


Abstract
Morbidity and mortality increase when diastolic dysfunction accompanies coronary artery disease (CAD). An elevated stress 201Tl lung-to-heart ratio (LHR) is a traditional marker of elevated left ventricular end-diastolic pressure (LVEDP), which adds prognostic value in CAD. Since the introduction of 99mTc-labeled agents, this valuable marker has been lost. Hence, there is only a limited ability to assess diastolic dysfunction by myocardial perfusion imaging (MPI). Methods: Fifty-two consecutive patients with an ejection fraction of ≥45% underwent MPI and cardiac catheterization within 15 d. Peak filling rate (PFR), time to PFR (TPFR), and filling rate during the first third of diastole (1/3FR) were obtained from MPI with SPECT software. Resting 201Tl LHR was calculated manually, and LVEDP was obtained at catheterization. Results: PFR, TPFR, and 1/3FR correlated significantly with LVEDP (r = −0.53, 0.45, and −0.45, respectively; P = 0.00005, 0.0009, and 0.0009, respectively), whereas resting 201Tl LHR did not (r = 0.10, P = 0.49). Receiver-operating-characteristic curve analysis of PFR, TPFR, and 1/3FR for detecting LVEDPs of ≥18 mm Hg showed areas under the curve of 0.83, 0.75, and 0.80, respectively. The combination of PFR and 1/3FR showed a negative predictive value of 84%, a positive predictive value of 86%, and a specificity of 94%. Conclusion: Diastolic filling variables obtained with the SPECT software showed a significant correlation with LVEDP. PFR, TPFR, and 1/3FR were superior to resting 201Tl LHR and showed good sensitivity, specificity, and predictive power for detecting LVEDPs of ≥18 mm Hg. Hence, combining data on the presence of perfusion defects with data on diastolic impairments can be achieved by adding these variables to MPI results.
Diastolic dysfunction, if present with coronary artery disease (CAD), increases morbidity and mortality 4-fold (1–3). Elevated stress 201Tl lung uptake during myocardial perfusion imaging (MPI) reflects left ventricular diastolic dysfunction. Studies have shown that increased stress 201Tl lung uptake correlates well with increased left ventricular filling pressure (4–7). Hence, an increased stress 201Tl lung-to-heart ratio (LHR) identifies diastolic dysfunction, which can be considered in combination with the presence of perfusion defects. However, the use of stress 201Tl LHR has declined because of the increased use of 99mTc-labeled tracers in most laboratories. 201Tl is still used as the rest imaging agent in dual-isotope stress and rest–redistribution viability protocols. Unfortunately, the value of resting 201Tl LHR and stress 99mTc LHR for detecting increased left ventricular end-diastolic pressure (LVEDP) is limited (8–10). Hence, there is a need for new methods for assessing diastolic dysfunction during MPI.
It is feasible to assess left ventricular diastolic function with the diastolic filling curve from radionuclide angiography (11,12). Good correlations have been shown for diastolic function variables derived from radionuclide ventriculography and 16-frame gated SPECT (13,14). However, it is not known whether these variables can predict LVEDP in patients undergoing MPI.
The purpose of this study was to assess the ability of left ventricular filling curve variables derived from 16-frame gated MPI to predict LVEDP in patients with preserved systolic function. We also compared the predictive power of these parameters with that of commonly used resting 201Tl LHR.
MATERIALS AND METHODS
Population
We reviewed our hospital electronic medical records to identify patients who had undergone MPI and cardiac catheterization between December 2005 and December 2006. A total of 52 patients had undergone both of these procedures within 15 d. All patients with an ejection fraction of ≥45% were included because such patients are considered to have preserved left ventricular systolic function (15). Patients were excluded if there was any significant interval clinical intervention or change in medication between MPI and cardiac catheterization, irregular rhythm, and an incomplete medical record. The study was approved by the local institutional review board.
MPI
All patients underwent dual-isotope MPI with 111–148 MBq of 201Tl at rest and 925–1,110 MBq of 99mTc for stress acquisition. Fifteen minutes after 201Tl-labeled tracer injection, resting SPECT images were acquired. Sixty minutes after 99mTc-labeled tracer injection, at peak stress, electrocardiogram-gated SPECT images were obtained. A fixed 90° dual-detector camera (C-cam; Siemens Medical Systems) with elliptic 180° arc (45° right anterior oblique to 45° left posterior oblique), 32 projections at 30 s per projection, and 16 frames per R–R interval was used to acquire SPECT data. The projection data were reconstructed into tomographic transaxial images by use of a filtered backprojection technique with a 3-dimensional ramp Butterworth filter (order, 4; cutoff frequency, 0.50 cycle per pixel). For data analysis, 4D-MSPECT software (University of Michigan) was applied to determine the left ventricular ejection fraction (LVEF), end-diastolic volume (EDV), and end-systolic volume. 4D-MSPECT software automatically fits the left ventricular volume curve (Fig. 1) with a fourth-order harmonic function and derives peak filling rate (PFR), time to PFR (TPFR), and filling rate during the first third of diastole (1/3FR). All diastolic measurements were obtained during stress-gated 99mTc MPI.
