


Abstract
Nonspecific incidental brain lesions (NILs) are being detected more frequently because of an increasing number of screening or research MRI scans of the brain, and their natural course is uncertain. Methods: In a prospective cohort study starting in 1999, we determined the outcomes of patients with incidental, nonenhancing, supratentorial, lobar, and small-volume (<10 mL) lesions, depending on the findings of MRI and PET with the 18F-labeled amino acid fluoroethyl-l-tyrosine (18F-FET). Patients with seizures, focal neurologic deficits, signs of local or systemic infection or inflammation, known brain disease, or any kind of previous cerebral treatment were excluded. Finally, 21 patients were eligible. MRI was performed in 19 of these patients because of nonspecific symptoms (such as headaches, dizziness, or sudden deafness), whereas 2 patients were healthy volunteers in MRI studies. Clinical follow-up and MRI scans were obtained at 4- to 6-mo intervals, and follow-up ranged from 3 to 8.5 y. Mean lesion-to-brain (L/B) ratios of ≥1.6 on 18F-FET PET were rated as positive. Results: Four different outcome groups were identified. In group A, 5 NILs regressed or vanished completely. All of these lesions were circumscribed on MRI, and 18F-FET uptake was negative, with an L/B ratio of 1.2 ± 0.2 (mean ± SD). In group B, 10 NILs were stable, without growth. All of these lesions were circumscribed on MRI, and 18F-FET uptake was negative (L/B ratio: 1.0 ± 0.1). In group C, 2 NILs grew slowly over years, and an astrocytoma of World Health Organization (WHO) grade II was diagnosed after resection in each case. The lesions were circumscribed on MRI, and 18F-FET uptake was negative (L/B ratios: 0.7 and 1.0). In group D, 4 NILs showed sudden and rapid growth, with clinical deterioration, and a high-grade glioma of WHO grade III or IV was diagnosed after resection in all cases. The lesions were diffuse on MRI, and 18F-FET uptake was significantly increased (L/B ratio: 2.0 ± 0.4) (P < 0.01 for group D vs. group A or group B). Conclusion: For NILs, a circumscribed growth pattern on MRI and normal or low 18F-FET uptake on PET are strong predictors for a benign course, with the eventual development of a low-grade glioma. In contrast, NILs with a diffuse growth pattern on MRI and increased 18F-FET uptake indicate a high risk for the development of a high-grade glioma.
An increasing number of cerebral MRI investigations are done in patients with relatively nonspecific symptoms, such as headaches or dizziness, in asymptomatic patients as a “brain check-up” MRI, or in healthy volunteers as research MRI. On these “screening” or “research” scans, sometimes an unexpected intracerebral lesion is visualized and is considered an incidental finding. On the basis of neuroradiologic criteria, most of these “incidentalomas” can be identified as meningiomas, pituitary adenomas, or aneurysms. For intracerebral white matter lesions, however, a specific neuroradiologic diagnosis is impossible in many cases. They are typically small, with a diameter of only 1 or 2 cm, are hypointense on T1-weighted images without contrast enhancement, and are hyperintense on T2-weighted images (Fig. 1). One of the possible differential diagnoses for this radiologic pattern is a low-grade glioma (LGG), although asymptomatic gliomas or lesions suggestive of gliomas are rarely identified on screening or research MRI examinations (1–5).

