


Abstract
It has been suggested that vascular endothelial growth factor (VEGF) and statins enhance the survival, proliferation, and function of endothelial progenitor cells (EPCs). We investigated whether reporter gene PET can be used to detect the effects of atorvastatin and VEGF on survival of EPCs after transplantation in the rat heart. Methods: Healthy nude rats received an intramyocardial injection of 4 million human EPCs retrovirally transduced with the sodium/iodide symporter gene for reporter gene imaging. Reporter gene expression was imaged at days 1 and 3 after injection on a small-animal PET scanner with 124I, and the presence of EPCs was confirmed by immunohistochemistry with human CD31 antibodies. The control group received EPCs transduced only with the reporter gene, whereas treatment groups received oral atorvastatin (10 mg/kg/d) and EPCs cotransduced with adenoviral vectors encoding VEGF in addition to sodium/iodide symporter. Results: Immunohistochemistry showed more EPCs at the site of injection after atorvastatin treatment and in the presence of VEGF expression in EPCs than in controls. PET successfully visualized EPCs as focal 124I accumulation at the site of injection. The quantitative amount of 124I accumulation assessed by PET was significantly higher in the pretreatment than control group. Autoradiography confirmed 124I accumulation in the myocardium that correlated with the number of EPCs. Conclusion: Early survival of transplanted EPCs in the rat myocardium is prolonged by pretreatment with a combination of atorvastatin and VEGF. Reporter gene PET, by successfully quantifying the effect, is an attractive tool for monitoring stem cell survival in vivo.
Cell transplantation is a promising future therapeutic option for patients with impaired regional or global function due to cell death (1,2). However, the limited number of therapeutic cells is considered a major factor limiting the efficacy of cell therapies (1,3). Methods to monitor cell migration, homing, survival, and engraftment may facilitate the understanding of heterogeneous results from early clinical investigations of intracoronary injection of bone marrow–derived cells (1,4).
Short-term visualization of cells after transplantation may be achieved by direct radioactive labeling of stem cells (5). Paramagnetic nanoparticles can be used to facilitate nontoxic labeling of stem cells before transplantation, which would enable repeated MRI (6,7). High spatial resolution and direct correlation of cell signals to regional function or delayed enhancement make this approach attractive for experimental and clinical research. However, because the signal is not directly related to cell viability, it may lose specificity for transplanted cells after cell death and macrophage phagocytosis (8,9). The reporter gene PET approach is one of the most promising to assess specific information on graft cell survival (9,10). For this approach, donor cells are stably transduced with reporter gene before transplantation; thereby, the encoding gene products mediate accumulation of a radioactive reporter probe into the donor cell (9). The probe signal is specific to graft cell survival, since the reporter genes are expressed in viable graft cells even after cell division but are silent after cell death.
Endothelial progenitor cells (EPCs) are capable of improving myocardial neovascularization and left ventricular function in experimental myocardial infarction and hind limb ischemia (11,12). Since these effects can be potentiated by overexpression of vascular endothelial growth factor (VEGF) and statin treatment, they have been proposed as strategies to facilitate therapeutic transplantation of EPCs (13,14). In addition to improving functional properties and tissue retention of EPCs, VEGF and statins increased survival of the cells (13,15–17). Therefore, we investigated whether the reporter gene cell imaging by PET can be used to noninvasively monitor augmented short-term survival of EPCs by statin and VEGF therapy after direct injection in the rat heart.
MATERIALS AND METHODS
Donor Cell Preparation
Human EPCs were isolated, cultured, and expanded as described previously (18). Briefly, cord blood mononuclear cells were obtained from healthy newborn donors. CD34+ cells were isolated using a magnet-activated cell-sorting cell isolation kit (Direct CD34 Progenitor Cell Isolation Kit; Miltenyi Biotec). Cells were cultured and expanded on medium as previously described to express endothelial cell markers including CD31 (>90% positive) (9).
The labeling procedure, effects on EPC viability, and uptake experiments confirming the functionality of sodium/iodide symporter (NIS) have been described previously (9). Briefly, vesicular stomatitis virus glycoprotein pseudotyped retroviral vectors expressing human NIS were produced by transient transfections after cloning of the respective complementary DNAs into pBullet. NIS complementary DNA was derived from FL-NIS/pcDNA3. EPCs were infected with the retroviral vector expressing NIS. Mean transduction efficacies were 50.6% ± 6.8% (SD) for NIS validated by fluorescence-activated cell-sorting analysis with monoclonal antibody directed against an extracellular domain of NIS (VJ2; kindly provided by Dr. Sabine Costagliola, Free University of Brussels, Belgium).
A recombinant human adenoviral vector type 5 (AdV) expressing the enhanced green fluorescent protein and luciferase (eGFP-Luc) fusion protein under control of the murine cytomegalovirus promoter was constructed by cloning the fusion gene derived from plasmid eGFP-Luc (Clontech) into pDC315 (Micorbix). The AdV expressing human vascular endothelial growth factor 165 (VEGF165) (19) under control of the human cytomegalovirus promoter has been characterized before (20). Cells were infected with double-purified AdV or control vector at the indicated multiplicity of infection (MOI) (plaque forming units/mL). All vectors were double-cesium-chloride-gradient–purified and verified to be negative for replication-competent adenovirus by polymerase chain reaction.
Growth of AdV-infected cells was monitored over time by exclusion dye staining with trypan blue. The susceptibility of EPCs to AdV infection was monitored using reporter gene–expressing vector. Detection was by flow cytometry for eGFP and luminometry for luciferase using standard techniques. VEGF secretion into medium was detected by enzyme-linked immunosorbent assay (R&D systems) after changing of medium to VEGF-free conditions 24 h before sample collection.
Uptake of reporter probe 99mTc into AdV-infected cells was performed 24 h after infection as described previously (9).
Animals and Cell Transplantation
Male athymic nude rats (CRL:NIH-rnu, 200–230 g; Charles River Laboratories) were used. Left thoracotomy was performed under anesthesia with intramuscular administration of midazolam (0.1 mg/kg), fentanyl (1 μg/kg), and medetomidine (10 μg/kg) and mechanical ventilation while exposing the heart. Subsequently, 200 μL of EPCs (4 × 106 cells) were injected into the anterolateral wall of the left ventricle using a 27-gauge insulin syringe. The chest was then closed, and the animals were allowed to recover.
The animal protocol was approved by the regional governmental commission for animal protection (Regierung von Oberbayern) and conformed with the guidelines of the U.S. National Institutes of Health (21).
