


Abstract
Visilizumab is an IgG2 humanized monoclonal antibody (mAb) characterized by non-FcγR binding and specific to the CD3 antigen, expressed on more than 95% of circulating resting T-lymphocytes and on activated T-lymphocytes homing in inflamed tissues. We hypothesized that the use of a radiolabeled anti-CD3 antibody might serve as a diagnostic tool for imaging T-cell traffic and lymphocytic infiltration of tissues and organs affected by autoimmune diseases. Here we describe the results of in vitro and animal experiments with 99mTc-succinimidyl-6-hydrazinonicotinate hydrochloride (SHNH)–visilizumab. Methods: For mAb labeling, we used a 2-step method with a heterobifunctional linker SHNH. Several titrations were performed to obtain the best labeling efficiency. In vitro quality controls included stability assay, cysteine challenge, sodium dodecyl sulfate polyacrylamide gel electrophoresis, binding assay, and immunoreactivity assay. In vivo studies by high-resolution images were performed at 6 and 24 h after the injection of 99mTc-SHNH–visilizumab. These included cell-targeting experiments in BALB/c mice xenografted subcutaneously with an increasing number of HuT78 cells in the leg and displaced with an excess of cold antibody. We also studied irradiated severe combined immunodeficient (SCID) mice reconstituted with human peripheral blood mononuclear cells (hPBMCs) and injected with 99mTc-labeled visilizumab or control mAb. After dynamic imaging for 3 h, major organs were removed, counted, and processed for immunohistologic examination. Results: Visilizumab was labeled with HYNIC with high labeling efficiency (>90%) and high specific activity (SA; 10,360–11,100 MBq/mg), with retained biochemical integrity and in vitro binding activity to CD3-positive cells. The in vivo targeting experiment showed a proportional increase of specific uptake with the number of injected cells, both at 6 and at 24 h, and the in vivo competition study demonstrated more than 60% decreased uptake after an excess of unlabeled antibody. In SCID mice, hPBMCs in different tissues were detected by 99mTc-labeled visilizumab and confirmed by histology. Conclusion: Visilizumab can be efficiently labeled with 99mTc with high efficiency and SA and could be a valuable tool for the study of human T-lymphocyte trafficking and lymphocytic infiltration of tissues and organs.
For successful therapy with anti-CD3 monoclonal antibodies (mAbs), it is an important prerequisite that the target organ is indeed infiltrated by CD3-positive cells. Infiltration can be demonstrated by biopsy, although not always, particularly for intraabdominal organs. Furthermore, the biopsy reflects minimally the situation of the whole organ unless multiple random sites are tested. Therefore, we hypothesized that the use of a radiolabeled antibody directed against the CD3 antigen might help for the selective detection of resting and activated T-lymphocytes and thus serve as a diagnostic tool for imaging T-cell traffic and lymphocytic infiltration of tissues and organs affected in autoimmune diseases. Thus, the use of a radiolabeled antibody would provide a rationale for treatment with anti-CD3 and a tool for therapy follow-up.
Visilizumab is an IgG2 isotype humanized monoclonal antibody (mAb) characterized by non-FcγR-binding due to mutation in the upper CH2 region of IgG2 and selective binding to the CD3 antigen (1). The human IgG2 isotype of the mAb decreases its ability to activate human complement or to interact with type I or type III Fc receptors (2).
More than 95% of circulating human peripheral T-cells and activated T-cells in inflamed tissues express CD3 antigen. In fact, there is a general consensus that CD3-positive T-cells may play an important role in inflammatory disease conditions. Several low-mitogenic anti-CD3 monoclonal antibodies have been tested for treatment for type I insulin-dependent diabetes mellitus (3), renal transplant rejection (4), and psoriatic arthritis (5,6). Moreover, a murine IgG2 anti-CD3 mAb OKT3 (muromonab [Orthoclone]; Ortho BioTech) is Food and Drug Administration–approved for the treatment of transplant rejection. The potential therapeutic effect of visilizumab has also been examined in several immune system–related disorders including ulcerative colitis (7), Crohn's disease (8), renal allograft, and acute graft-versus-host disease (9,10). However, besides activity in these diseases, a rapid and severe lymphopenia has been observed after visilizumab infusion in humans (at pharmacologic doses of 10 μg/kg or more). The reason for this transient lymphopenia (that starts as early as 30 min after infusion of antibody) is unknown (11), as it is unknown the organ where lymphocytes migrate from blood after visilizumab infusion.
The rationale of the present study was to radiolabel visilizumab with 99mTc and to check in vitro and in vivo its specificity for CD3-positive cells for the study of human T-lymphocyte trafficking. We also aimed to clarify the fate of human T-lymphocytes after the administration of pharmacologic doses of visilizumab.
MATERIALS AND METHODS
Antibodies
Visilizumab was kindly provided by PDL BioPharma. For all experiments, as control mAb, we used a humanized IgG2 antibody, non-FcR binding like visilizumab but also non-CD3 binding, also kindly provided by PDL BioPharma. We tried both direct and indirect radiolabeling methods to label visilizumab and control mAb with 99mTc, to obtain a high labeling efficiency (LE) and specific activity (SA) without any modification in biologic activity of the antibody.
Labeling of Visilizumab and Control mAb with 99mTc by Indirect Method
Antibodies were labeled by conjugation with the heterobifunctional linker succinimidyl-6-hydrazinonicotinate hydrochloride (SHNH), obtaining a hydrazinonicotinate–antibody conjugate. Antibodies were concentrated using Centricon Ultracel YM-50 (Millipore Corp.) to a concentration of 5 mg/mL and then modified by conjugation with SHNH (SoluLink) in dimethylformamide (Sigma-Aldrich Chemical). In brief, a different molar ratio of SHNH (100 mM in dimethylformamide) was added dropwise to a stirred solution of antibody (20 mM in 0.1 M phosphate buffer) and 100 mM phosphate and 150 mM NaCl buffer solution, pH 7.6–8.0. The mixture was purified by G-25 Sephadex PD10 column (GE Healthcare) using nitrogen-purged cold phosphate-buffered saline (PBS) (pH 7.4) as eluant. To couple the mAb–SHNH complex efficiently with 99mTc, reduce the percentage of colloid formation, and verify the influence of the amount of coligand on LE, titrations of tricine (100 mg/mL; Sigma-Aldrich Chemicals) and SnCl2 (2 mg/mL in 0.1 M HCl; Sigma-Aldrich Chemicals) were performed with the mAb–SHNH complex (100 μg) in 1 M sodium acetate (pH 5.5) and 1,110 MBq of freshly eluted  (100 μL), maintaining a constant volume of reaction.
(100 μL), maintaining a constant volume of reaction.
Labeling of Visilizumab and Control mAb with 99mTc by Direct Method
Both antibodies were also tested for labeling with 99mTc using the 2-mercapthoethanol (2-ME) method as described by Mather and Ellison (12). Briefly, disulfide bridges were reduced using different molar ratios of 2-ME-to-mAb (1,070:1, 2,145:1, and 4,290:1) to achieve the best activation of the antibodies and consequently the highest LE. The activated antibodies were then purified using G-25 Sephadex PD10 columns and nitrogen-purged cold phosphate buffer (pH 7.4) as eluant. Methylene diphosphonic acid (MDP; Amersham) was used as a weak competitive ligand. The bone scan kit (containing 10 mg of MDP, 0.17 mg of SnCl2, and 2 mg of ascorbic acid) was reconstituted with 1 mL of nitrogen-purged normal saline. Different amounts (from 1 to 7 μL) of methylene-diphosphonate were tested with 140 μg of activated antibodies and 370 MBq of  freshly eluted from a 99Mo/99mTc generator to achieve the highest LE.
freshly eluted from a 99Mo/99mTc generator to achieve the highest LE.
Quality Controls
Quality controls were performed using instant thin-layer chromatography–silica gel (ITLC-SG) strips (VWR International). The strips were analyzed by a radioscanner (Bioscan Inc.) to quantitate the percentage of activity incorporated. In 0.9% NaCl solvent (with normal ITLC-SG strips), the following were retention factors (Rfs): 99mTc-labeled antibody, 0; 99mTc-tricine, 99mTc- MDP, and free  , 0.9–1. In NH3:H2O:EtOH (1:5:2) solvent (with albumin-absorbed ITLC-SG strips), Rfs were 99mTc colloids, 0; 99mTc-labeled antibody, 1; and 99mTc tricine and free
, 0.9–1. In NH3:H2O:EtOH (1:5:2) solvent (with albumin-absorbed ITLC-SG strips), Rfs were 99mTc colloids, 0; 99mTc-labeled antibody, 1; and 99mTc tricine and free  , 0.9–1.
, 0.9–1.
The stability of the labeled antibodies was measured in human serum at 37°C up to 24 h. For this purpose, 100 μL of 99mTc-SHNH–visilizumab or 99mTc control mAb were added to 900 μL of fresh human serum and incubated at 37°C. The percentage of free 99mTc or bound to antibody was measured at different time points (1, 3, 6, and 24 h) by ITLC-SG.
A cysteine challenge assay was also performed to check the in vitro stability of the radiolabeled antibody. 99mTc-SHNH–visilizumab was incubated at different cysteine-to-mAb molar ratios, which ranged from 500:1 at the highest cysteine concentration to zero in the absence of cysteine, at 37°C for 1 h. At the end of the incubation time, each reaction mixture was evaluated by ITLC-SG, although all known chemical forms of 99mTc-cysteine have an Rf of 0.5–1 in normal saline.
