


Abstract
Tumor uptake of copper(II)-diacetyl-bis(N4-methylthiosemicarbazone) (copper-ATSM), a hypoxia-targeting radiopharmaceutical, assessed by PET has been found to correlate with prognosis in several human cancers. Wide clinical utility of this tracer will require its labeling with a copper radionuclide having a longer half-life than the 60Cu used in studies to date. The purpose of this work was to obtain the requisite preclinical data for copper-ATSM to file an investigational new drug application, followed by a crossover comparison of PET image quality and tumor uptake with 60Cu-ATSM and 64Cu-ATSM in women with cancer of the uterine cervix. Methods: The preclinical toxicology and pharmacology of a copper-ATSM formulation was examined using standard in vitro and in vivo assays, as well as 14-d toxicity studies in both rats and rabbits. For the clinical test–retest imaging study, 10 patients with cervical carcinoma underwent PET on separate days with 60Cu-ATSM and 64Cu-ATSM. Image quality was assessed qualitatively, and the tumor-to-muscle activity ratio was measured for each tracer. Results: The toxicology and pharmacology data demonstrated that the formulation has an appropriate margin of safety for clinical use. In the patient study, we found that the image quality with 64Cu-ATSM was better than that with 60Cu-ATSM because of lower noise. In addition, we found that the pattern and magnitude of tumor uptake of 60Cu-ATSM and 64Cu-ATSM on studies separated by 1–9 d were similar. Conclusion: 64Cu-ATSM appears to be a safe radiopharmaceutical that can be used to obtain high-quality images of tumor hypoxia in human cancers.
Tumor uptake of copper(II)-diacetyl-bis(N4-methylthiosemicarbazone) (copper-ATSM) (1,2), a hypoxia-targeting radiopharmaceutical, as assessed by PET, has been confirmed as a clinically important biomarker of prognosis in several human cancers. Copper-ATSM PET has been shown to distinguish patients likely and unlikely to respond to conventional therapies for cancers of the lung (3), uterine cervix (4,5), rectum (6), and head and neck (Chao, unpublished data, 2002).
Most clinical copper-ATSM studies have used the agent labeled with the short-lived positron-emitting radionuclide of copper (7), 60Cu (half-life, 0.395 h; β+-decay, 92.5%; electron capture, 7.5%) (3–6,8). To enable copper-ATSM to be translated for use in PET centers that do not have an in-house cyclotron, copper-ATSM labeled with one of the longer-lived positron-emitting nuclides, 64Cu (half-life, 12.7 h; β+-decay, 17.4%; β−-decay, 38.5%; electron capture, 43%) or 61Cu (half-life, 3.33 h; β+-decay, 62%; electron capture, 38%) (7), is required. The longer half-lives of 64Cu and 61Cu allow for production at a regional center and distribution to PET facilities in a fashion similar to that for 18F-labeled radiopharmaceuticals. The preparation of 62Cu (half-life, 0.16 h; β+-decay, 98%; electron capture, 2%), via a 62Zn/62Cu generator system, has been reported and commercialized (9) and offers an additional method for radiolabeling copper-ATSM for use in humans.
The initial clinical studies of 60Cu-ATSM (3–6,8) in cancers were undertaken at Washington University School of Medicine under the auspices of the Radioactive Drug Research Committee and in accordance with 21 Code of Federal Regulations 361.1 to obtain basic information on the metabolism (including kinetics, distribution, dosimetry, and localization) of copper-ATSM. These preliminary observations encouraged us to pursue confirmation of our findings in a larger, multicenter clinical trial. For such a trial to be undertaken within the United States, it was necessary to apply to the U.S. Food and Drug Administration (FDA) for investigational use of 64Cu-ATSM, thus allowing for production and shipping of the longer-lived radiopharmaceutical to imaging centers. This article describes the first clinical study undertaken after filing of the investigational new drug (IND) application that compares the image quality of 60Cu-ATSM and 64Cu-ATSM (test–retest) in a cohort of 10 women with cervical carcinoma.
MATERIALS AND METHODS
General
All chemicals, unless otherwise stated, were purchased from Sigma-Aldrich Chemical Co., Inc. All solutions were prepared using distilled, deionized water (>18 MΩ resistivity) by passing through a Milli-Q filtration system (Millipore Corp.).
Toxicology Formulation (Copper-ATSM/H2ATSM)
Guidance from the FDA was obtained in pre-IND discussions regarding the formulation of the agent to be tested. The selected formulation represented a worst-case scenario, based on the final composition of 64Cu-ATSM at the time of injection into humans. The formulation consisted of the following components: 2.1556 g of H2ATSM (69.73%), 153.9 mg of nonradioactive copper-ATSM (4.98%), 12.0 mg of CoCl2 (0.38%), and 0.77 g of NiCl2 (24.91%). These 4 solid materials were ground and mixed to produce a homogeneous mixture. The solid formulation was then dissolved in dimethylsulfoxide (1%), ethanol (5%), and saline (94%) before use in the preclinical toxicology studies.