Cell Enhancement Strategies
The rats were divided into 4 treatment groups. Control rats were injected with EPCs transduced with the reporter gene human NIS. In the group with VEGF overexpression, rats were injected with EPCs that had been transduced with NIS and infected 1 d before transplantation with AdV-encoding VEGF at an MOI of 10. Rats in the statin treatment group were orally administered atorvastatin (10 mg/kg/d), beginning 3 d before the EPC transplantation. Another group of rats received a combination of atorvastatin treatment and VEGF overexpression.
Autoradiographic Imaging
Autoradiographic imaging was performed 3 d after cell transplantation in the statin treatment group (n = 4), VEGF group (n = 5), statin + VEGF group (n = 5), and control group (n = 5). The rats were administered 124I solution (25–30 MBq obtained from Nuklearmedizinische Klinik, University Essen) via the tail vain and were sacrificed 90 min after the administration. The hearts were excised, frozen, and embedded in methylcellulose. Serial short-axis cryosections 20 and 5 μm thick and covering the entire heart at 1-mm intervals were obtained for autoradiography and histology, using a cryostat (HM500OM microtome; Micrim). Autoradiographic exposure for visualization of tracer uptake was performed for 7 d. Tracer distribution was determined by analysis of the digitized autoradiographs (PhosphoImager 445 SI; Molecular Dynamics). Regions of interest were manually defined in a region of focal tracer uptake and in a contralateral normal region of a mid-myocardial section. If no focal myocardial tracer accumulation was observed, a region of interest was placed in the anterolateral wall. The radioactivity values of each region of interest were recorded as background-corrected photostimulated luminescence per area (mm2) and expressed as uptake ratio calculated by dividing the value of the focal region of tracer uptake by the value of the contralateral normal area.
Histology and Immunohistochemistry
Histologic and immunohistochemical stainings were performed using standard techniques. Monoclonal mouse antihuman platelet endothelial cell adhesion molecule-1 antibodies (CD31, clone JC70A, 1:40 dilution; Dako) and antihuman VEGF antibody (Dako) were used for the detection of EPCs and VEGF165 expression in the rat heart. An index of the number of graft cells in the heart was calculated as an average number of human CD31-positive stained cells in the 3 adjacent slices that showed the largest amount of positive cells.
In Vivo PET and Analysis
Imaging studies were performed 1 and 3 d after cell transplantation in the statin + VEGF treatment group (n = 5 on both days) and the control group (n = 5 on both days). The rats were imaged prone on a dedicated small-animal PET scanner (Inveon; Siemens Medical Solutions), and anesthesia with midazolam, fentanyl, and medetomidine was maintained during the entire data acquisition. For injection of activity, a catheter was placed into a tail vein. Data acquisition commenced 60 min after intravenous injection of 124I solution (25–30 MBq) and continued for 30 min to detect NIS-expressing cells. All data were acquired in list-mode format and were graphed into sinograms. Sinograms were reconstructed into a 128 × 128 × 95 voxel image using filtered backprojection with a cutoff at the Nyquist frequency. The reconstructed voxel size was 0.43 × 0.43 × 0.80 mm. Data were normalized and corrected for random events, dead time, and decay. For quantification of tracer uptake, a region of interest was placed manually at the site of cell injection in a transverse slice of the mid ventricle, and uptake values were expressed as mean percentage injected dose per cubic centimeter.
Statistical Analysis
All results were expressed as mean ± SD. Statistical analysis was done with StatMate III (ATMS Co., Ltd.). Continuous variables were compared using the unpaired Student t test, and multiple groups were compared using ANOVA with ranks (Kruskal–Wallis test), followed by the Dunn multiple-contrast hypothesis test to identify the differences of each group. A value of P less than 0.05 was considered statistically significant.
RESULTS
EPCs were analyzed for susceptibility to adenoviral infection using increasing doses of reporter gene–expressing vector. Luciferase assay indicated a linear increase of reporter gene expression with increasing doses. The same was observed for the mean fluorescence intensity of eGFP as measured by flow cytometry. The number of positive cells was already 83% at an MOI of 5. From an MOI of 10 onward, at least 98% of cells were positive, indicating that EPCs are easily infected and that at a higher MOI, expression is increased by multiple copy numbers of vectors per cell as indicated by increasing mean fluorescence intensity. Similarly, VEGF expression increased with increasing virus doses (Fig. 1A). The influence of adenoviral infection on cell growth in vitro was monitored. At an MOI of 10, a slight reduction in cell growth was detected in cells infected with eGFP-Luc expressing AdV, whereas AdV VEGF infection had no influence on cell growth as compared with uninfected controls (Fig. 1B). Next, we analyzed if functionality of NIS on EPCs was changed by additional infection with adenoviral vectors. 99mTc uptake was not altered in AdV VEGF–infected NIS-expressing EPCs, compared with those not AdV VEGF–infected (Fig. 1C).
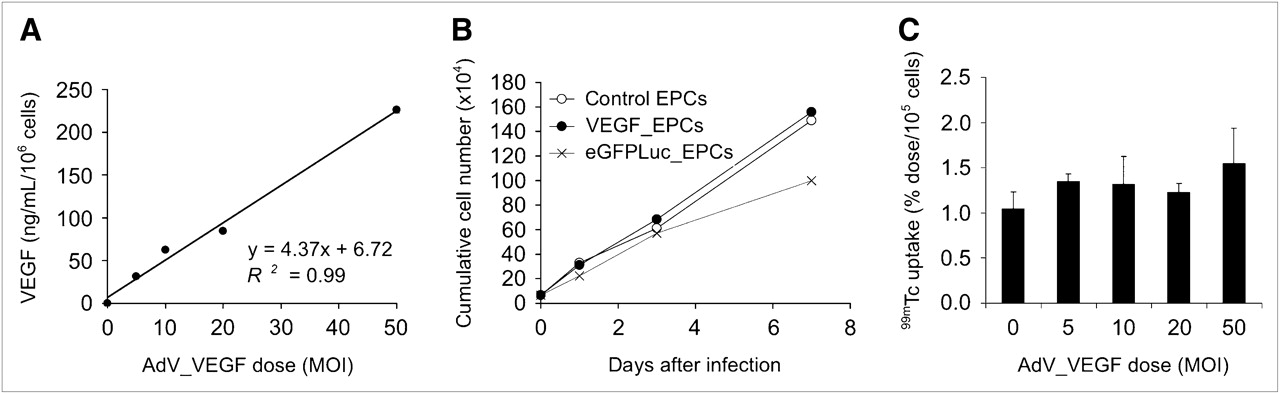
(A) Infection with AdV VEGF with increasing doses of AdV leads to increasing secretion of VEGF into cell culture supernatant, as measured by ELISA. (B) Influence of AdV infection on cell growth was determined at MOI of 10. AdV VEGF infection had no major influence on cumulative cell number. (C) 99mTc uptake into NIS expressing EPCs infected with different doses of AdV VEGF was monitored. There was no increase in uptake with increasing AdV VEGF dose, as compared with uninfected control.