Possible modifications induced by the conjugation procedure on the visilizumab were tested by sodium dodecyl sulphate polyacrylamide gel electrophoresis (SDS-PAGE) in nonreducing conditions, using Criterion Precast Gel (7.5% Tris-HCl 1.0 mm) (Bio Rad).
In Vitro Competitive Binding Assay
CD3 expression on human peripheral blood mononuclear cells (hPBMCs), HuT78, CEM, and Jurkat cell lines was tested by fluorescence-activated cell sorter analysis after staining cells with a fluorescein isothiocyanate–conjugated anti-CD3 antibody (Becton Dickinson) to verify which cell line presented the highest expression of CD3 receptors. Cells were maintained in a RPMI 1640 culture medium (Sigma-Aldrich Chemical) supplemented with 10% fetal calf serum, 2 mM glutamine, 100 U of penicillin per milliliter, 100 μg of streptomycin per milliliter, 10 mM 0.1 N-(2-hydroxyethyl)piperazine-N′-(2-ethanesulfonic acid) buffer (pH 7.4), and 2 mM sodium pyruvate. Cells were cultured at 4–6 × 105 cells/mL at 37°C in a CO2 incubator for 1 wk.
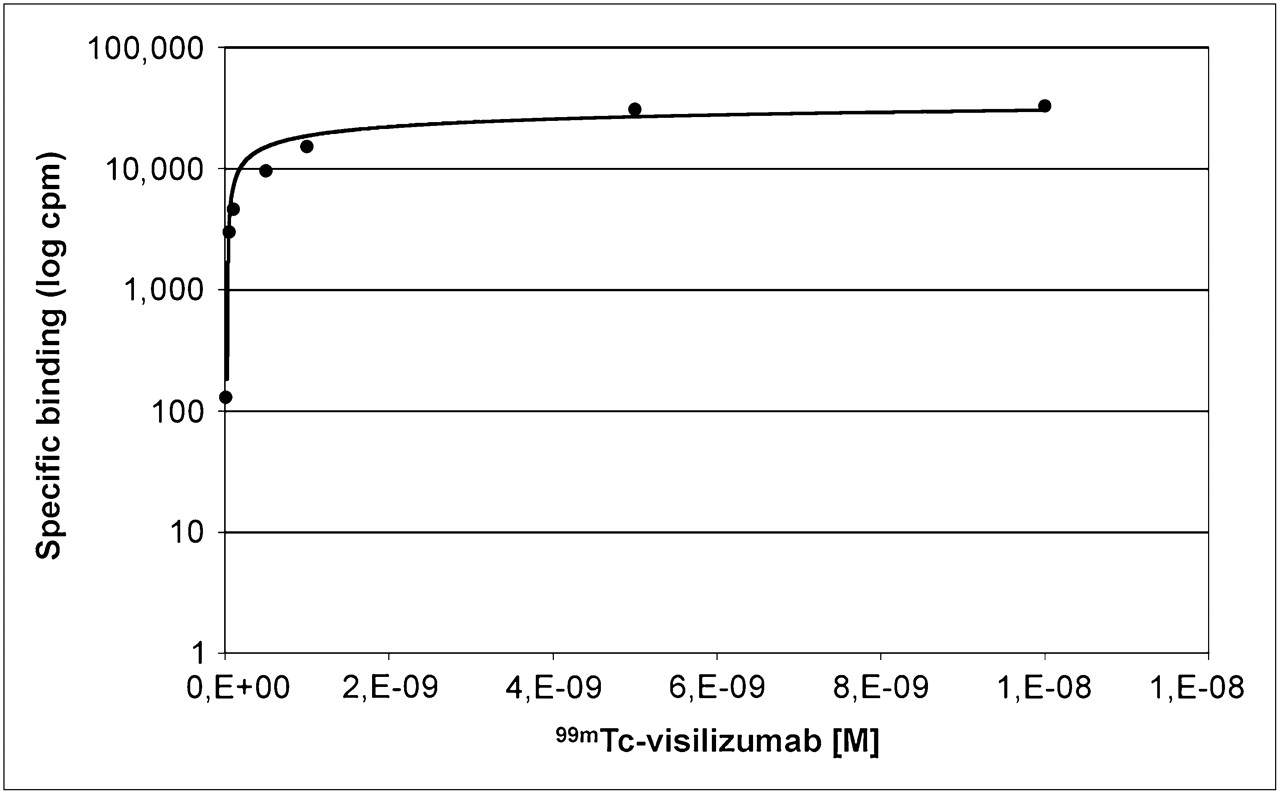
A binding assay was performed on the human lymphoma cell line HuT78 to test the specificity of binding of labeled antibody to human CD3. Briefly, radiolabeled visilizumab was incubated, in triplicate, at different concentrations (from 10 to 0.010 nM) for 60 min at 4°C with 2 × 105 HuT78 cells. Specific binding was determined by performing the assay, in triplicate, in the presence and absence of a 100-fold molar excess of unlabeled visilizumab (100 nM). At the end of the incubation time, cells were harvested by centrifugation (5,000g for 2 min). The supernatant was collected in different vials, and then vials containing cells and supernatants were counted separately for radioactivity in a well γ-counter. The curve of specific binding was generated as the difference between total binding and nonspecific binding.
Immunoreactive Fraction Assay (IRF)
The IRF assay has been adapted with slight modifications from the method described by Lindmo et al. for determining the fraction of immunoreactive antibody by linear extrapolation to conditions representing infinite antigen excess (13).
The IRF assay was performed using a constant concentration of radiolabeled mAb and serial dilutions of hPBMCs. The hPBMCs were isolated from the blood of a single healthy donor, washed 3 times in PBS (pH 7.4), and diluted to a final concentration of 4 × 106 cells/mL in a cold 1% bovine serum albumin (BSA)–PBS solution. All experiments were performed in duplicate. Radiolabeled mAb, at a constant concentration of 50 ng/mL in a 1% BSA–PBS solution, was added to different amounts of cells (final concentration ranging from 2.6 × 106 to 0.08 × 106 cells/mL). Cells were incubated for 2 h at 4°C and then washed twice with 500 μL of a cold 1% BSA–PBS solution before cell-associated radioactivity in a single well γ-counter was counted.
In Vivo Experiments by High-Resolution Imaging
The high-resolution γ-camera (HRC) (Li-tech; S.r.l.) has been previously described (14,15). The camera is composed of a crystal collimator coupled to an H8500 (Hamamatsu) position-sensitive photomultiplier tube, charge readout electronics, and data acquisition system. The system performs real-time acquisitions with a refresh time of 0.5 s. The HRC energy resolution is about 20% at 140 keV (99mTc). The sensitivity is 210 cps/MBq, and the uniformity is ±5%; the system provides 2.2-mm intrinsic resolution suitable for our imaging experiments in vivo in small animals.
In Vivo Targeting Experiment with HuT78 Cells
To evaluate the ability of radiolabeled visilizumab to bind to HuT78 cells in vivo, we performed a targeting experiment in 9 athymic nude BALB/c nu/nu mice. Mice were divided into 3 groups and subcutaneously implanted with an increasing number of HuT78 cells in the left thigh (5 × 106, 10 × 106, or 20 × 106 cells, respectively). In the right thigh, mice were implanted with the same number of CD3-negative tumor cells (TPC1) as the control (16). After 2 h, mice were injected in the tail vein with 11.1 MBq (approximately 1 μg) of radiolabeled visilizumab, and HRC images were acquired after 6 and 24 h. Regions of interest were drawn over the left (target) and right (background) thighs, and target-to-background (T/B) ratios were calculated.
In Vivo Competition Study of 99mTc-SHNH–Visilizumab
Eight nude BALB/c nu/nu mice underwent a competition study to assess to what extent the uptake and retention of 99mTc-labeled anti-CD3 mAb to CD3-positive cells was displaced by an excess of unlabeled antibody. To this aim, mice were subcutaneously implanted with 20 × 106 hPBMCs in Matrigel (BD Biosciences) in the right thigh. As a control, in the left thigh mice were implanted with the same volume of Matrigel, without cells. Four mice were preinjected intravenously with a 100-fold excess of unlabeled visilizumab immediately before the second injection of a tracer dose of 11.1 MBq (∼1 μg) of 99mTc-visilizumab, in the tail vein; the remaining 4 mice received only 99mTc-visilizumab. HRC images were acquired after 6 and 24 h. Regions of interest were drawn over the right (target) and left (background) thighs, and T/B ratios were calculated.
Biodistribution of 99mTc-Labeled Visilizumab or 99mTc-Labeled Control mAb in Severe Combined Immunodeficient (SCID) Mice Reconstituted with hPBMCs
The aim of these experiments was to check the biodistribution of 99mTc-labeled visilizumab or control mAb in SCID mice reconstituted with hPBMCs and treated with a pharmacologic dose of unlabeled visilizumab. Female SCID mice (10–12 wk old; Charles River Laboratories) were used. Mice were maintained in a specific pathogen-free facility without prophylactic antibiotics for 2–3 wk, and they received sterilized food and water ad libitum (17). One day before hPBMC administration, recipient SCID mice were depleted of natural killer cells and monocytes by whole-body irradiation with a 3-Gy 137Cs source (18). All animal studies were performed in compliance with the local Ethical Committee and according to national regulations.