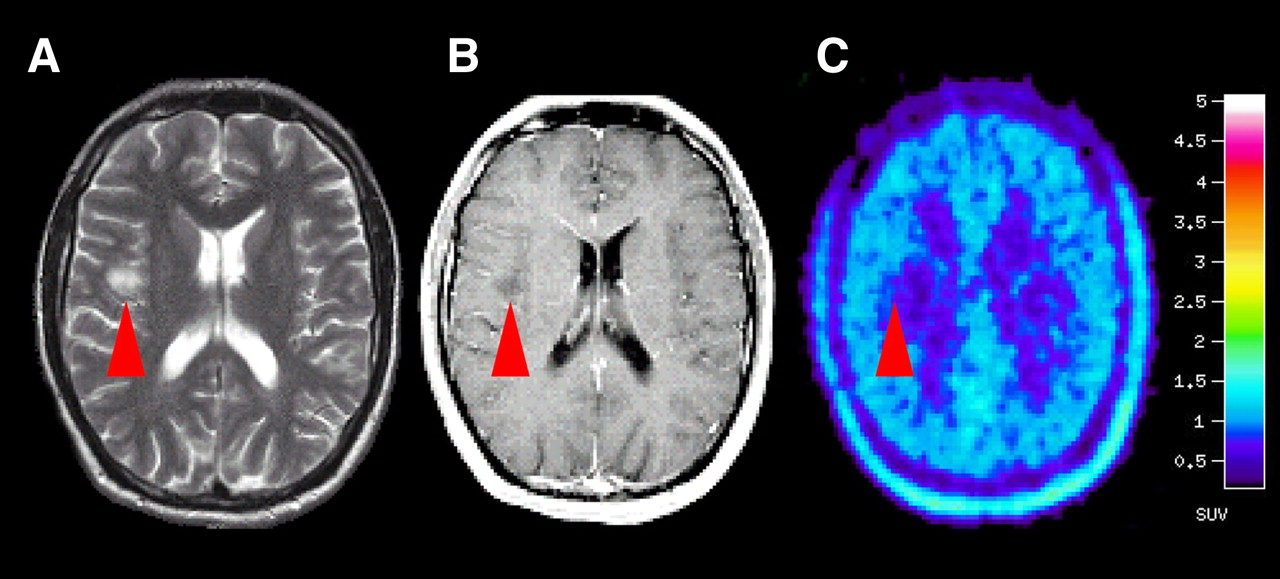
Typical example of NIL (red arrowhead) diagnosed in healthy young volunteer in brain research MRI study (patient 13). Axial T2-weighted (A) and contrast-enhanced axial T1-weighted (B) MR images revealed nonenhancing intracerebral right frontoinsular lesion. (C) Axial PET scan demonstrated no increased 18F-FET uptake in lesion compared with that in surrounding tissue (L/B ratio: 1.0). Five years later, MRI revealed unchanged, stable lesion.
Because patients with such white matter lesions are free of specific symptoms and a biopsy may not lead to therapeutic consequences, many patients hesitate to undergo a biopsy for histologic assessment of a nonspecific incidental brain lesion (NIL) and prefer MRI follow-up. For better care of these patients, the prediction of the individual course would be desirable, but there are no data in the literature about the natural course and outcome of NILs.
The results of PET with the 18F-labeled amino acid fluoroethyl-l-tyrosine (18F-FET) and specific features on MRI have been shown to be useful prognostic tools in patients with histologically verified LGGs. LGGs with increased 18F-FET uptake on PET and a diffuse growth pattern on MRI indicate a poor prognosis and lead to rapid clinical deterioration because of early malignant transformation to high-grade gliomas (HGGs). In contrast, LGGs with normal or low 18F-FET uptake on PET and a circumscribed growth pattern on MRI indicate a good chance of long-term survival with a high quality of life because of slow progression and a lack of malignant transformation to HGGs for many years (6).
In this prospective cohort study, we evaluated the role of MRI and 18F-FET PET features as prognostic factors in the natural course of small NILs suggestive of LGGs.
MATERIALS AND METHODS
Patient Population
From 1999 on, simultaneous MRI and 18F-FET PET scans were performed in 195 patients with newly diagnosed and untreated brain lesions. The study was approved by the Heinrich Heine University Ethics Committee and federal authorities. All subjects gave written informed consent for their participation in the study. A total of 162 symptomatic patients with nonincidental lesions (diagnosed after seizure, focal neurologic deficit, or increased intracranial pressure) were excluded from the study. Eligible patients had incidental findings in the cerebral lobes, with a hypointense signal on T1-weighted images but no signs of blood–brain barrier disruption after the administration of gadolinium–diethylenetriaminepentaacetic acid (Gd-DTPA) (no enhancement), and a hyperintense signal on T2-weighted images. The lesions were not space occupying and were small, with a maximum volume of 10 mL for circumscribed lesions or a maximum diameter of 30 mm for diffuse lesions. On the basis of neuroradiologic MRI patterns, LGG was the initial differential diagnosis.
All other possible differential diagnoses for a nonspecific, nonenhancing intracerebral lesion, such as a posttraumatic lesion, a local infection or inflammation, a demyelinating plaque in multiple sclerosis, ischemia, or infarction, were ruled out in all patients by a complete check of patient history, physical and neurologic status, genetic investigations, laboratory and microbiologic investigations of blood and cerebrospinal fluid samples, testing of cerebrospinal fluid pressure during lumbar puncture, electroencephalography, funduscopy of the eyes, and cardiac and cerebrovascular investigations. A screening for neurofibromatosis (NF) was done, because as many as 20% of patients with NF harbor asymptomatic lesions suggestive of gliomas. Because of the generally benign biologic behavior of these lesions, most do not require a specific intervention (7,8). Therefore, patients with NF were also excluded from the study.
