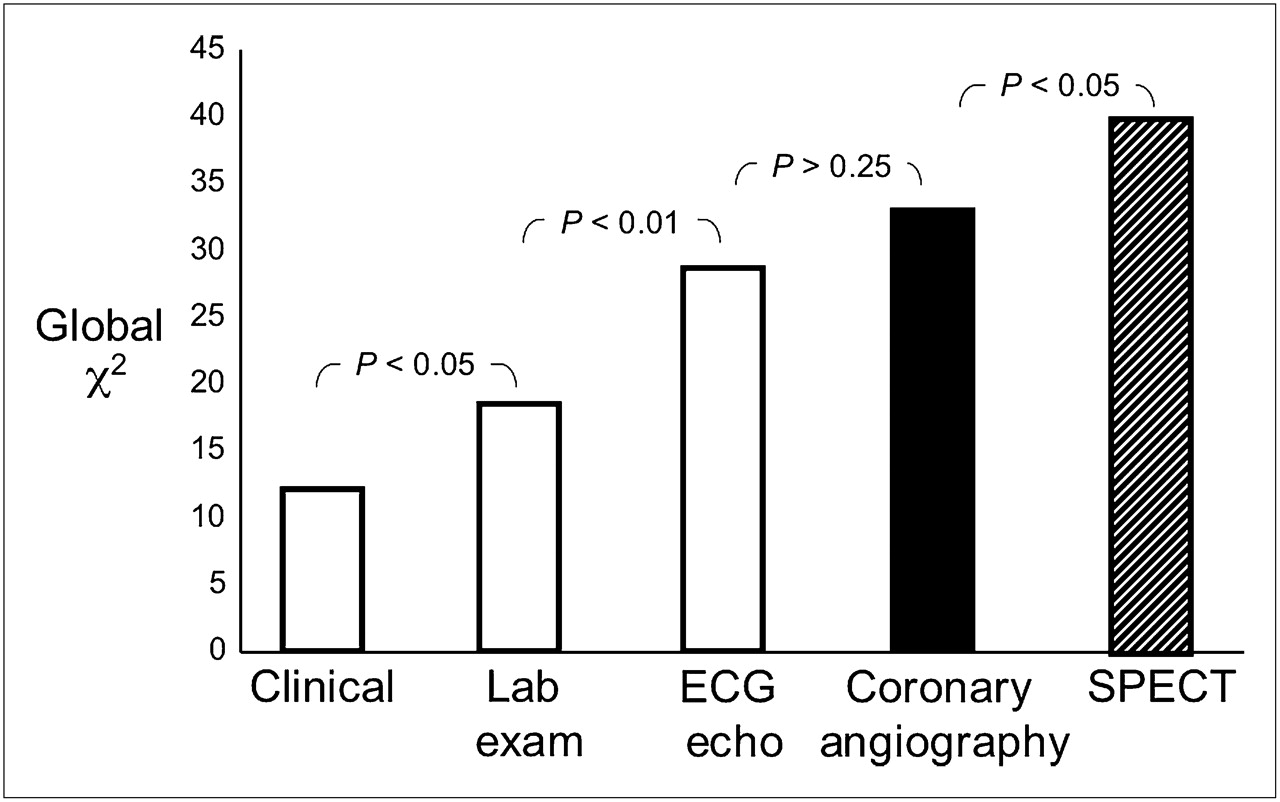
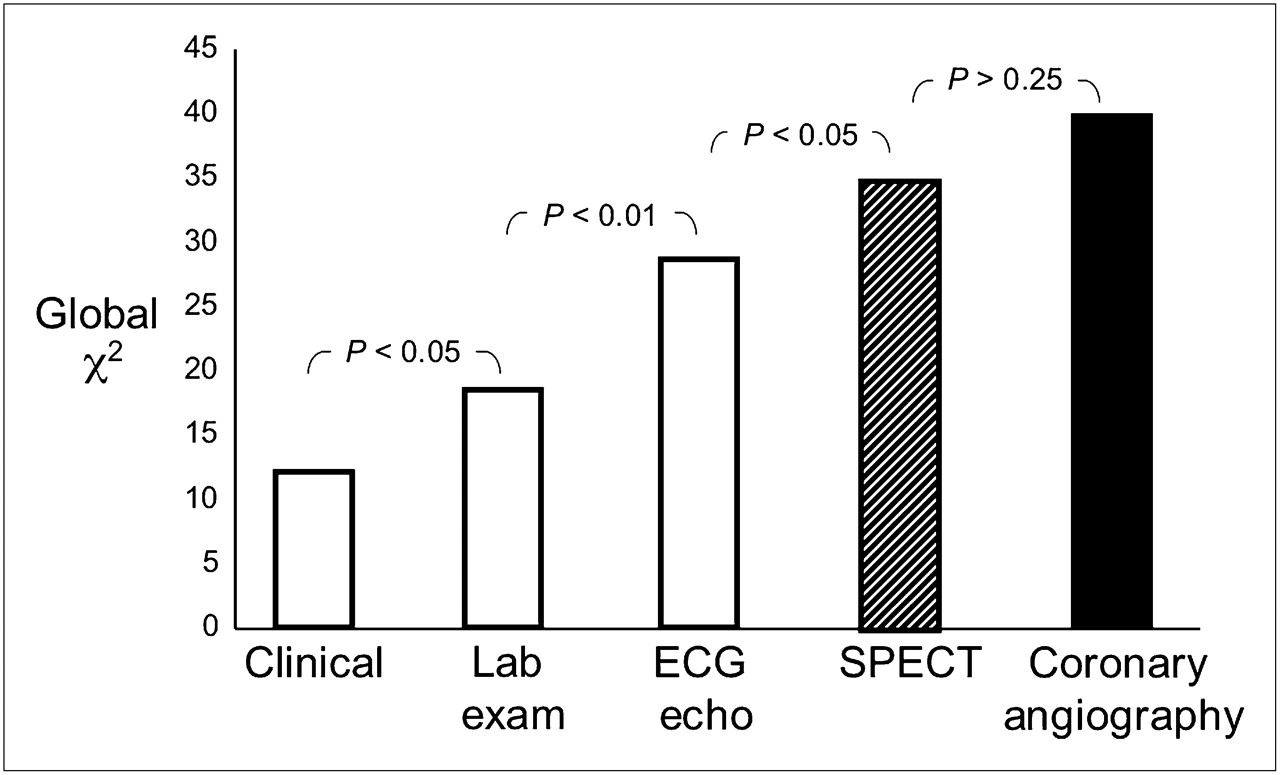
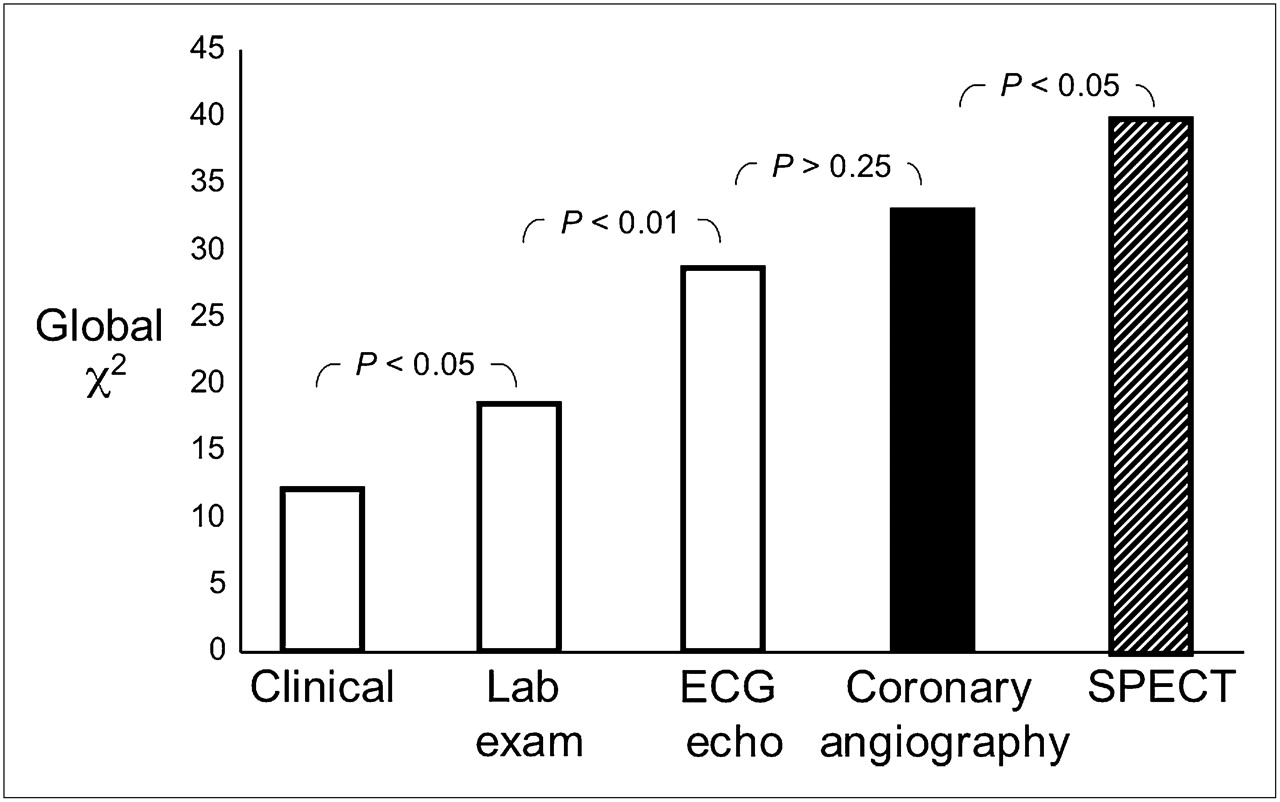
Figure 2 demonstrates that the prognostic information significantly increased, adding to the clinical variables those extracted from laboratory tests, 12-lead ECG, echocardiography, and gated SPECT in hierarchical order. The selected variables were those that were independent predictors of event-free survival at the different stages of diagnostic work-up. Once the above variables were considered, coronary arteriography did not add any significant prognostic information. Conversely, if the information provided by coronary arteriography was made available after ECG and echocardiography, gated SPECT still significantly improved the prognostic information (Fig. 3).