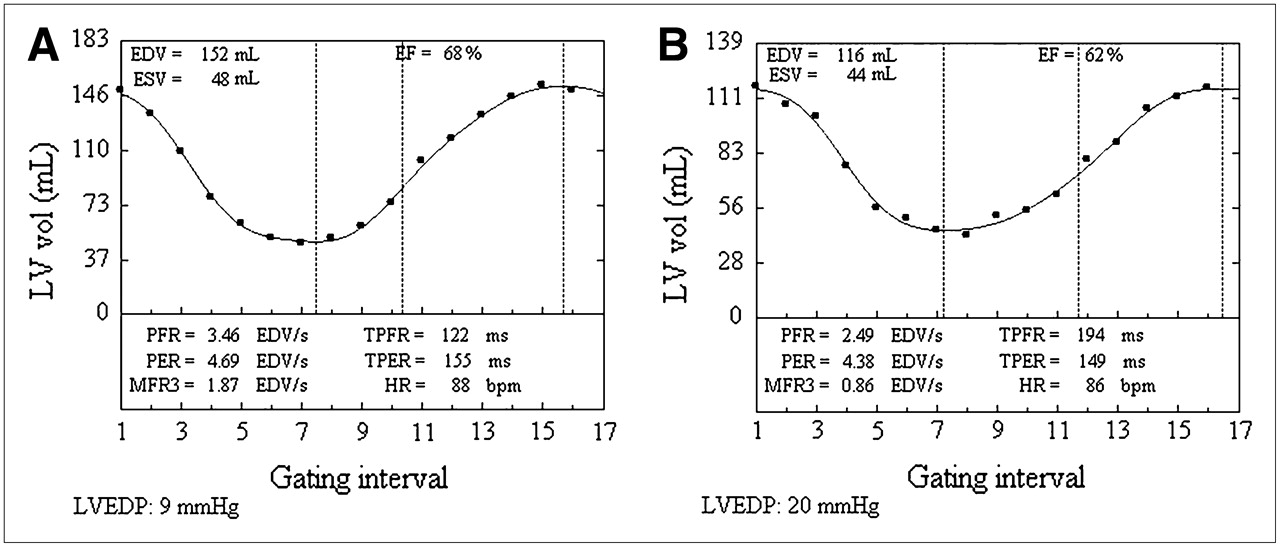
Left ventricular diastolic filling curves derived from 4D-MSPECT. (A) Curve with normal diastolic filling parameters. (B) Curve with abnormal diastolic filling parameters. LVEDPs determined at subsequent cardiac catheterization are shown. bpm = beats per minute; EF = ejection fraction; ESV = end-systolic volume; HR = heart rate; LV = left ventricular; MFR3 = filling rate during first third of diastole; PER = peak emptying rate; TPER = time to peak emptying rate; vol = volume.
Resting 201Tl LHR Calculation
The anterior projection frame obtained during resting 201Tl SPECT acquisition was used to calculate LHR. Fixed-size square regions of interest were drawn, one over the right lung field and the other over the myocardial wall with the highest count density. LHR was defined as mean counts per pixel in the lung regions of interest divided by mean counts per pixel in the myocardial regions of interest.
Cardiac Catheterization
All patients underwent left heart catheterization, coronary angiography, and left ventriculography within 15 d of MPI. A fluid-filled high-fidelity micromanometer pigtail catheter was placed in the left ventricle under fluoroscopic guidance. LVEDP was measured before and after ventriculography, and the average of all measurements was obtained. LVEDPs of ≥16 mm Hg are considered abnormal (15,16). We applied a more stringent criterion for abnormal LVEDPs: ≥18 mm Hg.
Statistical Analysis
Numeric variables are expressed as the mean ± 1 SD, and categoric variables are presented as numbers and percentages. The Pearson correlation was used to analyze the relationships of PFR, TPFR, 1/3FR, and resting 201Tl LHR with LVEDP. Hotelling t tests were performed to evaluate differences between correlation coefficients (17). Receiver-operating-characteristic (ROC) curve analysis was performed with Analyse-it software (Analyse-it Software, Ltd.) to evaluate the sensitivity and specificity of different PFR, TPFR, and 1/3FR values for detecting LVEDPs of ≥18 mm Hg. The optimal PFR, TPFR, and 1/3FR cutoff values for providing maximum accuracy were then determined. A P value of <0.05 was considered to be statistically significant.