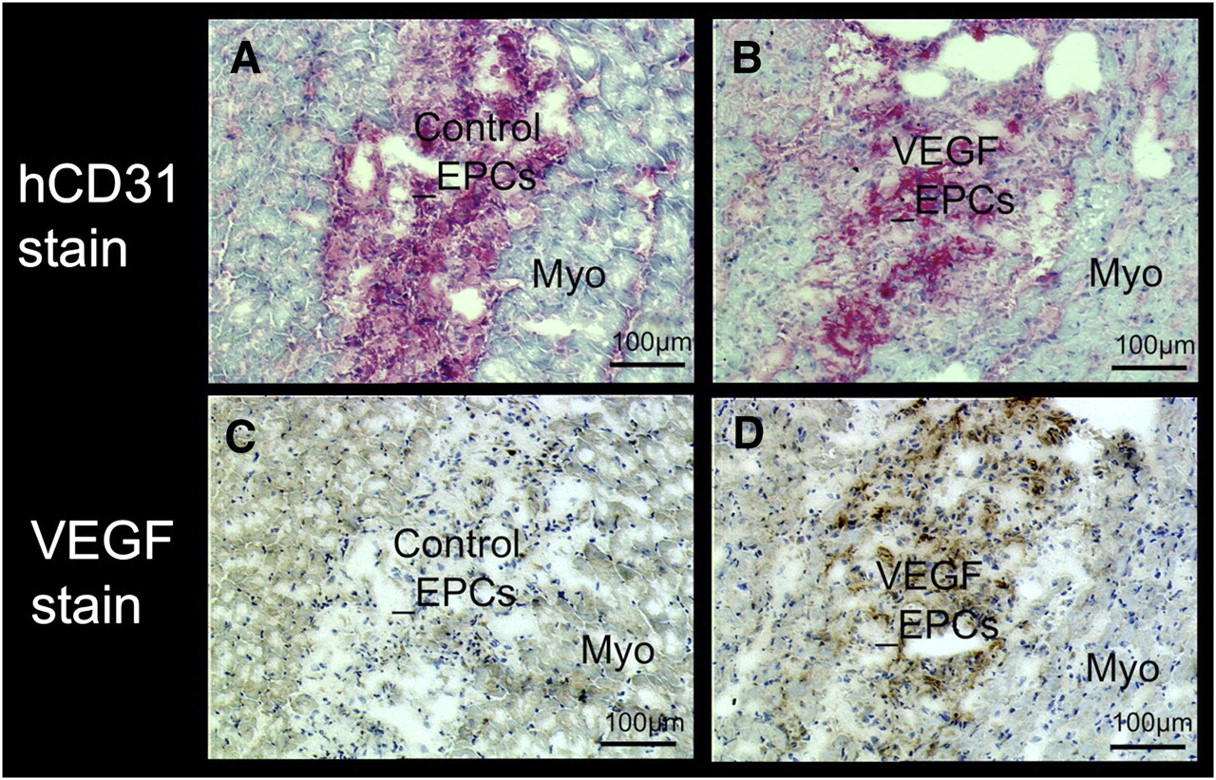
Immunohistochemical analysis with human CD31 antibodies demonstrated the presence of human EPCs in the myocardium at the site of injection. VEGF protein was detectable by immunohistochemistry at the site of cell transplantation only in the rats that received EPCs overexpressing the VEGF gene (Fig. 2).
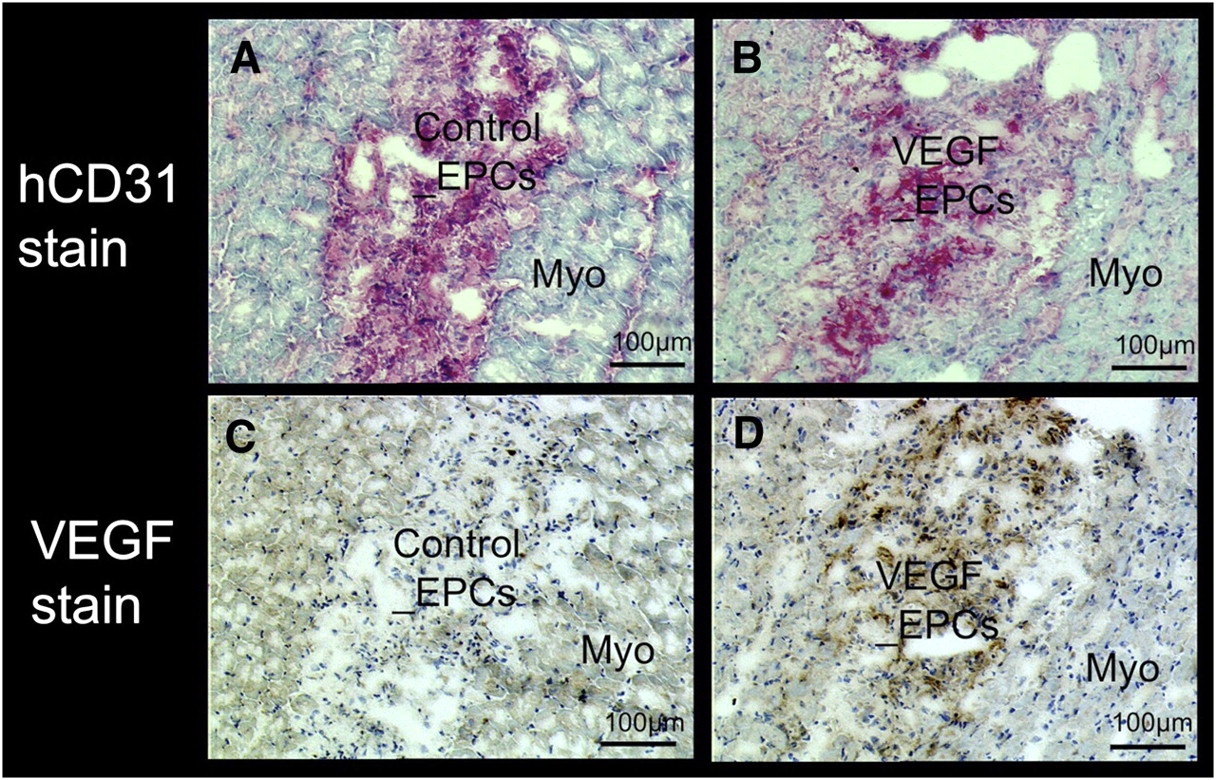
Detection of human EPCs and VEGF protein expression by immunohistochemical staining with human CD31 antibodies (A and B, red) and human VEGF antibodies (C and D, brown). Tissue sections are from rat transplanted with EPCs without either VEGF overexpression or statin pretreatment (control EPCs) (A and C) and EPCs with VEGF overexpression and statin treatment (VEGF EPCs) (B and D). Increased signal of VEGF protein is seen only in EPCs with VEGF overexpression. Myo = rat myocardium.
