


Abstract
Revascularization of viable myocardial segments has been shown to improve left ventricular (LV) function and long-term prognosis; however, the surgical risk is comparatively higher in patients with a low ejection fraction (EF). We compared contrast-enhanced MRI with 18F-FDG PET/201Tl SPECT for myocardial viability and prediction of early functional outcome in patients with chronic coronary artery disease (CAD). Methods: Forty-one patients with chronic CAD and LV dysfunction (mean age ± SD, 66 ± 10 y; 32 men; mean EF ± SD, 38% ± 13%) referred for 18F-FDG PET, 201Tl-SPECT and MRI within 2 wk were included. Twenty-nine subjects underwent coronary artery bypass grafting (CABG), and LV function was reassessed by MRI before discharge (17 ± 7 d after surgery). Two were excluded from outcome analysis (1 death due to sepsis; 1 perioperative myocardial infarction). The extent of viable myocardium by 18F-FDG PET/201Tl SPECT was defined by the metabolism–perfusion mismatch or ischemia, in comparison with the extent of delayed enhancement (DE) on MRI in a 17-segment model. Segmental functional recovery was defined as improvement in the wall motion score of ≥1 on a 4-point scale. EF and LV volume change were used as global functional outcome. Results: Three hundred ninety-four dysfunctional segments were compared, and the extent of DE on MRI correlated negatively with the viability on 18F-FDG PET. Of 252 dysfunctional segments that were successfully revascularized, the sensitivity, specificity, positive predictive value, and negative predictive value of PET/SPECT were 60.2%, 98.7%, 76.6%, and 96.7% and of MRI were 92.2%, 44.9%, 72.4%, and 78.6% using the cutoff value of 50% DE on MRI, without significant differences in overall accuracies. In 18 subjects who underwent isolated CABG, improvement of EF (≥5%) and reverse LV remodeling (≥10% LV size reduction) was best predicted by the no DE on MRI, and patients with substantial nonviable myocardium on 18F-FDG/SPECT predicted a poor early functional outcome (all P < 0.001). Conclusion: Accurate prediction of early functional outcome by PET/SPECT and contrast-enhanced MRI is possible.
- cardiovascular magnetic resonance
- 18F-FDG
- myocardial viability
- surgical revascularization
- cardiac function
Assessment of myocardial viability in patents with chronic coronary artery disease (CAD) and left ventricular (LV) dysfunction is of great clinical importance. Although surgical risk is increased in such patients, surgical revascularization has been shown to improve LV function and prognosis (1–3). However, not all patients with ischemic cardiomyopathy recover in function after successful revascularization, despite the presence of viable myocardium identified using various noninvasive imaging techniques (4–10). The functional outcome and temporal variations could reflect the pathophysiologic mechanism of the dysfunction (11,12). Patients with early functional recovery could have a shorter hospital stay, a lower early postoperative morbidity and mortality, and, possibly, a better long-term functional outcome. Combined flow and 18F-FDG PET has been shown to be a good predictor of functional recovery after revascularization (13). Recently, MRI has been considered to accurately assess the cardiac function, viability, and perfusion in 1 examination (14–17). However, there is limited information on viability detected by 18F-FDG PET or contrast-enhanced MRI in the prediction of early function outcome after surgical revascularization. We hypothesized that differences between contrast-enhanced MRI and 18F-FDG PET/201Tl SPECT tissue characterization of myocardium might be related to both the recovery and nonrecovery of function and the rate of recovery of function after surgical revascularization and, furthermore, that the combination of MRI and nuclear techniques could be incrementally beneficial for predicting segmental functional recovery.
MATERIALS AND METHODS
Subjects
Patients included in this retrospective study were referred for 18F-FDG PET from March 2004 to July 2006 and presented with chronic ischemic heart disease and New York Heart Association (NYHA) functional class of ≥II, LV ejection fraction (LVEF) of ≤50%, and regional wall motion abnormalities on resting echocardiography. Patients who had 18F-FDG PET, stress–reinjection or rest–redistribution 201Tl SPECT, and MRI studies within 2 wk were enrolled for subsequent analysis. No patient had atrial fibrillation, recent (<6 wk) myocardial infarction (MI), unstable angina pectoris, or interventions in the period between different examinations. Our institutional review boards approved this retrospective study, and informed consent was not required.
Patient Management
The clinical attending physicians determined the patient management (i.e., revascularization or medical treatment) based on clinical grounds. The findings of both MRI and PET/SPECT were made available to the clinicians. Patients who underwent first surgical revascularization within 4 wk of viability studies were analyzed for early functional outcome. Electrocardiographic (ECG) and cardiac enzyme studies were obtained to identify new periprocedural MI, and postoperative functional assessments by MRI were obtained before discharge.