RESULTS
Demographics
The characteristics of the study population are shown in Table 1. Fifty-two patients met all criteria. Patients were more likely to be men (58%), and the mean age of the population was 58 ± 11 y (range, 36–85 y). The mean interval between MPI and cardiac catheterization was 8 d. All patients underwent coronary angiography, and 38 patients (73%) had CAD. Fifteen patients (29%) had diabetes, and 42 patients (81%) had hypertension. All patients had LVEFs of ≥45% (the mean LVEF was 54%), and the mean LVEDP was 15 mm Hg.
Characteristics of Study Population
4D-MSPECT Diastolic Function Parameters and LVEDP
The association between diastolic function parameters from 16-frame gated SPECT and LVEDP is shown in Figure 2. There were significant inverse correlations between LVEDP and PFR (r = −0.53, P = 0.00005) and between LVEDP and 1/3 FR (r = −0.45, P = 0.0009). There was also a significant positive correlation between LVEDP and TPFR (r = 0.45, P = 0.0009). Correlations remained significant and similar in the presence or absence of CAD (r = 0.42–0.57, P < 0.05), except that 1/3FR did not achieve statistical significance in patients without CAD.
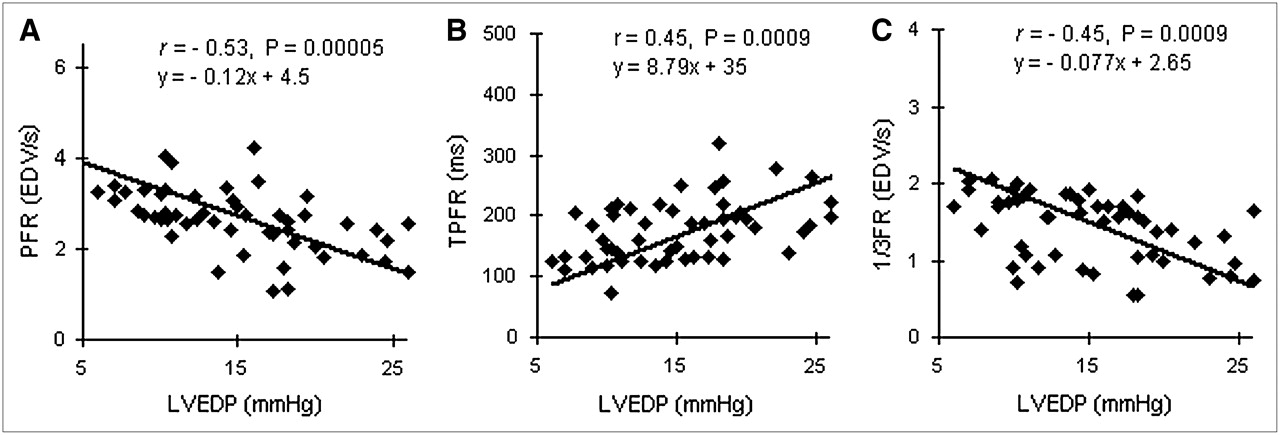
Correlations between 4D-MSPECT diastolic parameters and LVEDP.