Finally, a group of 21 patients with nonspecific, incidental, and nonenhancing intracerebral lesions were included in the study. There were 15 female and 6 male patients. Their ages at the time of diagnosis ranged from 11 to 74 y, with a mean of 39.9 y and a median of 38 y. Karnofsky scale performance status was 100% in all of the patients. Detailed information on the individual patients is given in Table 1.
Patient Data
None of the patients had previous surgery, a biopsy, or any kind of cerebral treatment. The follow-up period ranged from 3 to 8.5 y. All lesions remained untreated until significant growth was detected. The initial imaging was performed as a research scan in 2 healthy volunteers and as a screening scan because of nonspecific symptoms in 19 patients, as follows. Five patients had complaints of chronic headaches, 4 patients had chronic dizziness, and 2 patients each had chronic migraines, chronic blurred vision, and chronic mental problems with antisocial behavior. A single episode of unexplained collapse in 2 patients and acute sudden deafness in 2 patients led to MRI investigations.
The relatively large number of NILs without a histologic diagnosis is explained by the selective referral of patients to the University of Düsseldorf. Since 1999, we have offered PET with 18F-FET to all patients with newly diagnosed, gliomatous, or unclear lesions on MRI to evaluate the diagnostic and prognostic power of this additional method in prospective studies (for study results, see Floeth et al. (6,9,11), Pauleit et al. (10), and Messing-Jünger et al. (12)).
Initial Imaging
All patients underwent evaluation of their lesions at our institution with MRI and 18F-FET PET on the same day according to a standard protocol within 4 wk after referral to our institution. The delay between the initial imaging outside our institution and the referral to our institution ranged from 1.2 to 5.5 mo, with a mean of 3.4 mo.
MRI
MRI was performed with a 1.5-T system (Sonata; Siemens). The imaging protocol consisted of a T1-weighted 3-dimensional magnetization-prepared rapid acquisition gradient-echo sequence (field of view, 25 cm; matrix, 205 × 256; repetition time, 2,200 ms; echo time, 3.9 ms; inversion time, 1,200 ms; flip angle, 15°; number of slices, 128; slice thickness, 1.5 mm; slice gap, 0 mm; number of averages, 1; length of acquisition, 6 min 38 s) before and 2 min after the injection of 20 mL of Gd-DTPA (Magnevist; Schering) and a T2-weighted transverse fluid-attenuated inversion recovery (FLAIR) sequence (field of view, 25 cm; matrix, 205 × 256; repetition time, 9,000 ms; echo time, 119 ms; inversion time, 2,500 ms; flip angle, 90°; number of slices, 25; slice thickness, 5 mm; slice gap, 0 mm; number of averages, 2; length of acquisition, 4 min 32 s).
MRI scans were assessed by a senior neuroradiologist and 2 experienced senior neurosurgeons according to the inclusion and exclusion criteria with regard to location, gadolinium enhancement, size (volume or diameter), mass shift, initial neuroradiologic diagnosis, and growth of the lesion on follow-up MRI scans. None of the lesions showed significant contrast enhancement after the injection of Gd-DTPA. On the basis of their appearance on MRI, the lesions were classified as circumscribed in 17 patients (81%) and diffuse in 4 patients (19%). Circumscribed lesions were characterized by a homogeneous structure and sharp borders that were identical on T1- and T2-weighted images. Diffuse lesions had a nonhomogeneous signal pattern and poorly defined borders on MRI. For these lesions, the extent of hyperintensity on T2-weighted images was generally larger than the area of hypointensity on T1-weighted images.
A reliable volumetric assessment was possible for circumscribed lesions with well-defined borders but not for diffuse lesions. For semiquantitative evaluation of diffuse lesions, size was estimated from the maximal cross-sectional diameter of the area of hypointensity on T1-weighted images respective to the area of hyperintensity on FLAIR images. Circumscribed lesions with a volume of ≤10 mL and diffuse lesions with a diameter of ≤30 mm were rated as small.
