


Abstract
Although 6-18F-fluoro-l-dopa (18F-FDOPA) has been available to study the striatal dopaminergic system for more than 2 decades, the full potential of the tracer was not realized before the introduction of 18F-FDOPA PET and PET/CT to image a variety of neuroendocrine tumors (NETs) and pancreatic β-cell hyperplasia. Together with receptor-based imaging, 18F-FDOPA offers a formerly unforeseen means to assist in the management of NETs and infants with persistent hyperinsulinemic hyperplasia. Institutions with special expertise in surgical, oncologic, and radiologic therapeutic modalities for NETs derive the highest benefit from 18F-FDOPA PET/CT. 18F-FDOPA–guided therapy may add to NET control by ensuring maximal cytoreduction.
Neuroendocrine tumors (NETs) constitute a distinct group of relatively slowly growing and rarely occurring neoplasms, although a recent report from the Surveillance Epidemiology and End Results Program indicated an almost 5-fold increase in incidence over 3 decades to 5.25 per 100,000 in 2004 (1). Notably, gastric and pancreatic NETs are detected more commonly than before because of increased awareness and the use of endoscopy and advanced imaging methods such as multidetector-row CT, MRI, and somatostatin receptor scintigraphy (SRS) (2). NETs secrete peptides and biogenic amines, leading to symptoms including the classic carcinoid syndrome, but approximately half of the patients do not show any symptoms related to peptide or hormone secretion. Typically, patients with NETs present with advanced disease because the primary lesion may remain clinically silent and small despite multiple-organ metastases. Although curative surgical treatment can be offered only to a minority, recent studies indicate that successful cytoreductive surgery can both effectively control symptoms and potentially improve outcome (3). Nonsurgical treatment of NETs consists of somatostatin analogs, radiofrequency ablation, chemotherapy, and biologically active substances that can alleviate symptoms related to hormone secretion and sometimes affect disease progression (4). The increased expression of somatostatin receptors makes NETs a potential target for molecular therapy using radionuclides tagged to receptor ligands (5). Because of the limited sensitivity of CT, MRI, and other standard diagnostic work-up in unveiling all lesions and characterizing their nature, molecular imaging holds great promise in improving the management of NETs. The preconception is that accurate staging with molecular imaging enables maximum cytoreductive treatment, which may at best offer cure or confer additional years without disease progression.
MECHANISM OF UPTAKE OF 6-18F-FLUORO-L-DOPA (18F-FDOPA) IN NEUROENDOCRINE CELLS
Uptake of 18F-FDOPA is characteristically high in neuroendocrine cells, which are offspring from the amine precursor uptake and decarboxylation stem cells. The origin of neuroendocrine cells is local, throughout the gut wall in the gastroenteropancreatic NETs (2); the catecholamine-producing NETs arise from chromaffin cells and their common sympathoadrenal progenitors, which migrate from the neural ectoderm (6). Neuroendocrine cells store the transported and decarboxylated amines in cytoplasmic neurosecretory granules that vary in size, shape, and capacity to store peptide hormones. 18F-FDOPA is transported into neuroendocrine cells via the sodium independent system L, in which a large neutral amino acid transporter (LAT1) protein linked to the glycoprotein CD98 is the principal mediator (7). It has been repeatedly shown that the activity of amino acid decarboxylase (AADC) is important for intracellular retention of the metabolized 18F-FDOPA (8,9). Increased transport together with AADC activity result in a positive PET image of the target lesion having the origin in the amine precursor uptake and decarboxylation system (Fig. 1). Storage into neurosecretory granules via vesicular monoamino transporters is not a prerequisite for retention of 18F-FDOPA in gastroenteropancreatic NETs. Generally, signal-to-background ratio is improved by inhibition of the peripheral AADC activity with an advance administration of oral carbidopa (9,10). By inhibiting the peripheral conversion of 18F-FDOPA into 18F-fluorodopamine with carbidopa, the bioavailability of the native tracer for tumor cells increases and uptake in the surrounding tissues such as the pancreas and kidneys decreases. Some tumors that do not possess features of NETs, such as cerebral gliomas, may still show increased uptake of 18F-FDOPA because of the overexpression of the LAT1 protein (11). However, tracer avidity in non-NETs, with the exception of brain tumors, is less predictable, and the role of 18F-FDOPA for diagnosis in major cancer forms seems to be limited (Fig. 2) (11,12).