Resting 201Tl LHR and LVEDP
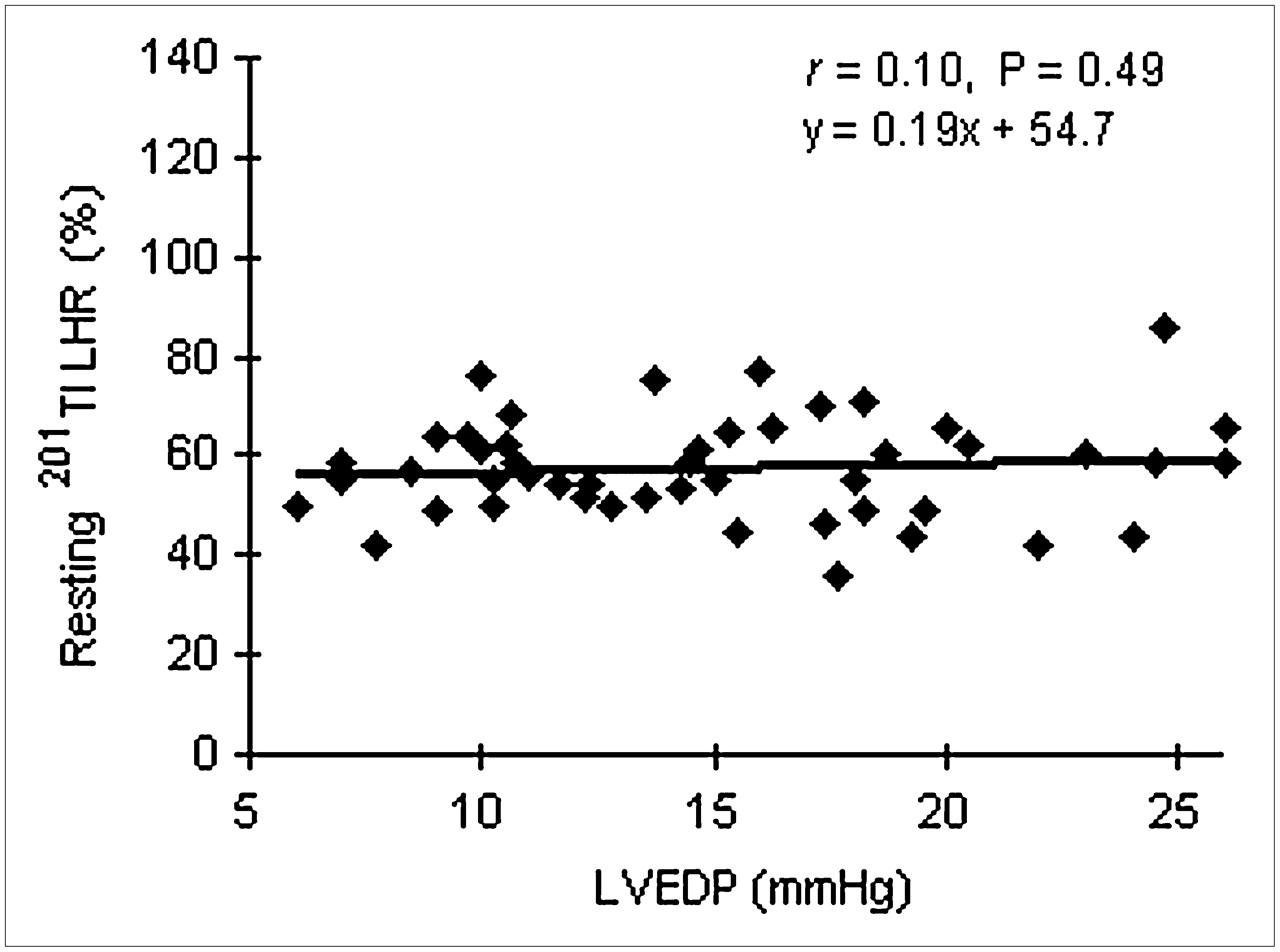
The correlation between LVEDP and resting 201Tl LHR was not statistically significant (r = 0.10, P = 0.49) (Fig. 3).
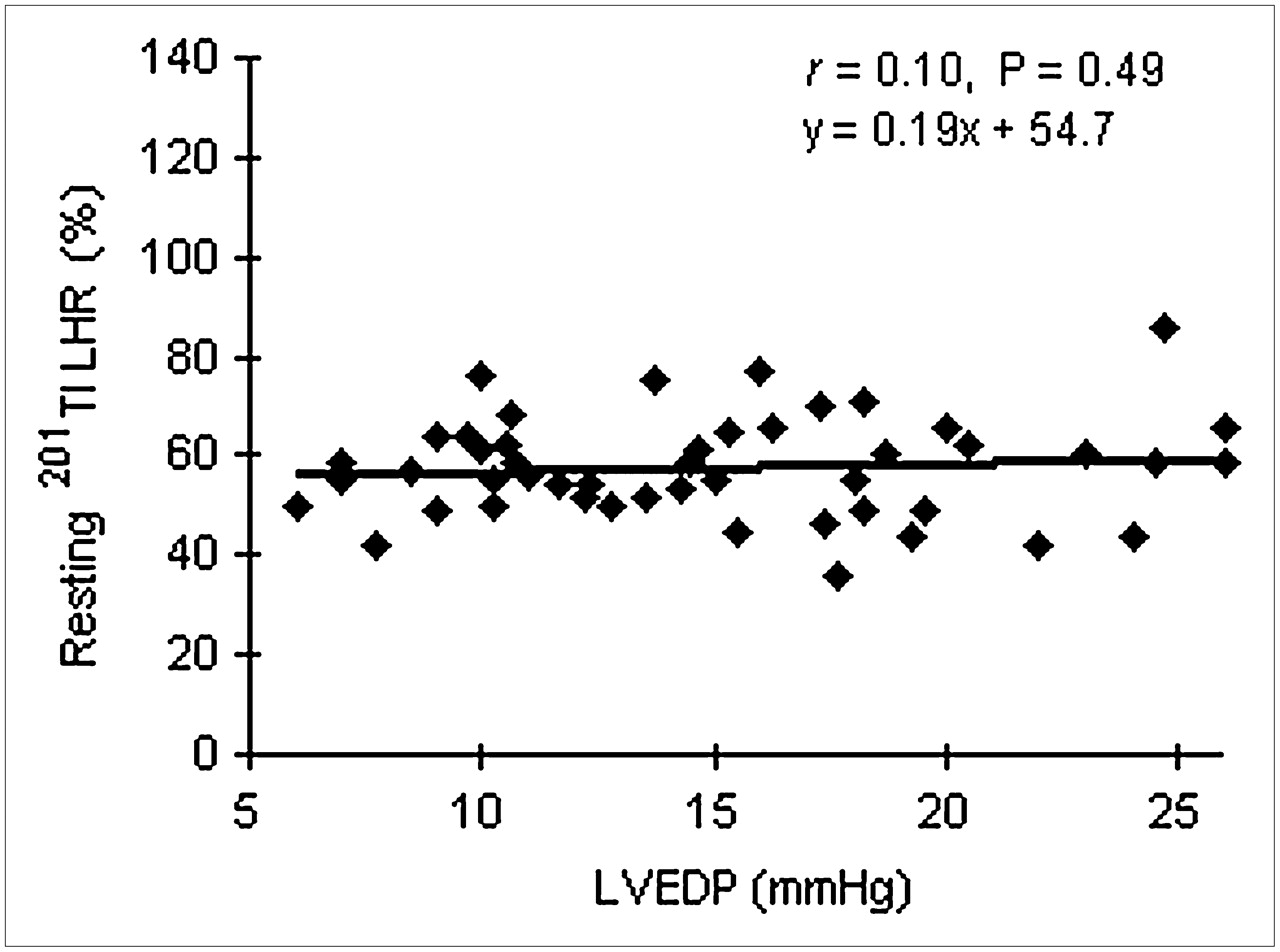
Correlation between LVEDP and resting 201Tl LHR.
Comparison of Correlation Coefficients
Hotelling t test values, used for comparisons among 3 correlation coefficients (for PFR, TPFR, and 1/3FR vs. LVEDP), were not significant (t ≤ 1, P > 0.05 for all). Therefore, no linear correlation with LVEDP was superior among the 3 filling parameters.