Toxicology and Pharmacology Studies
The preclinical toxicology and pharmacology of a copper-ATSM formulation was examined using standard in vitro and in vivo assays, as well as 14-d toxicity studies in both rats and rabbits. All toxicology and pharmacology studies were conducted in compliance with good laboratory practice regulations (21 Code of Federal Regulations, part 58). Mutagenicity was determined with the in vitro Salmonella reverse-mutation plate-incorporation assay, the in vitro L5178Y/TK+/− mouse lymphoma mutation assay, and the in vivo micronucleus assay in rats. Safety pharmacology studies were performed by cardiovascular and pulmonary safety testing on beagle dogs and neurologic safety assessment on rats. A 14-d toxicity study of the toxicology formulation in rats and rabbits was also performed. The full experimental details, protocols, and results of these evaluations can be accessed at http://imaging.cancer.gov/programsandresources/specializedinitiatives/dcide/page13.
Radiopharmaceutical Synthesis
60Cu and 64Cu were produced in the CS15 cyclotron (Cyclotron Corp.) at the Washington University Medical Center, as previously described (10,11). 60Cu-ATSM and 64Cu-ATSM were produced on the basis of methods previously described (3,5). The methods for production are identical for both compounds. The final sterile, apyrogenic, and isotonic 60Cu-ATSM or 64Cu-ATSM solution had greater than 98% radiochemical purity at the time of injection.
PET Phantom Analysis
The PET image-quality accreditation phantom (12) of the American College of Radiology was used to compare the quantitative accuracy of 64Cu and 60Cu imaging in the ECAT HR+ scanner (Siemens-CTI). The performance specifications of this scanner have been previously reported (13). The scanner has a spatial resolution of 4.5 mm in full width at half maximum for imaging with short-range positron emitters such as 18F or 64Cu. The phantom is composed of a cylinder 20 cm in diameter and 20 cm long, with fillable cylinders attached to the top lid. The diameter of these cylinders is 8, 12, 16, and 25 mm, and their length is 25 mm. The phantom was prepared with a 9.87:1 activity ratio between the cylinders and the surrounding background area. The lower part of the phantom, which contains a pattern of cold rods of various diameters in a pielike configuration, was not analyzed in this work. Peak and average activity concentrations in the cylinders were compared with the average activity in the uniform area to calculate ratios to mimic the tumor-to-muscle ratios from the patient data analysis. The 64Cu experiment was done by preparing 13.0 MBq (0.352 mCi) of 64Cu diluted in 600 mL. This solution was then used to fill the cylinders. The rest of the solution was placed in the uniform area of the phantom, and water was added to completely fill the phantom for a total volume of 5.92 L. For the 60Cu experiment, the initial activity was 72.15 MBq (1.95 mCi). These values correspond to an injected patient activity of 185 MBq (5 mCi) and 925 MBq (25 mCi), respectively, assuming a typical patient weight of 70 kg. The phantoms were then scanned for 1 h, with the same acquisition protocol as for patients (2-dimensional [2D] for 60Cu and 3-dimensional [3D] for 64Cu), and the images were reconstructed using the same algorithm (ordered-subsets expectation maximization, 2D, 2 iterations/32 subsets, with a Hann filter at 0.3 cm−1 followed by a 3D gaussian filter of 7.5 mm). Regions of interest were drawn on the hot cylinders at 50%, 50%, 40%, and 25% of the maximum inside the 25-, 16-, 12-, and 8-mm cylinders, respectively. The attenuation correction was measured by a 10-min transmission scan using the three 68Ge rotating rod sources of the camera followed by the manufacturer's segmentation algorithm.
Treatment of Cascade Coincidences in 60Cu Imaging
Given that 60Cu decays by positron decay with the concurrent emission of numerous cascade γ-photons, the fortuitous cascade coincidences were removed by convolution of the cascade γ-ray kernel as previously reported (14,15) and validated for 86Y and 76Br imaging in clinical cameras. Using this technique, the fully corrected projection data (corrected for normalization, attenuation, and scatter) were further corrected by subtraction of the cascade background, and the images were then reconstructed from those corrected data with the same reconstruction algorithm. All imaging with 60Cu was performed in 2D mode because the collimator septa minimize contamination by cascade coincidences.