Incremental prognostic value during diagnostic work-up. Information provided by stress/rest gated SPECT is available after clinical examination, laboratory tests, and ECG and echocardiography but before coronary arteriography.
Prognostic value during diagnostic work-up when information provided by gated SPECT is available after coronary arteriography.
Effect of Treatment
Of the 492 patients with ascertained IHD, 187 were treated medically and 305 were revascularized (180 by percutaneous coronary interventions, 110 by coronary artery bypass graft surgery, and 15 by both). Medically treated patients had less extensive IHD than those who were revascularized. Specifically, medically managed patients had lower values of SDS (4.9 ± 3.5 vs. 5.7 ± 2.9, P = 0.0001), a lower number of coronary stenotic vessels (0.7 ± 1.0 vs. 1.9 ± 0.9, P = 0.0005), and a lower score of coronary stenoses (6.0 ± 4.8 vs. 8.7 ± 4.2, P < 0.0001) than did revascularized patients. Cardiac events occurred in 12 medically managed and in 25 revascularized patients. At multivariate Cox regression analysis, the type of treatment (P = 0.485) did not affect the ability of gated SPECT (SRS: HR, 1.20; 95% CI, 1.12–1.28; P = 0.000; and SDS: HR, 1.15; 95% CI, 1.04–1.27; P = 0.008) to predict event-free patient survival.
