


Abstract
The imaging of neuroendocrine tumors has become one of the most significant areas in nuclear oncology. In an attempt to provide high-quality imaging and possible sensitivity at a reduced cost, time, and radiation dose, several 99mTc agents have been proposed. The aim of this initial study was to compare the tumor uptake and biodistribution of 2 new 6-hydrazinopyridine-3-carboxylic acid (HYNIC)–derivatized Tyr3-octreotide analogs, 99mTc-[HYNIC,Tyr3]octreotide (99mTc-TOC) and 99mTc-[HYNIC,Tyr3,Thr8]octreotide (99mTc-TATE), in patients with somatostatin receptor–expressing tumors. Methods: Each of 12 patients with proven gastrointestinal pancreatic neuroendocrine tumors received a mean activity of 520 MBq of 99mTc-TOC and 99mTc-TATE. Scintigraphy with both tracers was performed 3–4 h after their injection using standard whole-body and SPECT imaging. The images were reviewed subjectively by 2 readers, who reported tumor uptake lesion by lesion. Results: Both radiotracers demonstrated concordance between the results in 7 patients (58%). In total, 110 sites of disease were identified with 99mTc-TOC, compared with 115 with 99mTc-TATE. There was 1 case in which 99mTc-TOC identified sites of disease not seen on 99mTc-TATE imaging but 4 cases in which some sites of disease were seen with 99mTc-TATE and not 99mTc-TOC. Conclusion: In this initial study, both tracers seem to show similar sites of tumor, with 99mTc-TATE having a slight edge in the total number of lesions seen, especially in lymph node metastases.
Gastrointestinal pancreatic (GEP) neuroendocrine tumors (NETs) represent 70% of all NETs. Most of this group of tumors have metastatic spread at diagnosis, and most express somatostatin receptors (SSRs), usually with high density (1). SSR scintigraphy has normally been performed with the somatostatin analog 111In-pentetreotide (OctreoScan; Mallinckrodt Medical) and is accepted for determining the presence of SSR type 2 and SSR type 5 in NETs (2). One of the major drawbacks of 111In-pentetreotide is its high cost, and the isotope has physical characteristics resulting in suboptimal image resolution and the need for medium-energy collimators that reduce the counting rate. These drawbacks have led to a search for more suitable radioligands based on 99mTc for detecting SSRs. Among the newer agents studied so far are two 6-hydrazinopyridine-3-carboxylic acid (HYNIC)–derivatized Tyr3-octreotide analogs, 99mTc-[HYNIC,Tyr3]octreotide (99mTc-HYNIC-TOC, or 99mTc-TOC) and 99mTc-[HYNIC,Tyr3,Thr8]octreotide (99mTc-HYNIC-TATE, or 99mTc-TATE), labeled with tricine and ethylenediamine N,N′-diacetic acid as a coligand.
99mTc-TOC shows a high affinity for SSR type 2 (3–6), but in preclinical studies of the AR42J rat pancreatic tumor cell line, 99mTc-TATE was more rapidly internalized and had a more favorable biodistribution in tumor-bearing rats (7).
Imaging with 99mTc-TATE and 99mTc-TOC showed these agents to have a greater tumor-to-nontumor ratio and greater uptake than 111In-pentetreotide (5,6,8). A further advantage of these 99mTc-labeled pharmaceuticals is a single-day procedure with an optimal acquisition time of between 3 and 4 h after injection—a protocol that costs less and is more convenient for patients and imaging staff than the standard 2-d protocol using 111In-pentetreotide (2,6,8).
The aim of this initial prospective study was to directly compare 99mTc-TOC and 99mTc-TATE in patients with confirmed GEP NET (group 2, according to the World Health Organization [WHO] classification) (9) who were undergoing routine SSR scintigraphy for staging or restaging, to determine whether the number of sites of disease seen with the 2 agents differed significantly and whether this number was affected by the biodistribution of the agents.
MATERIALS AND METHODS
Patients
This initial prospective clinical study was approved by the local Ethics Committee of the Central Clinical Hospital of the Ministry of Internal Affairs and Administration. All patients gave their informed consent before being included in the study.