Immediately after reconstitution (intravenously, 8 × 106 hPBMCs per mouse), 3 mice were injected intravenously with 300 ng (10 μg/kg dose) of visilizumab, part of which was 99mTc-labeled (∼30 ng, 0.37 MBq). As a control, 3 mice were injected intravenously with 300 ng (10 μg/kg dose) of control mAb, part of which was 99mTc-labeled (∼140 ng, 0.37 MBq). Sequential images were acquired of all mice with the HRC at 1, 2, 3, 4, 5, 10, 15, 30, 45, 60, 90, 120, and 180 min after visilizumab or control mAb injection. At the end of the imaging schedule, all mice were killed by neck dislocation, and major organs and tissues were removed (blood, lungs, liver, spleen, small bowel, large bowel, and kidneys), weighed, and counted for radioactivity in a single-well γ-counter. Organ radioactivity was represented as the percentage radioactivity per gram of tissue.
Histology and Immunoperoxidase Staining of Mouse Organs
To confirm the presence of hPBMCs in different tissues after visilizumab (or control mAb) infusion, we histologically evaluated tissues from SCID mice at different time points. Specifically, organs were stored in formalin vials and paraffin-embedded. Five-millimeter sections of major organs were freed of paraffin, and endogenous peroxidase activity was blocked with H2O2. A primary antibody against human CD3 (1:200 dilution; NeoMarkers) was incubated for 1 h at room temperature, followed by a secondary antibody incubation (biotinylated goat antimouse, 1:40 dilution) for 30 min at room temperature. Then, avidin biotin amplification (ABC kit; Dako) was added for 30 min. Incubation with a 3-amino-9-ethylcarbazole chromogen kit (Sigma-Aldrich Chemical) at room temperature for 5–10 min produced a red reaction pigment. CD3-positive cells were counted separately at a magnification of ×400 using a test grid with a 0.22 mm2 area.
RESULTS
Labeling of Visilizumab and Control mAb with 99mTc by Indirect Method
The best molar ratio for conjugation of SHNH to mAb was 20:1. An amount of 10 μL of tricine (100 mg/mL) and 10 μL of SnCl2 (2 mg/mL) was found to be the best for the highest LE with the lowest percentage of colloids to efficiently couple the visilizumab–SHNH conjugate (100 μg) with 99mTc. A high LE (≥90%) was achieved for the 99mTc-SHNH–visilizumab complex with a high SA of 10,360–11,100 MBq/mg after 60 min of incubation using SHNH as a heterobifunctional linker. On the other hand, for the 99mTc-SHNH–control mAb complex, a lower LE (<40%) with low SA (<4,440 MBq/mg) was achieved. In SHNH determination using o-sulphonic benzaldehyde, an average of 4–10 hydrazino groups was found, conjugated to each molecule of visilizumab. Because of the low LE of the control mAb, we did not use this labeling method; however, we selected this labeling method for visilizumab.
Labeling of Visilizumab and Control mAb with 99mTc by Direct Method
For both antibodies, the highest LE was obtained using a molar ratio of 2,145:1 (2-ME:mAb). The control mAb showed the highest LE, with a negligible amount of colloids, on adding only 1 μL of MDP (MDP kit). A low LE and SA were achieved using this radiolabeling method for visilizumab, whereas for the control mAb a high LE (∼99%) was achieved, thus avoiding G-25 Sephadex PD10 column purification. For the control mAb, we used this labeling method for in vivo studies despite an SA (≥2,600 MBq/mg) that was lower than that obtained for visilizumab using the indirect labeling method.
Quality Controls
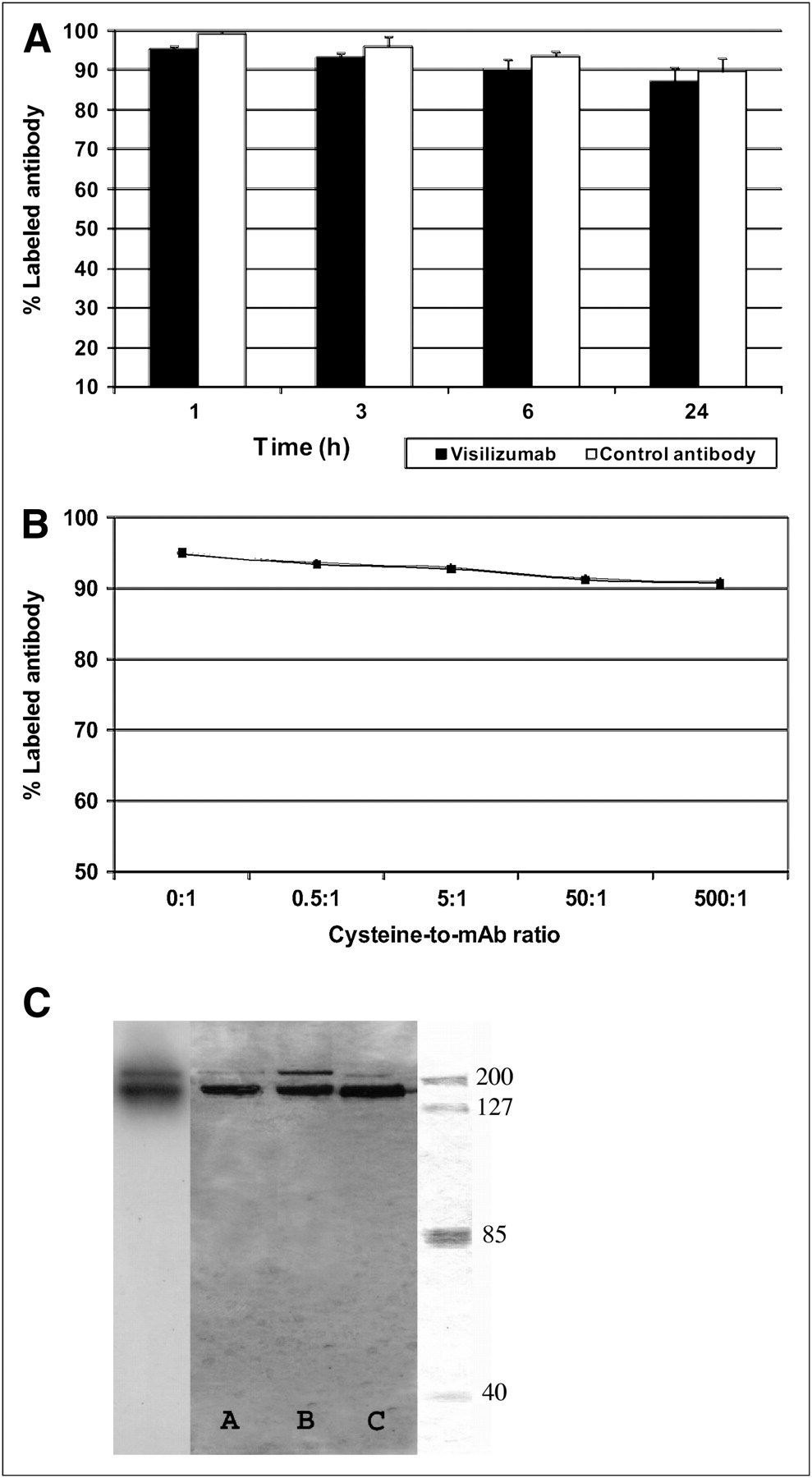
Both the 99mTc-SHNH–visilizumab and the 99mTc control mAb were stable when incubated in human serum at 37°C (87% for visilizumab and 89% for control mAb) at 24 h, as shown in Figure 1A. The cysteine challenge assay also demonstrated high stability up to a 500:1 ratio between cysteine and radiolabeled mAb (Fig. 1B).