Imaging Protocols
MRI.
All MR examinations were performed at a 1.5-T scanner (Symphony; Siemens Medical Solutions USA, Inc.). A 12-element surface-coil array was used. Breath-hold cine MRI was performed using the segmented ECG-triggered steady-state, free-precession cine images with echo sharing (true fast imaging with steady-state, free-precession [TrueFISP]; repetition time/echo time [TR/TE], 3.0/1.5; flip angle, 62°; lines per segment, 12–28; field of view, 380 × 285 mm; matrix size, 192 × 256). Cine MRI of 10–12 contiguous sections in 8-mm-section thickness with an interslice gap of 2 mm were obtained in the short-axis planes, covering the entire LV from the base to the apex, to acquire 3-dimentional LV data, and also were acquired in the vertical and horizontal long-axis planes. Fifteen minutes after injection of a 0.15-μmol/kg dose of gadodiamide contrast agent (Omniscan; Nycomed Amersham), delayed enhanced MR images (phase-sensitive reconstructed inversion-recovery TrueFISP) were acquired in the same views as for cine images, using an inversion-recovery segmented gradient-echo sequence. The typical imaging parameters were as follows: TR/TE = 2.6/1.3; flip angle, 55°; field of view, 340 × 280 mm; matrix size, 256 × 200. In-plane image resolution was typically 1.3 × 1.6 mm (18).
PET/SPECT Protocol.
After fasting for at least 4 h, nondiabetic patients received 50 g of glucose orally, whereas diabetic patients received soluble insulin intravenously according to their blood glucose levels to achieve fasting glucose levels of <115 mg/dL (6 mmol/L) (19). Sixty minutes later, 18F-FDG (259–370 MBq) was administered intravenously. Each subject was positioned in the gantry of the PET camera (Advance; GE Healthcare) 1 h after 18F-FDG injection. A 10-min transmission scan using 2 rotating 68Ge pin sources was obtained for the attenuation correction. The spatial resolution of the reconstructed clinical PET images is ∼8-mm full width at half maximum at the center of the field of view, and the axial resolution is ∼4 mm (20).
In the symptom-limited treadmill exercise test, 201Tl (74–111 MBq) was injected intravenously at the peak exercise depending on the patient's weight, and exercise was continued for an additional minute. In patients who could not exercise adequately, dipyridamole stress tests were performed with a 4-min infusion of 0.14 mg/kg/min dipyridamole; 201Tl was injected intravenously 3 min after dipyridamole infusion (21). Initial imaging was started within 5 min after the tracer injection. Four hours after the initial examination, additional 201Tl (37 MBq) was injected and reinjection images were acquired 10 min later. In patients who had symptomatic heart failure (NYHA functional class III or IV) and could not tolerate stress, rest and redistribution SPECT images were acquired 15–20 min and 3–4 h after 111 MBq of 201Tl were given (22).
ECG-gated SPECT images were obtained with a dual-head γ-camera (Millenium; GE Healthcare) equipped with low-energy, thin-section collimation (30 projections over 180°, 8 frames per cardiac cycle, 60 s per projection). Two energy windows were set at 70- and 167-keV peaks (±15%) of 201Tl. ECG-gated SPECT images were prefiltered with a Butterworth filter (order, 5; voxel size, 72 mm; cutoff frequency, 0.4 cycle/pixel). A zoom factor of 1.28 was used. Data were reconstructed using a filtered-backprojection technique without attenuation or scatter correction (21).
Image Analysis
Global LV Function.
Global functional parameters were derived from cine MRI by an experienced reader in random order, with the aid of commercially available software (Argus; Siemens), and were followed by manual correction of the LV border (18). LV end-diastolic volume (EDV) and end-systolic volume (ESV) were calculated on the basis of Simpson's rule. Subsequently, EF was calculated with EDV and ESV values (23).
Segmental Analysis.
Images of delayed enhancement (DE) on MRI and PET/SPECT were evaluated by 2 experienced observers—each using an identical 17-segment model (24)—who had no previous knowledge of any patient's clinical data. All cine images and DE on MRI were evaluated independently by 2 experienced observers who were unaware of other study results. If there was no agreement in the interpretations, the image was reevaluated by the 2 physicians until a consensus was reached.
The basal, midventricular, and apical segments were evaluated on short-axis images, whereas the apical cap was evaluated on a 2-chamber long-axis view with MRI and on the vertical and horizontal long-axis views with PET and SPECT.