Human PET
The comparison study was performed under the auspices of IND 62,675. To test the safety of 60Cu-ATSM and 64Cu-ATSM, we monitored the vital signs of the participants and the results of their various laboratory tests, including a standard complete blood cell count, a comprehensive metabolic panel, and urinalysis, within 4 h before and 1 h to 7 d after radiopharmaceutical injection. All examinations were monitored for clinically significant changes that may have been related to copper-ATSM administration. A change in heart rate of more than 20 beats/min or in systolic or diastolic blood pressure of more than 20 mm Hg was considered to be significant. A change in hemoglobin of more than 2 g/dL, in serum glutamate pyruvate transaminase of more than 150 IU/L, in total bilirubin of more than 0.5 mg/dL, or in serum creatinine of more than 0.75 mg/dL was also considered to be significant. This investigation was approved by the Human Research Protection Office and the Radioactive Drug Research Committee of Washington University School of Medicine and by the Protocol Review and Monitoring Committee of the Siteman Cancer Center. Ten women with newly diagnosed squamous cell carcinoma of the uterine cervix underwent PET with both 60Cu-ATSM and 64Cu-ATSM before beginning conventional treatment by chemoradiotherapy. All patients had locally advanced cervical cancer with primary lesions more than 2.0 cm in diameter. The women ranged in age from 33 to 79 y; their clinical FIGO (International Federation of Gynecology and Obstetrics) stages were IB1 in 1, 1B2 in 1, IIB in 3, IIIA in 1, and IIIB in 4. The tumor histology was squamous cell carcinoma in all patients. All patients gave written informed consent before participating in the study. All patients underwent clinically requested PET/CT with 18F FDG, as previously described (16). PET with 60Cu-ATSM and 64Cu-ATSM was performed with an ECAT HR+ scanner. Imaging with 60Cu-ATSM and 64Cu-ATSM was performed on separate days in a randomized order (4 patients underwent 60Cu-ATSM PET first and 6 patients underwent 64Cu-ATSM PET first). The time difference between the 2 scans averaged 5.8 d (range, 1–9 d). If 60Cu-ATSM was injected first, 64Cu-ATSM was injected at least 24 h (mean, 3.5 d; range, 1–7 d) after 60Cu-ATSM injection. If 64Cu-ATSM was injected first, 60Cu-ATSM was injected at least 6 d, that is, at least 11 half-lives of 64Cu (mean, 7.3 d; range, 6–9 d), after 64Cu-ATSM injection. For optimization of image quality, all 10 patients were to receive approximately 925 MBq (25 mCi) of 64Cu-ATSM and 740 MBq (20 mCi) of 60Cu-ATSM. These dosages of 60Cu-ATSM and 64Cu-ATSM were chosen to acquire the same number of decays in the 30- to 60-min-postinjection scan. A 925-MBq (25-mCi) dose of 64Cu-ATSM results in a 361 mGy dose to the liver and an effective dose of 33.3 mSv; the corresponding doses from a 740-MBq dose of 60Cu-ATSM are 47.4 mGy and 8.14 mSv, respectively (17). The imaging procedure and image processing were the same for both 60Cu-ATSM PET and 64Cu-ATSM PET except with regard to imaging mode and the treatment of the cascade γ-ray emission. The 64Cu-ATSM PET images were acquired in the 3D mode (with septa retracted) to maximize sensitivity. As for the phantom studies, all imaging with 60Cu was performed in the 2D mode, because the collimator septa minimize contamination by cascade coincidences. Where the injected activity of 60Cu-ATSM was less than the planned 740 MBq (20 mCi), the duration of image acquisition with 64Cu-ATSM was adjusted so that the images with both radionuclides had similar count statistics. Because the data from 30 to 60 min were acquired as six 5-min frames, the summed image was created from the approximate number of 5-min frames to achieve matching image statistics.
Image Analysis
Clinical 18F-FDG PET/CT images were evaluated qualitatively with image interpretation criteria routinely used in scintigraphic imaging. For qualitative analysis, the 60Cu-ATSM PET and 64Cu-ATSM PET images were evaluated subjectively by an experienced nuclear medicine physician who was not aware of which copper-ATSM scan was being interpreted. Then, the images were evaluated in correlation with the CT and 18F-FDG PET/CT images. In addition, the overall tumor uptake of 60Cu-ATSM and 64Cu-ATSM was assessed semiquantitatively by determining the tumor-to-muscle activity (T/M) ratio based on the 30- to 60-min summed images, as previously described (3–6,8). For the 60Cu-ATSM images, the patient data were processed by the cascade subtraction technique.
Statistical Analysis
The tumor uptake of 60Cu-ATSM was correlated with that of 64Cu-ATSM to determine whether there was a relationship between the uptakes of these 2 radiotracers. P values less than 0.05 were considered statistically significant.
RESULTS
Phantom Data
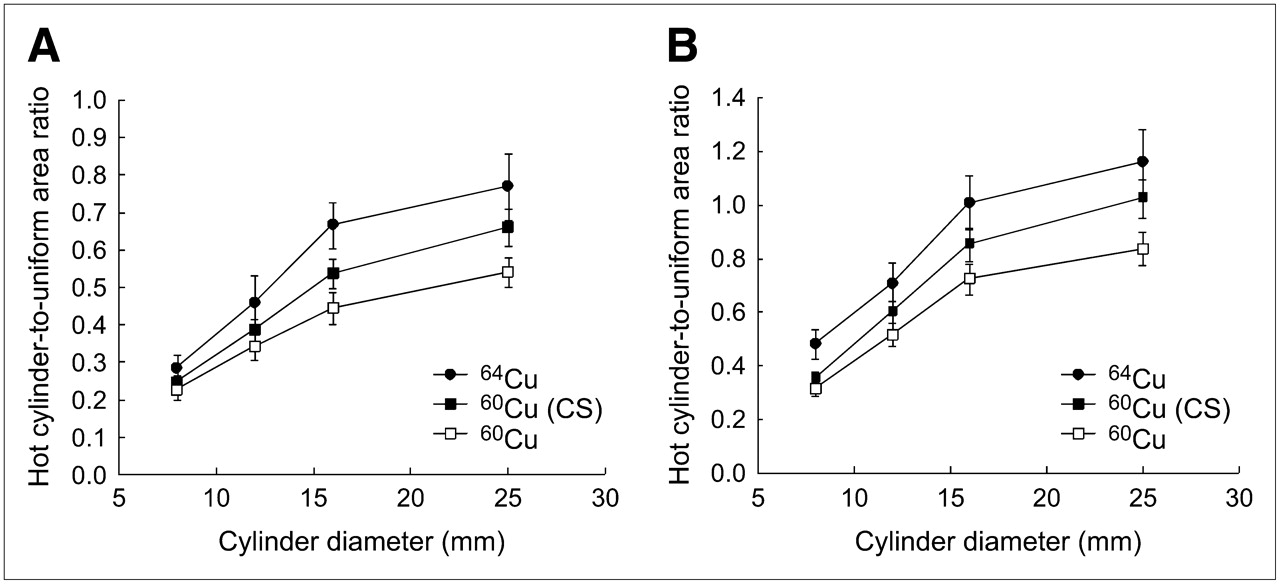
The cylinder–to–uniform-area ratios are presented in Figure 1A for the peak values within the cylinder and in Figure 1B for the average values for 64Cu and 60Cu (with and without cascade subtraction). This phantom analysis indicates that similar cylinder-to-background ratios are observed for both radionuclides when cascade subtraction is used. The positron range of 60Cu is likely responsible for the reduced recovery coefficients observed for this nuclide.