18F-FET PET
The labeled amino acid 18F-FET was produced by phase transfer–mediated nucleophilic 18F fluorination of N-trityl-O-(2-tosyloxyethyl)-l-tyrosine-tert-butyl ester and subsequent deprotection. The uncorrected radiochemical yield was about 35% at a specific radioactivity of greater than 200 GBq/μmol and a radiochemical purity of greater than 98% (13). The tracer was administered as an isotonic neutral solution. All patients fasted for at least 12 h before the PET studies. PET studies were acquired 15–40 min after the intravenous injection of 200 MBq of 18F-FET. The measurements were obtained in the 3-dimensional mode with an ECAT EXACT HR+ scanner (Siemens Medical Systems, Inc.) (32 rings; axial field of view, 15.5 cm). For attenuation correction, transmission scans with 3 68Ge/68Ga rotating line sources were obtained. After correction for random and scattered coincidences and dead time, image data were obtained by filtered backprojection in Fourier space with ECAT 7.2 software (direct inverse Fourier transformation; Shepp filter; full width at half maximum, 2.48 mm; pixel size, 2 × 2 × 2.4 mm3). The reconstructed images were decay corrected; the reconstructed image resolution was about 5.5 mm.
Presurgery MRI and 18F-FET PET were coregistered and evaluated by regions of interest (ROIs) with dedicated software (MPI tool, version 3.28; ATV). For lesions with increased 18F-FET uptake, the transaxial slice showing the highest tracer accumulation was chosen, and an isocontour region around the lesion maximum was drawn automatically at a cutoff of 3 SDs above average activity in the reference region. A larger reference ROI of variable size was placed in the normal brain tissue in the contralateral hemisphere, including white matter and gray matter. Because most of the lesions exhibited 18F-FET uptake similar to that of the normal brain, an objective positioning of ROIs on the PET scans on the basis of threshold values was impossible. Therefore, a singular irregular ROI was placed manually in the area of the signal abnormality on the T1- and T2-weighted transverse MRI scans and transferred to the coregistered 18F-FET PET scan in each case. Mean lesion-to-brain (L/B) ratios were calculated by dividing the mean ROI (Bq/mL) of the lesion by the mean ROI of the normal brain tissue on the 18F-FET PET scan.
In 2 previous biopsy-controlled studies of patients with newly diagnosed gliomas of all World Health Organization (WHO) grades, we found for tissue samples corresponding to normal and peritumoral tissues an L/B ratio for 18F-FET uptake of 1.2 ± 0.4 (mean ± SD), with a threshold of 1.5 separating glioma tissue from normal brain tissue (10,11). Therefore, in the present study, lesions with a mean L/B ratio for tracer uptake of ≤1.5 were judged as 18F-FET negative, and lesions with a mean L/B ratio of ≥1.6 were judged as 18F-FET positive.
Follow-up and Outcome
Clinical and radiologic follow-up with MRI was performed on a regular schedule at 4- to 6-mo intervals. The patients were screened for neurologic deterioration and for radiologic regression or progression of the lesion, measured as a change in the largest diameter of the lesion. Regression was defined as a decrease in lesion diameter of at least 30% during a follow-up period of at least 3 y. For shrinking lesions, follow-up including MRI was continued. For lesions with complete disappearance, additional follow-up including MRI was continued for 1 or 2 y, with at least 3 negative MR control scans, and only clinical follow-up was continued afterward. A stable course was defined as an unchanged lesion diameter within a range of maximum ± 30% during a follow-up period of at least 3 y. For stable lesions, follow-up including MRI will be continued indefinitely, with longer intervals after 5 y. Progression was defined as an increase in lesion diameter of at least 30% on follow-up MRI compared with initial MRI or contrast enhancement within the initially nonenhancing lesion. In cases of progression, there was strong evidence for a tumorous lesion (6 cases so far), and all patients underwent cytoreductive surgery. The cutoff for analysis of clinical and radiologic follow-up data was November 2007.
Histopathology
There was no initial cytologic assessment of the lesions. In cases of progression, open tumor resection with histologic investigation of the resected tissue was performed. The diagnoses were established from formalin-fixed and paraffin-embedded tissue samples according to the WHO classification of tumors of the nervous system (14). Additional immunohistochemical analyses were performed with antibodies against tumor suppressor protein p53 (clone D07; Dako; primary antibody dilution, 1:100) and proliferation-associated antigen Ki-67 (clone Mib1; Dako; primary antibody dilution, 1:200) according to standard protocols.
Statistical Analysis
Values are expressed as mean ± SD. Statistical methods used were t tests or Mann–Whitney rank sum tests for group comparisons. Probability values of less than 0.05 were considered significant.