For regional wall motion analyses, cine MRI was evaluated on a 4-point scale (1 = normal, 2 = mild-to-moderate hypokinesis, 3 = severe hypokinesis, 4 = akinesis or dyskinesis). A summed wall motion score was calculated as the sum of the individual scores of 17 segments in each patient. In the contrast-enhanced MRI, the average segmental transmural extent of DE on MRI was graded visually using the following scale: 0 = no enhancement, 1 = 1%–25%, 2 = 26%–50%, 3 = 51%–75%, and 4 = 76%–100% of enhancement (14). To compare viability between MRI and nuclear techniques of a myocardial segment, a cutoff value of ≤50% DE on contrast-enhanced MRI, indicating viable myocardium, was used.
In PET/SPECT, reconstructed slices were displayed as short-axis slices and horizontal slices, as well as vertical long-axis slices, and were visually analyzed side by side. For each patient, measurements of regional 201Tl activity and 18F-FDG PET quantification were performed on the short-axis slice. Segmental 201Tl activity was normalized first (25), and 18F-FDG uptake in each segment was normalized to the myocardial segment with maximal 201Tl uptake on reinjection or redistribution SPECT images. Segments with preserved perfusion (201Tl uptake ≥ 50% of maximal activity) on 4-h SPECT images, and segments with decreased perfusion (201Tl uptake <50%) but preserved or increased metabolism (18F-FDG ≥ 50%, mismatch pattern) were considered viable. Segments with decreased perfusion and metabolism (matched defect) were considered nonviable (26). The ECG-gated SPECT images were applied to assist in differentiation of tissue attenuation in regions of decreased 201Tl activity—not for viability comparison with MRI.
Early Functional Outcome After Surgical Revascularization
In patients who had surgical revascularization, an improvement in segmental wall motion by 1 grade or more on cine MRI was considered significant. An increase of EF ≥ 5% was used to define global functional improvement. In addition, a reductions of 10% or more in EDV and ESV were considered clinically meaningful reverse remodeling (27).
Statistical Analysis
Data are expressed as mean ± SD. A paired Student t test was used to compare the continuous data between and within groups. Differences in proportions were analyzed with the χ2 test. The κ-analyses of the global agreement between 2 observers in regional wall motion scores within each imaging modality were as follows: 0–0.2, low; 0.21–0.40, moderate; 0.41–0.60, substantial; 0.61–0.80, good; and ≥0.81, perfect agreement (28).
For the prediction of regional functional improvement, all analysis was performed on a per-segment basis. Changes within groups were assessed using the Student t test or the Wilcoxon signed-rank test. Logistic regression analyses were performed to identify the best predictors of early functional reversibility in viability findings from MRI or PET/SPECT studies. Sensitivity and specificity for the prediction of improvement of regional function were subsequently determined. Receiver-operating-characteristic (ROC) curves were used to compare predictive accuracy between 2 tests.
For the prediction of global LV recovery of function, in terms of improvement of LVEF (≥5%) or reverse LV remodeling (≥10% ESV and ESV reduction), analysis was performed by patient-based analysis. Univariable and multivariable logistic regression analysis was performed to determine which variables were the best predictors. Categoric variables included sex, diabetes mellitus, history of MI, and mode of surgical revascularization. Continuous variables included age, baseline LV volumes and LVEF, and number of viable and nonviable segments. To define the predictive value of the transmural extent of DE on MRI, different cutoff values of 0, ≤25%, ≤50%, and ≤75% DE that indicated viable myocardium were included in the analyses. Variables entered the multivariable stage that had P < 0.05 in the univariate analysis and then were selected in a stepwise forward selection manner at a significance level of 0.05. All tests were 2-sided. P < 0.05 was considered statistically significant. All statistical analyses were performed using Stata 8 software packages (Stata).
RESULTS
Study Population
A total of 65 patients with chronic CAD were referred for cardiac 18F-FDG PET viability evaluation from March 2004 to August 2006. Forty-one subjects (mean age ± SD, 66 ± 10 y; 32 men; mean EF ± SD, 38% ± 13%) received MRI for clinical evaluation within 2 wk of PET studies, and all had 201Tl SPECT (exercise [n = 2] or dipyridamole–reinjection [n = 19], rest–redistribution [n = 20]) during the same period. Eight patients (20%) had PET before the MRI studies. The time interval between PET and MRI studies was 3.3 ± 2.9 d (range, 1–14 d).
All patients had multivessel diseases, and 20 (49%) had a history of MI, with an interval from MI to imaging studies of at least 3 mo. There were 21 (51%) subjects with EF of ≤30%. Eight patients (20%) had well-controlled diabetes (fasting glucose, ≤150 mg/dL). The glucose levels at the time of 18F-FDG injection were 112 ± 29 mg/dL (range, 60–145 mg/dL). All imaging studies were adequate for interpretations. The characteristics of patients recruited for comparative study between MRI and PET/SPECT are shown in Table 1.