SSR scintigraphy was performed on every patient using both 99mTc-TOC and 99mTc-TATE in random order. A total of 12 consecutive patients (5 men and 7 women; age range, 38–75 y; mean age, 55 y) were studied. All patients had a standard clinical work-up for NET in our dedicated diagnostic center. In addition to SSR scintigraphy, contrast-enhanced CT was performed on all patients, and clinical data from each patient were collected and collated (Table 1). The interval between the studies ranged from 7 to 28 d (mean, 12 d). None of the patients had received any radiolabeled peptide therapy before the study.
Patient Data
Radiopharmaceuticals
The peptide conjugates 99mTc-TOC and 99mTc-TATE were synthesized by standard F-moc solid-phase synthesis (7) and used for kits manufactured under aseptic conditions (Institute of Atomic Energy, Radioisotope Centre POLATOM). Commercially available stannous chloride, mannitol, tricine, and N,N′-diacetic acid were added. The detailed method of kit labeling with 99mTc, as well as the quality control of the radiopharmaceuticals, has been presented earlier (8). The labeling yield exceeded 90% in all cases, with free pertechnetate content being in the range of 3.63% ± 1.67% (thin-layer chromatography). Tests for sterility and bacterial endotoxins (limulus amoebocyte lysate test) were routinely performed to assess the quality of the prepared kits.
Imaging
Images were acquired 3–4 h after intravenous injection of a mean activity of 520 MBq (range, 480–560 MBq) of 99mTc-TOC and 99mTc-TATE using a double-head camera (e-cam; Siemens) A low-energy, high-resolution, parallel-hole collimator with a single-photopeak window (140 keV ± 15%) was used, and all patients underwent a whole-body scan using a standard 256 × 1,024 matrix and an 8 cm/min table speed. In each case, a tomographic SPECT acquisition was performed using a 360° orbit, 64 projections, 25 s per projection, a 128 × 128 matrix, and no zoom. Reconstruction algorithms were based on commercially available iterative reconstruction software: 3-dimensional ordered-subsets expectation maximization (e-soft workstation, version 4.5; Siemens).
CT
To confirm the presence and sites of tumors, we routinely performed multislice 3-phase CT (Aquilon; Toshiba) on all patients. CT was performed with 1-mm contiguous sections using a standard 512 × 512 matrix.
Image Analysis
Each study was visually and independently evaluated by nuclear medicine physicians who were experienced in the interpretation of SSR scintigraphy studies using either technetium- or indium-labeled radiopharmaceuticals. The readers of the scans were aware of the underlying disease and the results of standard staging procedures. Corresponding studies were compared and analyzed lesion by lesion.
Any focal tracer accumulation exceeding expected regional tracer uptake was rated as a pathologic finding (tumor uptake). Diffuse low-activity intestinal uptake was rated as nonspecific, physiologic uptake. In relevant areas, SPECT images using an additional 3-dimensional reconstruction and a cine view were available to the viewer for each patient.
All data were analyzed from planar views using an e-soft tool. For each patient, regions of interest (ROIs) for semiquantitative analysis were drawn over the most active regions of tumor activity from the liver and left kidney (taking care in drawing the ROIs to prevent liver activity from interfering with the right-kidney ROI and to clearly separate left-kidney activity from spleen activity). An additional separate ROI was drawn over a peripheral part of the right lung to act as a surrogate background ROI. This region was chosen because it could easily be seen on both the nuclear medicine image and the confirmatory CT scan to ensure that any site of tumor was avoided in the background region when the ROI was drawn.
Parts of organs showing tumor infiltration or superimposition were excluded in the evaluation of organ uptake. Mean counts per pixel in each ROI were calculated. In each case, when the target-to-background ratio was calculated, the most prominent site of confirmed tumor, left kidney, and liver was included. Anterior views were used to analyze the results, with the same ROIs being used within the same patient.
To ensure good matching of tumors detected by each radiopharmaceutical, we used the standard image-fusion tool supplied with the Siemens computer system. Tumor extent was determined on the basis of structural and functional imaging and clinical follow-up for at least 6 mo (2,4–8).
Statistical Analysis
The calculated target-to-background ratios for the tumor, liver, and kidneys were tested using a Kolmogorov-Smirnov 1-sample test. The Wilcoxon matched-pair test was used to determine statistically significant differences in the target-to-background ratio between 99mTc-TOC and 99mTc-TATE (P < 0.05 was defined as significant).