A total of 256 patients were revascularized within 60 d of nuclear testing (165 by percutaneous coronary interventions, 84 by coronary artery bypass graft surgery, and 7 by both) and 49 subsequently. Censoring of the patients at the time of revascularization cardiac events occurred in 12 patients, and SRS was the only final independent predictor of cardiac event–free survival (HR, 1.24; 95% CI, 1.12–1.37; P = 0.0006).
DISCUSSION
This study shows that myocardial perfusion abnormalities obtained after stress and the extent of scar tissue detected by gated SPECT are the best predictors of cardiac events in patients with suspected or ascertained IHD. The ability of nuclear cardiology to predict the outcome of patients with IHD has been well known for several years (1–7,10). In respect to these pivotal and to more recent studies (27–29), we compared gated SPECT data with those obtained during the diagnostic work-up (13–17). Although several variables were able to predict cardiac event–free survival, myocardial perfusion abnormalities remained the best predictor of patient outcome when all the different stages of the diagnostic process were considered, including coronary arteriography.
Gated SPECT and LVEF
Since the initial study performed using gated blood-pool scintigraphy (30) in post-MI patients, LVEF has been acknowledged to be a powerful predictor of mortality in patients with IHD. The prognostic impact of LVEF has been widely confirmed in large multicenter studies (11,31). Furthermore, the prognostic impact of LVEF has been extended to a wide variety of patients, including those with heart failure, cardiomyopathies, and valvular heart disease (32). Thus, the value of LVEF has become one of the main determinants of therapeutic decision making, as in the case of implantable cardioverter defibrillators or cardiac resynchronization therapy (33). In the present study, when the prognostic power of LVEF at rest was compared with that of scar-tissue extent, the power of LVEF disappeared.
This observation is not surprising, because LVEF represents a global normalized ratio and is susceptible to changes in preload and afterload and contractility. On the other side, SRS is an index of normalized uptake, coupled to viable or scarred segments and normalized to control subjects, and is independent of hemodynamic changes, myocardial contractility, and medical treatment. The superiority of perfusion imaging in prognostic stratification might suggest a superiority in guiding decision making; however, this hypothesis should be addressed in specific prospective studies.
In a previous study, poststress EF and end-systolic LV volumes were shown to have incremental prognostic values over prescan and perfusion information (34). Subsequently, poststress EF was the strongest predictor of mortality, whereas the SDS was the strongest predictor of MI (35). The divergence with these studies could be explained by the way we performed the prognostic analysis. Indeed, Sharir et al. (34,35) censored patients revascularized within 60 d of nuclear testing. However, when we censored revascularized patients the number of events was small, and SRS was the only final independent predictor of cardiac events. Furthermore, we combined the 2 endpoints cardiac death and nonfatal MI. Finally, enrolling patients who had undergone coronary arteriography might have selected a patient population at higher risk than in previous studies, in which patients were enrolled mainly on the basis of symptoms and the pretest probability of IHD.
Gated SPECT and Coronary Anatomy
The greater diagnostic accuracy of stress-induced myocardial perfusion abnormalities over electrocardiographic signs of ischemia and greater contribution of nuclear imaging to risk stratification are widely acknowledged. It is also well known that myocardial perfusion imaging is superior to coronary arteriography in risk stratification of patients with IHD. In 1992, Pollock et al. demonstrated that myocardial perfusion is superior to coronary arteriography in risk stratification of IHD patients (4); at variance with our study, these authors used 201Tl and static planar imaging, and all the patients had suspected IHD. In a series of 316 patients, Iskandrian et al. (5) showed the independent and incremental prognostic information of exercise SPECT thallium imaging even when catheterization data are available; unlike us, these authors studied patients with definite coronary artery disease who were medically treated. In addition, in none of the above studies were laboratory variables and echocardiography considered. This study largely confirms the advantages of perfusion imaging over clinical, electrocardiographic, laboratory, and resting echocardiographic data and shows the incremental prognostic value of gated SPECT information over angiographic data. Thus, the severity and extent of stress-induced myocardial perfusion abnormalities provide a better prognostic stratification than does the severity of coronary artery disease, using both a 50% and a 70% stenosis threshold and taking into account the proximality of the lesions along the coronary tree. This observation should suggest a wider use of myocardial perfusion imaging in risk stratification of patients with known or suspected IHD.