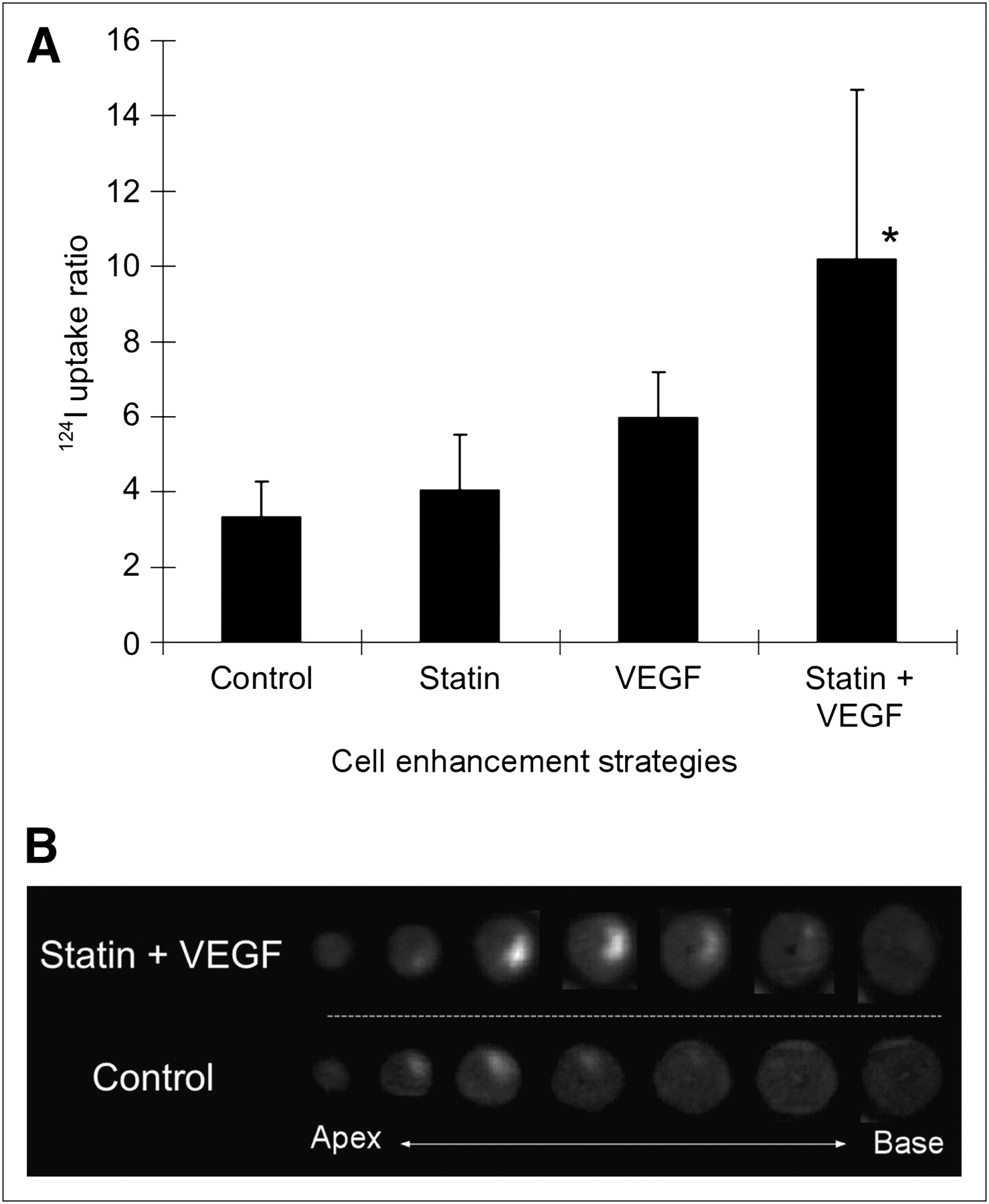
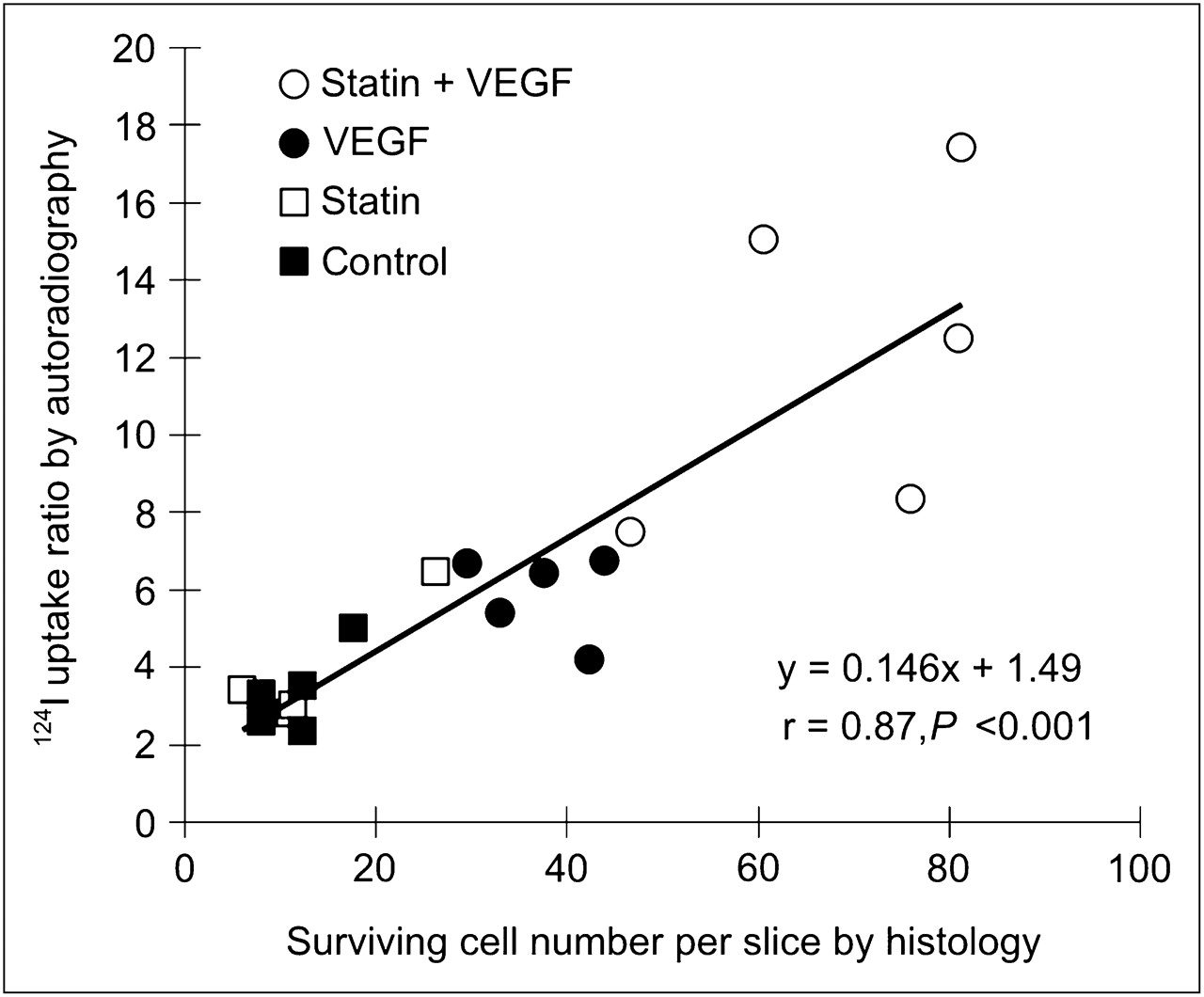
There was myocardial 124I uptake at the site of EPC injection as assessed by ex vivo autoradiography. Quantitatively, 124I uptake was higher in the hearts of rats in the statin + VEGF group than in the controls or the rats treated with statin only (Fig. 3). Additionally, the number of graft cells assessed by immunohistochemistry (human CD31 antibodies) had a significant linear correlation with 124I uptake, indicating that 124I uptake reflects the number of transplanted EPC cells in the heart (Fig. 4).