RESULTS
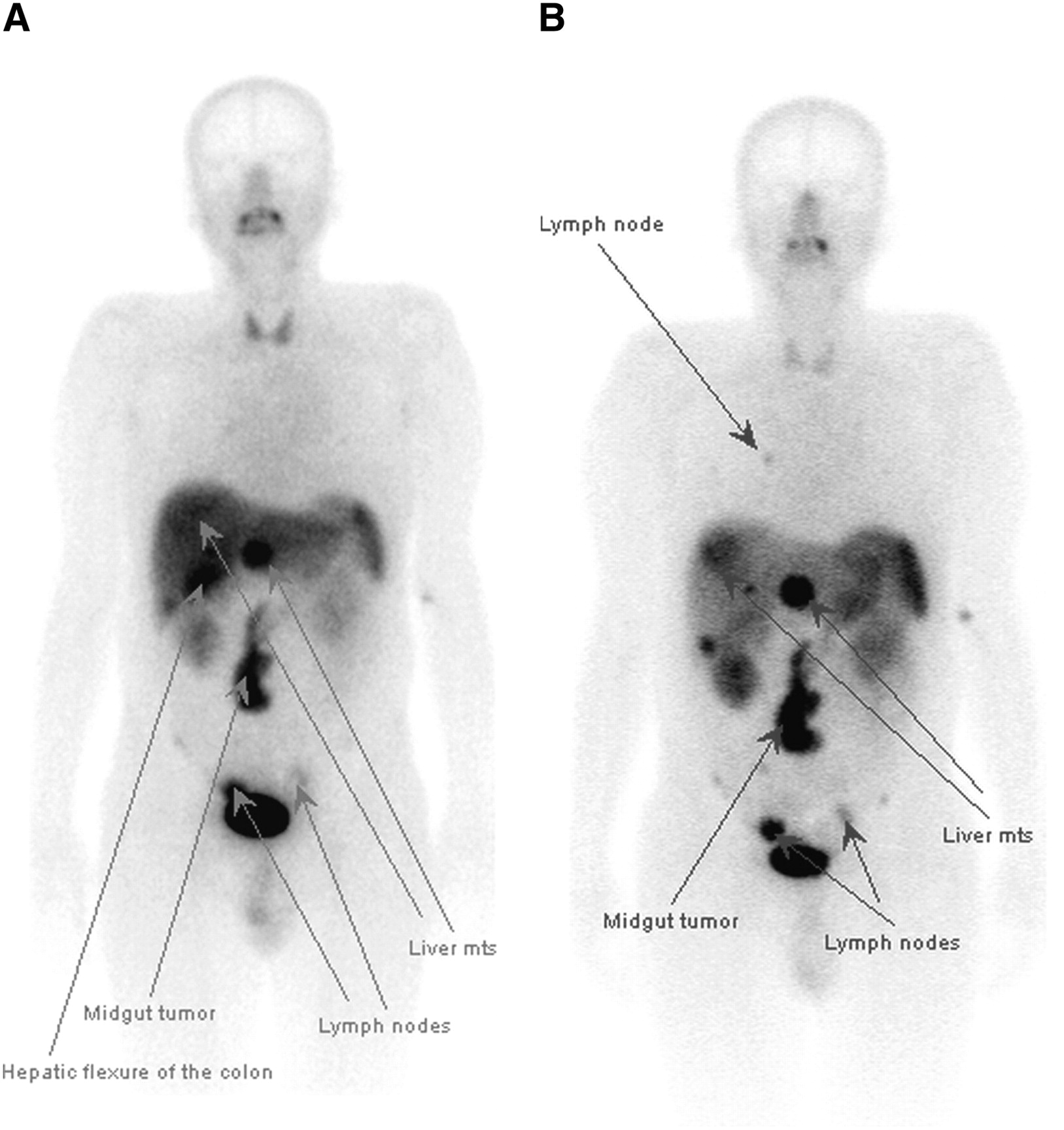
The image quality with both agents was determined by both readers to be excellent, with lesion definition as good as or better than that expected from 111In pentetreotide imaging. 99mTc-TOC revealed 110 sites of disease, and 99mTc-TATE 115 sites. All lesions were at sites of abnormalities on CT. An interobserver analysis demonstrated 95% agreement between the 2 readers, including both the site and the number of detected lesions, and 100% agreement for evaluation of tumor extent. 99mTc-TOC and 99mTc-TATE were congruent in identifying tumor extent in 7 patients (58%) (Table 2). In a single patient, uptake in the neck lymph nodes was seen with 99mTc-TOC but not with 99mTc-TATE, and these nodes were confirmed as pathologic on CT. However, in 4 patients, more sites of lymph node metastasis were seen with 99mTc-TATE imaging, including 1 patient in whom uptake in the right lung hilum was seen with 99mTc-TATE but not 99mTc-TOC (Fig. 1).