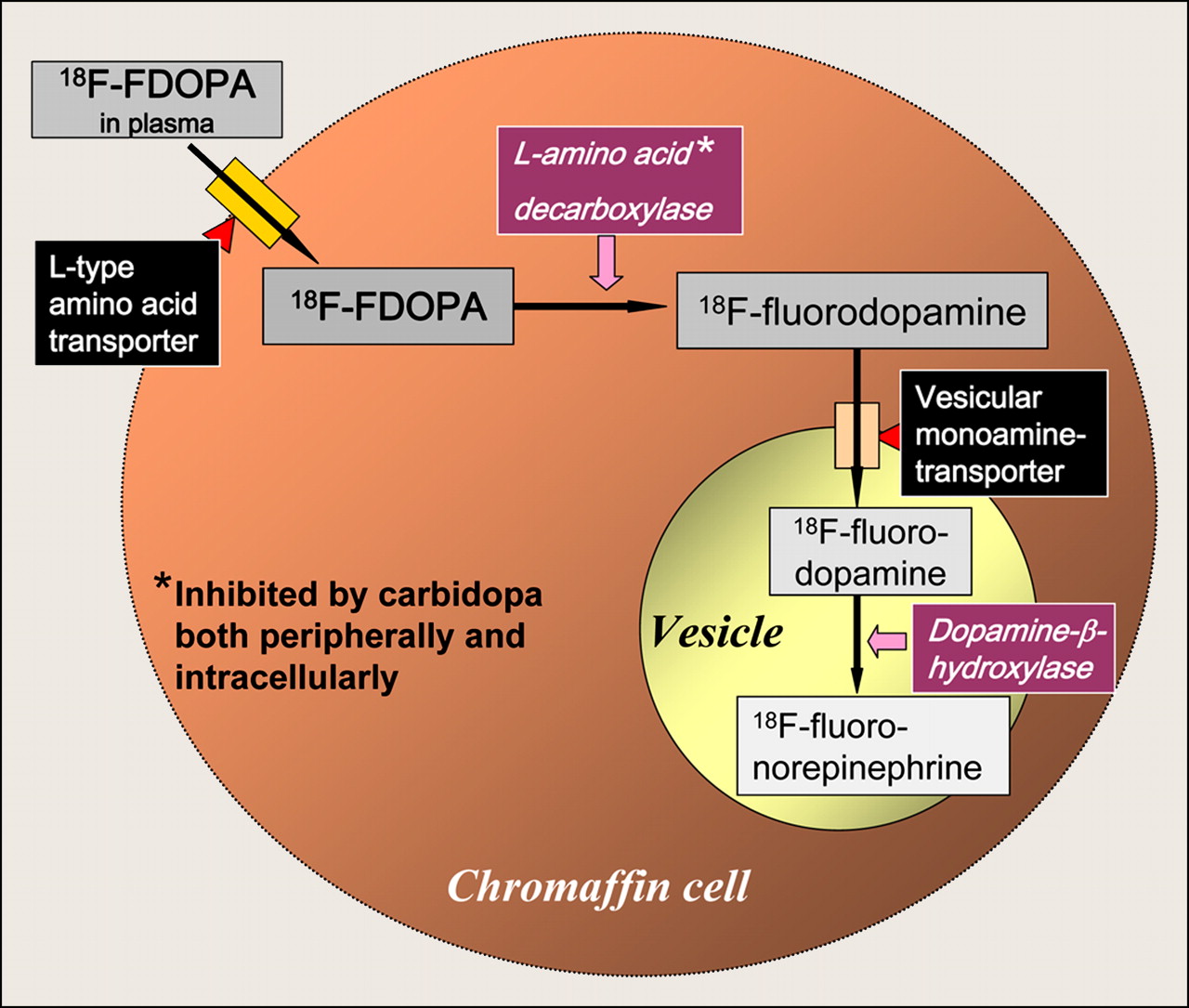
Schematic presentation of uptake mechanism of 18F-FDOPA in neuroendocrine chromaffin cells.