Baseline Characteristics of Patient Population (n = 41)
Twenty-nine (70%) subjects underwent surgical revascularization (age, 66 ± 9 y; 24 men). There were no significant differences with regard to age, sex, history related to CAD, and LV function between patients who received medical therapy and those who received surgical intervention. The baseline EF was 37% ± 14% (range, 12%–50%), and 15 of these subjects (52%) had EF ≤ 30%. Fourteen (48%) patients had previous MI, and 15 had prior revascularization procedures (bypass surgery in 3 and percutaneous coronary intervention in 12). The surgical procedures included isolated coronary artery bypass grafting (CABG) in 20 (69%), concomitant mitral valve repair in 4 (14%) for severe (grade 3–4) mitral regurgitation, and ventricular restoration (VR) procedure in 5 (17%) subjects. Of them, 18 (62%) patients had surgical interventions primarily for relief of angina pectoris. Patients who received concomitant VR procedures had more previous MI, symptoms of heart failure, significantly lower EF, and larger LV volumes before surgical interventions (all P < 0.001); in addition, they also tended to be younger (P = 0.7). Except for 1 subject who died of methicillin-resistant Staphylococcus aureus sepsis on postoperative day 60, all patients had follow-up MRI examinations (17 ± 7 d after surgery; range, 7–29 d). One perioperative MI was documented by an elevation of cardiac enzymes and Q-wave on the ECG, and new transmural DE was evident on the postoperative MRI. The cases of noncardiac death and perioperative MI were excluded from functional outcome analyses. Other patients received stress–reinjection 201Tl SPECT within 6 mo after bypass surgery and had no evidence of stress-induced ischemia. The baseline characteristics and functional outcomes of the remaining 27 patients are summarized in Table 2.
Baseline Characteristics and Follow-up LV Function in Patients Who Underwent Successful Surgical Revascularization (n = 27)
Comparison of Viability Findings on MRI and PET/SPECT (n = 41 Subjects)
In regional wall assessment, the mean κ statistics of interobserver agreement were 0.90 (range, 0.84–0.95) on cine MRI. In transmural DE assessment on the 0–4 scales, the mean κ of interobserver agreement were 0.78 (range, 0.64–0.88). The consensus of interpretations was used for subsequent comparison.
On the basis of a total of 394 dysfunctional segments, more viable myocardium was detected using 18F-FDG PET than using 201Tl SPECT (perfusion–metabolism mismatch) on 55 (14%) segments from 13 (45%) patients. The transmurality of DE on MRI was negatively correlated with the viability detected on PET/SPECT (Fig. 1; Table 3). In addition, there were 6 cases with partial fill-in on 201Tl reinjection–redistribution images (37 segments), and 34 segments (92%) had 18F-FDG uptake ≥ 50% and DE ≤ 50% on MRI. The other 3 segments were regards nearly transmural DE on MRI and also < 50% of 18F-FDG maximal uptake on PET.
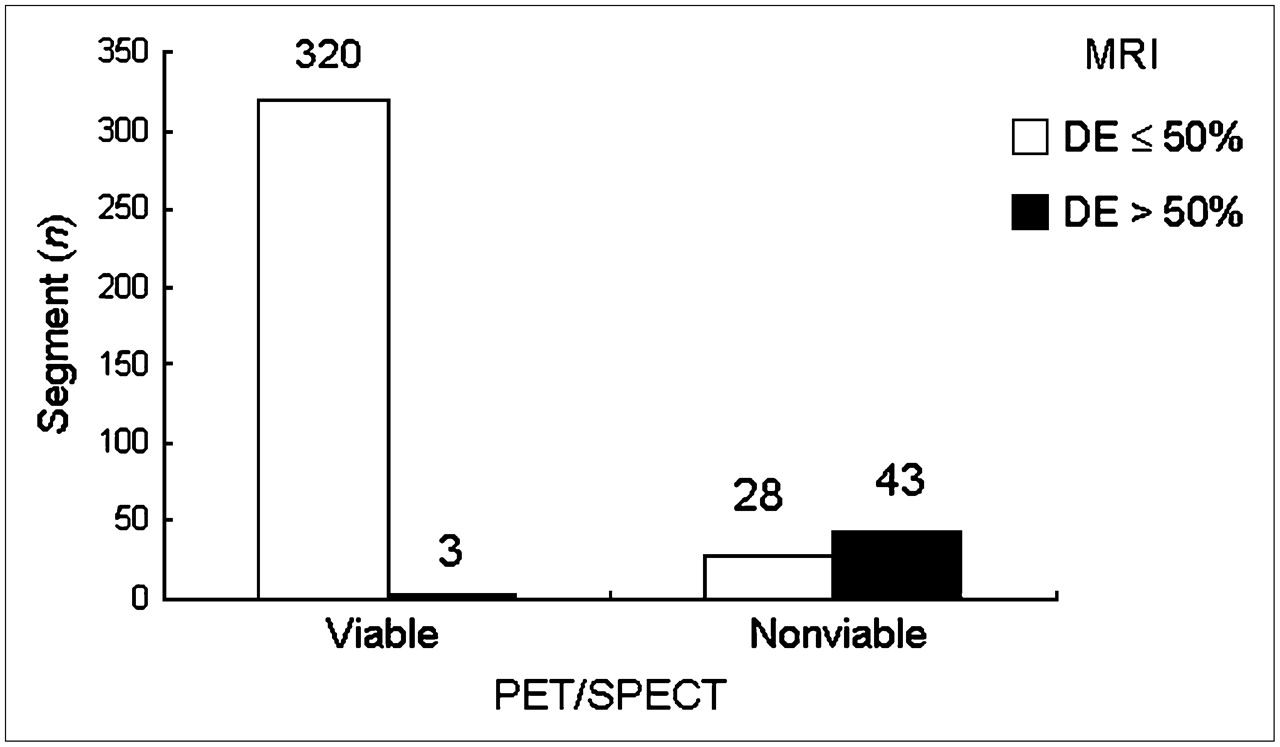
Segmental extent of DE by MRI categorized according to 18F-FDG PET/201Tl SPECT in dysfunctional myocardium (n = 394).