RESULTS
The patients were classified into 4 outcome groups on the basis of the clinical and radiologic development of the lesions during the observation time. This classification revealed a clear relationship of the appearance of the lesion on the initial MRI scan and 18F-FET uptake and prognosis (Table 1).
Group A: Lesions That Have Regressed or Disappeared
In 5 patients (24%), the NILs regressed slowly over a period of 1 y (patient 2) or vanished completely within 3–6 mo (patients 1, 3, 4, and 5). An example is shown in Figure 2 (patient 5). The clinical and neurologic course was stable or improved in these 5 patients. All of these NILs were circumscribed on MRI and had negative 18F-FET PET results (mean L/B ratio: 1.2 ± 0.2; range: 1.0–1.4). The initial imaging was done as screening MRI because of nonspecific symptoms in 4 patients, and 1 patient had research MRI as a healthy volunteer.

Regression of NIL (red arrowhead) detected in young woman during screening MRI performed for chronic dizziness (patient 5). (A) Initial axial T2-weighted MR image (left) and sagittal T2-weighted FLAIR image (right) revealed right parietal lesion. (B) Corresponding PET scan demonstrated low 18F-FET uptake in lesion compared with that in surrounding tissue (L/B ratio: 1.4). (C) Ten months later, lesion had disappeared completely on MRI, and results of 2 further MRI scans were unremarkable.
Patient 1 had had an unexplained collapse 3 d after his first marathon run. A thromboembolic event attributable to unusual dehydration may have been the cause of the collapse and the NIL in this patient. Patient 3 had sudden deafness. The NIL in this patient vanished after 5 mo, and the patient recovered completely. Thirty months later, she developed deep-vein thrombosis, and protein S deficiency was diagnosed. Therefore, a thromboembolic event may have been the origin of the NIL in this patient. In the other patients, the clinical follow-up was unremarkable.
Group B: Lesions That Are Stable, Without Growth
In 10 patients (48%), the NILs were stable, without any significant growth or regression within a follow-up period of at least 3 y (patients 6–15). The clinical and neurologic course was stable or improved in all patients. All lesions were circumscribed on MRI and had negative 18F-FET PET results (mean L/B ratio: 1.0 ± 0.1; range: 0.8–1.0). The initial imaging was done as screening MRI because of nonspecific symptoms in 9 patients and as research MRI in 1 patient.
Group C: Lesions with Slow and Continuous Growth
In 2 patients (9%), the NILs showed continuous slow growth over years, with a concomitant stable clinical and neurologic course (patients 16 and 17). An astrocytoma of WHO grade II was diagnosed after resection in both patients. The lesions were circumscribed on MRI and had negative 18F-FET PET results (mean L/B ratios: 0.7 and 1.0). The initial imaging was done as screening MRI because of nonspecific symptoms in both patients. These 2 small NILs had an initial diameter of 2 cm, and follow-up MRI showed continuous slow growth, with an increase in the lesion diameter of 2–3 mm/y. The clinical course was unremarkable, without seizures or neurologic deficits. Because of the increasing lesion size, with final diameters of 4 and 5 cm after 6 y of observation, resection of the lesions in the still asymptomatic patients was performed.
Group D: Lesions with Sudden and Rapid Growth
After an initially stable clinical and radiologic course, 4 patients (19%) with NILs showed acute clinical deterioration, with concomitant sudden and rapid growth of the lesions (patients 18–21). A high-grade glioma of WHO grade III or IV was diagnosed after resection in all patients. The initial MRI showed diffuse lesions, and the 18F-FET PET results were positive. The mean L/B ratio in group D was significantly higher than those in group A and group B (mean L/B ratio: 2.0 ± 0.4; range: 1.6–2.4) (P < 0.01 for group D vs. group A or group B). A statistical comparison with group C was not applicable (only 2 patients). The initial imaging in all patients in group D was done as screening MRI because of nonspecific symptoms. Patient 18 presented with sudden deafness and recovered completely from deafness. MRI revealed an 18F-FET–positive diffuse NIL that remained unchanged on MRI for 3 y. After 3.5 y, the patient developed rapidly progressive hemiparesis, and an anaplastic astrocytoma of WHO grade III was diagnosed. Patient 19 had chronic dizziness for more than 10 y. The 18F-FET–positive diffuse NIL remained unchanged on MRI for 1 y. After 1.3 y, the patient developed left-side hemiparesis, and a glioblastoma of WHO grade IV was detected. Patient 20 had chronic migraines for more than 15 y. The 18F-FET–positive diffuse NIL remained stable on MRI for 1 y. After 1.3 y, the patient developed rapidly progressive aphasia, and a glioblastoma of WHO grade IV was diagnosed. Patient 21 had chronic headaches for 3.5 y. MRI revealed a right frontal diffuse NIL with significant 18F-FET uptake (L/B ratio: 2.4) on PET. The MRI and PET scans for this patient are shown in Figure 3. Two months after initial imaging, the patient developed rapidly progressive left-side hemiparesis. The MRI scan demonstrated sudden growth of the tumor, ring enhancement, and central necrosis. Resection yielded a glioblastoma of WHO grade IV.