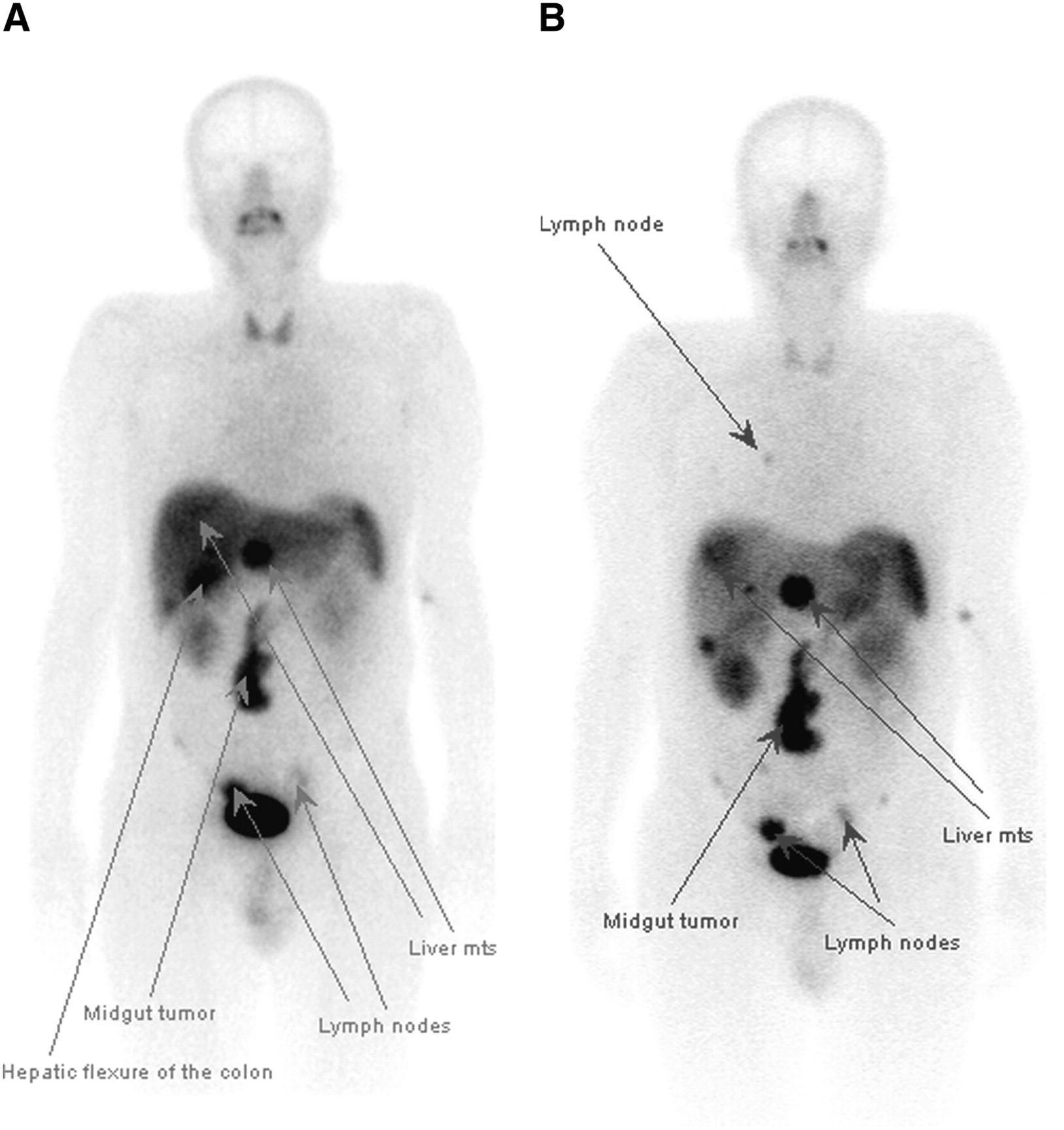
A 56-y-old patient with WHO group 2 GEP NET (midgut carcinoid with carcinoid syndrome). Whole-body images obtained with 99mTc-TOC (A) and 99mTc-TATE (B) show nonresectable large tumor of small-bowel mesentery, multiple liver deposits, and local and regional lymph node involvement, with additional right-side mediastinal lymph node involvement seen only with 99mTc-TATE. False-positive uptake in hepatic flexure of colon is seen with 99mTc-TOC but not with 99mTc-TATE. mts = metastases.