Activity ratios of hot cylinders to background, with cylinders of 8-, 12-, 16-, and 25-mm diameter for 64Cu and 60Cu (without and with cascade coincidence subtraction [CS]). Ratios of hot cylinder to uniform area in A are averages within cylinder and in B are peak values. Values were normalized to expected ratio of 9.87 to be equal to 1.
Patient Studies
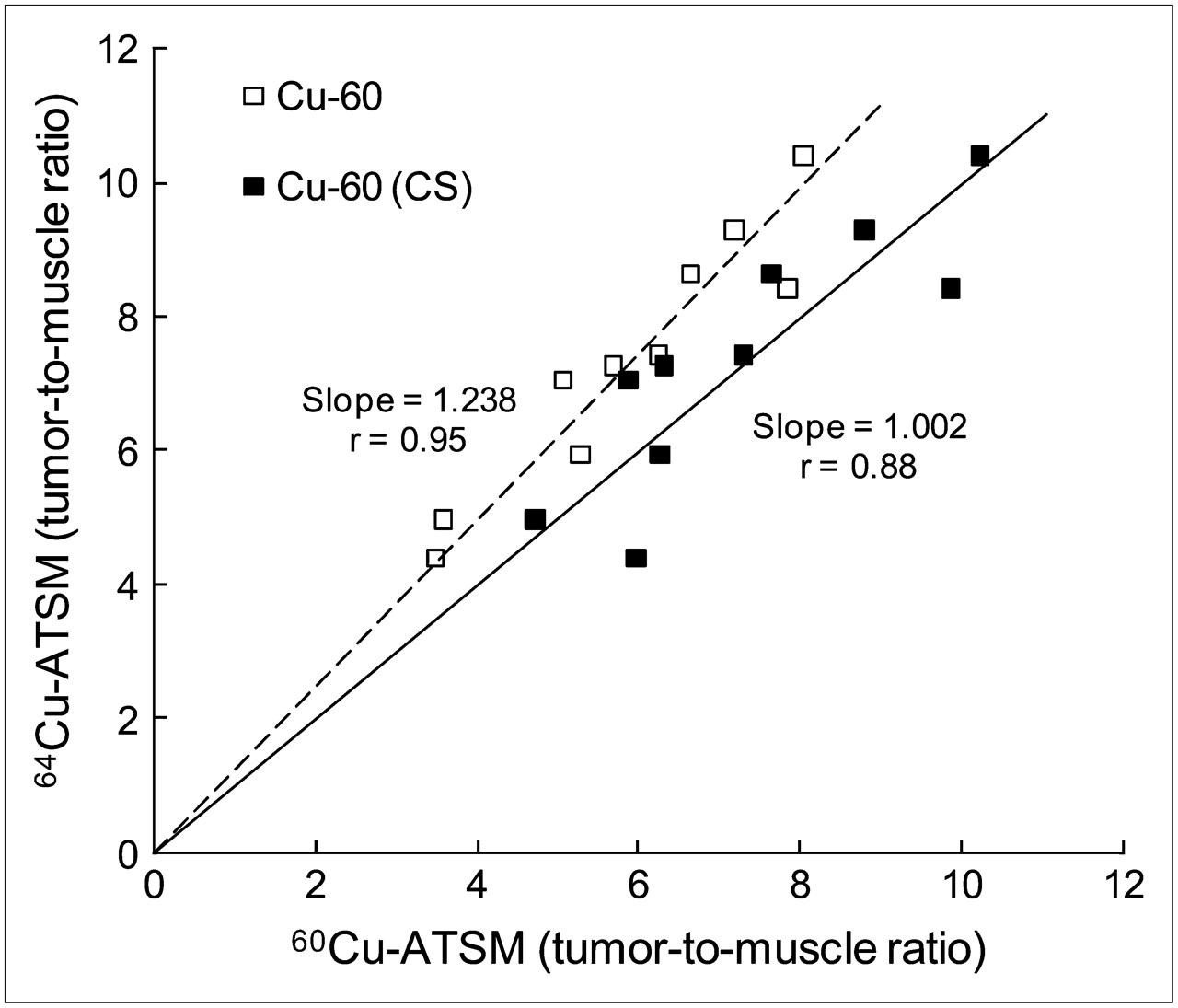
There were no clinically significant changes in vital signs or laboratory test results after injection of 60Cu-ATSM and 64Cu-ATSM. No adverse events or clinically detectable pharmacologic effects related to either 60Cu-ATSM or 64Cu-ATSM were observed. The comparison study demonstrated increased 60Cu-ATSM and 64Cu-ATSM uptake in the tumors of all 10 patients (T/M ratios of 5.9 ± 1.6 and 7.3 ± 1.9, respectively) (Table 1). The 10 patients received a mean of 903 MBq (24.3 mCi) (range, 821–952 MBq) of 64Cu-ATSM and a mean of 478 MBq (12.9 mCi) (range, 204–740 MBq of 60Cu-ATSM (Table 1). A significant correlation was observed between the uptakes of 60Cu-ATSM and 64Cu-ATSM (r = 0.95, P < 0.0001) (Fig. 2). The image quality was comparable; although generally, the images with 64Cu-ATSM had a slightly better target-to-background ratio and tumors were delineated more clearly than on the 60Cu-ATSM images (Figs. 3A and 3B). Importantly, the pattern of uptake was similar on the images obtained with the tracers during 2 different imaging sessions 1–9 d apart, indicating that the macroscopic distribution of hypoxia did not change greatly over this interval.