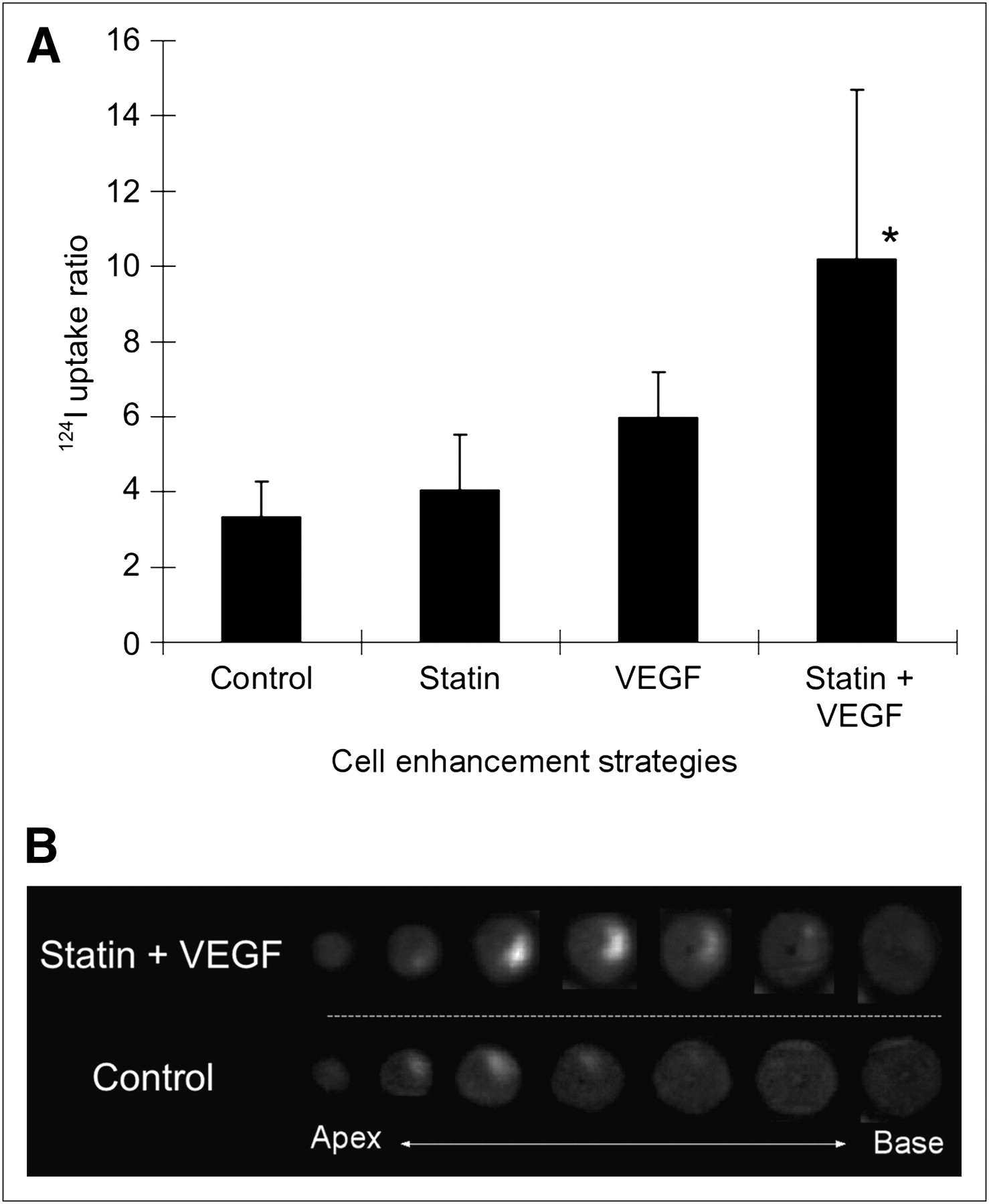
(A) 124I uptake at site of injection normalized to remote myocardium by autoradiography in study groups on day 3 after cell transplantation. 124I uptake is higher in rats with statin treatment and VEGF-overexpressing EPCs than in controls and rats with statin pretreatment only. (B) Representative autoradiographic images of rat hearts of statin + VEGF pretreatment and control groups. Focal 124I uptake is seen at cell-injected site. *P < 0.05.
