


Abstract
Our objective was to evaluate the role of 99mTc-pertechnetate scintigraphy on microvascular autologous transplantation of the submandibular gland in patients with severe keratoconjunctivitis sicca (KCS). Methods: 99mTc-Pertechnetate scintigraphy was performed on 106 patients with severe KCS. The patients were examined before surgery and at 1 wk and 3 mo afterward using a standardized protocol that included static scintigrams, time–activity curves, and delayed scintigrams to check the function and secretion of the major salivary glands. The scintigraphic findings were assessed visually. When possible, the scintigraphic findings were compared with the clinical appearance of the transplanted gland. Results: The function of all 4 major salivary glands was almost completely lost in 10 patients, indicating that these patients were not suitable for transplantation. The other 96 patients were treated by autologous transplantation of the submandibular gland. In 14 patients, the function of the major salivary glands was below normal. One patient's scintigram, obtained on the second day after surgery, showed no uptake of 99mTc-pertechnetate in the transplanted gland. Surgical exploration showed embolism of the artery of the transplanted gland. Scintigraphy was performed 1 wk after surgery in 90 patients. There was no uptake of 99mTc-pertechnetate in the temporal region in 8 patients, indicating that the glands were not revascularized. Scintigraphy showed obvious uptake of 99mTc-pertechnetate in the temporal region of the other 82 patients, indicating that the transplanted glands were viable. At more than 3 mo after surgery, scintigraphy was again performed on 30 patients. Scintigraphy after a 120-min delay showed that 99mTc-pertechnetate drained into the orbit through the duct of the transplanted gland in 26 patients. However, no secretion into the orbit was found in 4 patients, indicating obstruction of the duct. Conclusion: Scintigraphy plays an important role in microvascular autologous transplantation of the submandibular gland in patients with severe KCS. Scintigraphy can be used to select patients and donor glands, to evaluate the viability of the graft, and to check the patency of Wharton's duct of the transplanted gland.
Keratoconjunctivitis sicca (KCS) is a relatively common disease (1), the severe form of which had no effective treatment before the advent of microvascular autologous transplantation of the submandibular gland. Submandibular gland transplantation with insertion of Wharton's duct into the upper conjunctival fornix offers an alternative to artificial tears and prevents the damage to the cornea caused by KCS (2). Murube-del-Castillo's original work was followed by experience by others (3–7). Initially, the principles of treatment were studied in an experimental model (8). Then, since 1999, a cohort of 96 patients (the largest reported series) with severe KCS has been treated by this technique. Scintigraphy with 99mTc-pertechnetate was performed before and after surgery. In successful cases, the symptom of dry eye was relieved. The patients could stop using artificial tears (9). This paper evaluates the role of scintigraphy in microvascular autologous transplantation of the submandibular gland in patients with severe KCS.
MATERIALS AND METHODS
Patient Recruitment
From 1999 to 2005, 106 patients with severe KCS were referred for assessment to the Department of Oral and Maxillofacial Surgery at Peking University School and Hospital of Stomatology. The Ethical Committee for Human Experiments of Peking University approved the study. The study was prospective, and consecutive patients with KCS were enrolled in the study after giving informed consent to participate. As a prerequisite for study entry, patients underwent salivary scintigraphy and assessment of salivary flow (whole-mouth unstimulated saliva in 5 min). Patients with inadequate salivary function (n = 10) were excluded. Of the remaining cohort of 96 patients, 46 were male and 50 were female, with a median age of 35 y (range, 10–60 y). Ninety-three patients underwent unilateral and 3 patients bilateral transplantation.
Scintigraphic Method
Before and after surgery, each patient underwent scintigraphy using a standardized protocol. The patient was positioned supine under the γ-camera (Starcam 4000 I; GE Healthcare), and a low-energy, high-resolution, parallel-hole collimator was centered over the face. Immediately after intravenous injection of 185 MBq of 99mTc-pertechnetate, sequential 1-min images were acquired for 40 min. The static scintigrams were obtained with a ×1.33 zoom in a 256 × 256 matrix. After 20 min, approximately 0.5 mL of citric acid was applied to accelerate salivary secretion. Digital data on uptake secretion of pertechnetate were collected simultaneously by an online computer system. Time–activity curves were calculated using manually drawn oval regions of interest around both submandibular glands.