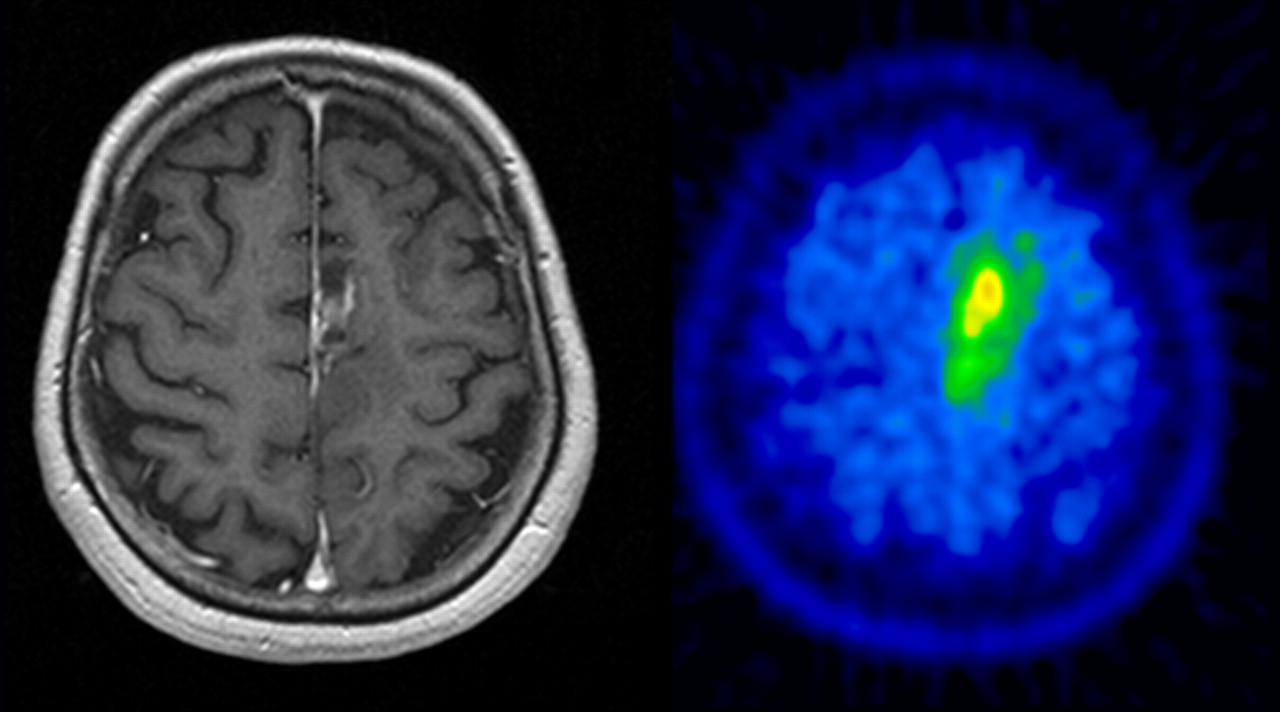
MR and 18F-FDOPA PET images of left parasagittal recurrent malignant glioma. Diagnosis of glioma recurrence represents promising application for 18F-FDOPA imaging.
EVOLVING CLINICAL ROLE IN CONTEXT OF RADIOSYNTHETIC METHODS
A comprehensive review of clinical progress in using 18F-FDOPA to image NETs was recently published in The Journal of Nuclear Medicine (12). This review covered published literature until May 2007, and our review here will mostly update with studies appearing after that time. Clearly, the past 10 y have been instrumental in the development of 18F-FDOPA to image gastroenteropancreatic NETs, pheochromocytomas and paragangliomas, medullary thyroid carcinoma (MTC), and pediatric and adult patients with hyperinsulinemic disorders. In parallel with 18F-FDOPA, tracers such as 18F-fluorodopamine and 11C-hydroxytryptophan have shown potential in the imaging of pheochromocytomas (13) and islet cell tumors (10), respectively. From a practical point of view, neither 18F-fluorodopamine nor 11C-hydroxytryptophan is likely to propagate outside specialized centers with a large expertise in radiochemical synthesis procedures. By contrast, 18F-FDOPA can now be purchased in Europe from a commercial service provider, which indicates wider clinical interest in the use of the tracer. At our institution, the electrophilic fluorination of 18F-FDOPA with posttarget-produced 18F-F2 is a straightforward and fast (∼50 min) radiochemical synthesis method, resulting in a typical yield of 1.5 GBq of the end product and with high specific activity (∼3.7 GBq/μmol) (14). The electrophilic synthesis procedures have now been adopted in most centers using 18F-FDOPA, although nucleophilic methods are preferred by a few (12).