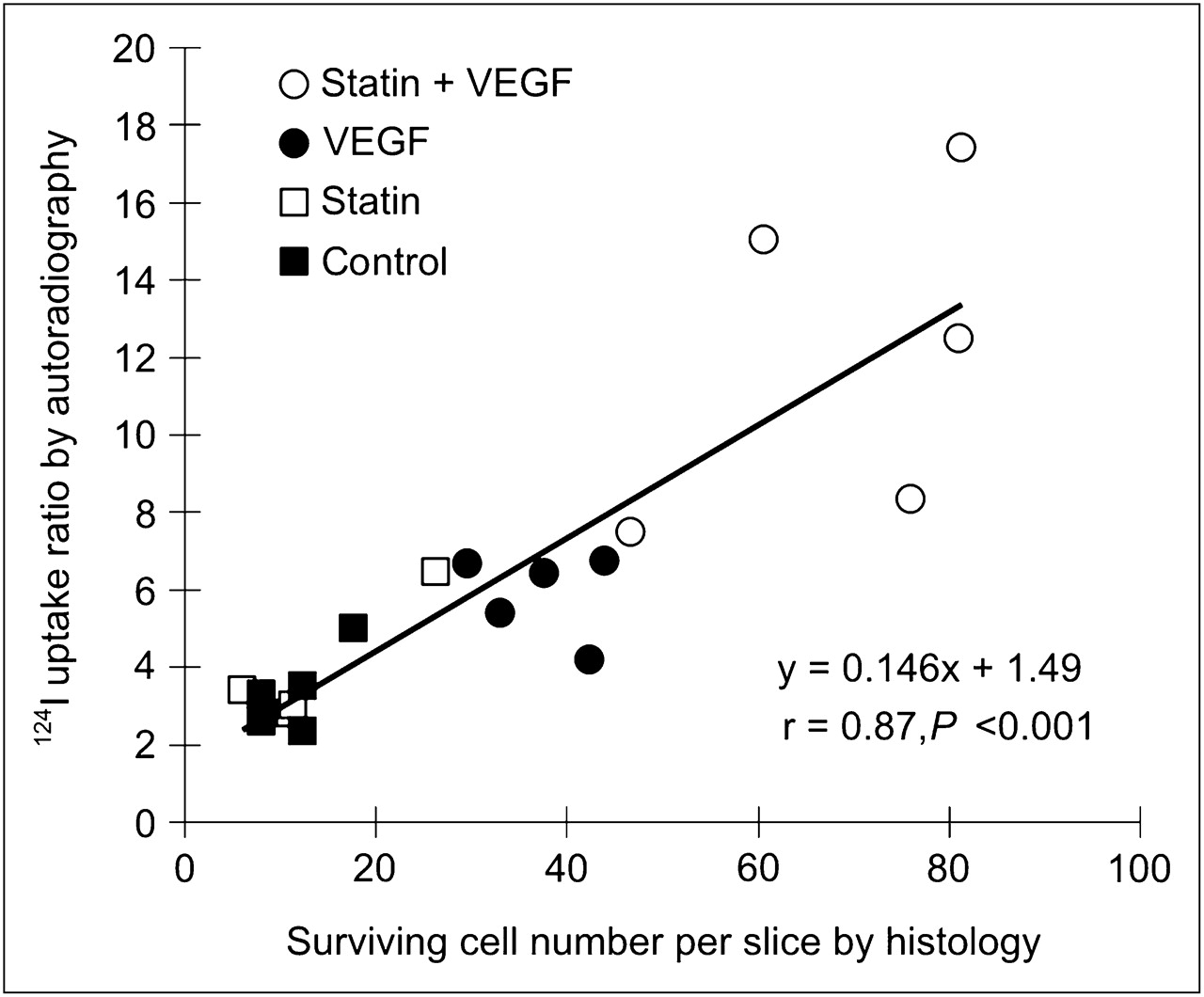
124I uptake at site of injection normalized to remote myocardium by autoradiography vs. number of EPCs determined by immunohistochemistry using human CD31 antibodies. Significant linear correlation between 124I uptake and EPC number is seen.
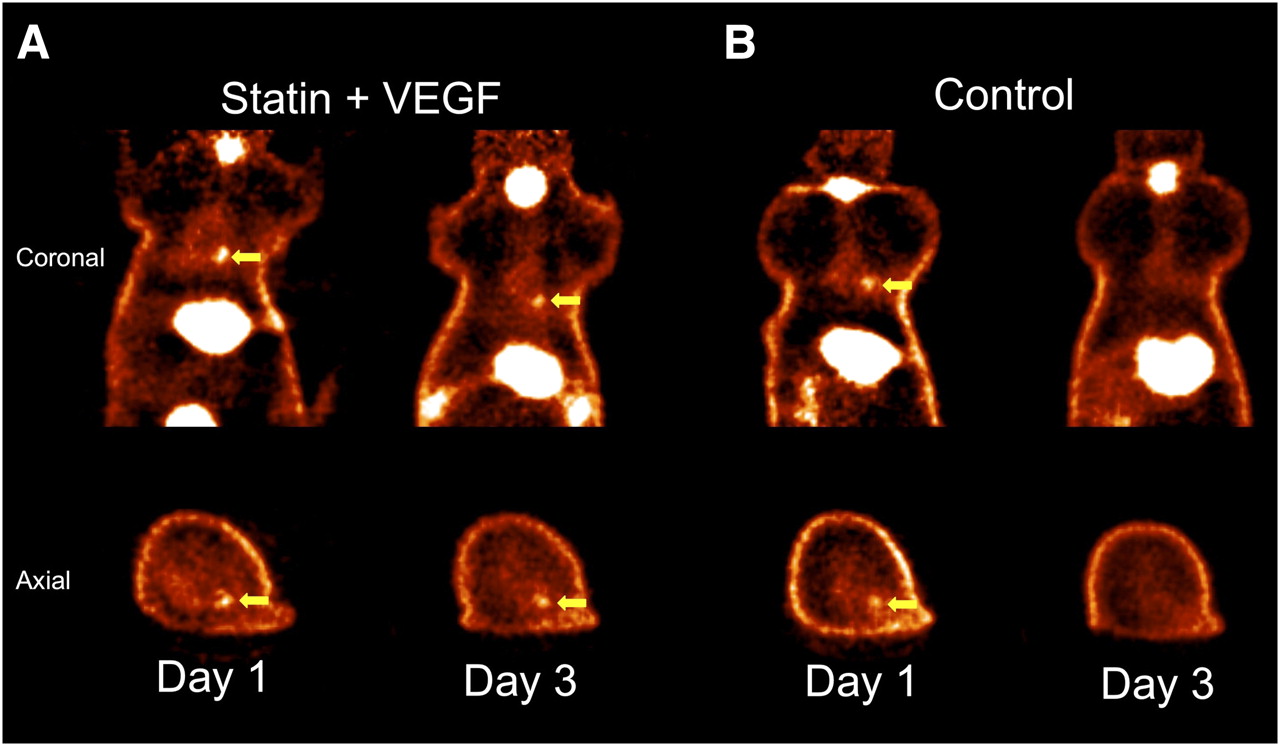
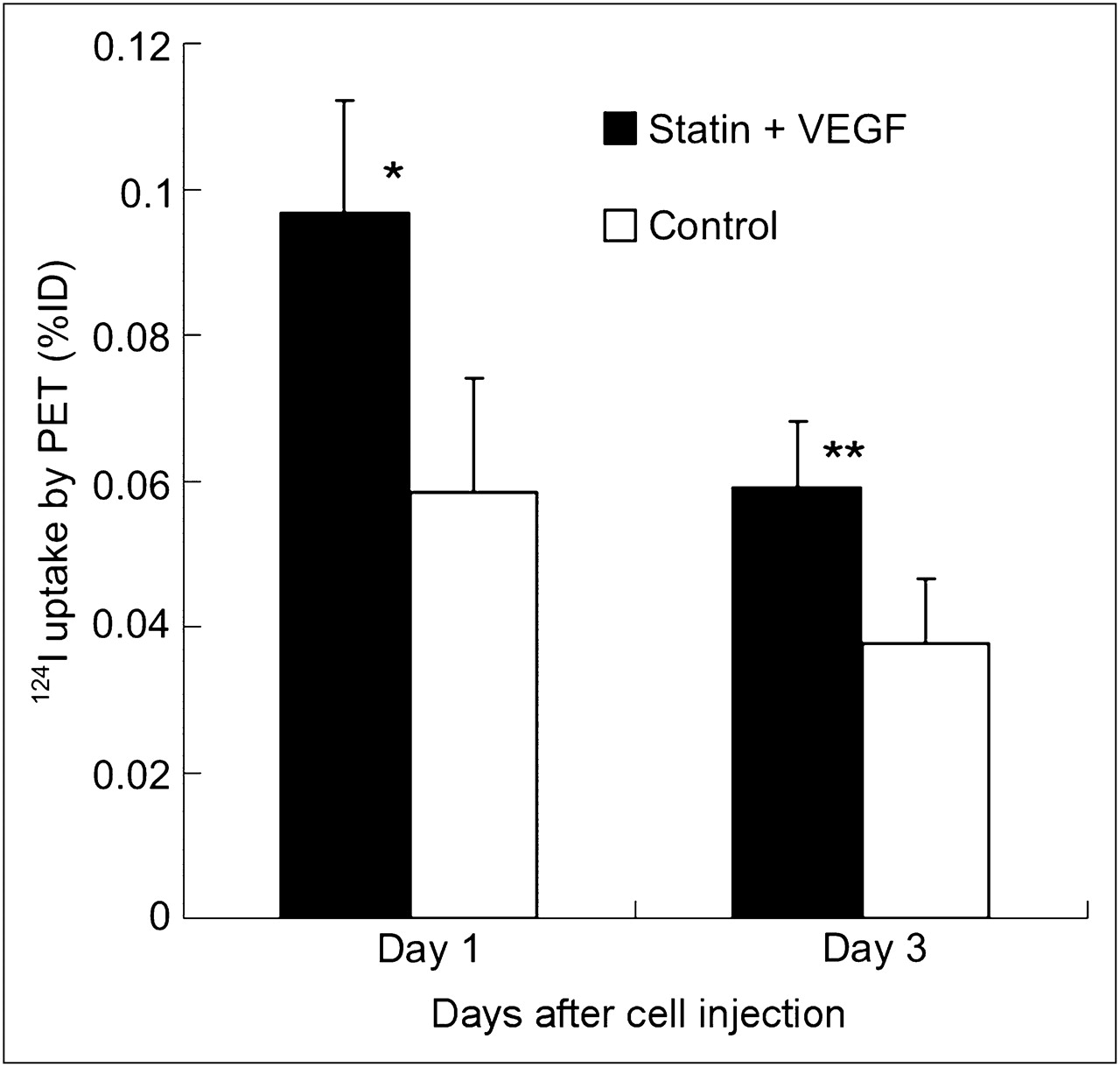
Noninvasive PET after 124I administration successfully visualized the focal 124I accumulation in the heart of all rats 1 d after injection of EPCs. However, 3 d after injection, signal was detectable in rats in the statin + VEGF treatment group but not in controls (Fig. 5). Quantitatively, percentage injected dose of 124I at the site of injection was significantly higher in rats treated with statin and injected with EPCs overexpressing VEGF than in controls at both day 1 and day 3 (Fig. 6).
