


Abstract
High tumor uptake of 18F-FDG is associated with an unfavorable outcome in cancer patients. We evaluated pretreatment 18F-FDG uptake as guidance for the primary treatment modality in patients with squamous cell carcinoma (SCC) of the oropharynx. Methods: Fifty-two consecutive patients with newly diagnosed resectable SCC of the oropharynx underwent 18F-FDG PET before treatment. Primary treatment modalities consisted of surgical resection plus radiotherapy (RT) (surgery group, n = 31) or radical RT plus chemotherapy (RT group, n = 21). The sex, age, tumor stage, histologic grade, TNM classification, treatment strategy, and maximum standardized uptake value (SUV) categories were analyzed for association with local control (LC) and disease-free survival (DFS). The median follow-up of the surviving patients was 36 mo. Results: The median SUV was significantly higher in the 11 patients who failed treatment than that in the remaining controlled patients (8.0 vs. 5.4; P = 0.021). Patients having tumors with a high SUV > 6.0 had poorer LC and DFS (P < 0.05). In multivariate analysis, the SUV remained an independent determinant of LC and DFS (P < 0.05). Patients with a SUV > 6.0 in the surgery group had a higher 3-y DFS than that in the RT group (78% vs. 33%; P = 0.043). Conclusion: Pretreatment tumor 18F-FDG uptake represents an independent prognostic factor in patients with oropharyngeal SCC. Patients with high 18F-FDG uptake may be better treated by surgery followed by RT with or without chemotherapy, which needs to be verified by a prospective randomized study.
The predominant treatment modalities for squamous cell carcinomas (SCCs) of the oropharynx consist of surgery, radiation therapy (RT), and chemoradiation therapy (CRT), individually or in combination (1). A single-modality therapy with radiation or surgery can achieve similar locoregional control for early-stage cancers, with RT generally yielding better functional outcomes (2,3). Although patients with more advanced disease (stages III and IV) have been traditionally treated with surgery followed by RT, there has been an increase in the use of chemoradiation organ-preserving protocols. Prospective randomized studies have shown that, compared with RT alone, concurrent chemotherapy resulted in significant improvements in local control (LC), relapse-free survival, and overall survival (OS) (4,5). However, no randomized trials have been performed comparing the combination of chemotherapy and RT with surgery. Moreover, these complex treatments have substantial toxicity and, therefore, are not suitable for all patients. Thus, by predicting response or survival after the combined treatment, individualized treatment strategies can be developed that lead to improved LC and survival outcomes.
18F-FDG PET has been used increasingly for the staging and follow-up of patients with head and neck cancer (6,7). Tumor 18F-FDG uptake may also have prognostic significance, in that patients with high 18F-FDG uptake have been shown to have a less-favorable outcome (8,9). Therefore, 18F-FDG PET may be used to identify the subset of patients who might respond to CRT. This has implications not only for the clinical management of head and neck cancer patients but also for their prognostic stratification. The relationship between tumor 18F-FDG uptake and the outcomes of different treatment strategies in patients with oropharyngeal SCC has received little attention. Therefore, we evaluated pretreatment 18F-FDG uptake as a predictor of survival and as guidance for the primary surgery or RT plus chemotherapy in patients with resectable SCC of the oropharynx.
MATERIALS AND METHODS
Patient Eligibility and Study Design
Between January 2001 and December 2004, consecutive patients presenting with newly diagnosed, resectable SCC of the oropharynx at Asan Medical Center underwent 18F-FDG PET evaluation before treatment. Tumor staging was based on all information provided by the different examinations, including the 18F-FDG PET scan. Patients with cancers other than SCC, primary tumors of organs other than the oropharynx, unresectable tumors, second primary tumors, distant metastatic disease at initial diagnosis, and significant comorbidities were excluded. Three patients who did not receive complete treatments because of toxicity or poor patient cooperation and 1 patient who died within 3 mo of therapy with unknown disease status or complications of treatment were also excluded. Fifty-two eligible patients with oropharyngeal SCC were suitable for analysis. These patients were grouped by primary treatment modality: curative surgery plus postoperative RT with or without chemotherapy (surgery group, n = 31) and radical RT plus chemotherapy (RT group, n = 21). Primary treatment modalities were selected by the patients and their families and the multidisciplinary tumor board and were not based on 18F-FDG PET or other imaging results. The study protocol was reviewed and approved by the institutional Ethics Review Committee.