Transmurality of DE in Dysfunctional Myocardium (n = 394)
Early Regional Reversibility by Segmental Analysis
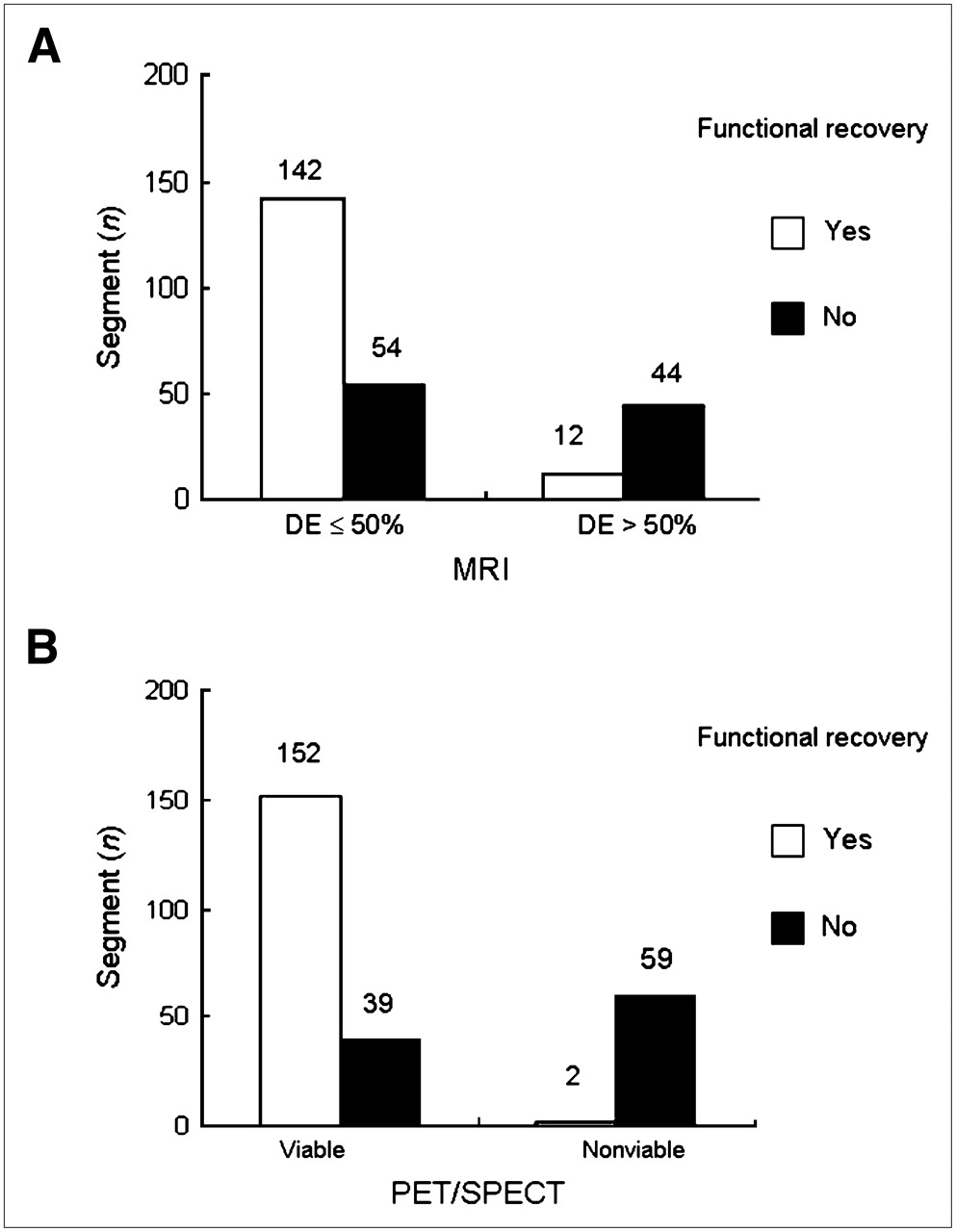
Of 252 dysfunctional segments from 27 subjects (9.6 ± 6.5 segments per subject) that underwent successful surgical revascularization, 154 (61%) segments showed functional improvement. The summed wall motion scores increased from 30 ± 9 to 26 ± 10 (P = 0.001). A gradual decrease in the probability of segmental functional recovery was observed as an increase in the extent of DE on MRI (β-coefficient = −1.09 ± 0.14; P < 0.001; in Fig. 2A). On the other hand, segments considered nonviable by PET/SPECT revealed a very low likelihood of functional recovery (β-coefficient = −4.85 ± 1.03; P < 0.001) (Fig. 2B). Accordingly, the sensitivity, specificity, positive predictive value, and negative predictive value were 60.2%, 98.7%, 76.6%, and 96.7% of PET/SPECT viability criteria in prediction of early functional recovery, whereas these values were 92.2%, 44.9%, 72.4%, and 78.6%, respectively, using the cutoff of 50% DE on MRI. There were no significant differences in overall accuracies using MRI or PET/SPECT by ROC area analysis.

Relation between segmental viability status by MRI categorization (A) and 18F-FDG PET/201Tl SPECT (B) and early functional outcome after surgical revascularization (n = 252).