Numbers of Lesions Seen Using 99mTc-TOC and 99mTc-TATE
The number of liver metastases seen with both agents was identical in 7 of 8 patients with liver metastases, and up to 20 individual liver lesions were seen with both agents. Clear-cut uptake and good separation of the lesions were much better seen on SPECT than planar images; however, in 1 patient liver metastases were seen only with 99mTc-TATE. There was complete agreement in identification of the site of the primary tumor (nonresectable) in 8 patients with both tracers (Fig. 2).
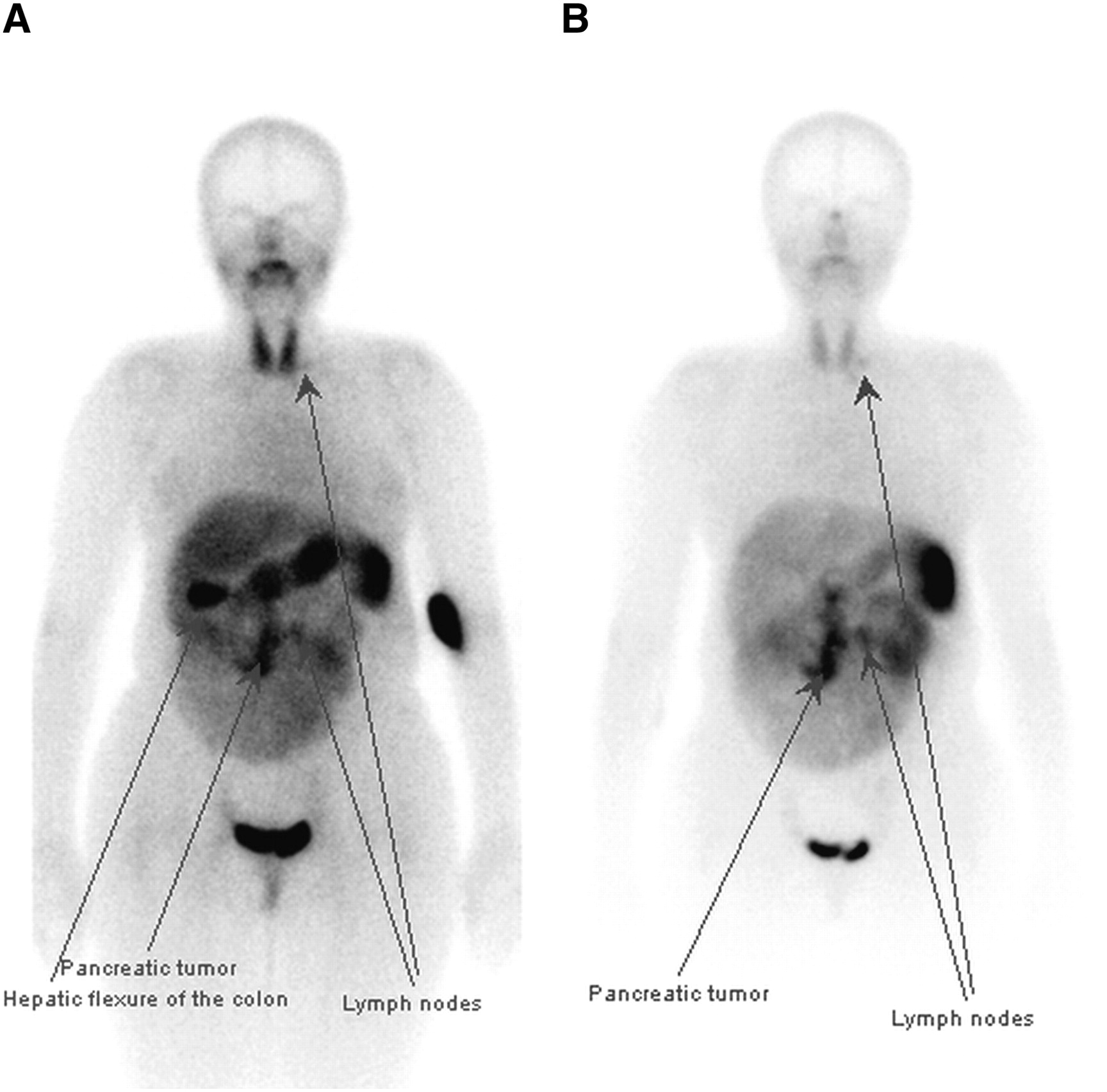
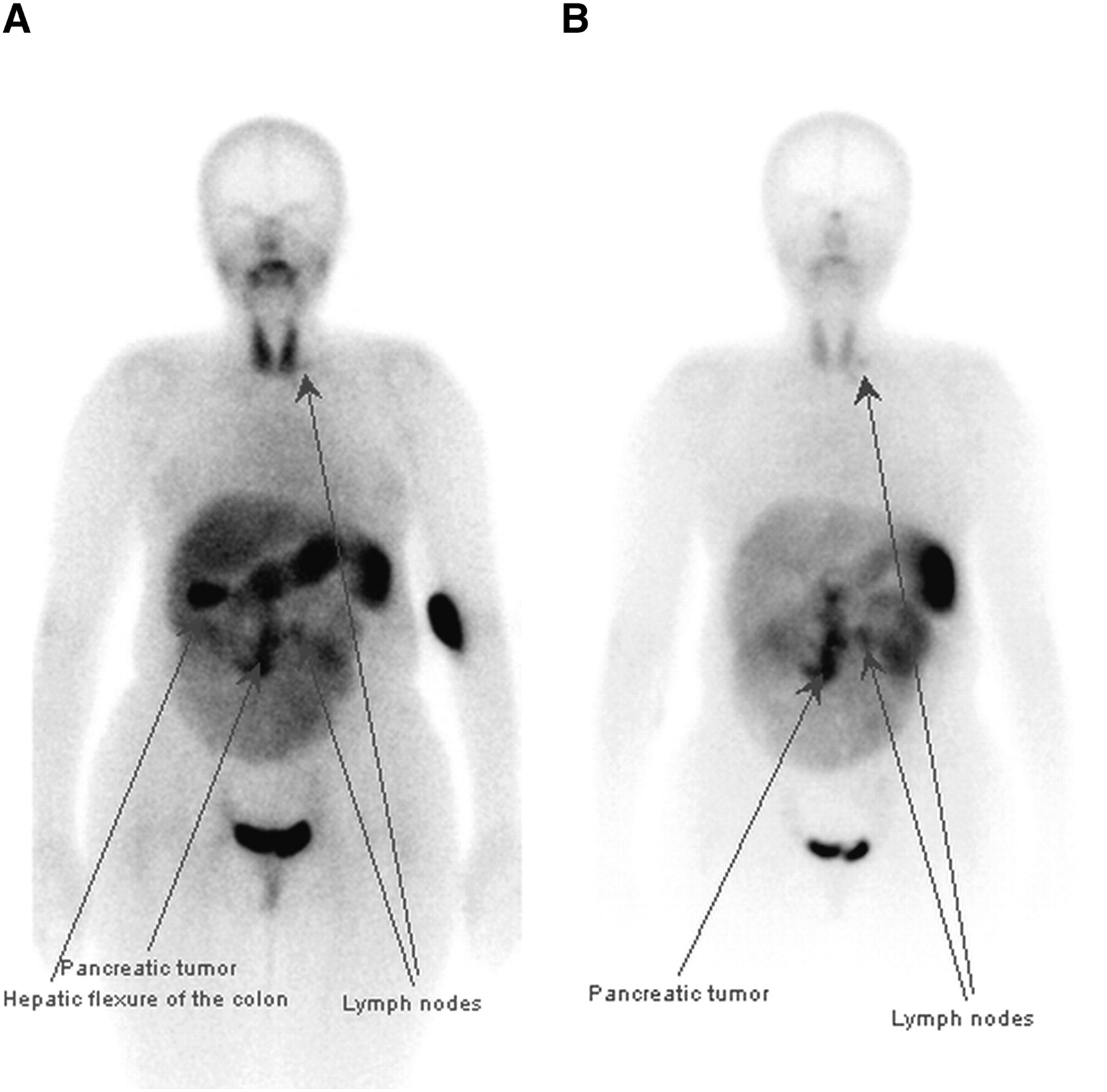
A 46-y-old patient with WHO group 2 GEP NET (foregut, pancreas, nonsecretor). Whole-body images obtained with 99mTc-TOC (A) and 99mTc-TATE (B) show nonresectable large tumor within pancreas, regional lymph node involvement, small amount of ascites, and 2 supraclavicular lymph nodes. Additional false-positive uptake in colonic hepatic flexure is seen clearly with 99mTc-TOC but not with 99mTc-TATE.