One week after surgery, static scintigrams in lateral and anterior views were obtained to visualize tracer uptake in the transplanted submandibular gland. Sequential images were obtained to show the reaction of the transplanted gland to citric acid stimulation. In 30 patients, imaging was repeated at more than 3 mo after surgery, with delayed scintigrams (120–180 min) obtained to visualize tracer uptake in the secretory duct of the transplanted submandibular gland or secretion into the eye (10).
Scintigraphic Analysis
The scintigrams were assessed visually (11).
Saliva-Sampling Method
All patients were asked to refrain from eating, drinking, brushing the teeth, and using tobacco for at least 1 h before saliva collection, which took place between 9:00 and 11:00 am. Unstimulated saliva was collected when the participant was positioned in a relaxed position leaning slightly forward. After clearing the mouth by swallowing, saliva was drooled for 5 min into a sterilized plastic tube, which was weighted beforehand and quantified by electronic balance. Then, the salivary flow rate was calculated by the following formula and recorded as mg/min: salivary flow rate = (weight of the tube with collected saliva – weight of the empty tube)/5 min.
RESULTS
Preoperative Scintigraphic Findings
At the initial assessment, the function of all 4 major salivary glands was normal in 82 patients (unstimulated salivary flow rate, 0.594 ± 0.432 mg/min) (Fig. 1). In the other 14 patients, the function of 1 or 2 major salivary glands was abnormal, but the total salivary flow rate was still within the normal range (unstimulated salivary flow rate, 0.323 ± 0.201 mg/min) and the operation succeeded. When 1 submandibular gland was hypofunctional (n = 8), this gland was selected as the donor gland for microvascular transplantation. The function of all 4 major salivary glands was almost completely lost in 10 patients (unstimulated salivary flow rate, <0.01 mg/min) (Fig. 2), indicating that the glands were not suitable for transplantation.

Scintigram showing normally functioning parotid and submandibular glands.

Scintigram showing seriously damaged functioning of all parotid and submandibular glands, indicating that they are not suitable for transplantation.
Perioperative Scintigraphic Findings
A series of scintigraphic images showed that uptake of 99mTc-pertechnetate in normal and transplanted submandibular glands increased gradually during the first 20 min. About 0.5 mL of citric acid was applied at 20 min to stimulate secretion. The quantity of 99mTc-pertechnetate in normal glands decreased promptly and increased again 3–5 min later. However, uptake of 99mTc-pertechnetate in denervated transplanted glands increased slowly and steadily during the first 30 min and was not influenced by acid stimulation. The same result was shown on the time–activity curves (Fig. 3).

Scintigraphy series showing 99mTc-pertechnetate uptake by normal and transplanted (arrowheads) submandibular glands. About 0.5 mL of citric acid was applied at 20 min to stimulate salivary secretion.
In one patient on the second postoperative day, the temporal region showed obvious swelling and the transplanted gland was hard. Thrombosis was suspected and scintigraphy was performed. The findings showed no uptake of 99mTc-pertechnetate in the operated temporal region. Subsequent surgery showed that the transplanted gland was purple. Both the artery and the vein of the gland were obstructed.
Postoperative Scintigraphic Findings
At 1 Week.