ROC Curve Analysis
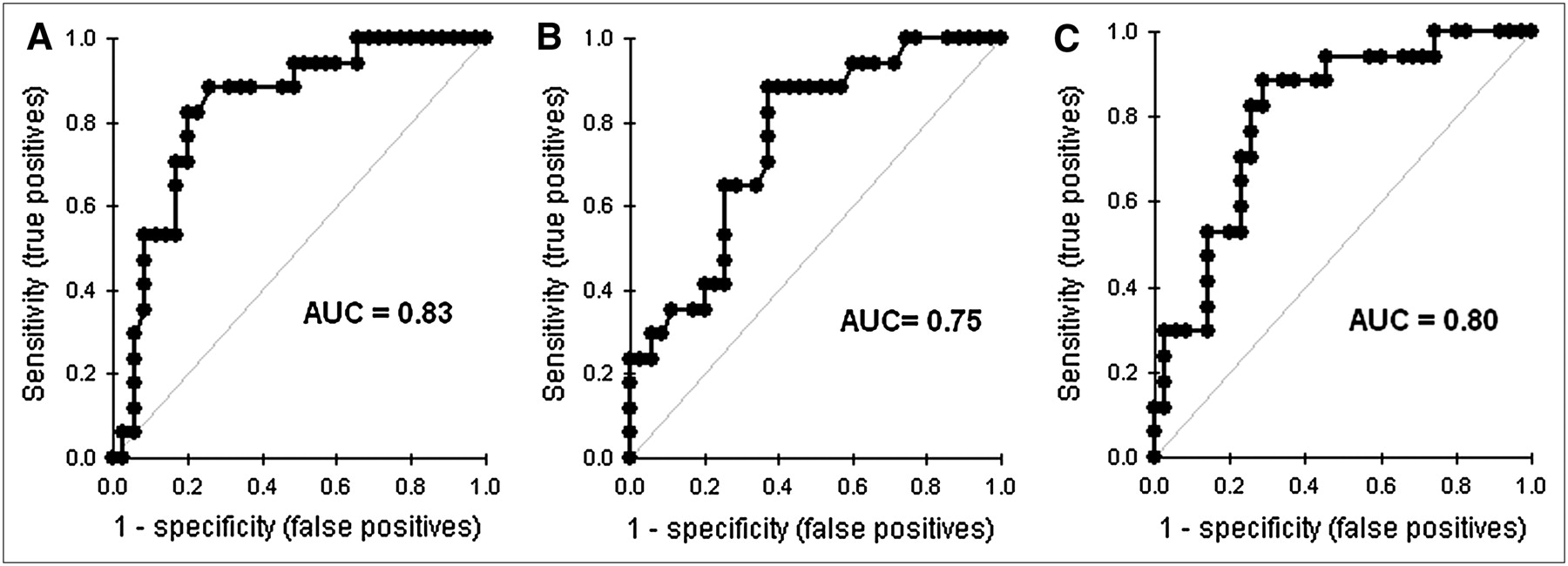
The ROC curves for detecting LVEDPs of ≥18 mm Hg or <18 mm Hg with PFR, TPFR, and 1/3FR are shown in Figure 4. The areas under the curve (AUCs) for PFR, TPFR, and 1/3FR were 0.83, 0.75, and 0.80, respectively. The optimal PFR, TPFR, and 1/3FR cutoff values for providing maximum sensitivity and specificity were ≤2.57 end-diastolic volume per second (EDV/s), ≥161 ms, and ≤1.52 EDV/s, respectively.