In a subgroup analysis of isolated CABG (n = 18), 151 dysfunctional segments (8.8 ± 5.9 segments per subject) were analyzed, of which 110 (73%) segments showed functional improvement. The summed wall motion scores increased from 30 ± 7 to 24 ± 7 (P < 0.001). Significantly less functional recovery was noted with increasing DE on MRI (β-coefficient = −0.67 ± 0.14; P < 0.001). None of the segments considered nonviable on PET/SPECT improved function on follow-up. The sensitivity, specificity, positive predictive value, and negative predictive value were 57.5%, 100%, 86.7%, and 100% of PET/SPECT viability criteria, whereas these values were 67.6%, 77.5%, 89.3%, and 46.2%, respectively using the cutoff of 50% DE on MRI, without significant difference.
In addition, the combination of 50% DE on MRI and PET/SPECT had slightly higher overall accuracy than either examination result but not reach statistical significance.
Global LV Function and Remodeling After Isolated CABG (n = 18 Subjects)
Because the time course and magnitude of functional changes could be different in patients with concomitant MV repair or VR, 18 subjects who received isolated CABG without complication were analyzed for global functional outcome. Of these patients, 11 (61%) sustained improved function (i.e., 10 with ≥5% EF improvement and 9 with ≥10% reduction in LV volume) postoperatively. Patient-based multivariable logistic regression analysis showed that patients with no DE on MRI always had a favorable early recovery, whereas patients with substantial scar (≥4 segments) on PET/SPECT always showed the predicted failure with respect to the clinical EF improvement and also in reverse LV remodeling (all P < 0.0001). The representative examples are shown in Figures 3–5⇓⇓.