CLINICAL UPDATE OF NEUROENDOCRINE TUMORS AND HYPERINSULINISM
The formerly used nomenclature carcinoid for gastroenteropancreatic NETs and bronchopulmonary NETs is now reserved for the syndrome for which intermittent release of biogenic amines in the circulation causes characteristic symptoms including flushes and diarrhea. Furthermore, the present World Health Organization classification has proposed gastroenteropancreatic NETs to be assigned to 1 of 3 categories (well-differentiated tumor, well-differentiated carcinoma, and poorly differentiated carcinoma) based on histology, size, and proliferative activity (2). In addition to proliferative index, prognostic factors include size, angioinvasion, and mitotic activity. The current World Health Organization recommendations for classification and prognostic factors may help the selection of tracer likely to show a positive image on PET. Poor differentiation may suggest loss of neuroendocrine features and expression of glycolytic phenotype in favor of using 18F-FDG while other NETs should be imaged with 18F-FDOPA.
Pheochromocytoma and Paraganglioma
Since January 2000 our experience in imaging NETs with 18F-FDOPA in the setting of primary diagnosis, staging, and restaging has been encouraging (15). We have studied 25 patients with pheochromocytoma, 39 patients with gastroenteropancreatic NET, and 29 patients with other forms of NET, including 12 patients with suspected recurrent MTC. Although the overall diagnostic accuracy was high at 90%, in the primary diagnosis and staging of 16 pheochromocytomas both the sensitivity and specificity were 100% (Fig. 3). Others have confirmed our results in both benign and malignant pheochromocytoma. Imani et al. (16) detected and localized pheochromocytoma in their visual analysis of 11 of 13 patients without false-positive findings, giving an overall diagnostic accuracy of 92%. Taïeb et al. (17) identified more tumor sites with 18F-FDOPA than with metaiodobenzylguanidine (MIBG) scintigraphy in all 5 patients with metastasized pheochromocytoma and in 2 of 3 neck and abdominal paragangliomas; concurrent 18F-FDG imaging, compared with 18F-FDOPA, provided additional information in 3 cases. Together with the authors of previous studies reviewed by Jager et al. (12), we propose that 18F-FDOPA would be the first method for radionuclide imaging of primary and metastatic pheochromocytoma in those institutions having routine access to this tracer. However, 18F-FDG complements 18F-FDOPA in patients with metastatic disease in whom the metabolic phenotype has shifted to glycolysis (i.e., patients with a mutation in the succinate dehydrogenase gene B), and MIBG retains its place in radionuclide therapy (13,17). The role of SRS, especially using ligands predominantly targeting somatostatin receptor type 2 such as octreotide, seems to be limited (8).
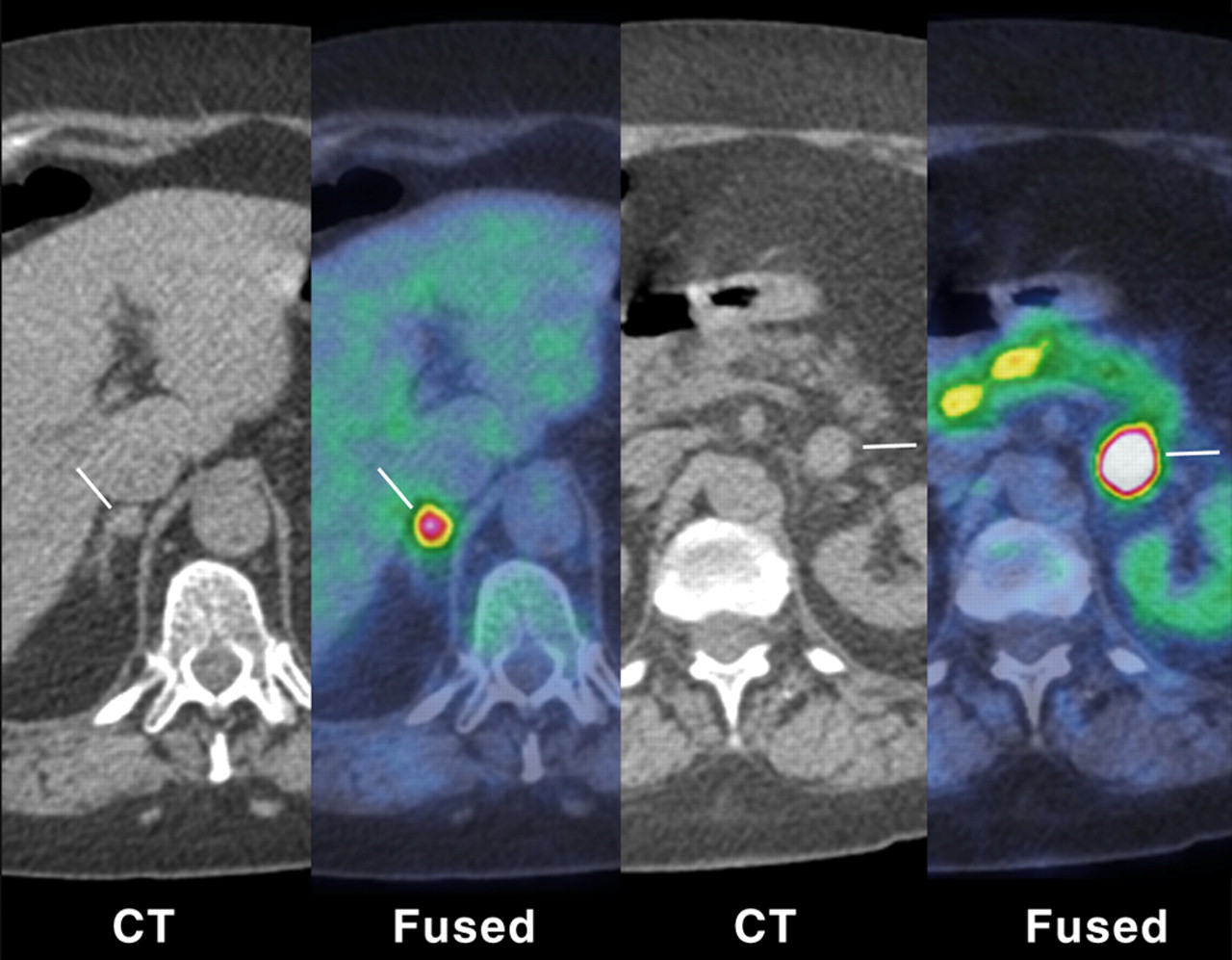
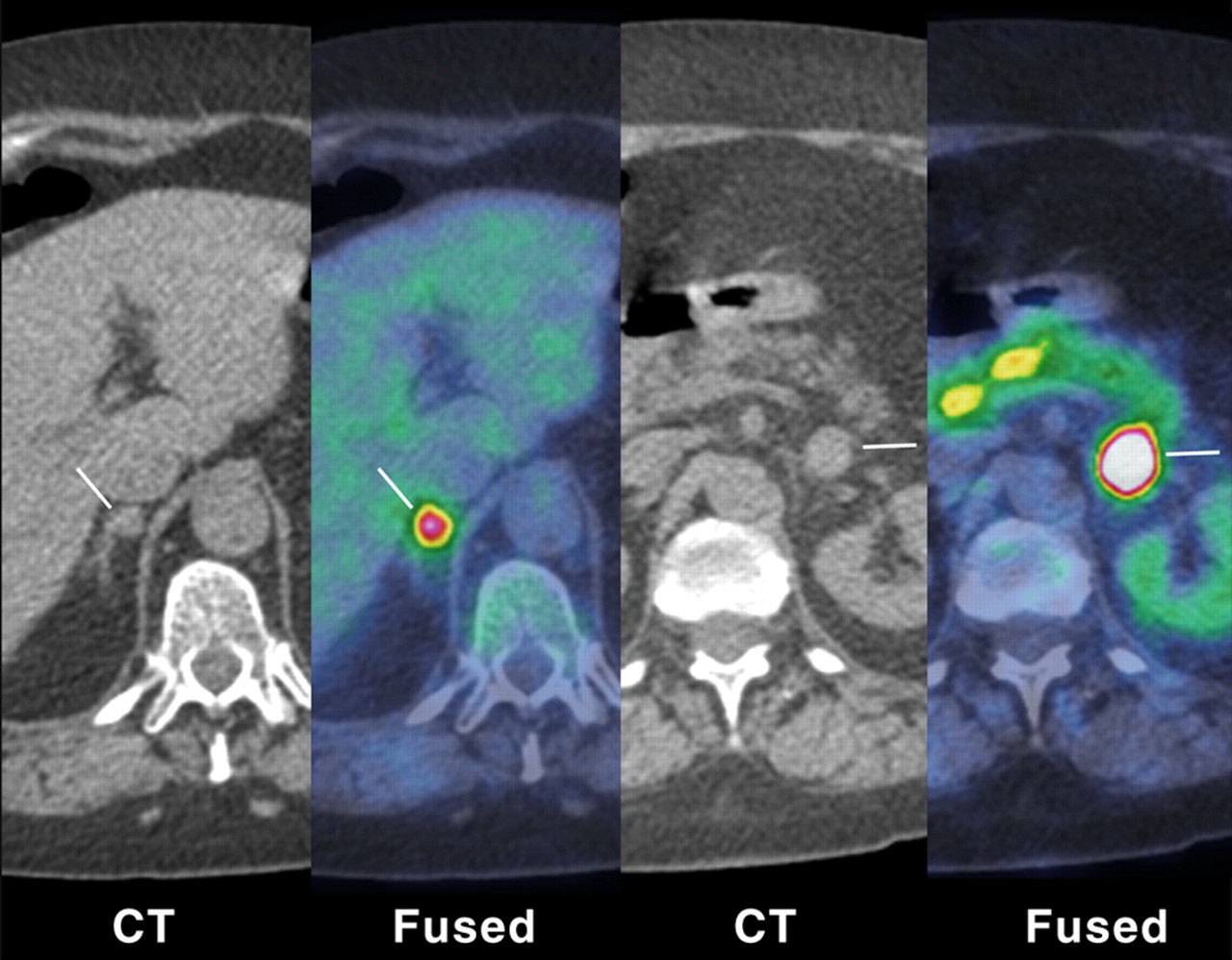
Bilateral pheochromocytomas demonstrated with 18F-FDOPA PET/CT (white lines) and negative on MIBG scintigraphy. Paraaortic nodal metastasis measuring 6 mm (not shown) was also found on 18F-FDOPA imaging. Diagnosis of all 3 tumors was confirmed at surgery. Uptake of 18F-FDOPA is low in dorsal and normally functioning part of right adrenal.
Gastroenteropancreatic NET
Previously the Dutch and the French groups (12) have demonstrated the superiority of 18F-FDOPA PET to SRS in imaging of gastroenteropancreatic NETs with carcinoid features, whereas the sensitivity of 18F-FDOPA to detect noncarcinoid gastroenteropancreatic NETs has been less satisfactory at 50%. Montravers et al. (18) made a survey with questionnaires sent to referring physicians who requested PET as a last resort when conventional diagnostic methods had failed. In a total of 71 responses, 18F-FDOPA PET was found to affect management in 50% of cases among gastroenteropancreatic NETs of carcinoid type, whereas the rate of impact was only 16% in occult endocrine