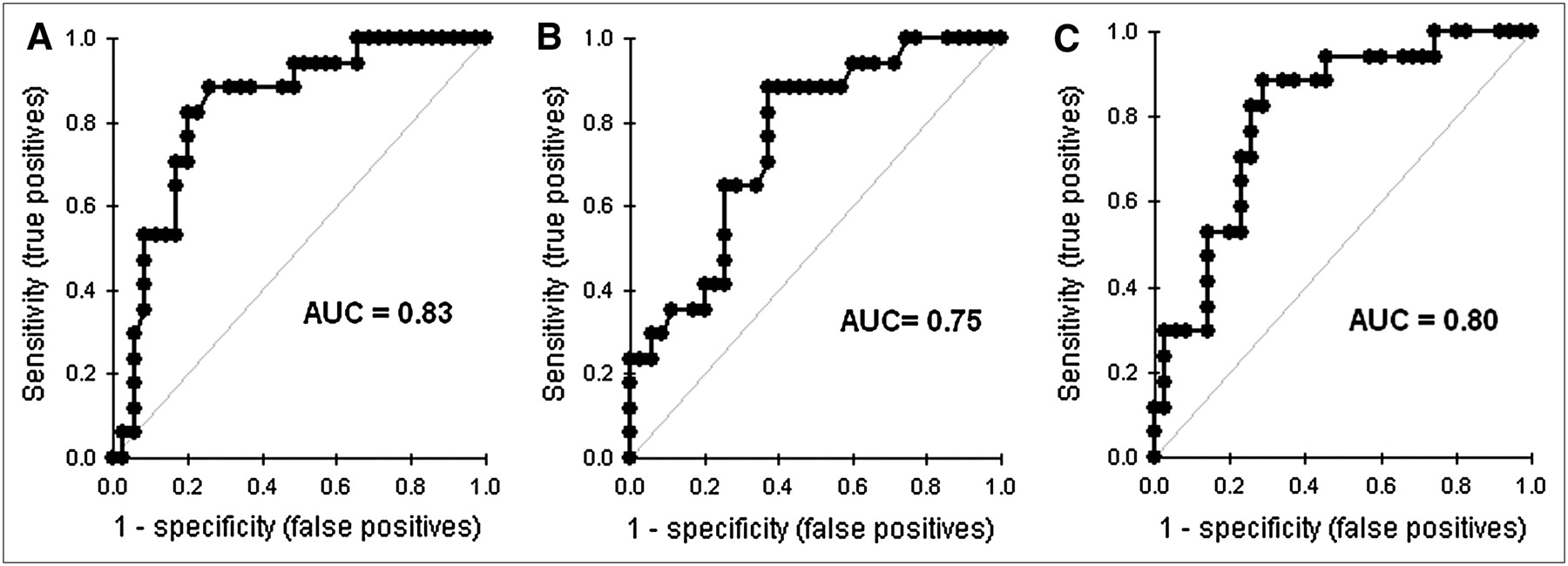
ROC curve analysis for ability of PFR (A), TPFR (B), and 1/3FR (C) to detect LVEDPs of ≥18 mm Hg or <18 mm Hg.
These PFR, TPFR, and 1/3FR values showed sensitivities of 82%, 88%, and 82% and specificities of 80%, 63%, and 74%, respectively, for correctly identifying patients with LVEDPs of ≥18 mm Hg. Each diastolic filling variable showed a positive predictive value (PPV) of ≥54% and a negative predictive value (NPV) of ≥90%.