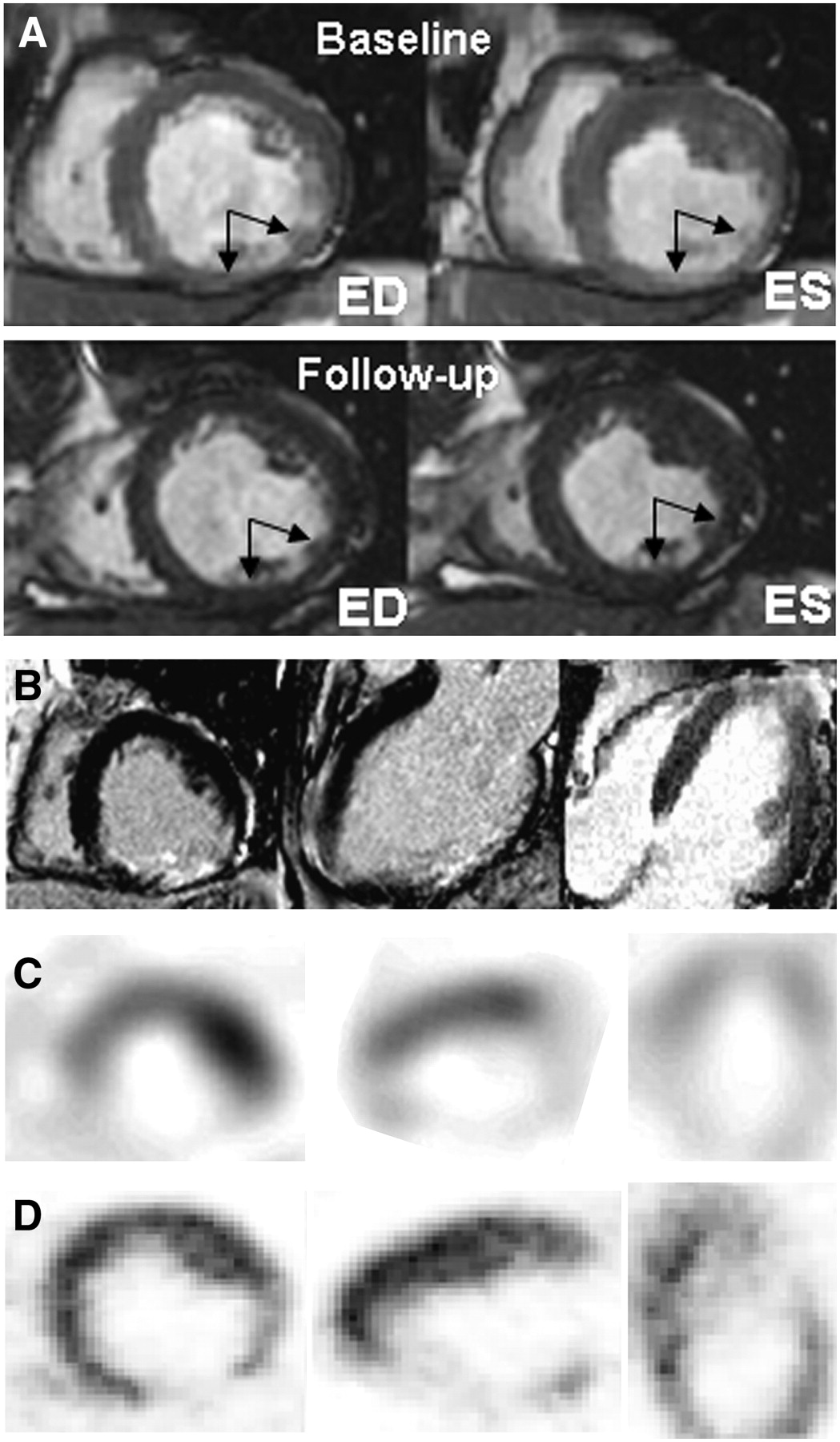
A 70-y-old man with history of anterior wall MI. (A) Steady-state, free-precession cine MR images in short-axis (top panel) and long-axis (bottom panel) planes show apical aneurysm and anterior wall hypokinesis (left column); the myocardial wall motion and systolic wall thickening improves in these segments after CABG (right column; arrows). ED = end-diastole; ES = end-systole. (B) Transmural DE in apex and >50% DE in anterior wall are evident. (C) Severe hypoperfusion on redistribution 201Tl SPECT (C) and preserved 18F-FDG uptake on PET (D) are observed in the corresponding segments.

A 56-y-old man with history of inferior wall MI. (A) Cine MR images in short-axis plane show inferior wall akinesis (top panel) and regional wall motion that do not change after CABG (bottom panel; arrows). ED = end-diastole; ES = end-systole. (B) Transmural DE in inferior wall is evident. Hypoperfusion on redistribution 201Tl SPECT (C) and enhanced 18F-FDG uptake on PET (D) are observed (mismatch pattern).

A 64-y-old man with history of inferior wall MI. (A) Cine MR images in short-axis plane show akinesis with wall thinning in inferior wall (top panel), without significant improvement after bypass surgery (bottom panel; arrows). ED = end-diastole; ES = end-systole. (B) More than 75% DE is noted in these segments. (C) Severe hypoperfusion in inferior wall on redistribution 201Tl SPECT (C) and decreased 18F-FDG uptake on PET (with smaller extent than SPECT) (D) are observed.
DISCUSSION
Assessment of viability has become important in the management of patients with chronic CAD. The aim of the present study was to investigate the prediction of contrast-enhanced MRI and 18F-FDG PET on an early functional outcome after successful surgical revascularization. The major findings of this study are as follows. First, a correlation between the amount of DE on MRI and 18F-FDG uptake is observed on dysfunctional segments. Second, segments considered viable on PET/SPECT predicted a functional improvement after surgical revascularization, whereas 50% DE on MRI was not a good discriminator of early functional outcome. Third, patients without any DE on MRI are prone to have EF improvement and reverse LV remodeling early after surgical revascularization. On the other hand, patients with substantial nonviable myocardium detected on PET/SPECT always had a poor global functional outcome.