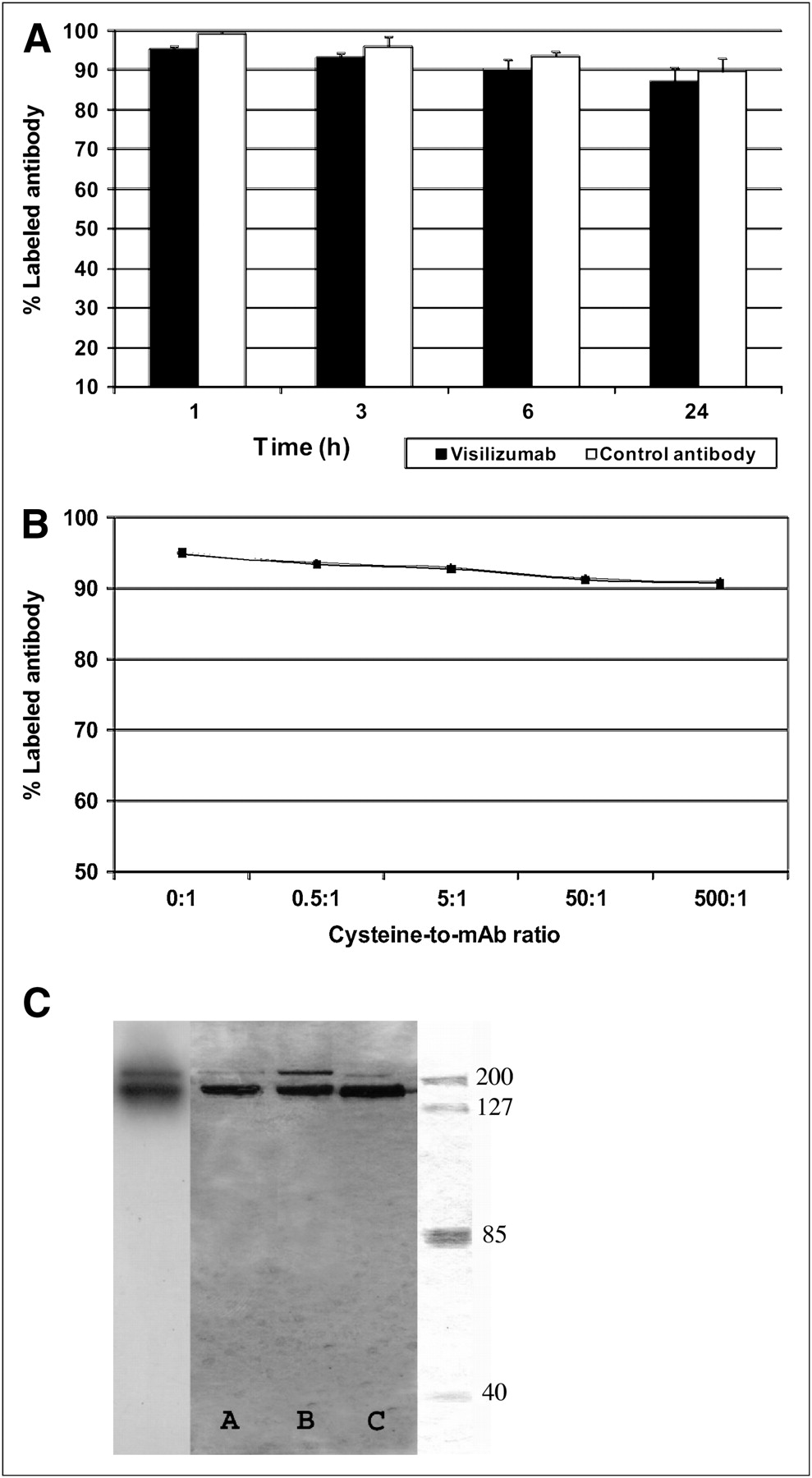
(A) Stability of 99mTc control mAb and 99mTc-SHNH–visilizumab in plasma assessed by ITLC-SG at different time points. (B) Cysteine challenge assay demonstrating high stability of 99mTc-SHNH–visilizumab assessed by ITLC-SG at increasing ratio between cysteine and mAb. (C) SDS-PAGE of 99mTc-SHNH–visilizumab performed in nonreducing condition showing conjugated (lane A), labeled (lane B), and native (lane C) and associated radioactivity at level of conjugated antibody and at level of possible dimers of visilizumab (300 kDa).
SDS-PAGE of labeled, conjugated, and native visilizumab (Fig. 1C) showed no detectable modification of the molecule (in molecular weight), despite conjugation of 4–10 molecules of SHNH per molecule of antibody, as shown by a single band at 150 kDa. A minor band with high molecular weight (300 kDa) was found, possibly due to the presence of dimers of antibody in all lanes and in the autoradiographic lane, despite most radioactivity being associated with the 150-kDa band of intact antibody.
In Vitro Competitive Binding Assay
When stained with fluorescein isothiocyanate–conjugated anti-CD3 antibody, hPBMCs showed a mean fluorescence intensity of 300 (80% positive cells), CEM of 38 (50% positive cells), HuT78 of 18 (>95% positive cells), and Jurkat cells of 30 (60% positive cells). We therefore used hPBMCs and HuT78 for different experiments. Specific saturation of receptors on HuT78 cells was obtained with concentrations of radiolabeled visilizumab above 5 × 10−10 M (Fig. 2). Radiolabeled antibody binding was displaced by a 100-fold molar excess of unlabeled antibody, and this showed that visilizumab retained its specific binding activity with CD3 receptors expressed on HuT78 cells, even after the radiolabeling with 99mTc.
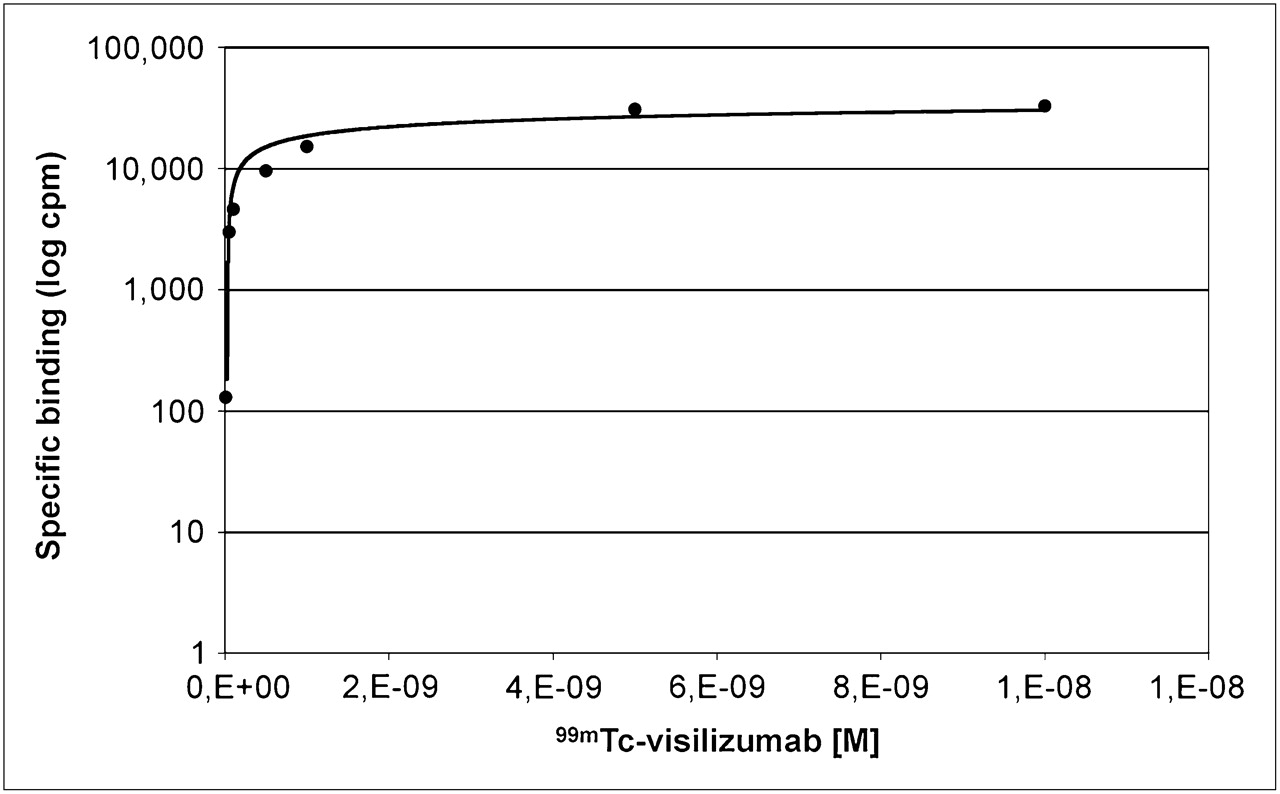
Results of binding assay of labeled visilizumab to HuT78 cells. cpm = counts/min.
IRF Assay
The immunoreactive fraction of radiolabeled visilizumab calculated in 2 experiments was 68% and 75%, respectively.
In Vivo Targeting Experiment with HuT78 Cells
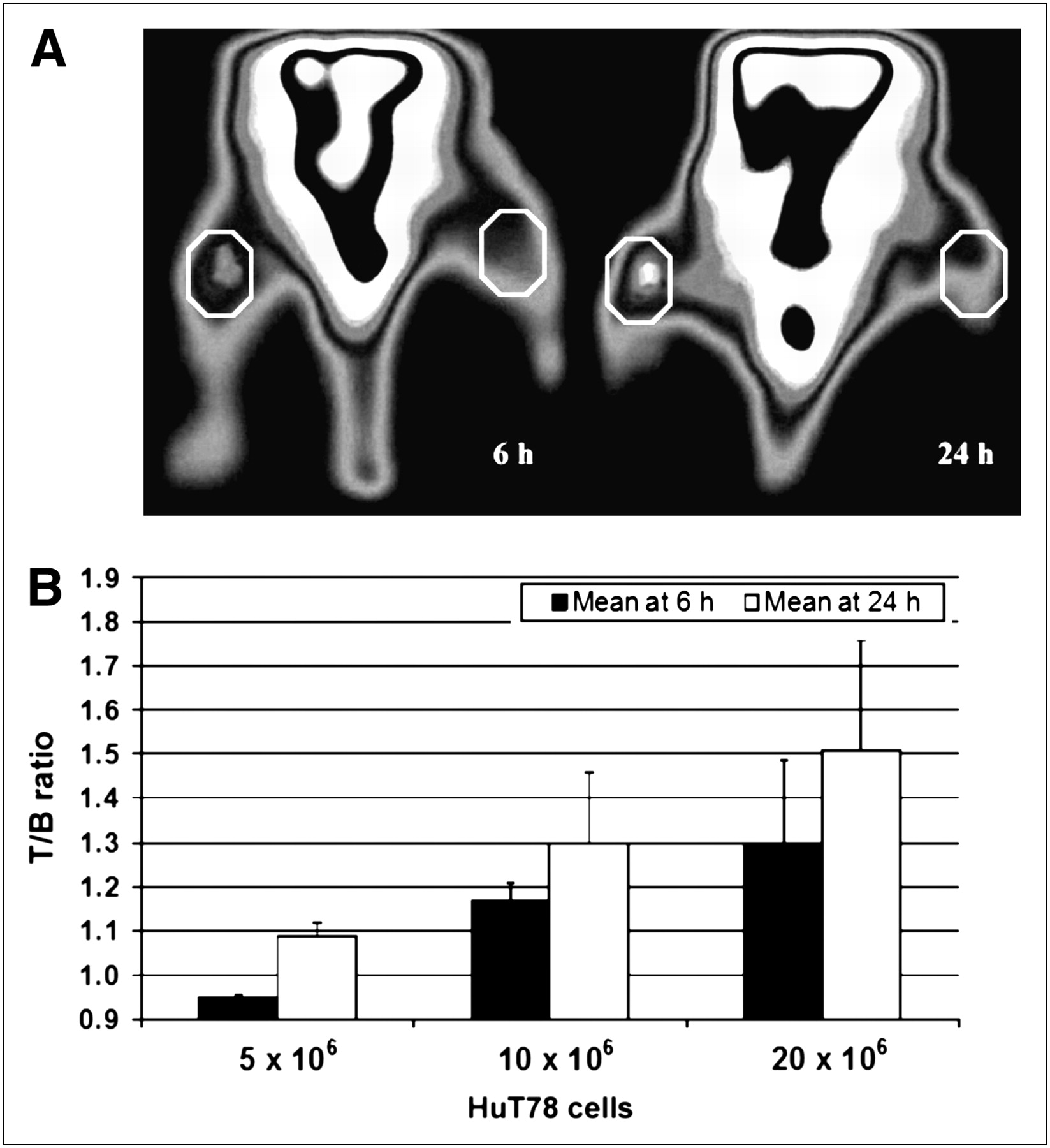
CD3-positive cells were detected by HRC imaging in mice implanted with 20 × 106 HuT78 cells (Fig. 3A). The quantification of 99mTc-SHNH–visilizumab uptake showed that the T/B ratio increased significantly with the number of cells both at 6 and at 24 h after injection (0.98 ± 0.03 for 5 × 106 cells, 1.17 ± 0.03 for 10 × 106 cells, and 1.34 ± 0.12 for 20 × 106 cells at 6 h; and 1.08 ± 0.06 for 5 × 106 cells, 1.30 ± 0.17 for 10 × 106 cells, and 1.56 ± 0.13 for 20 × 106 cells at 24 h) (Fig. 3B). We also observed a small but statistically nonsignificant increase of uptake to cells from 6 to 24 h that may be explained by the fast binding kinetics of labeled mAb to target cells (within a few hours from injection), with no further significant increase with time.