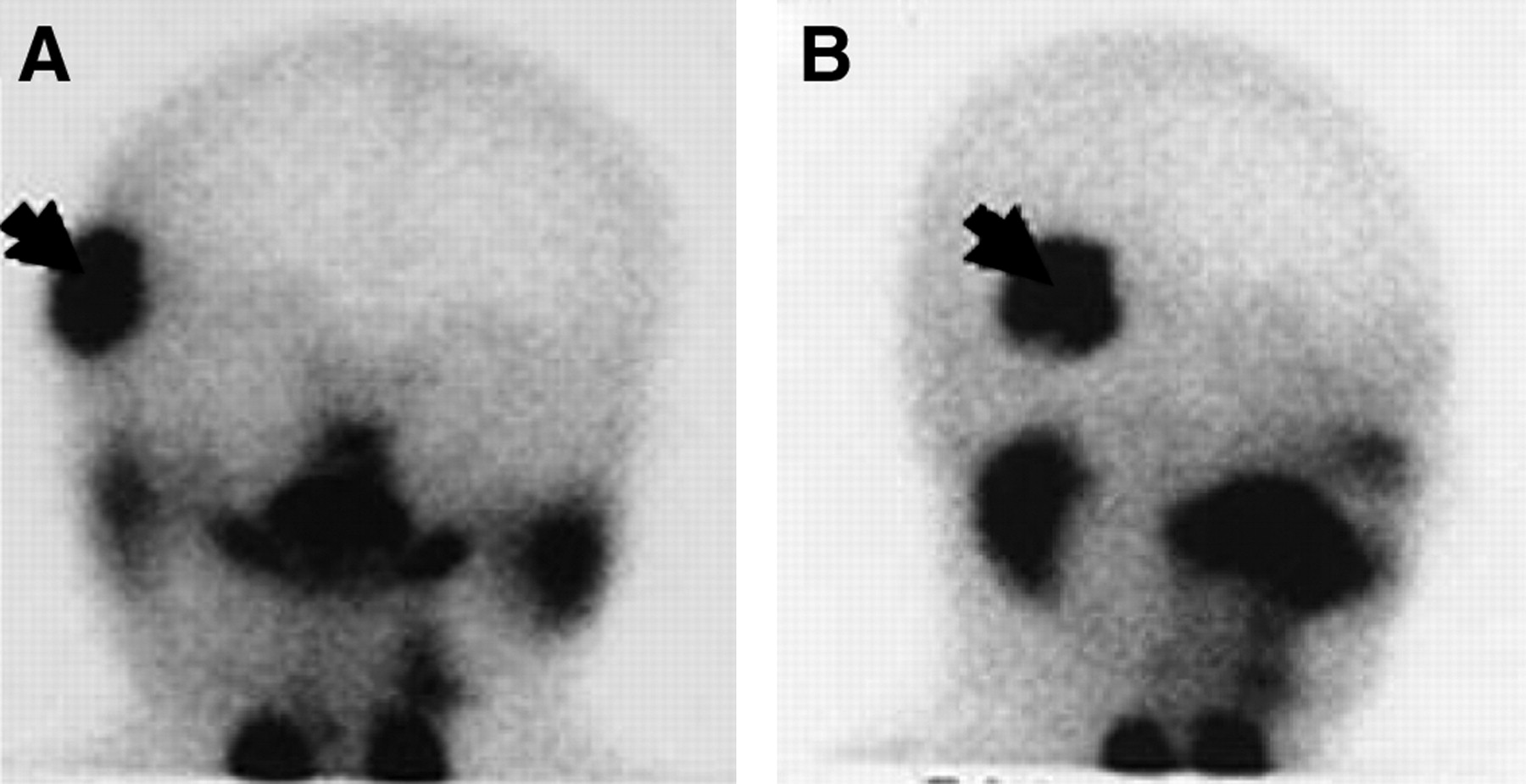
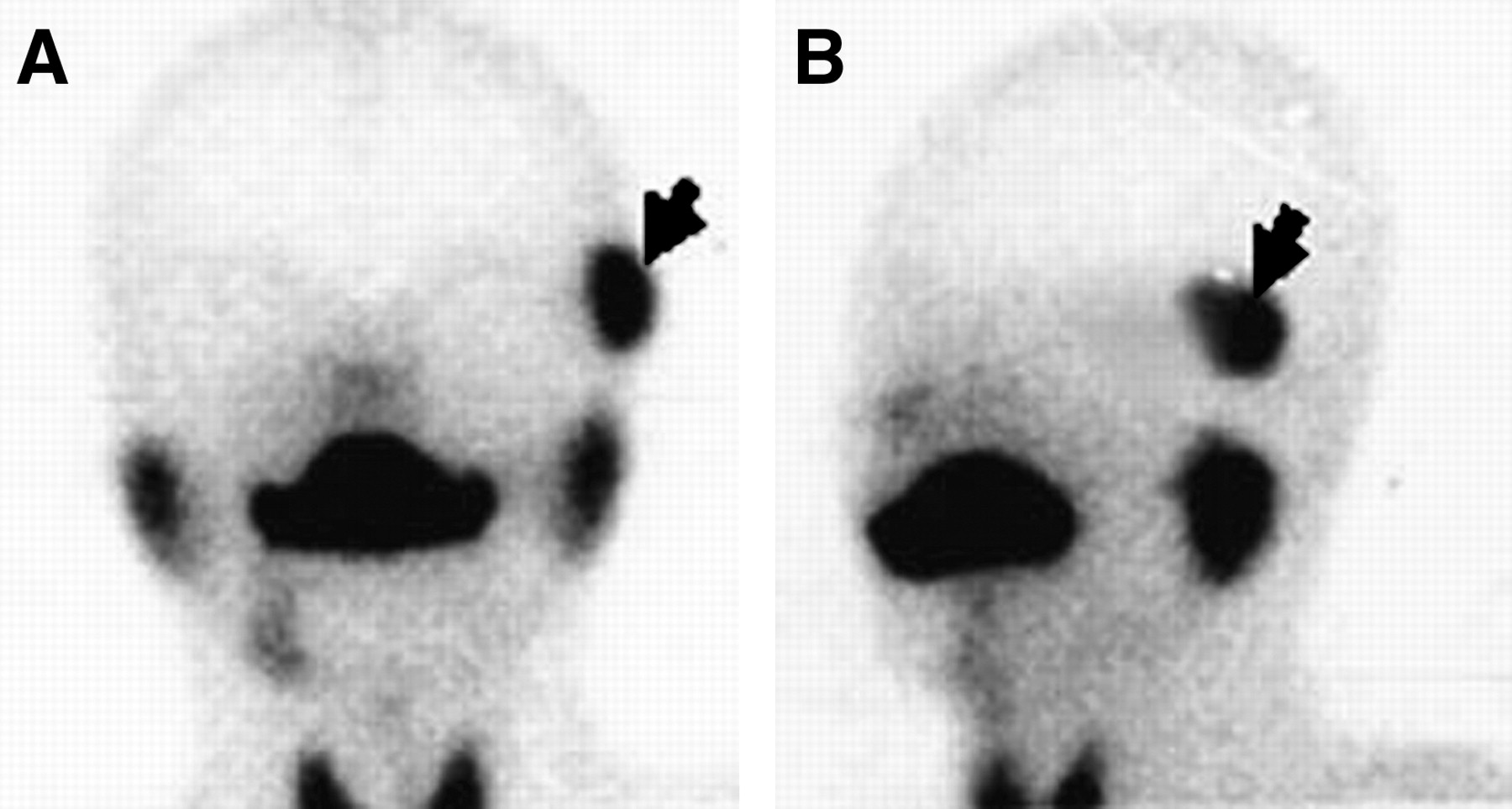
At 1 wk after surgery, scintigrams (n = 90) showed significant tracer uptake in the temporal region in 82 patients (Fig. 4), but in 8 patients there was no uptake, demonstrating nonvascularization of the transplant. We found that thrombosis of the blood vessels had caused macroscopic necrosis of the transplanted glands, which had to be removed (Fig. 5).