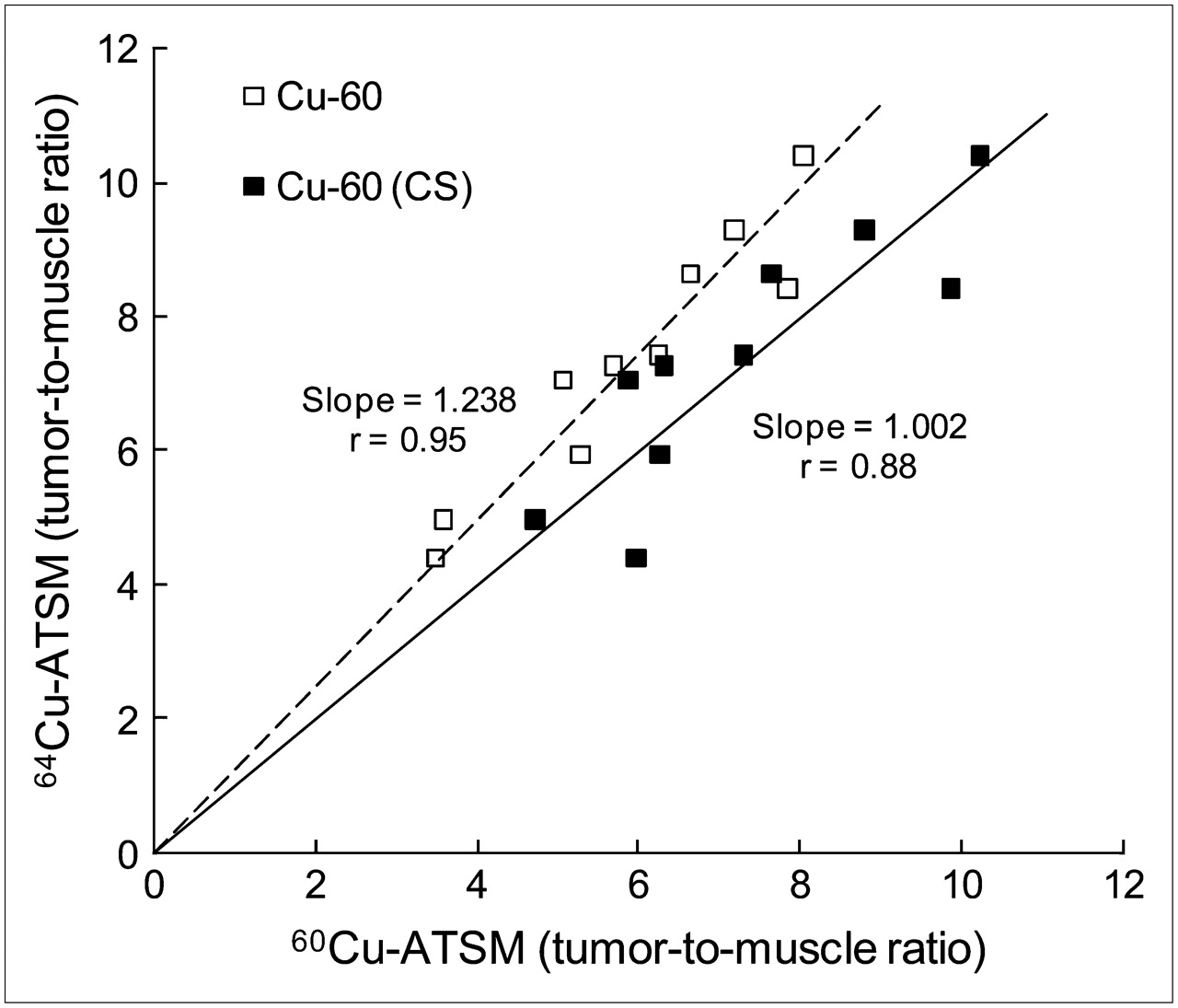
Correlation of 60Cu-ATSM uptake (without and with cascade subtraction [CS]) and 64Cu-ATSM uptake in 10 patients with cervical cancer. Results are expressed as T/M ratios. Good correlation between uptakes of these 2 radiotracers was found. This analysis was performed to demonstrate that similar T/M ratios can be obtained with both nuclides and that applying 60Cu cascade coincidence correction improves comparability of measured T/M ratios. Linear regressions were determined by setting y-intercept to zero and slope derived from least-square minimization.