tumors and 13% in noncarcinoid NETs. Our experience is in line with this because the 4 patients with false-negative findings on 18F-FDOPA PET all had advanced neuroendocrine carcinoma (15). Overall, we found that 18F-FDOPA PET provided additional information in 44 of 82 patients, and in 11 other patients a clinical diagnosis was allowed with this form of PET when findings on conventional methods remained obscure. The experience in regard to the choice of the molecular imaging method in gastroenteropancreatic NETs is 18F-FDOPA PET/CT when the tumor is of carcinoid type, whereas SRS-, 18F-FDG–, or PET-based somatostatin receptor imaging (19) should be considered in other cases.
MTC
Detection of recurrent MTC after increasing calcitonin levels deserves special attention. The clinical problems are the high risk of recurrence after seemingly radical surgery, difficulties in predicting the rate of progression, and lack of an effective nonsurgical treatment modality. The initial, albeit small, experience indicates that 18F-FDOPA, compared with the conventional method, improves staging but also implies that CT or MRI continues to be important for proper management (20). We have found 18F-FDOPA PET/CT highly useful in guiding surgery of regional metastases after recurrences first detected chemically, even if it is recognized that some disease is left behind (15). Beheshti et al. (21) recommended 18F-FDOPA PET/CT as a 1-stop diagnostic procedure in candidates for surgery in their study of 26 patients in which 18F-FDG clearly showed inferior diagnostic performance. In a role similar to the one they share in pheochromocytoma, 18F-FDOPA and 18F-FDG have a complementary role in the restaging of MTC; 18F-FDOPA assists in the planning of local treatment and 18F-FDG in the determination of progression to a more aggressive phenotype (20). The likelihood for false-negatives with molecular imaging techniques remains high if calcitonin doubling time is higher than 2 y (20,21).