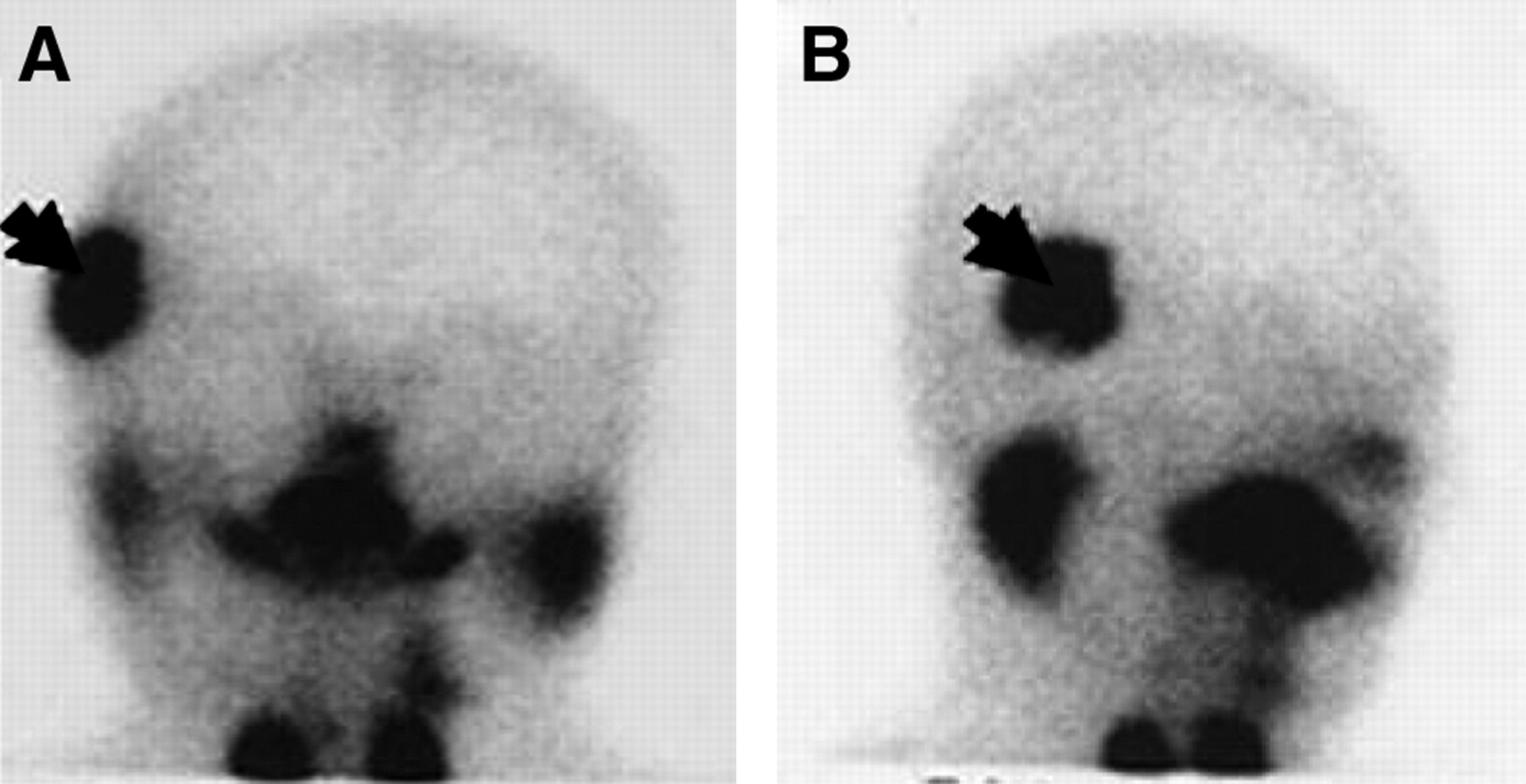
Anterior (A) and lateral (B) scintigrams showing significant 99mTc-pertechnetate uptake in temporal region, indicating that transplanted gland (arrow) is revascularized and viable.

Anterior (A) and lateral (B) scintigrams showing no uptake of 99mTc-pertechnetate in temporal region, suggesting that transplanted gland (arrowhead) is not revascularized.
At More Than 3 Months.