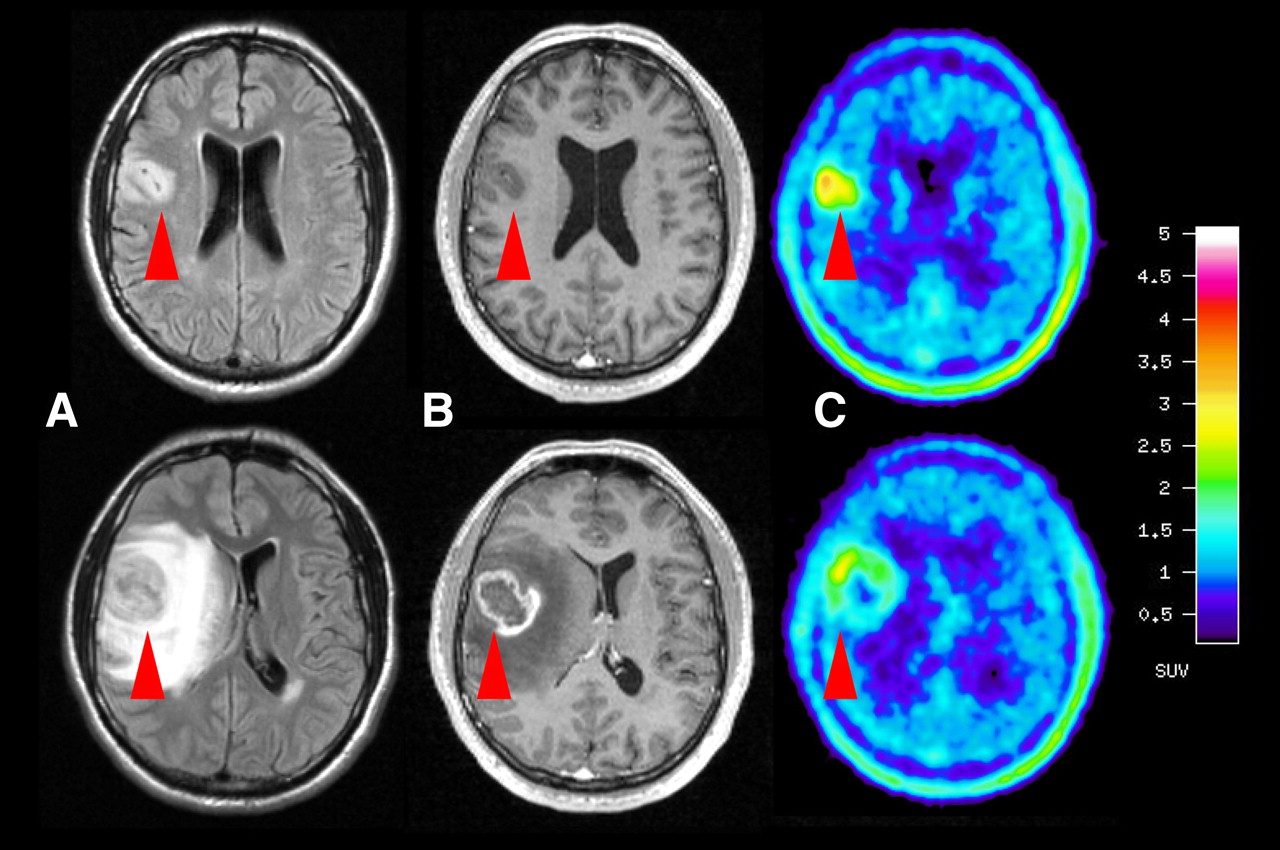
Progression of NIL (red arrowhead) diagnosed in young man during screening MRI performed for chronic headaches (patient 21). (Upper row) Initial axial T2-weighted (A) and contrast-enhanced axial T1-weighted (B) MR images revealed nonenhancing intracerebral left frontal lesion. (C) PET scan demonstrated increased 18F-FET uptake (L/B ratio: 2.4). (Lower row) Only 2 mo later, patient demonstrated severe clinical deterioration. T2-weighted (A) and contrast-enhanced T1-weighted (B) MR images revealed massive growth with ring enhancement, central necrosis, and strong perifocal edema. (C) PET scan demonstrated increased 18F-FET uptake corresponding to contrast enhancement on MRI (L/B ratio: 2.5). Subsequent tumor resection confirmed suspected diagnosis of glioblastoma of WHO grade IV.