Neonatal and Adult Hyperinsulinism
Congenital hyperinsulinism of infancy (CHI) is due to focal or diffuse adenomatous hyperplasia of the pancreas. The focal form is caused by a paternally inherited ABCC8 or KCNJ11 gene mutation, whereas several other mutations are associated with the diffuse form, and in 50% of the cases the genetic basis is unknown (22). The introduction of 18F-FDOPA PET and later PET/CT have made a tremendous change in the management of infants with the focal disease who can now be cured by molecular imaging–guided laparoscopic surgery (23). The sensitivity and specificity of 18F-FDOPA PET for detecting a focus usually measuring between 2 and 10 mm is approximately 90% and 100%, respectively (21). Screening of mutations of ABCC8 and KCNJ11 is necessary, because infants likely to have the diffuse form do not benefit from 18F-FDOPA imaging. Current guidelines recommend 18F-FDOPA PET/CT whenever genetic changes suggest a focal form of CHI and pancreatic surgery is considered. PET may be helpful in finding ectopic foci of focally presenting CHI as well (22).
Insulinoma is the most likely cause of hyperinsulinemic hypoglycemia in adults, and although 18F-DOPA is a promising molecular probe, its performance in the detection of adult islet cell tumors is not completely characterized (10). We were able to localize insulinoma or β-cell hyperplasia with PET in 9 of 10 adult patients who did not receive preadministration carbidopa and who had negative findings on CT, MRI, and ultrasound (24) (Fig. 4). The depletion of all pancreatic tracer uptake with carbidopa may sometimes mask focal uptake in the insulinoma or hyperplastic β-cell islet, leading to false-negative findings (25). This finding may be related to low intralesional AADC activity and the resultant lack of accumulation of the decarboxylated tracer in the form of 18F-dopamine (8). Until wider experience in using 18F-FDOPA to localize insulinoma and other islet cell tumors with and without carbidopa is available, we would refrain from using this peripheral decarboxylase inhibitor whenever neonatal or adult hyperinsulinism is studied (25).

Insulinoma in dorsal surface of pancreatic body on 18F-FDOPA PET/CT (white line). PET guided successful surgical treatment of this tumor in adult patient.
FUTURE DIRECTIONS
Molecular imaging of NETs has evolved rapidly during the past decade. We have confirmed the great potential of 18F-FDOPA to monitor metabolic activity of enterochromaffin cells in pheochromocytoma and hyperplastic β-cells in the focal form of CHI but recognize that other tracers, notably 68Ga-labeled peptides binding to somatostatin receptors, may prove to be more convenient in the routine diagnosis of most NETs. Recently, Ambrosini et al. (19) showed the superior performance of 68Ga-DOTA-NOC over 18F-FDOPA PET in finding primary and secondary lesions associated with gastroenteropancreatic and lung NET. Commercially available 68Ge/68Ga-generators enable on-site production of radiolabeled peptides in hospitals that do not have a cyclotron for the radiosynthesis of 18F-FDOPA. Furthermore, the 68Ga-labeled compounds give information about receptor density and biodistribution that is necessary if peptide receptor radionuclide therapy is considered (5). We predict that in the close future, 18F-FDOPA will maintain a primary role in the diagnosis of pheochromocytomas, focal form of CHI, and MTC, whereas most of the gastroenteropancreatic and lung NETs will be studied with 68Ga-labeled peptide analogs. However, lessons learned from the evaluation of uptake of 18F-FDOPA have been highly useful in understanding the potential of molecular imaging for precision diagnosis and treatment of all NETs.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication August 18, 2009.
- Accepted for publication September 25, 2009.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Patient-Derived Medullary Thyroid Cancer Organoids; a Model for Patient-tailored Drug and PET-Tracer Screening
- Molecular Imaging of Gastroenteropancreatic Neuroendocrine Tumors: Current Status and Future Directions
- 18F-Fluorodihydroxyphenylalanine PET/CT in Patients with Neuroendocrine Tumors of Unknown Origin: Relation to Tumor Origin and Differentiation
- Production at the Curie Level of No-Carrier-Added 6-18F-Fluoro-L-Dopa
- Characterization of Neuroblastic Tumors Using 18F-FDOPA PET
- 18F-DOPA PET/CT unravels malignant paraganglioma mimicking temporomandibular joint disorder