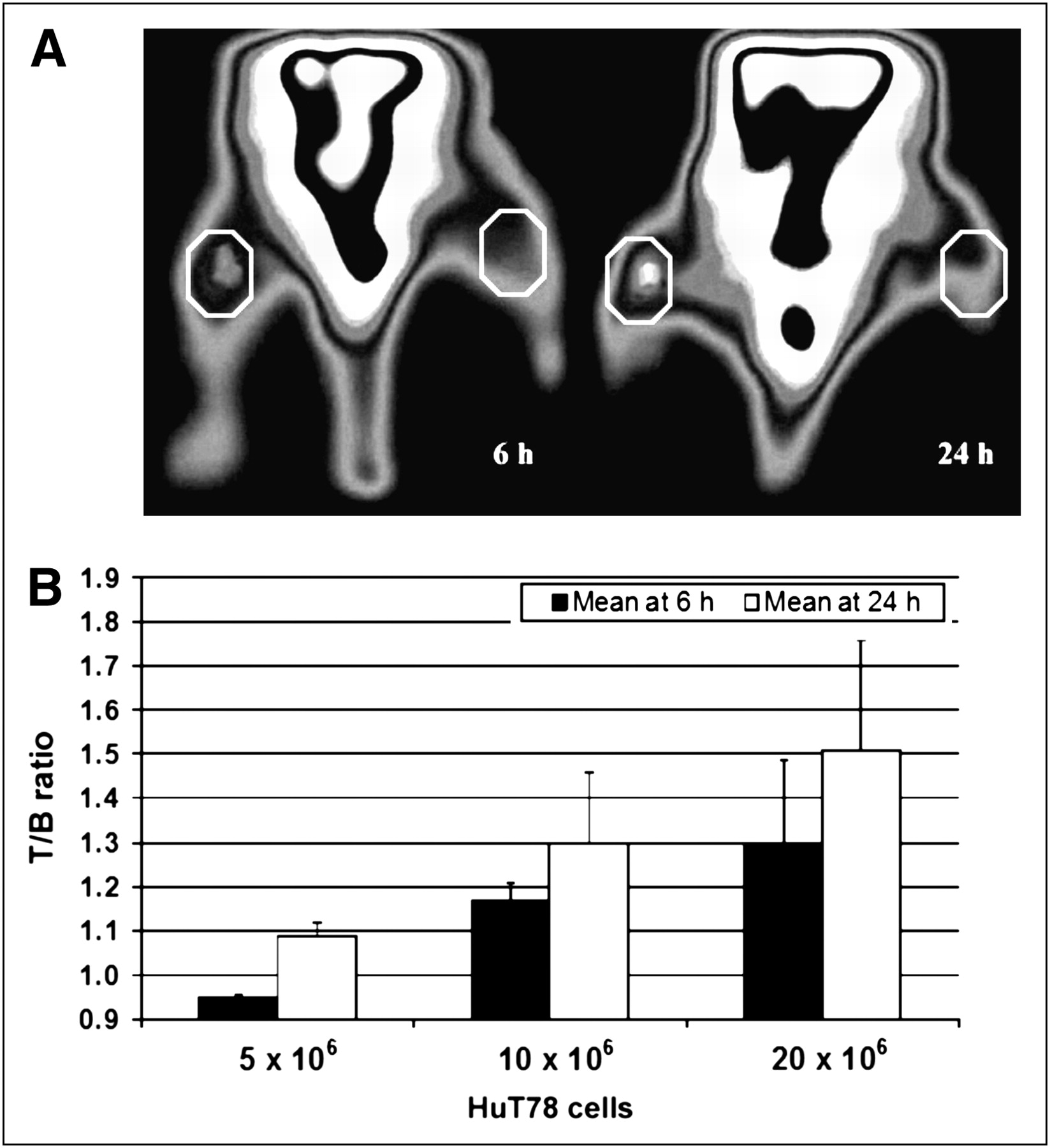
(A) Dorsal scintigraphic images obtained with HRC, at 6 and 24 h in mice xenografted with 20 × 106 HuT78 tumor cells in left thigh and 20 × 106 TPC1 control cells in right thigh. Mice were injected with 11.1 MBq of 99mTc-SHNH–visilizumab. Higher uptake to HuT78 cells is visible as compared with CD3-negative cells. Regions of interests for T/B calculation are also shown. (B) Mean ± SD of T/B ratios calculated for 3 groups of mice xenografted with 5 × 106, 10 × 106, and 20 × 106 cells, respectively.
In Vivo Competition Study of 99mTc-SHNH–Visilizumab
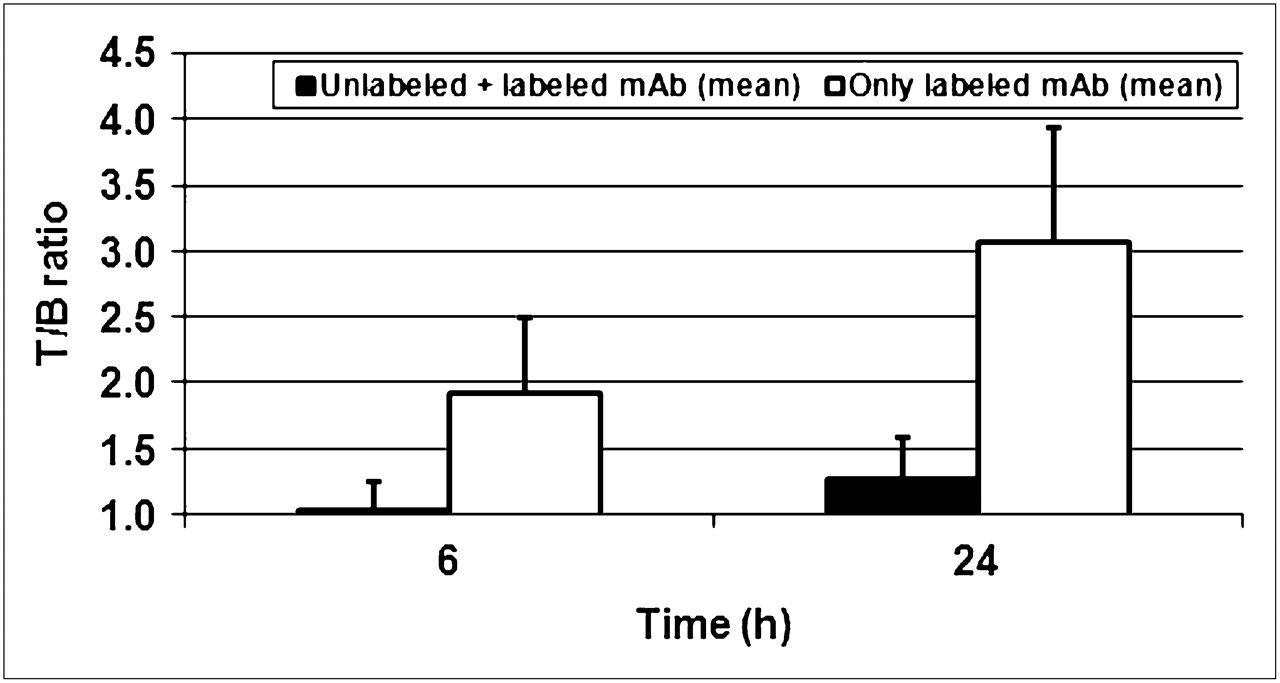
As shown in Figure 4, the uptake of radiolabeled anti-CD3 mAb decreased after an excess of unlabeled anti-CD3 mAb. Quantitative analysis of uptake showed a significant decrease (96% at 6 h and 87% at 24 h) in T/B ratio in mice preinjected with cold visilizumab versus control mice (1.91 ± 0.6 and 1.04 ± 0.2 at 6 h; 3.06 ± 0.8 and 1.27 ± 0.3 at 24 h, control versus displaced animals, respectively, all P < 0.05).