At more than 3 mo after surgery, 120- to 180-min delayed scintigrams (n = 30) showed in 26 patients drainage of pertechnetate into the orbit through Wharton's duct (Fig. 6) and in some cases into the nasolacrimal duct and finally into the nasal cavity. This finding was often observed on static imaging performed at intervals of up to 2 h after administration of 99mTc-pertechnetate. The symptom of dry eye was relieved in these 26 patients. Four patients showed no secretion, indicating obstruction of Wharton's duct (Fig. 7). These 4 patients retained the symptom of dry eye. In 2 of them, the ducts were refashioned with a venous graft, and eventually the symptom of dry eye was relieved.
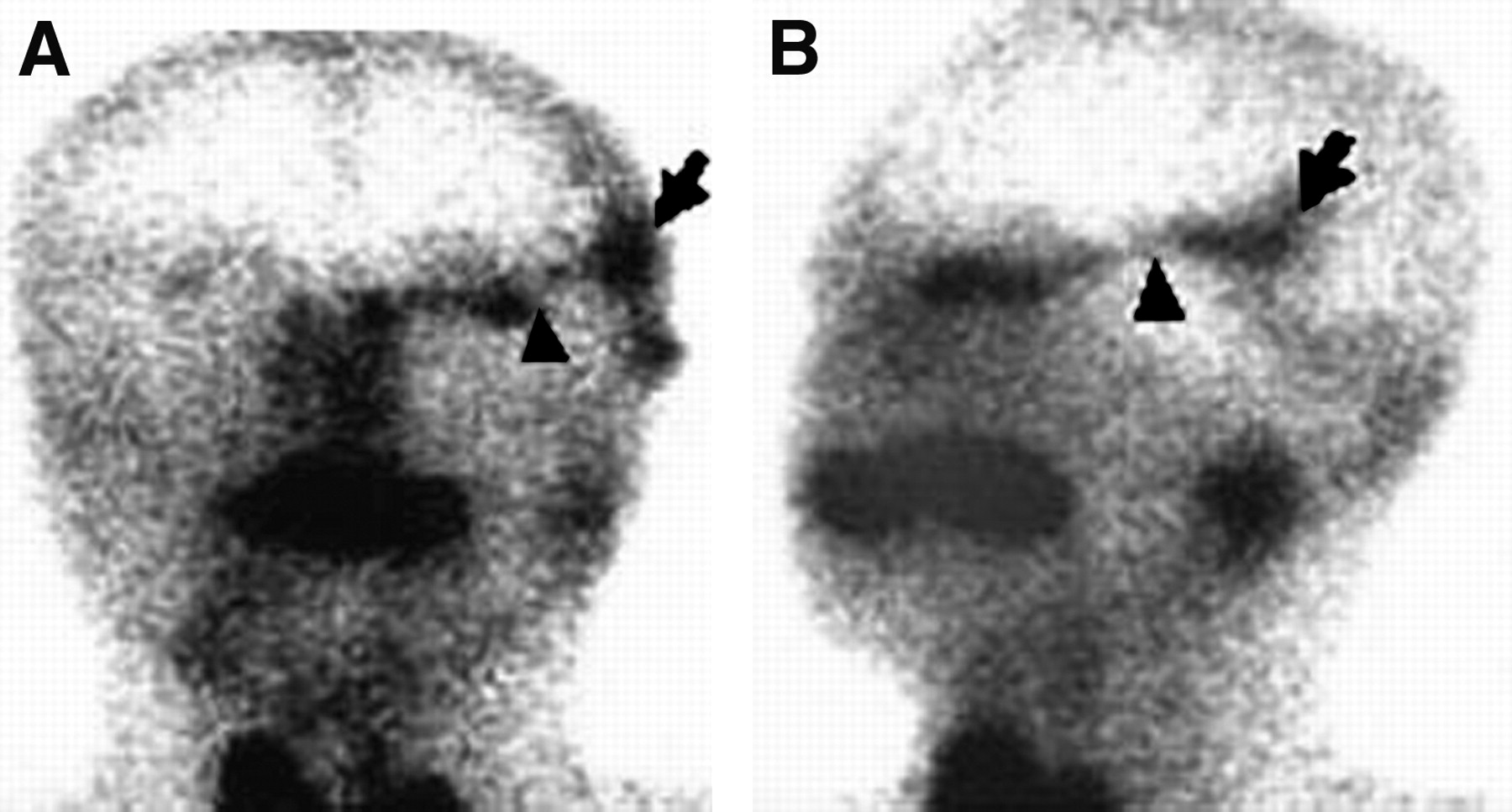
Anterior (A) and lateral (B) 180-min delayed scintigrams showing drainage of 99mTc-pertechnetate into orbit through Wharton's duct (arrowhead) of transplanted gland (arrow).