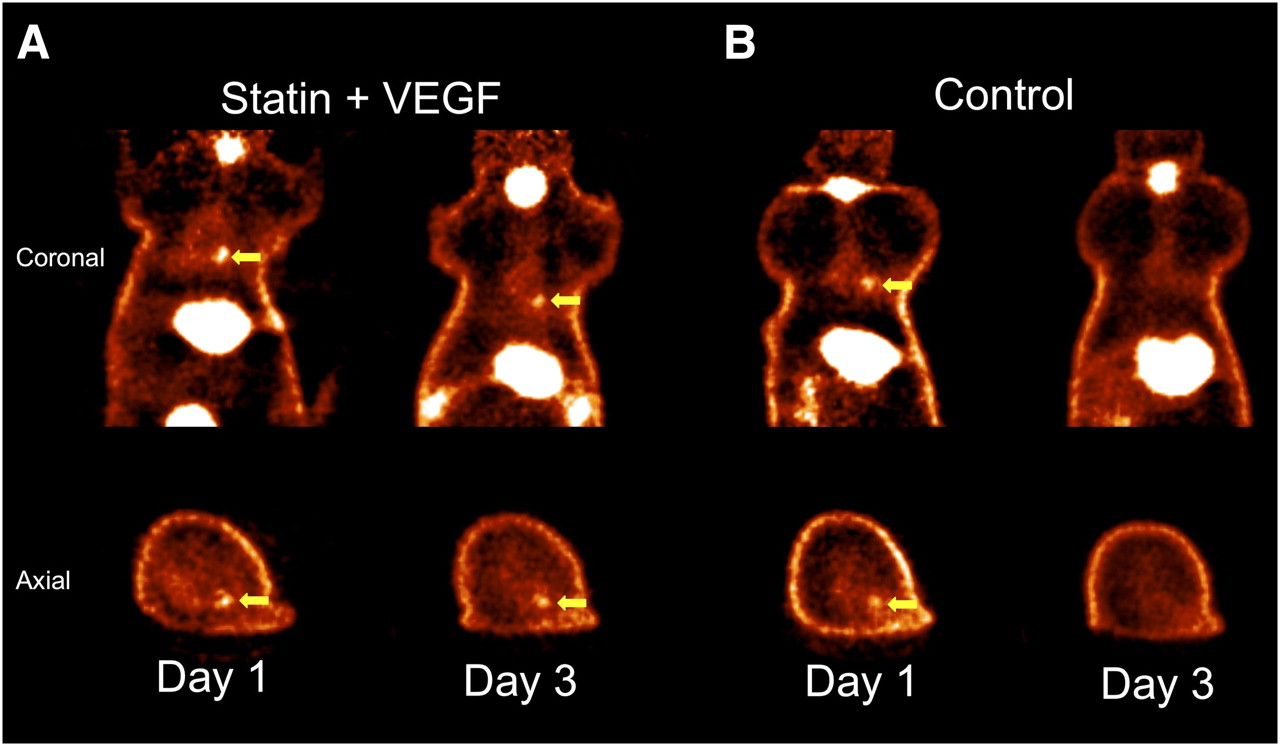
124I PET images at days 1 and 3 after cell transplantation of rat treated with statin and injected with EPCs overexpressing VEGF (A) and control rat injected with normal EPCs (B). Signals from transplanted cells (arrows) were more intense in pretreatment rat than control rat on day 1 and not detectable in controls on day 3.

Results of quantification of 124I uptake (percentage injected dose [%ID]) of EPCs by in vivo PET. Uptake was higher in rats treated with statin and injected with EPCs overexpressing VEGF than in controls on days 1 and 3 after cell transplantation. *P < 0.01. **P < 0.05.
DISCUSSION
This study was the first to investigate reporter gene imaging for monitoring strategies to enhance cell survival in myocardial cell therapy. Reporter gene PET allowed successful visualization of the 124I uptake signal mediated by NIS reporter on human EPCs after intramyocardial cell transplantation (9). Indeed, PET could detect the improved early survival of graft cells using a cell enhancement strategy by combining VEGF overexpression and statin pretreatment. This reporter gene cell imaging technique may allow objective, noninvasive assessments of strategies to enhance graft cell survival.
Decreasing the rapid cell death that occurs within a few days after intramyocardial transplantation of graft cells is of great relevance for the success of cell transplantation therapies (22,23). Some different approaches to enhancing graft cell survival are under investigation (14). Gene transfer techniques to enhance EPC survival were first reported by Muraswa et al. using the human telomerase reverse transcriptase gene (24). Successful improvement of cell survival, proliferation, and neovascularization of EPCs was observed after the cells had been modified with human telomerase reverse transcriptase gene. Other groups tested the effects of VEGF transduction for EPCs (16). VEGF-overexpressing EPCs demonstrated better proliferation and adhesion than nontransferred control EPCs in vitro and enhanced the contribution to neovascularization in mice with hindlimb ischemia. Statin treatment has also demonstrated an improvement in the proliferation, survival, and function of EPCs (13,17). Landmesser et al. suggested the statin improves EPC cell mobilization and myocardial neovascularization by increasing the availability of endothelial nitric oxide (25). Consistent with these studies, we found evidence that VEGF and statin treatment can promote survival of EPCs. However, in our experimental model, neither pretreatment with statin nor overexpression of VEGF alone significantly increased the number of EPCs remaining in the heart 3 d after transplantation as assessed by reporter gene analysis and histology. Only a combination of statin pretreatment with EPCs overexpressing VEGF resulted in a modest but significant increase in the number of EPCs. We speculate that statin pretreatment and VEGF may have a synergistic effect on the survival of transplanted EPCs, but further studies are needed to confirm and elucidate the mechanism of the interaction.
Consistent with our previous experience (9), we observed rapid declines in the number of viable cells within a short time that may be related to immunologic responses toward human cells in rats. It may be that the effects of pretreatment would be more pronounced in the presence of ischemic or infarcted myocardium instead of the healthy myocardium used in this study.
Noninvasive monitoring of graft cell survival by the reporter gene imaging assay may be attractive for finding optimal approaches to maximize the potential of cell transplantation therapy. Our results provide evidence that reporter gene imaging can be used to detect differences in cell numbers early after transplantation. Although absolute quantification of EPCs in the heart is complicated by their patchy distribution, the 124I signal was linearly related to the cell number in myocardial tissue sections obtained at 0.2-mm intervals. The rapid decline in cell numbers in our model resulted in a decrease of 124I PET below the detection limit of PET. Therefore, PET studies beyond a follow-up of 3 d were not feasible, and the value of NIS imaging for prolonged monitoring of cell survival remains to be studied. Although we studied only healthy rats, reporter gene imaging with NIS using a similar approach has previously been shown to be feasible also after cell transplantation in infarcted myocardium (26).
CONCLUSION
Early survival of transplanted EPCs in the rat myocardium is prolonged by pretreatment with a combination of atorvastatin and VEGF. Reporter gene PET, by successfully quantifying the enhancement effect, is an attractive tool for monitoring stem cell survival in vivo.
Acknowledgments
We are grateful to Betina Wagner, Sybille Reder, Axel Weber, Marc Huisman, and Axel Martínez-Möller for technical assistance. We also thank the technologists of the cyclotron and MRI units of the TU München for assistance with conducting experiments. We are grateful to Gola Javadi for her careful editorial assistance. This project was funded by the Deutsche Forschungsgemeinschaft (Be2217/4-1 and -2), by the EU EC-FP6-project DiMI (LSHB-CT-2005-512146), and by the EU Clinigene Network of Excellence (LSHB-CT-2006-018933).
Footnotes
-
↵* Contributed equally to this work.
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication June 29, 2009.
- Accepted for publication July 29, 2009.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}