Hence, all diastolic filling parameters improved the ability to detect LVEDPs of ≥18 mm Hg (AUCs of ≥0.75). These parameters showed good sensitivity (≥82%), but the specificity (≥63%) and the PPV (≥54%) were modest. The NPV of these parameters for identifying patients with LVEDPs of <18 mm Hg was remarkably good (≥90%).
After identifying these 3 variables as predictors of diastolic dysfunction, we investigated the incremental effect of the presence of more than one variable. TPFR correlated well with PFR and 1/3FR (r = −0.32 and −0.64, respectively; P = 0.02 and <0.0001, respectively), whereas PFR did not correlate with 1/3FR (r = 0.18, P = 0.19). Because there was no correlation between PFR and 1/3FR, it was feasible to use these 2 parameters in combination to assess their combined predictive power for LVEDPs of ≥18 mm Hg. When the results for both were above the cutoff values, PFR and 1/3FR combined showed a PPV of 86%, a sensitivity of 67%, and a specificity of 94% for detecting LVEDPs of ≥18 mm Hg. Similarly, the normal values for both of these parameters showed an NPV of 84% for detecting LVEDPs of <18 mm Hg. All values from the ROC curve analysis are shown in Table 2.
ROC Curve Analysis, Sensitivity, Specificity, PPV, and NPV
DISCUSSION
The predictive power of MPI for subsequent cardiac events and the severity of CAD is significantly enhanced when stress 201Tl lung uptake is added to the extent and severity of perfusion defects (4,18–20). Several studies have shown that increased stress 201Tl lung uptake correlates very well with increased left ventricular filling pressure (4–7). Elevated LVEDP is a major predictor of left ventricular diastolic dysfunction (15,16) and has been shown to be an independent predictor of future clinical heart failure events (21) and mortality (1,22). In these circumstances, the ability to predict an elevation of LVEDP during MPI could improve the predictive power of myocardial perfusion studies for subsequent cardiac events.
At the present time, the majority of MPI studies are performed with stress 99mTc-labeled perfusion agents. With the transition from 201Tl to 99mTc, access to stress 201Tl lung uptake data is no longer available. With the loss of stress 201Tl LHR data, few studies have assessed the utility of stress 99mTc and resting 201Tl lung uptake for predicting left ventricular filling pressure (8–10,23).
Studies with 99mTc MPI have shown a very poor correlation between stress 99mTc LHR and elevated left ventricular filling pressure (9,10), probably because of the rapid washout of 99mTc from the lung during stress (24). Marcassa et al. (23) investigated the use of resting 201Tl LHR, which is quite often used with 99mTc in dual-isotope imaging. In a group of 159 consecutive patients with LVEFs of ≤35% (mean ± 1 SD, 23% ± 6%), resting 201Tl LHR had significant predictive power for subsequent cardiac events and mortality. Resting 201Tl LHR also correlated well with pulmonary capillary wedge pressure in 19 patients. This approach appeared to show some promise, especially because Patel et al. (10) showed a significant correlation between resting 201Tl LHR and stress 99mTc LHR (r = 0.55, P < 0.01). However, correlation coefficients for stress 99mTc LHR with LVEDP and with pulmonary capillary wedge pressure were very modest, at 0.29 and 0.34, respectively. Despite the strong correlation between resting 201Tl LHR and stress 99mTc LHR, multivariate linear regression indicated that the relationship between pulmonary capillary wedge pressure and LVEDP was significant with stress 99mTc LHR but not with resting 201Tl LHR. Given the modest correlations and the rapid washout of 99mTc, the reporting of LHR with stress 99mTc is not a common practice. LHR with resting 201Tl appears to be somewhat inferior to LHR with stress 99mTc but, more importantly, it has never been validated in a group of patients with preserved left ventricular systolic function (8,10,23).
With the improved count statistics and resolution of MPI with a 99mTc-labeled radiotracer, LVEF and wall motion can be reliably assessed during MPI (25,26). More recently, diastolic filling curves were derived from an assessment of wall motion during diastole (13,14,27,28) with 16-frame acquisitions. Studies with gated MPI have shown that PFR, TPFR, and 1/3FR can be derived and show excellent correlations with the same markers derived from radionuclide angiography (13,14). Furthermore, these diastolic function parameters have been shown to correlate well with Doppler echocardiographic variables of diastolic dysfunction (28) and with plasma B-type natriuretic peptide levels (28). 4D-MSPECT software derives the second-derivative curve from wall motion and automatically calculates PFR, TPFR, and 1/3FR. We are not aware of any studies in which 4D-MSPECT was used to assess left ventricular diastolic parameters at MPI and correlating these parameters with LVEDP at subsequent cardiac catheterization.