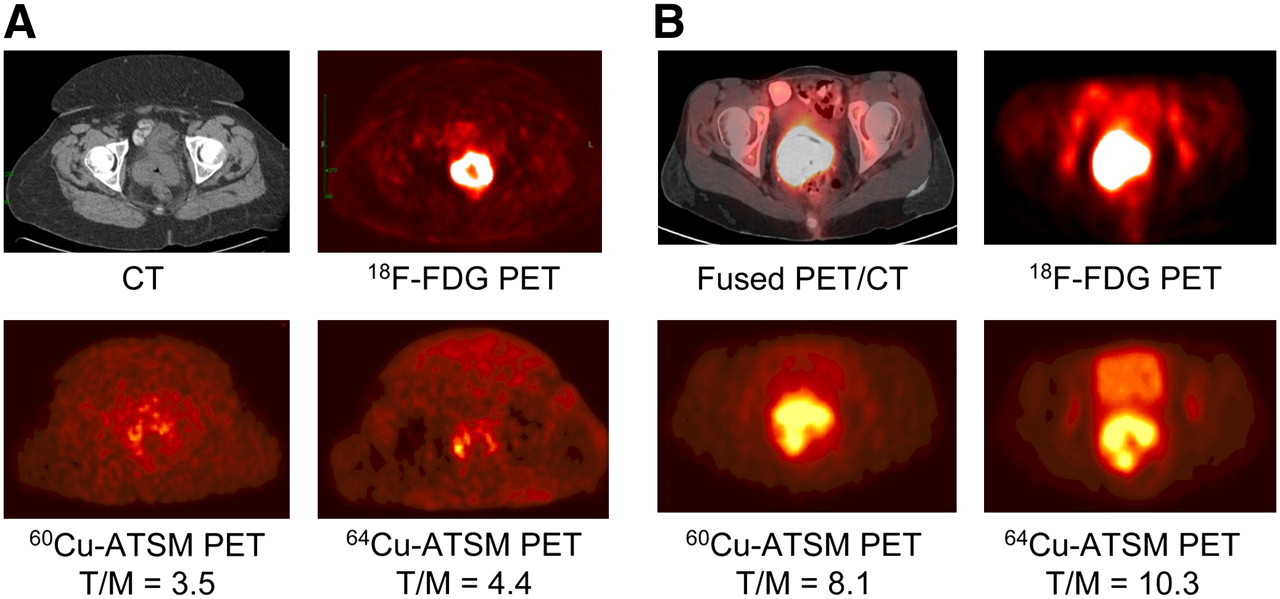
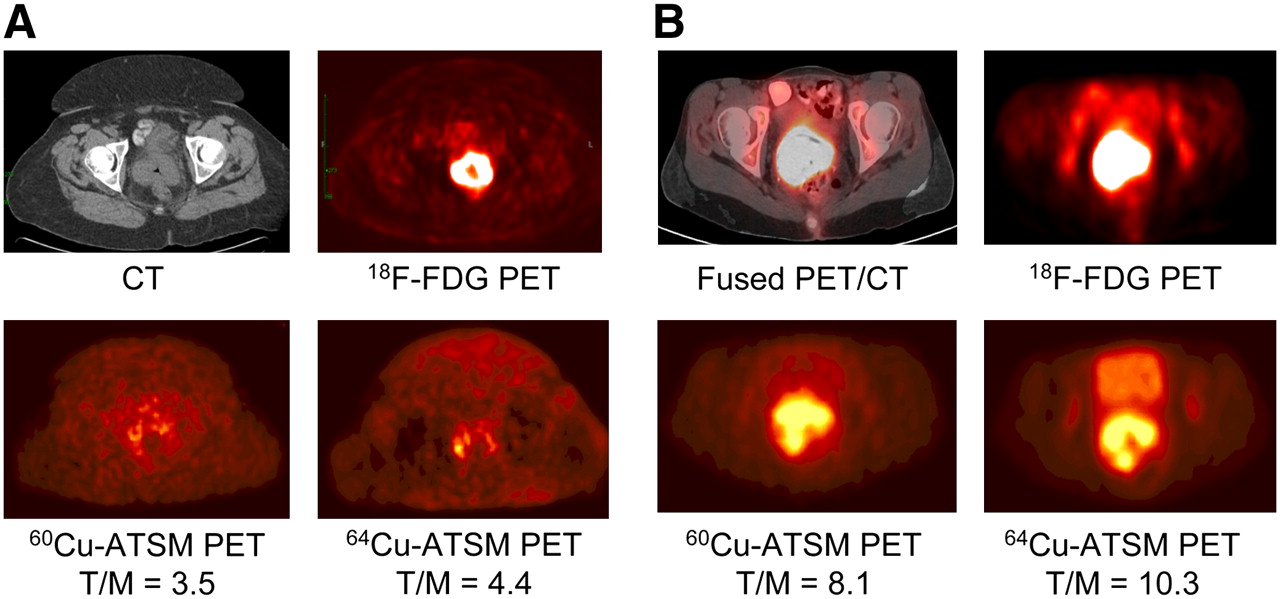
(A) Transaxial CT (top left) and 18F-FDG PET (top right) images of pelvis show intense 18F-FDG uptake within known cervical tumor at site of cervical mass seen on CT. Transaxial 30- to 60-min summed images of 60Cu-ATSM PET (bottom left) and 64Cu-ATSM PET (bottom right) of pelvis at same level demonstrate mildly increased uptake within known primary cervical tumor. There are similar patterns of 60Cu-ATSM and 64Cu-ATSM uptake within tumor. (B) Transaxial coregistered 18F-FDG PET/CT (top left) and 18F-FDG PET (top right) images of pelvis show intense 18F-FDG uptake within known cervical tumor at site of cervical mass seen on CT. Transaxial 30- to 60-min summed images of 60Cu-ATSM PET (bottom left) and 64Cu-ATSM PET (bottom right) of pelvis at same level demonstrate markedly increased uptake within known primary cervical tumor. There are similar patterns of 60Cu-ATSM and 64Cu-ATSM uptake within tumor.