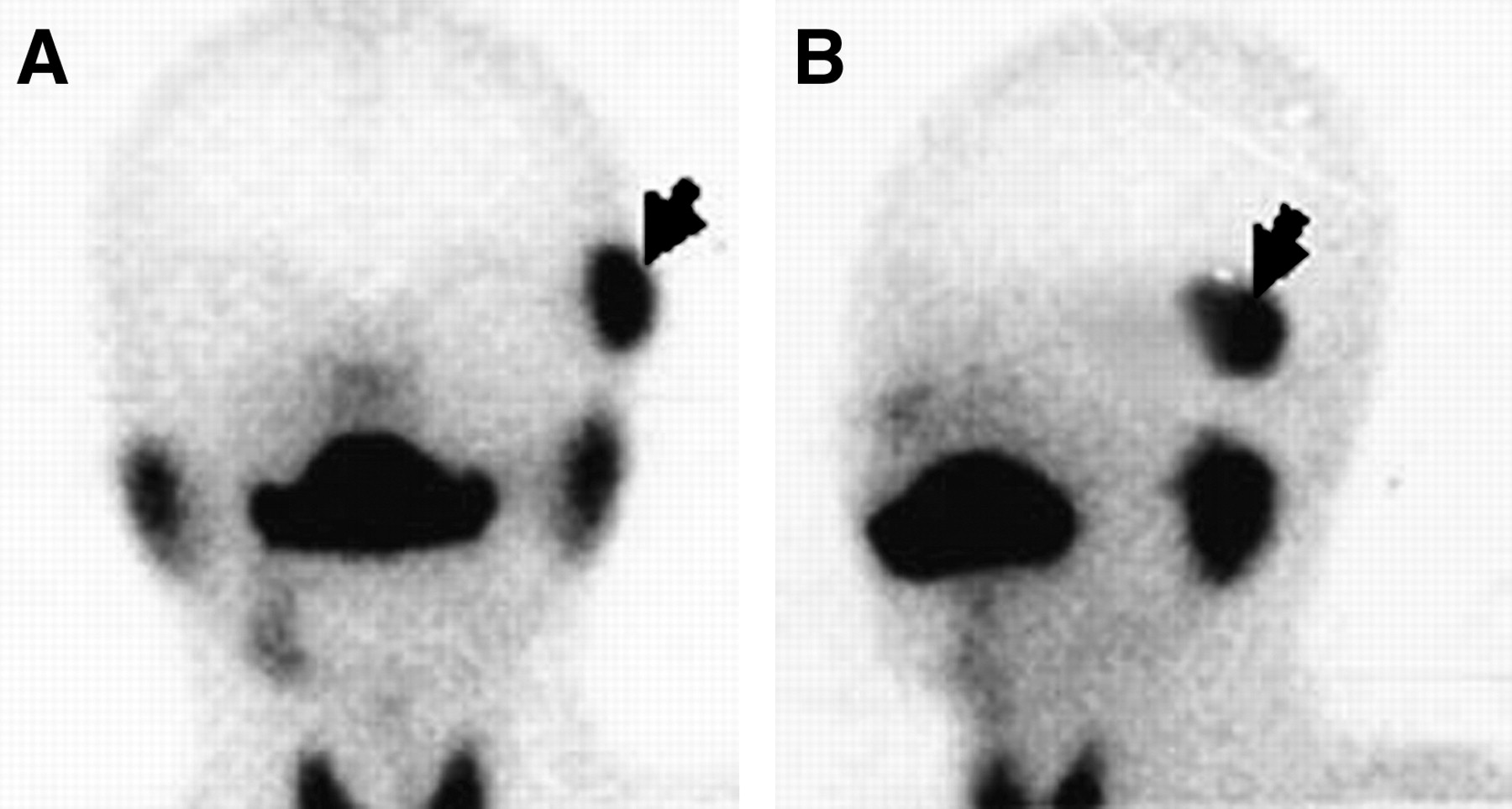
Anterior (A) and lateral (B) 120-min delayed scintigrams showing no secretion in orbit, indicating obstruction of Wharton's duct of transplanted gland (arrow) (more than 3 mo after operation).