Three diastolic parameters measured by 4D-MSPECT showed a robust correlation with LVEDP at subsequent cardiac catheterization within 15 d and without an interval event, an intervention, or a change in blood pressure medication. PFR and 1/3FR correlated negatively with LVEDP. An inverse correlation of decreasing values for PFR and 1/3FR with increasing values for LVEDP is expected in diastolic dysfunction, in which the filling rate decreases as LVEDP increases. Conversely, as diastolic dysfunction worsens, TPFR increases, as reflected by the positive correlation between increasing values for TPFR and LVEDP. Interestingly, resting 201Tl LHR was not correlated with LVEDP when LVEFs were ≥45%. These observations suggest the superiority of 4D-MSPECT diastolic filling variables over resting 201Tl lung uptake for assessing diastolic function.
We also evaluated the diagnostic utility of PFR, TPFR, and 1/3FR for detecting specific levels of LVEDP in patients with preserved systolic function. ROC curve analysis showed that the AUC was ≥0.75 for each of these parameters for detecting LVEDPs of ≥18 mm Hg. Individual parameters showed excellent sensitivity (≥82%) and modest specificity (≥63%), whereas the combination of abnormal values for PFR and 1/3FR showed a specificity of 94% for determining LVEDPs of ≥18 mm Hg. Hence, these parameters will provide excellent screening individually and, when combined, will represent a powerful diagnostic tool for the assessment of diastolic function during MPI.
The era of planar imaging and stress–redistribution 201Tl protocols enabled us to obtain stress 201Tl LHR, which provided significant predictive power for subsequent cardiac events. Our findings indicate that diastolic filling variables could improve the predictive power of MPI by allowing the integration of data on diastolic impairments with data on the severity and extent of myocardial perfusion defects. This integration could be applied to the new era of stress 99mTc-labeled agents and SPECT MPI. This investigation was performed with equipment that is either present or easily available in every clinical nuclear cardiology laboratory performing SPECT MPI. We believe that values of PFR, TPFR, and 1/3FR should be reported for all SPECT MPI studies to allow the detection of diastolic dysfunction in the presence or absence of CAD.
The novel aspect of the present study is that it is directly and widely applicable to the general population of patients being evaluated by MPI for suspected CAD. The vast majority of these patients have preserved systolic function and sometimes present with symptoms of dyspnea, which is considered an equivalent of angina (29,30). Patients with preserved systolic function generally have lesser degrees of diastolic dysfunction, unlike patients who were evaluated in previous nuclear studies (8,10,23) of LHR. We believe that our study is the first to combine a methodology for assessing myocardial perfusion with a methodology for detecting diastolic dysfunction in patients with preserved LVEF. If our retrospective findings are confirmed prospectively, then this technique can be applied immediately to most patients being evaluated for the presence of CAD in nuclear cardiology laboratories.
The use of left ventricular filling curve parameters to assess diastolic function is not helpful for patients with irregular heart rhythm because gating is disabled. Our patient population underwent MPI and cardiac catheterization within 15 d. This delay could have affected the volume status of the patients and therefore the LVEDPs measured at different time points. Despite this limitation, we found good correlations between diastolic function indices from MPI and LVEDPs. Because our study was retrospective, we relied on the accuracy of medical records. However, tracings of all LVEDP readings were manually checked, and nuclear studies were reprocessed and reanalyzed. Because the present study was a retrospective series of consecutive patients, a prospective investigation of this technique is indicated to validate its utility in predicting LVEDP at cardiac catheterization.
CONCLUSION
In patients with LVEFs of ≥45%, resting 201Tl LHR did not correlate significantly with LVEDP. Diastolic function parameters (PFR, TPFR, and 1/3FR) derived from 16-frame gated SPECT with 4D-MSPECT correlated significantly with LVEDP at cardiac catheterization. If the assessment of diastolic function is combined with MPI results for risk stratification, then 4D-MSPECT diastolic filling parameters are superior to resting 201Tl LHR, according to our observations. These parameters showed good sensitivity and specificity for detecting LVEDPs of ≥18 mm Hg and a good NPV for identifying patients with LVEDPs of <18 mm Hg. Combining PFR and 1/3FR can result in improved PPV (86%) and specificity (94%).
Acknowledgments
We thank Jimel Carpenter and Laura Norman for performing the reconstruction of myocardial perfusion scans and Mahendra K. Mandawat for critical revision of the article.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 28, 2007.
- Accepted for publication January 16, 2008.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.