Gated SPECT and Laboratory Examinations
In previous myocardial perfusion imaging studies, the prognostic value of several laboratory tests has received little attention. Chronic kidney disease is known to be an important risk factor for atherosclerosis. In the setting of chronic kidney disease, myocardial perfusion abnormalities are common (13). However, most radionuclide imaging studies have examined populations with end-stage renal failure. Whether mild forms of renal dysfunction are associated with IHD among patients with positive myocardial perfusion imaging has not been investigated previously. This study shows the prognostic impact of even mild increments in creatinine levels.
In cardiac patients, a low triiodothyronine syndrome has been related to a poor outcome (14), and a mildly altered thyroid status has been associated with an increased risk of mortality (14). More recently, thyrotropin levels within the reference range were positively and linearly associated with IHD mortality (36). In our study, thyroid status was not able to predict event-free survival, probably because of the relatively small sample size and because of the inclusion of several patients without heart failure.
In previous studies, HDL cholesterol level was a significant inverse predictor of subsequent major cardiovascular events (15,16). When the LDL cholesterol level achieved in patients receiving therapy was considered, the role of HDL cholesterol was less marked, though still of borderline significance. The relationship remained significant even in patients whose LDL cholesterol level was less than 70 mg/dL (16). Our study shows a negative incremental prognostic value for a reduction in the ratio between LDL and HDL cholesterol levels. Finally, we did not find any prognostic impact of C-reactive protein, likely because of the selection of patients in the chronic phase of IHD.
Study Limitations
A limitation of this study is the selection of patients who have an intermediate pretest probability of coronary artery disease and thus do not reflect the general population of subjects undergoing gated SPECT for known or suspected IHD. More likely enrolled patients—though stable—reflect a higher-risk population, as indirectly shown by the high prevalence of previous MI (43%) and the main cardiovascular risk factors and by the fact that all enrolled patients underwent coronary arteriography. Another limitation is related to the small patient cohort, which does not allow an in-depth evaluation of the potential benefits of treatment.
A mandatory clarification concerns the difference between prognostic and diagnostic impact. Specifically, our considerations on myocardial perfusion imaging are limited to the prognostic stratification; we were aware that several variables that did not enter into our prediction model (such as coronary arteriography) carry clinically significant information in terms of diagnosis and therapeutic decision making.
In clinical practice, stress echocardiography is widely used for risk stratification of patients with IHD. Stress echocardiography was not performed in this study because patients were selected on the basis of having undergone gated SPECT. Finally, the values of cardiac peptides were not available for the entire patient population and were not considered among the tested predictors.
CONCLUSION
In a population of patients with known or suspected IHD, gated SPECT appeared to be the best predictor of cardiac event–free survival, considering all the main variables derived from the diagnostic work-up. In particular, the extent of scar tissue predicted event-free survival better than did LVEF, and stress-induced myocardial perfusion abnormalities predicted event-free survival better than did coronary arteriography. Laboratory variables such as serum creatinine and LDL/HDL cholesterol levels were independent predictors of event-free survival but were less powerful than SRS and SDS.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication July 13, 2008.
- Accepted for publication December 8, 2008.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prognostic Value of Combined Clinical and Myocardial Perfusion Imaging Data Using Machine Learning
- Outcome of revascularisation in stable coronary artery disease without ischaemia: a Danish registry-based follow-up study
- Detection of Significant Coronary Artery Disease by Noninvasive Anatomical and Functional Imaging
- 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons
- 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons
- Structural Abnormalities of the Coronary Arterial Wall--in Addition to Luminal Narrowing--Affect Myocardial Blood Flow Reserve
- Improved Outcome Prediction by SPECT Myocardial Perfusion Imaging After CT Attenuation Correction