Though gut uptake of 99mTc-TOC was greater than gut uptake of 111In-pentetreotide on 24-h imaging, identification of intraabdominal disease with 99mTOC still was possible. For disease in the abdominal lymph nodes and other intraabdominal sites, more lesions were shown with 99mTc-TATE than with 99mTc-TOC in 2 patients.
Analysis of mean target-to-background ratios for 99mTc-TOC showed tumor uptake to be 8.9 (range, 1.0–39.9; SD, 11.6), liver uptake to be 5.9 (range, 2.5–21.6; SD, 5.4), and kidney uptake to be 4.7 (range, 1.7–9.5; SD, 2.5). The mean target-to-background ratio for 99mTc-TATE was in the tumor (7.3; range, 1.0–23.6; SD, 6.4), liver (4.2; range, 1.7–8.6; SD, 2.4), and kidney (5.9; range, 2.7–11.6; SD, 3.0). Tumor uptake did not significantly differ between the 2 radiopharmaceuticals. Uptake of 99mTc-TOC was significantly higher in the liver (P = 0.008), and a nonsignificant tendency toward higher uptake of 99mTc-TATE in the kidney was observed (P = 0.071) (Fig. 3). The number of lesions identified did not significantly differ at any site between the 2 agents.
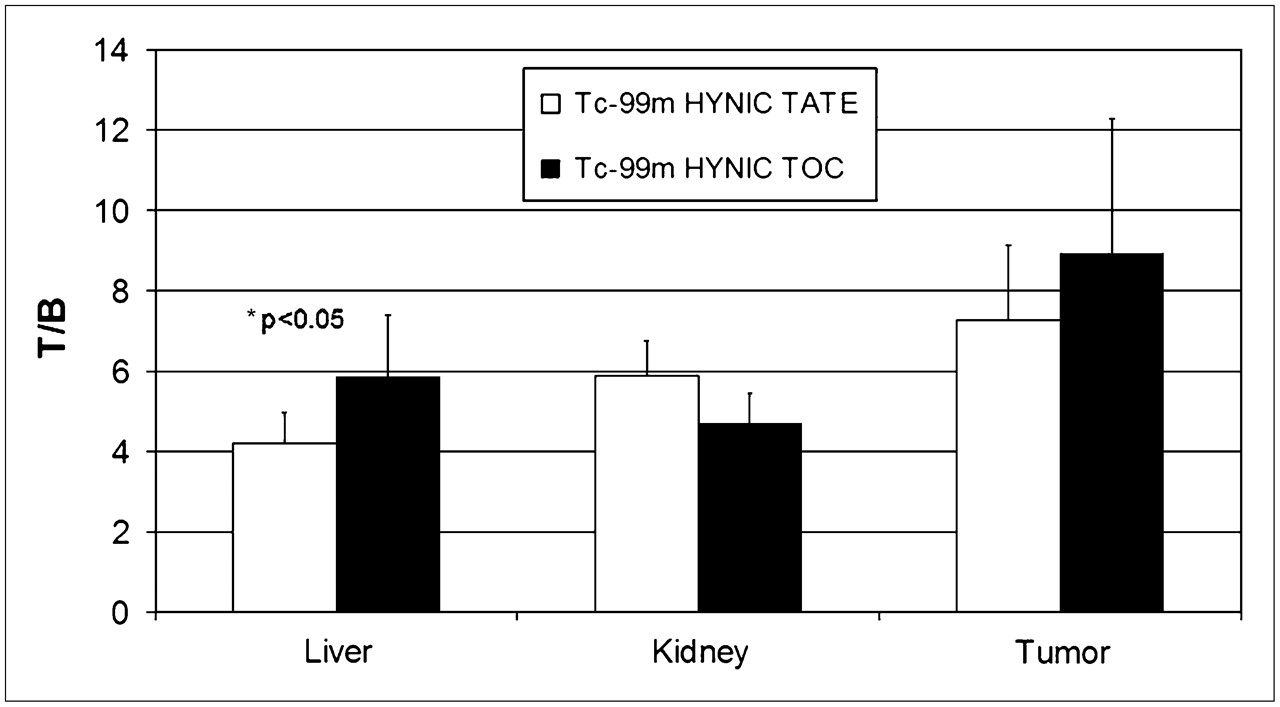
Comparison of mean target-to-background (lung) ratios (T/B), including liver, kidney, and tumor uptake of both 99mTc-TOC and 99mTc-TATE.