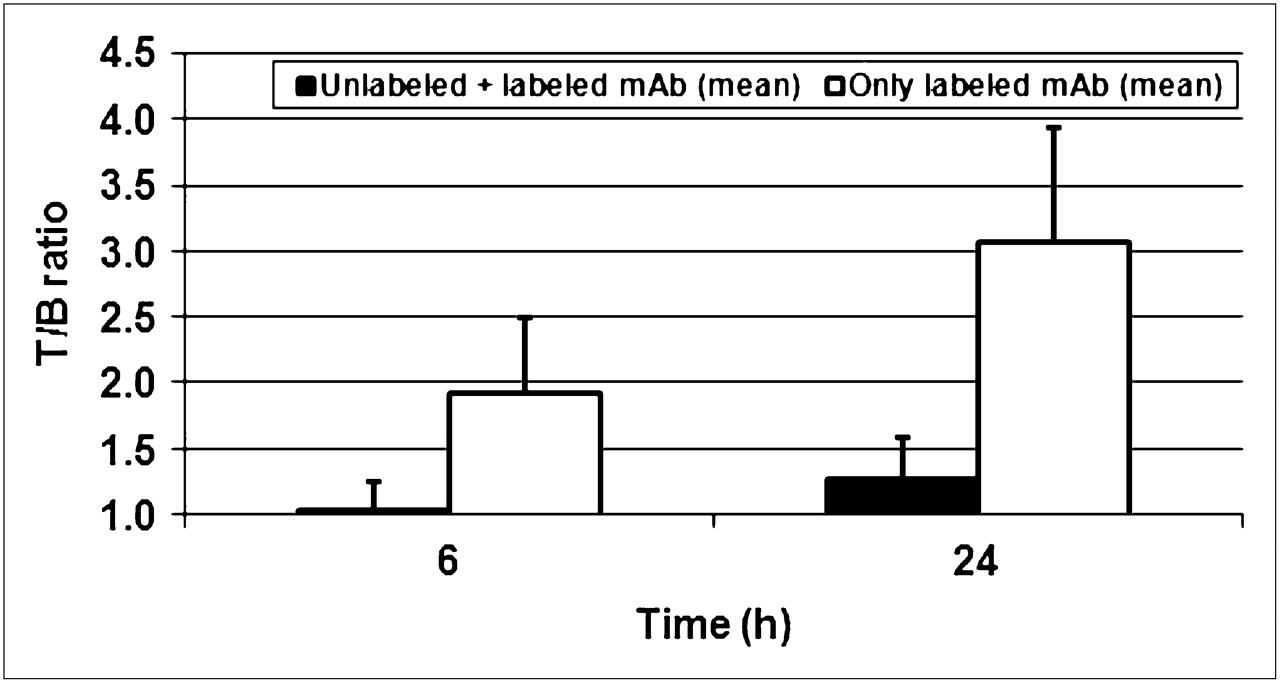
Mean ± SD of T/B ratios calculated for 2 groups of mice xenografted with 20 × 106 hPBMCs and injected with either 100-fold excess of unlabeled visilizumab immediately before tracer dose of 11.1 MBq (∼1 μg) of 99mTc-visilizumab or only tracer dose of 99mTc-visilizumab (as control mice).
Biodistribution of 99mTc-Labeled Visilizumab or 99mTc-Labeled Control mAb in SCID Mice Reconstituted with hPBMCs
Experiments performed on SCID mice reconstituted with hPBMCs and injected simultaneously with 99mTc-labeled visilizumab or 99mTc-labeled control mAb showed a different migration pattern of lymphocytes (as detected by histologic analysis) and different biodistribution of radioactivity as detected by scintigraphic imaging with an HRC.
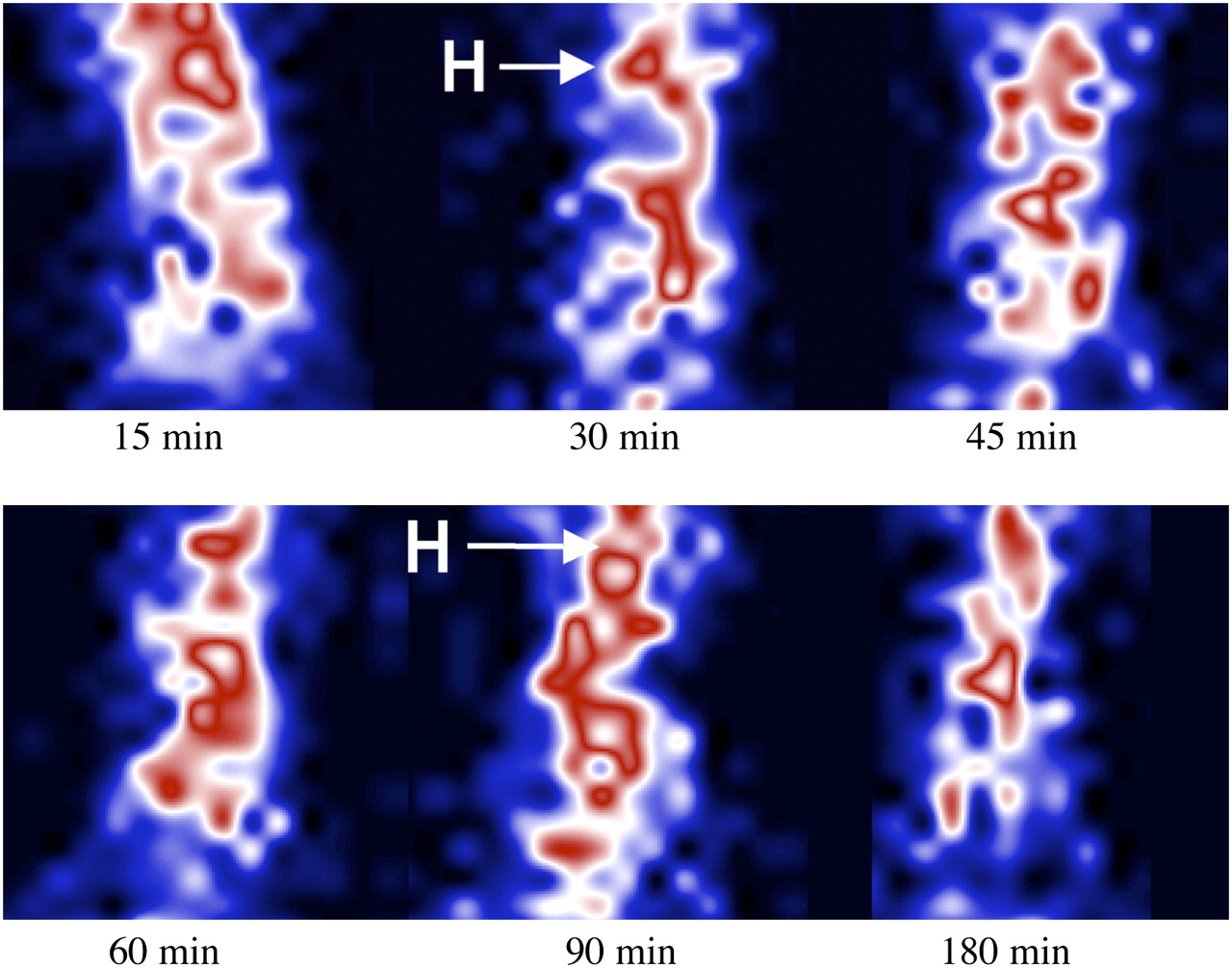
In particular, 99mTc-SHNH–visilizumab, by binding to lymphocytes in blood, induced cells to accumulate in the liver, spleen, and small bowel of the SCID mice (Fig. 5). By contrast, 99mTc-labeled control mAb showed a long resident time in the blood of mice (Fig. 6), with little accumulation of radioactivity and cells in the liver and small bowel. In particular, the calculation of radioactivity per gram of organ at 3 h showed a significant difference between visilizumab and control mAb in blood, with the radioactivity being higher in mice injected with control mAb (>60%). In the liver (>400%), spleen (>720%), and small bowel (>230%), radioactivity was higher in mice injected with visilizumab (Fig. 7). Minor and nonstatistically significant differences were found in the radioactivity counts in other organs including the lung, spleen, kidney, and large bowel, with the counts being higher for visilizumab than for control mAb (data not shown). Thus, it seems that after an intravenous injection of a pharmacologic dose of visilizumab, lymphocytes migrate from the blood to the liver, spleen, and small bowel. This finding was confirmed for the spleen and small bowel by histologic examination of tissues.