Relationship Between Contrast-Enhanced MRI and PET/SPECT
Previous studies have suggested that DE on contrast-enhanced MRI represented irreversible myocardial injury, thus allowing determination of myocardial viability. Our results showed that the proportion of the transmural extent of enhancement on MRI was negatively correlated with 18F-FDG uptake on PET, in close agreement with previously comparative analyses (16,17,26,29). Although the spatial resolution of MRI with regard to delineating subendocardial abnormalities is far superior to that of PET/SPECT—and tends to identify more scar tissue than nuclear imaging—the results of 50% DE used as the cutoff value on MRI were comparable to viability detected by PET/SPECT, with an overall agreement of 91.8%.
Early Functional Outcome
Thus far, data relating to myocardial viability on the early functional outcome are scarce. We found that early functional improvement was not uncommon after successful surgical revascularization, even in patients with a lower EF. Our results confirmed that the probability of early functional recovery was significantly higher when both modalities demonstrated preserved viability and was almost negligible when both indicated nonviability. In addition, no DE on MRI provided the best predictive value for functional improvement after surgical revascularization. On the other hand, 18F-FDG PET is useful for predicting nonreversible myocardial scarring when it shows extensive nonviable myocardium.
Our study shows rather low sensitivity and excellent specificity of PET/SPECT on segmental and global functional recovery early after surgery, in comparison with previously reported sensitivities of 87%–93% and specificities of 76%–86% at 6 mo or later after revascularization (26,30,31). On the other hand, the predefined threshold of 50% transmural extent of enhancement on MRI was not a good discriminator of segmental functional recovery as previously reported (14,15,17,26,29,32). Instead, no DE on contrast-enhanced MRI could be considered as a good independent predictor of a favorable global functional outcome, whereas substantial nonviable myocardium on PET always revealed a poor response to surgical revascularization, suggesting that extensive scar tissue does not permit early functional improvement. The results also reflect nuclear imaging modalities and MRI in detection of different pathphysiologic aspects of dysfunctional but viable myocardium. Nuclear imaging modalities are less sensitive in detecting the subendocardial scar; however, it might provide functional information of residual viable myocardium, which could play a significant role in early functional recovery (33).
The prevalence of patients with severe LV dysfunction referred for CABG is increasing, and the surgical survival is critically dependent on patient selection (34,35). The early functional recovery could be associated with improved hospital outcome and comparable long-term results. The early functional outcome could be considered as a surrogate prognostic marker, although an improvement could still happen late, especially in more severely injured myocardium (11–13,36). Our data suggested that a multimodality diagnostic strategy for viability detection might provide complementary information for decision making in certain cases that are most likely to benefit from surgical revascularization.
Limitations
This investigation is a retrospective, nonrandomized, small-size study and patient management is based on clinical decisions, which could have been sources of selection bias. The characteristics of patients and surgical procedures were rather heterogeneous, which could influence the functional outcomes. The cases of noncardiac death (n = 1) and perioperative MI (n = 1) were excluded from functional outcome analyses, which might also influence the results. The lack of a longer-term assessment is a limitation. Assessing functional recovery before discharge could underestimate regional and global functional recovery; as prior investigations have demonstrated, recovery of contractile function may require longer time periods. In the current study, the small proportion of patients with severe LV dysfunction (EF ≤ 30%) who underwent surgery could influence the results, which also was revealed in the higher prevalence of functional recovery. The use of 99mTc-labeled agents, instead of 201Tl, could increase the diagnostic specificity of SPECT. Finally, attenuation correction was not used in the current study; however, we used gated SPECT as an aid.
CONCLUSION
Our study indicated that the preserved viability by PET/SPECT could accurately identify early reversibility of segmental wall motion abnormality. In global functional recovery, improvement of EF and reverse LV remodeling were best predicted by no DE on MRI. Patients with substantial nonviable myocardium on PET/SPECT may represent a poor early functional outcome after surgical revascularization. Thus, combined assessment of metabolism and tissue composition could provide a better prediction of early functional outcome.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication December 2, 2006.
- Accepted for publication April 17, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-FDG PET in Myocardial Viability Assessment: A Practical and Time-Efficient Protocol
- CMR Imaging Assessing Viability in Patients With Chronic Ventricular Dysfunction Due to Coronary Artery Disease: A Meta-Analysis of Prospective Trials
- Use of cardiovascular magnetic resonance imaging in the assessment of left ventricular function, scar and viability in patients with ischaemic cardiomyopathy and chronic myocardial infarction
- Current issues in nuclear cardiology