DISCUSSION
The principle governing this technique is that basal secretion from a revascularized autologous submandibular gland can be used as an adequate substitute for natural tears (4,5,9). Patients with severely limited submandibular gland secretion because of underlying Sjögren's syndrome were excluded from the study. Experience has shown the importance of assessing salivary function before surgery to prevent complaints of postoperative xerostomia and inadequate graft function (9,12). Scintigraphy with 99mTc-pertechnetate has proven effective for evaluating the function of the major salivary glands. The procedure is also relatively easy, noninvasive, and well tolerated (13).
If the scintigrams showed mild or moderate uptake of tracer and the rate of saliva flow was normal, unilateral transplantation did not result in xerostomia. Although, to avoid xerostomia, bilateral transplantation was not performed, studies of allograft substitutes in these types of patients are ongoing (14).
Our experience shows that even submandibular glands with reduced function can relieve the symptom of dry eye. In addition, epiphora may result if a normally secreting submandibular gland is transplanted (9,15). Therefore, preoperative scintigraphy is an important step toward selecting an appropriate donor submandibular gland. Hypofunctional submandibular glands may avoid epiphora and reduce the risk of xerostomia.
Because transplanted glands are not visible beneath the temporal skin, it is difficult to judge whether the microvascular graft has failed early after surgery. A failure to take up 99mTc-pertechnetate suggests that the gland is not revascularized. In contrast, significant tracer uptake confirms that the transplanted submandibular gland is viable (13).
Hans et al. (12) found that scintigraphy was useful for assessing the patency of the salivary gland duct, and scintigraphy was used for that purpose in the present study. Normally, a 120- to 180-min delayed image shows drainage of 99mTc-pertechnetate into the orbit through Wharton's duct and subsequently into the nasolacrimal duct and finally into the nasal cavity. In 4 of our patients, the symptom of dry eye remained despite obvious uptake of tracer into the temporal region, indicating obstruction of Wharton's duct. For patients with complete obstruction of the duct, reconstruction of the duct with a venous graft is the treatment of choice (9).
It is well known that secretion of the salivary gland is controlled by parasympathetic nerves. In series imaging, the quantity of 99mTc-pertechnetate in the normal major salivary glands decreased promptly when citric acid was applied to stimulate secretion. However, uptake of 99mTc-pertechnetate in the transplanted gland was not influenced by acid stimulation and increased slowly and steadily. The finding indicated denervation of the transplanted submandibular gland and a change in its mechanism of secretion.
CONCLUSION
Scintigraphy can be used to select both patients and donor submandibular glands suitable for transplantation, to assess the viability of the graft, and to show whether the duct is patent more than 3 mo after surgery. Therefore, scintigraphy does play an important role in microvascular autologous transplantation of the submandibular gland in patients with severe KCS.
Acknowledgments
This study was supported by the National Natural Science Foundation of China (grants 30371545 and 30640093), the Ministry of Education (grant 104002), the Ministry of Science and Technology (grant 2003CCC00800), and the Beijing Board of Health (grant 2005–2009). The authors are grateful to Professor Mark McGurk and Dr. Eddie C.K. Yau for their revision of the manuscript.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication October 30, 2006.
- Accepted for publication May 31, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}