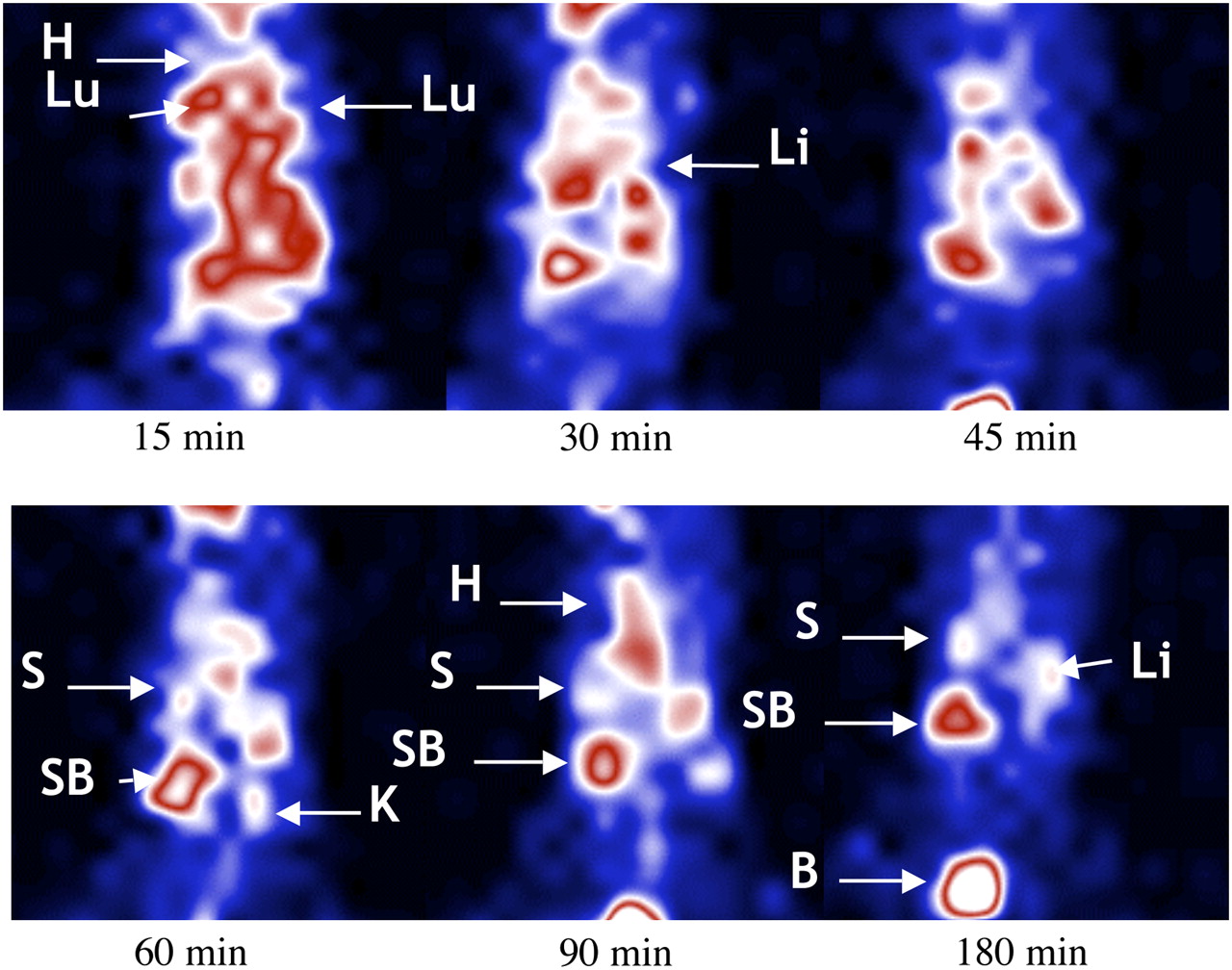
Scintigraphic images (dorsal view) of SCID mice injected simultaneously with 8 × 106 unlabeled hPBMCs and 300 ng of visilizumab, part of which was 99mTc-labeled (0.37 MBq, 30 ng). Images were acquired after 15, 30, 45, 60, 120, and 180 min. Accumulation with time in spleen and small bowel is clearly detectable. B = bladder; H = heart; LB = large bowel; Li = liver; Lu = lungs; S = spleen; SB = small bowel.
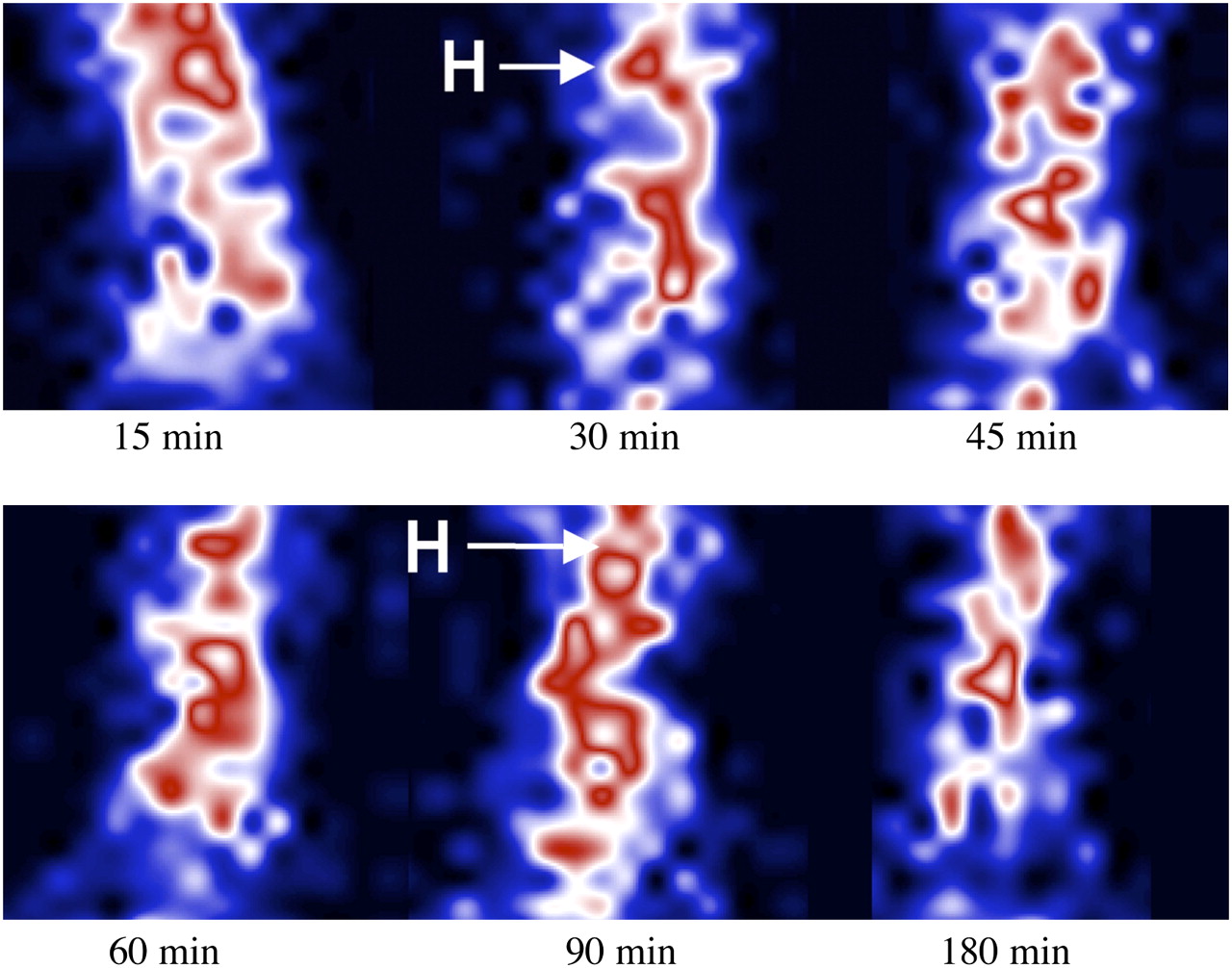
Scintigraphic images (dorsal view) of SCID mice injected simultaneously with 8 × 106 unlabeled hPBMCs and 300 ng of control mAb, part of which was 99mTc-labeled (0.37 MBq, 140 ng). Images were acquired after 15, 30, 45, 60, 120, and 180 min. Labeled antibody remains in blood for entire study time. H = heart.