DISCUSSION
Incidental findings on brain MRI are defined as previously undetected abnormalities of potential clinical relevance that are unexpectedly discovered and unrelated to the purpose of the examination. The incidence of such findings reaches 15%–20% for brain anomalies or variants of the norm without any clinical significance, such as cavum vergae, and ranges from 2%–8% for potentially clinically significant neuropathologies, such as pineal cysts, with the need for routine neurosurgical referral. Finally, 1%–2% of incidental findings are of urgent clinical significance, such as a tumorous mass, a vascular disorder, or a Chiari I malformation, with the possible need for medical or surgical intervention (15–19). Most of these incidentalomas can be identified by neuroradiologic criteria as meningiomas, pituitary adenomas, arteriovenous malformations, or even aneurysms, and treatment can be offered according to the present guidelines for these entities. Incidental gliomas are very rare, and their diagnosis can be very challenging, especially for small lesions, because of their nonspecific signal pattern on MRI. Moreover, there are no treatment guidelines for asymptomatic gliomas because there is no evidence that early treatment of diffusely infiltrating gliomas is beneficial for patient outcome (15).
There has been a broad discussion about the ethical aspects of incidental findings; in particular, Illes et al. have contributed to this issue (16,18,19). The devastating impact of an incidental finding with regard to psychologic, insurance, financial, and social aspects has been described in a letter of a neuroscientist who wanted to “observe MRI scans of his own brain” and in whom a brain tumor was diagnosed (20).
The development of noninvasive diagnostic tools for risk stratification in such cases is highly desirable. The prevalence of incidental MRI findings in asymptomatic healthy volunteers in brain research or screening investigations is dependent on sex (the percentage of findings in men is usually twice that in women), age (the percentage of findings clearly increases with age), and study population. Several large studies of different populations have demonstrated that asymptomatic gliomas or lesions suggestive of gliomas are rarely identified on MRI examinations, with average prevalences of 0.1%–0.2% for histologically verified LGGs and 1%–2% for nonspecific, nonenhancing white matter lesions with a differential diagnosis of diffuse LGGs (1–5).
LGGs and 18F-FET PET
For LGGs, meaningful data are available regarding the natural course, including growth patterns and kinetics, prognostic factors, and outcome (21–33). Nevertheless, the natural course of disease in individual patients is not yet predictable, and the treatment strategy remains controversial (23,25). PET with radiolabeled amino acids such as [11C-methyl]-l-methionine (11C-MET) demonstrated a variable uptake pattern in LGGs (34), and low 11C-MET uptake before treatment was found to be an important prognostic factor in these tumors (35). The use of 11C-MET, however, is restricted to a few centers because of the short physical half-life of the 11C label (20 min). In contrast, the labeled amino acid 18F-FET fulfills all requirements for a widespread clinical application, that is, efficient radiosynthesis, 18F labeling with a 109-min half-life, in vivo stability, and ideal tracer kinetics for brain tumor imaging (36,37). Several studies have demonstrated the diagnostic and prognostic aspects of 18F-FET PET for gliomas (9–12,38,39). Recently, a prospective study showed that LGGs with increased 18F-FET uptake on PET and a diffuse growth pattern on MRI had a grim prognosis, with a short life expectancy, because of rapid progression and malignant transformation to HGGs within only 2–3 y. In contrast, LGGs with normal or low 18F-FET uptake on PET and a circumscribed growth pattern on MRI had a fair prognosis, with slow progression and a lack of malignant transformation to HGGs within the first 5 y after diagnosis (6).
NILs Suggestive of LGGs and 18F-FET PET
In contrast to data for histologically confirmed LGGs, few data are available in the literature concerning the natural course of NILs. It is unclear whether an early biopsy or clinical and radiologic observation is the preferable treatment strategy for such lesions. To the best of our knowledge, this is the first prospective long-term study with a systematic evaluation of prognostic factors and outcome for NILs suggestive of LGGs.