Summary of Patient Demographics and Imaging Comparison Results
In addition, the patient data were quantitatively analyzed and T/M ratios were measured on the images obtained with 64Cu-ATSM, 60Cu-ATSM, and 60Cu-ATSM processed with cascade subtraction (Fig. 2; Table 1). This analysis demonstrated that similar T/M ratios are obtained with both radionuclides and that application of the cascade subtraction correction improves the correlation between the 64Cu-ATSM and the 60Cu-ATSM measurements. The T/M ratio for 60Cu-ATSM processed with cascade subtraction was 7.3 ± 1.8, closely similar to that reported for 64Cu-ATSM. The slope of the regression line was 1.002 with the corrected 60Cu-ATSM values, versus 1.238 without the cascade subtraction correction. The corresponding correlation coefficients were 0.88 and 0.95, respectively.
DISCUSSION
Hypoxia is an important feature of solid tumors affecting tumor aggressiveness and response to therapy. Tumor hypoxia has been shown to be an adverse prognostic factor independent of standard prognostic factors such as tumor stage (18). In cervical cancer, direct assessment of tumor oxygenation by oxygen electrodes has demonstrated that patients with hypoxic tumors have worse disease-free survival than patients with nonhypoxic tumors (19). Although the oxygen electrode method is considered the gold standard for direct measurement of hypoxia, it is invasive, applicable only to accessible tumors, and technically difficult to perform, thus limiting its clinical use. Accordingly, noninvasive imaging methods such as PET have been studied as alternatives. We recently showed that the results of 60Cu-ATSM PET predict prognosis in patients with locally advanced cervical cancer and rectal cancer (4,6). This method offers clinically relevant information that may have future applicability to directing hypoxia-targeted therapy.
Among the several radionuclides of copper, 64Cu is the most commonly used for basic science investigations and clinical PET, and its production and use have now been reported in the United States, Europe, and Japan (20). With a half-life of 12.7 h, 64Cu is ideally suited for PET studies that require a longer-lived nuclide: distribution of 64Cu radiopharmaceuticals to facilities other than the production site is possible, and imaging can be conducted as long as 48 h after tracer administration. Moreover, because 64Cu has a maximum positron energy of 0.66 MeV, similar to that of 18F, the resulting PET images are of high quality and are the best obtainable with any of the positron-emitting radionuclides of copper. The 38.5% β− emission of 64Cu opens the possibility of therapeutic applications with this nuclide but adds a radiation burden to the patient when the nuclide is used for imaging purposes (7,21). This current work was undertaken to translate use of 64Cu-ATSM to humans, in order to allow for the production and supply of the radiopharmaceutical to multiple PET facilities. This process required a series of toxicology and pharmacology studies necessary to file an IND application with the FDA. These data demonstrated that the formulation has an appropriate margin of safety for clinical use. Thereafter, a small, crossover bioequivalence study was performed to compare the quality of clinical PET images and the quantitative reproducibility of measured tumor uptake of copper-ATSM with 60Cu and 64Cu labeling.
After completion of the preclinical safety studies and submission of an IND application to the FDA, we studied patients with cervical cancer to assess whether the images obtained with 64Cu-ATSM are of similar quality to those obtained with 60Cu-ATSM. 60Cu decays by positron emission, with the concurrent emission of numerous γ-photons in cascade (most notably 826 keV, 21.7%; 1,333 keV, 88%; and 1,792 keV, 45.4%), originating from the β-decay to excited states in the 60Ni daughter nuclide. These additional γ-photons can downscatter into the acceptance energy window of the scanner and, as such, are not effectively suppressed. They will form fortuitous coincidences with incorrect positional information, thus increasing background activity and impairing image quality and quantitative accuracy. Those coincidences are typically not corrected adequately by the manufacturer-provided random or scatter corrections. Several techniques have been described for correction of cascade coincidences (15,22,23), but we used a convolution of the cascade γ-ray kernel, as previously reported (14). This technique was validated for 86Y and 76Br in a clinical tomograph operated in the 2D mode. In this technique, fully corrected projection data (corrected for normalization, attenuation, and scatter) are further corrected for cascade coincidence subtraction, and the images are then reconstructed from those corrected data. After cascade subtraction, the hot-cylinder–to–background ratio for 60Cu became closer, but not equal, to that of 64Cu. This result is expected because of the longer positron range of 60Cu. Similar observations have been seen in other studies, where higher sphere-to-background ratios were observed after a uniform background subtraction was used (24,25). We chose here to use the deconvolution approach because it approximately accounts for the attenuation of the cascade γ-rays (14).