DISCUSSION
In our initial study of SSR scintigraphy using 99mTc-TOC and 99mTc-TATE, we compared a limited group of 12 patients with histologically confirmed GEP NET. Those tumors had a well-known high expression of SSR type 2 receptor, and both radiotracers had high affinity to this type of receptor (1,2,4,5,8). Although 99mTc-TOC has been used in research for 7 y (and has been licensed for clinical use in Poland) and 99mTc-TATE has been available only for research for 4 y (3–8,10–12), this is the first time they have been directly compared in the same patients. The limitation of this initial study was the small number of patients, though the tumor group was fairly uniform. The results of this study showed that both agents could be used in routine SSR scintigraphy, though 99mTc-TATE may have the advantage, especially in tumors within the liver. Planar whole-body and SPECT images with both agents have good quality when acquired as soon as 1 h and up to 4 h, with the highest target-to-background ratio seen at 4 h. SPECT images of the liver and abdomen, especially, showed clear-cut uptake of the tracer in NET metastases.
Experience with these peptides that specifically label SSR type 2, which have been available only for clinical trials, has been limited to a small number of countries mainly in Europe. 99mTc-depreotide (NeoSpect; CIS Bio), which also binds to SSRs, has been available in the United States and Europe for many years, but its affinity is not optimal for most GEP NETs. In transfected cell lines, 99mTc-depreotide has a slightly lower affinity than does standard 111In-pentereotide for SSR type 2 (Kd, 2.5 vs. 1.5) and for SSR type 5 (Kd, 2 vs. 0.5) but higher affinities for SSR type 3 (Kd, 1.5 vs. 15) (13). At present, there has been no direct comparison between either 99mTc-TOC or 99mTc-TATE and 99mTc-depreotide, though the preclinical data suggest that in NETs depreotide may have a poorer image quality possibly because of increased background activity resulting form its pan-receptor affinity. Consequently, depreotide is unlikely to present sufficient affinity at any tumor site to be used for radiotargeted therapy using 90Y- or 177Lu-labeled forms (14).
In common with many labeled proteins, significant nonspecific accumulation sometimes occurs within the bowel and can be misreported as tumor. This problem has been described in previous studies using 99mTc-TOC and a single study using 99mTc-TATE (4–8,12). In our experience, routine bowel preparation was not helpful in preventing persistent nonspecific bowel activity (Figs. 1A and 2A). For example, in a few cases using 99mTc-TOC we found that activity in the hepatic flexure of the colon had no confirming tumor on correlative imaging and clinical follow-up. Nonspecific bowel activity has been described by other authors, especially with 99mTc-TOC, with reports of high levels of uptake in the bowel or gallbladder (6,7,12). The physiologic bowel accumulation was seen near the hepatic flexure, but we have not seen gallbladder accumulation. In our experience in performing more than 400 clinical examinations on NET patients, large-bowel uptake has been seen in less then 10% of patients using 99mTc-TOC.
CONCLUSION
This initial report and other studies conform that the 99mTc-based SSR type 2 receptor ligands 99mTc-TOC and 99mTc-TATE could be effective agents for SSR scintigraphy in GEP NET. A similar number of metastatic sites can be seen with both agents, with an 85% concordance rate on a site-by-site analysis, though 99mTc-TATE may have some advantage in lymph node and liver metastases. Likewise, the lower physiologic uptake of 99mTc-TATE in the liver makes this the agent of choice to pursue in wider, phase III, trials.
Acknowledgments
This work was supported in part by research grant 2 P05A 02428 from the Polish Ministry of Science and Higher Education.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 3, 2007.
- Accepted for publication March 4, 2008.





{kind=link}
{kind=link}
{kind=link}