The results of this preliminary study indicate 2 major factors with predictive value for the natural course and outcome of NIL: the morphologic features on MRI (circumscribed lesion vs. diffuse lesion) and amino acid uptake measured by 18F-FET PET. All 17 circumscribed and 18F-FET–negative lesions had a benign course, and follow-up with MRI at 4- to 6-mo intervals with clinical evaluation was adequate for monitoring. Most of these “benign” lesions were stable, regressed, or vanished within 1 y after the initial diagnosis. Only 2 lesions grew slowly and, finally, LGGs were diagnosed after surgical intervention. These data support a conservative strategy without biopsy for circumscribed and 18F-FET–negative small NILs.
In contrast, none of the 4 diffuse and 18F-FET–positive lesions (Fig. 3) had a benign course. All 4 led to sudden and dramatic clinical deterioration and showed progression on follow-up MRI examinations. The characteristic feature of these lesions was the absolutely stable clinical and radiologic course with an unchanged lesion on follow-up MRI for months, followed by sudden and rapid clinical deterioration and a sudden change on MRI. There was no slow growth, like that of typical LGGs. This small subgroup of lesions “went out of control,” and 3 of the 4 patients died because of a glioblastoma during the observation time. Obviously, a strategy of “wait and see” with MRI scans at 4- to 6-mo intervals is not an appropriate strategy for such lesions. An early biopsy should be attempted to establish a histopathologic diagnosis, and early aggressive treatment should be considered. Nevertheless, it remains to be demonstrated that tissue changes and changes in cellularity at this early stage will allow for a proper tumor diagnosis. Moreover, it remains unclear whether early treatment of such lesions may delay malignant progression because there is still no evidence that early treatment of histologically proven gliomas improves the overall prognosis. These rare entities are a dilemma, and further studies are needed to evaluate the impact of surgery, radiation, and chemotherapy on these high-risk, early-stage gliomatous lesions. If no biopsy can be achieved, then follow-up of such lesions at shorter intervals (2 or 3 mo) is recommended.
The conclusions drawn from the present study must be considered with caution because the number of patients studied was small because of the low incidence of LGGs. Furthermore, we cannot exclude the possibility that some of the lesions that remained stable during the observation time may progress at a later stage and convert to malignant tumors. Usually, however, untreated LGGs exhibit a constant growth rate of a few millimeters per year during their premalignant phase (24). These observations are in accordance with the growth kinetics of the 2 lesions that were determined to be LGGs in the present study: within the follow-up period of more than 5 y, both lesions showed continuous expansion of 2–3 mm per year until resection. Because the pattern of a circumscribed lesion versus a diffuse lesion on MRI alone may be a strong predictor of outcome, one may conclude that the additional effort of amino acid PET may be unnecessary. A recent study, however, demonstrated that circumscribed LGGs on MRI with increased 18F-FET uptake had a significantly worse prognosis than circumscribed LGGs without 18F-FET uptake (6). Therefore, at present, the combination of MRI and 18F-FET PET appears to be the most powerful approach for obtaining reliable prognostic information for NILs.
CONCLUSION
Our data suggest that assessment with the combination of MRI and 18F-FET PET provides a better prediction of course and outcome for small NILs with a differential diagnosis of LGGs. A circumscribed growth pattern on MRI and normal or low 18F-FET uptake on PET were strong predictors of a benign course, with the eventual development of an LGG. Because of the benign course of such lesions, an early biopsy for histologic assessment does not appear to be mandatory.
In contrast, a diffuse growth pattern on MRI and increased 18F-FET uptake on PET were strong predictors of a highly malignant course with a poor outcome. After a short, stable interval of approximately 1 y, all of these lesions showed malignant transformation to HGGs. An early biopsy, shorter MRI follow-up intervals, and early aggressive therapy appear to be necessary for these rare but devastating lesions.
Acknowledgments
The authors thank Suzanne Schaden, Elisabeth Theelen, and Barbara Elghahwagi for assistance in the participant studies and Sascha Rehbein, Silke Grafmüller, and Erika Wabbals for the radiosynthesis of 18F-FET. This work was supported by the Brain Imaging Center West (BICW) and a grant from the Deutsche Krebshilfe (70-3088-Sa I). The facility for magnetic resonance imaging at the Research Center Jülich was supported by the Bundesministerium für Bildung und Forschung (grant BMBF 01GO0104).
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication December 17, 2007.
- Accepted for publication January 24, 2008.





{kind=link}
{kind=link}
{kind=link}