In our patient studies, we found that the image quality with 64Cu-ATSM was better than that with 60Cu-ATSM, but in most subjects fewer positron decays occurred during the 30- to 60-min 60Cu-ATSM scan than during the corresponding 64Cu-ATSM collection. In addition, the increased sensitivity (∼ by a factor of 2) of the 3D acquisition mode improved the statistics in the 64Cu images, resulting in improved image quality. The cascade subtraction technique does increase the image noise, especially in scans of low image statistics (because of short scan duration or low administered activity), but because of the relatively high statistics in our 60Cu patient images, this increase in noise was not a major problem. We found that the pattern and magnitude of tumor uptake of 60Cu-ATSM and 64Cu-ATSM on studies separated by 1–9 d were similar (Figs. 3A and 3B). Thus, tumor uptake of copper-ATSM appears to be reproducible regardless of the radionuclide used for imaging. It also appears that 60Cu-ATSM and 64Cu-ATSM measure a property of the tumor that is stable over time, likely related to chronic hypoxia as opposed to acute hypoxia (26). This finding is of importance given that the treatment of tumor hypoxia typically targets the chronic form of hypoxia.
The initial estimates of the injected activity for 64Cu-ATSM were based on previous imaging experience with 60Cu and on theoretic considerations regarding the relative half-live, positron decay branching ratio, and greater sensitivity in 3D mode relative to the 2D data acquisition mode of the PET scanner (17). The image quality obtained with an injected dose of 925 MBq (25 mCi) of 64Cu-ATSM was excellent.
CONCLUSION
The technology for production and widespread delivery of 64Cu is in place and commercialized. Several companies, including MDS Nordion (Canada), ACOM (Italy), Trace Life Sciences (United States), IBA Molecular (United States and Europe), and IsoTrace (United States) are supplying 64Cu for use in preparation of radiopharmaceuticals such as 64Cu-ATSM (20). Copper-ATSM has several well-known advantages over other radiopharmaceuticals used for PET of hypoxia (1,2), including a simpler method for synthesis, a faster clearance rate from normoxic tissue allowing a short time between injection and imaging, and a simpler method for quantification. All these qualities of 64Cu-ATSM make it an attractive tracer for clinical imaging of tumor hypoxia. This method can be used to identify patients for clinical trials of treatment strategies designed to overcome hypoxia.
Acknowledgments
We greatly appreciate the technical support by Linda Becker, Jennifer Frye, and Helen Kaemmerer. We also acknowledge Tom F. Voller, Lucie Tang, Todd A. Perkins, Dr. Rajendra Singh, Sally W. Schwarz, and the cyclotron staff at Washington University School of Medicine for their valuable assistance in the production of 60Cu and 64Cu. We also thank Dr. Brad Beattie (Memorial Sloan-Kettering) for sharing part of his program for the cascade subtraction. Toxicology and pharmacology studies were supported by the Development of Clinical Imaging Drugs & Enhancers (DCIDE) program of the Division of Cancer Treatment and Diagnosis (http://imaging.cancer.gov/programsandresources/specializedinitiatives/dcide) of the National Cancer Institute. This work was supported by NIH grant CA81525 and DOE grant DE-FG02-87ER60512.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication February 1, 2008.
- Accepted for publication April 7, 2008.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Use of Novel PET Tracers to Image Breast Cancer Biologic Processes Such as Proliferation, DNA Damage and Repair, and Angiogenesis
- Cardiac Hypoxia Imaging: Second-Generation Analogues of 64Cu-ATSM
- A Comparison of the Imaging Characteristics and Microregional Distribution of 4 Hypoxia PET Tracers
- Interrogating Tumor Metabolism and Tumor Microenvironments Using Molecular Positron Emission Tomography Imaging. Theranostic Approaches to Improve Therapeutics
- VPAC1 Receptors for Imaging Breast Cancer: A Feasibility Study
- Application of 62Cu-Diacetyl-Bis (N4-Methylthiosemicarbazone) PET Imaging to Predict Highly Malignant Tumor Grades and Hypoxia-Inducible Factor-1{alpha} Expression in Patients with Glioma
- Understanding the hypoxic niche of multiple myeloma: therapeutic implications and contributions of mouse models
- Diacetylbis(N(4)-methylthiosemicarbazonato) Copper(II) (CuII(atsm)) Protects against Peroxynitrite-induced Nitrosative Damage and Prolongs Survival in Amyotrophic Lateral Sclerosis Mouse Model
- Molecular Imaging of Hypoxia
- Radiopharmaceuticals in Preclinical and Clinical Development for Monitoring of Therapy with PET