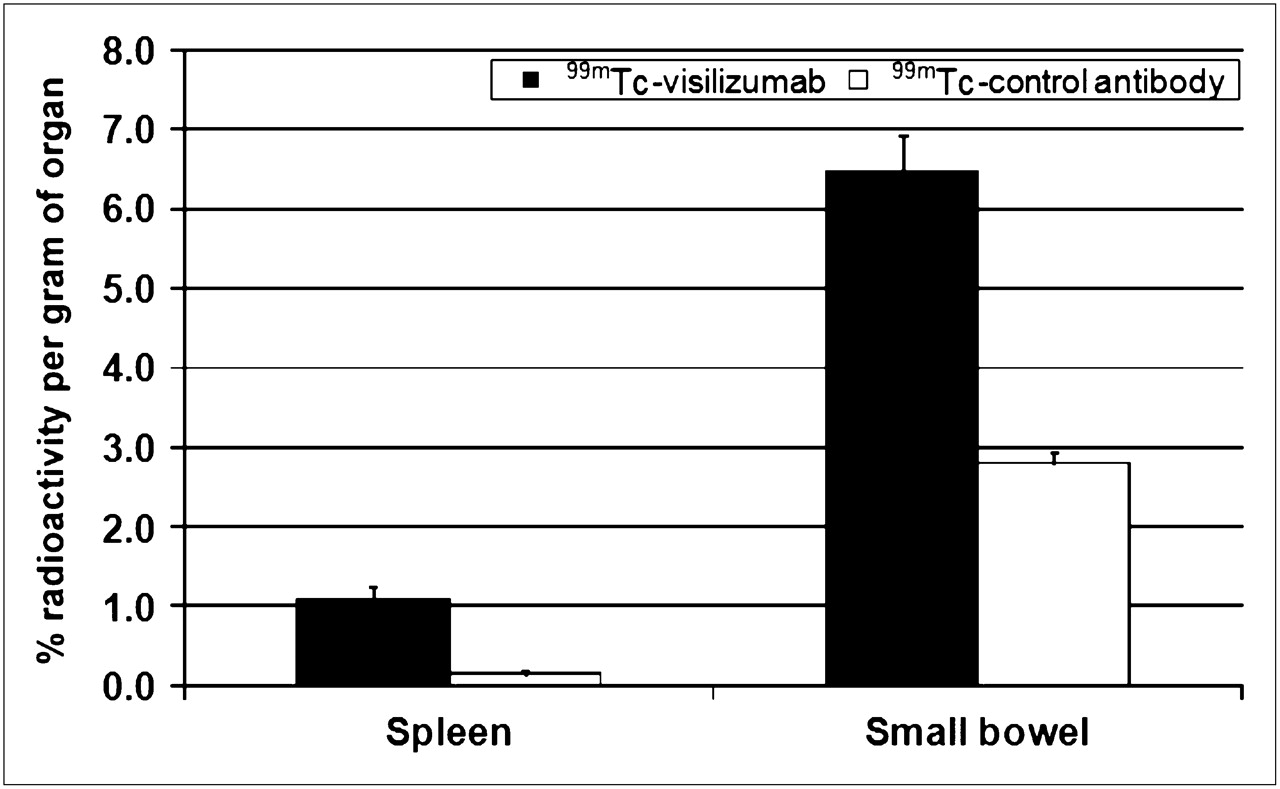
Radioactivity (% of injected dose/g) in spleen and small bowel of SCID mice previously irradiated and reconstituted with hPBMCs and injected with 99mTc-SHNH–visilizumab or 99mTc control mAb. Animals (mean of 3 ± SD) were killed 3 h after intravenous injection of labeled mAb.
Histology and Immunoperoxidase Staining of Mouse Organs
Histologic examination of organs from mice injected either with visilizumab or with control mAb performed by immunoperoxidase staining with antihuman CD3 antibody showed statistically significant differences in the presence of human lymphocytes between visilizumab and control mAb–injected mice for the spleen and small bowel (Table 1) but not for the liver, lungs and large bowel. Interestingly, lymph nodes and intestinal mucosa–associated lymphoid tissue (MALT) showed the same behavior as the spleen in mice injected with visilizumab (data not shown). This finding further supports the hypothesis that visilizumab induces lymphocyte migration from blood into primary and secondary lymphoid organs together with the appendix.
Number of Lymphocytes per Histologic Field in Different Tissues
DISCUSSION
Several attempts have been made in recent years to find specific and sensitive radiopharmaceuticals for imaging chronic T-cell–mediated inflammation. Human polyclonal immunoglobulin is a non–antigen-specific IgG antibody that is labeled with 99mTc. Several studies demonstrated that the 99mTc–human polyclonal immunoglobulin could be used not only for the assessment of disease activity but also as an effective prognostic tool for the inflammation-mediated disorders (19,20). But data in the literature showed that IgG also accumulates in the inflammatory foci by nonspecific extravasation facilitated by locally enhanced vascular permeability (21). Therefore, there is a need for more specific and sensitive radiopharmaceuticals for the diagnosis of inflammation, possibly targeting different molecules such as lymphocyte activation markers, soluble cytokines, endothelial activation markers, or other cell receptors. The information provided by these radiopharmaceuticals could be useful also for therapy decision making and evaluating response to specific therapies. These radiopharmaceuticals may include radiolabeled anti-TNFα, anti-CD25, anti-CD20, anti-CD3, anti-CD4, and anti-E-selectin antibodies. Recently, 2 anti-TNF-α monoclonal antibodies (infliximab and adalimumab) have been labeled with 99mTc, and different scintigraphic studies in Crohn's disease (22) and rheumatoid arthritis (RA) patients (23–25) showed their potential use for therapy decision making and follow-up. A B-cell transmembrane antigen (CD20)–specific IgG1κ mAb (rituximab) was also recently radiolabeled with 99mTc and found to be reliable in showing the disease activity in non-Hodgkin's lymphoma and RA patients (26,27). Experience has also been cumulated for anti-CD25 mAb radiolabeled with 131I, 99mTc, 18F, and 67Ga for imaging activated lymphocytes and monitoring response to anti-CD25 therapy (27,28). A mAb against E-selectin, an endothelium-specific cytokine-inducible adhesion molecule, was radiolabeled and successfully studied in patients with active RA. This radiolabeled mAb was found to be more reliable than other commercially available radiopharmaceuticals (29). In several scintigraphic studies, 99mTc-labeled CD4-specific antibody proved to image inflamed joints in RA patients, and this has been proposed to assess the disease activity (30,31). Moreover, an anti-CD3 murine IgG2α mAb, OKT3 (muromonab), was also labeled with 99mTc, and in different studies authors concluded that 99mTc-OKT3 imaging could be useful as a measurement of therapeutic effectiveness in acute renal transplant rejection and in RA (32,33). Unfortunately, OKT3 is of murine origin and showed side effects after administration in humans (34). Visilizumab, by contrast, is a humanized anti-CD3 monoclonal antibody, and if radiolabeled, visilizumab may provide a valuable diagnostic tool for imaging T-cell traffic and lymphocytic infiltration in tissues and organs affected by different autoimmune diseases. We therefore tried to label visilizumab with 99mTc. We tried both direct and indirect labeling procedures to develop a reliable and simple method that allows the formation of a stable 99mTc conjugate with no modification in its biologic activity. The labeling procedure described here is easy and rapid, and using tricine as a coligand we were able to stabilize the coordination of 99mTc to the SHNH–visilizumab conjugate and achieve a high LE (≥90%) and a high SA (10,360–11,100 MBq/mg) without the need of postlabeling purification. By contrast, the control mAb used in our experiments was labeled with a direct method using 2-ME reduction because we achieved a high LE of approximately 99% without the presence of colloids and therefore had no need of postlabeling purification. Both radiolabeled antibodies were stable in normal saline and serum up to 24 h.
Results of the targeting experiment in mice showed an in vivo accumulation of radiolabeled visilizumab to HUT78 cells with time, proportional to the number of implanted cells. In vivo competition (unlabeled vs. labeled mAb) was performed in mice using hPBMCs instead of HuT78 cells and proved in vivo the specificity of 99mTc-visilizumab binding to CD3. We also found a higher T/B ratio when using hPBMCs instead of the same number of HuT78 cells, and this is in line with the higher CD3 expression on cell surface of hPBMCs than HuT78.
Finally, using radiolabeled antibody and a model of SCID mice reconstituted with hPBMCs, we were able to demonstrate the effect of pharmacologic doses of visilizumab on resting circulating peripheral blood CD3-positive cells. Images acquired and single organ counting, supported by the histologic data, confirmed that visilizumab induces lymphocyte migration mainly into the small bowel and spleen. We also examined a few little lymph nodes and MALT tissue and found the same behavior as for the spleen, indicating that lymphocytes migrate from blood into primary and secondary lymphoid organs including the appendix. Therefore, the high liver uptake of visilizumab, compared with the control mAb, is not due to lymphocyte migration into this organ because not many lymphocytes were found at histologic examination and this phenomenon should be attributed to different antibody kinetics.
From the clinical point of view, our results show that 99mTc-SHNH–visilizumab can be used for diagnostic purposes, presumably without any side effects because of its high SA. Indeed, only 30 μg of radiolabeled visilizumab could be sufficient for a diagnostic scan in humans (i.e., with 370 MBq) as compared with approximately 700–1,000 μg (10–15 μg/kg) given for therapy. This radiopharmaceutical could also be useful for therapy decision making in patients who are candidates for anti-CD3 therapy by providing a rationale for such a therapy by showing CD3-positive lymphocytes infiltrating target organs.
In addition, we provided the explanation of a pathophysiologic finding observed in patients after the pharmacologic administration of visilizumab (i.e., the lymphopenia associated with migration of lymphocytes from blood to peripheral lymphoid organs). This explanation seems to rule out the hypothesis of lymphocyte migration to nonlymphoid organs, such as the liver and lungs, in which they are not used to home and in which they could induce tissue damage by activation and cytokine release.
In the future, we plan to use 99mTc-SHNH–visilizumab for imaging lymphocytic infiltration in patients affected by autoimmune diseases and for therapy decision making and therapy follow-up in patients treated with anti-CD3 mAb. Finally, because visilizumab has a short plasma half-life it could also be radiolabeled with positron emitters (such as 68Ga or 18F) that may provide a short-life radiopharmaceutical for specific targeting and sensitive detection of T-lymphocytes with PET cameras.
CONCLUSION
Visilizumab can be efficiently labeled with 99mTc with high LE and can be used for imaging T-cell traffic and lymphocytic infiltration in tissues and organs. The defined method is simple, rapid, reliable, and effective, yielding a high SA without the loss of immune reactivity and with excellent cell targeting in vivo. In particular, we were able to demonstrate that 99mTc-SHNH–visilizumab targets CD3-positive cells in different mouse models, and a pharmacologic dose of unlabeled visilizumab induces migration of hPBMCs from circulation into small bowel and peripheral lymphoid organs (spleen, lymph nodes, and MALT tissue in small bowel). This migration can be visualized with 99mTc-SHNH–visilizumab imaging.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication October 21, 2008.
- Accepted for publication June 30, 2009.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}