All patients in the surgery group underwent wide curative resection of their primary tumors, with or without mandibulotomy and reconstructive procedures. Patients had radical (n = 9), modified radical (n = 14), or selective (n = 8) neck dissections, with 11 having bilateral dissections. Twenty-five patients received postoperative locoregional RT (median dose, 62.6 Gy; range, 32.4–68.4 Gy), using a single daily fraction. Five patients in the surgery group also received adjuvant chemotherapy with 1 or 2 cycles of cisplatin, with or without a continuous infusion of 5-fluorouracil, before or after surgery.
Twenty-one patients in the RT group received radical locoregional RT, using 6-MV photons, to the primary tumor site and head and neck lymphatics, without curative surgery. The altered fractionated RT was not used in all patients, and the mean radiation dose for all patients was 68.8 Gy (range, 60.2–76.2 Gy) using the daily fraction in all patients. Eighteen patients also received concomitant chemotherapy, generally 2 or 3 cycles of cisplatin with or without a continuous infusion of 5-fluorouracil or docetaxel administration. Of them, 4 received neoadjuvant chemotherapy followed by concomitant chemoradiotherapy (CRT). Salvage resections of primary tumors and neck dissections were performed in 6 and 7 patients, respectively, with persistent or recurrent tumors after RT or CRT.
18F-FDG PET
18F-FDG PET was performed using an ECAT HR+ scanner (Siemens Medical Solutions USA, Inc.), which provided an in-plane spatial resolution of 4.5 mm and an axial field view of 15.5 cm. All patients fasted for at least 6 h before 18F-FDG PET, and their blood glucose concentrations were measured; patients with diabetes mellitus were required to have controlled blood glucose levels (<150 ng/mL) before having the scan. All patients rested for at least 1 h before 18F-FDG PET scanning and received an intravenous injection of approximtely 555 MBq 18F-FDG. Sixty minutes after 18F-FDG injection, with the patient in the supine position, whole-body imaging was performed from the head to the midthigh. Data were reconstructed into coronal, sagittal, and transverse sections and a 3-dimensional rotating projection. Visible lesions with increased tracer uptake were identified and their 18F-FDG uptake was quantified. The maximum standardized uptake value (SUV) was semiquantitatively analyzed according to the equation, SUV = A/(ID/LBW), where A is the decay-corrected activity in tissue (in MBq/mL), ID is the injected dose of 18F-FDG (in MBq), and LBW is the patient's lean body weight. The SUVs of primary lesions were measured from focal 18F-FDG uptake greater than background activity in the oropharyx and corresponding to lesions detected on CT/MRI. Because 3 patients had no definitively abnormal focal 18F-FDG uptake in the oropharynx, the SUVs (<2.5) were measured from the values close or equal to background activity of the oropharyngeal subsites corresponding to CT/MRI findings and reported by physicians. The SUV of the primary tumor was used as a reference for correlation with LC and survival.
Statistical Analysis
Actuarial LC, disease-free survival (DFS), and OS rates were calculated by the Kaplan–Meier method. Persistent or recurrent tumors were documented by endoscopy, CT/MRI, or 18F-FDG PET. The time intervals for LC and survival endpoints were calculated from the first day of treatment until the date of an event or of the last follow-up. The log rank test was used to assess the correlation of these endpoints with SUV and with the other clinical (sex, age, tumor site, T category, N category, TNM stage, histologic grading) and therapeutic (treatment group) variables. Variables found to be significant by univariate analysis were subjected to multivariate analysis using the Cox proportional hazards model. Analysis of data in contingency tables or mean comparison was performed using the χ2 test or the t test. Data were expressed as mean ± SD. A P value < 0.05 was considered statistically significant.
RESULTS
The study cohort consisted of 52 patients (45 men, 7 women; median age, 56 y; age range, 32−73 y). Patient characteristics are summarized in Table 1. Distribution of sex, age, and TNM classification and of site, size, histologic grading, and SUV of primary tumors were comparable in the surgery and RT groups (P > 0.15). At last follow-up, 42 patients were alive and 10 had died: 9 from oropharyngeal cancer and 1 from a second primary tumor. The median follow-up for surviving patients was 36 mo (range, 12–71 mo). Ten patients presented with recurrent local or regional disease, and 6 presented with distant metastases. At 3 y, actuarial LC was 82%, DFS was 74%, and OS was 76%.
Patient Characteristics
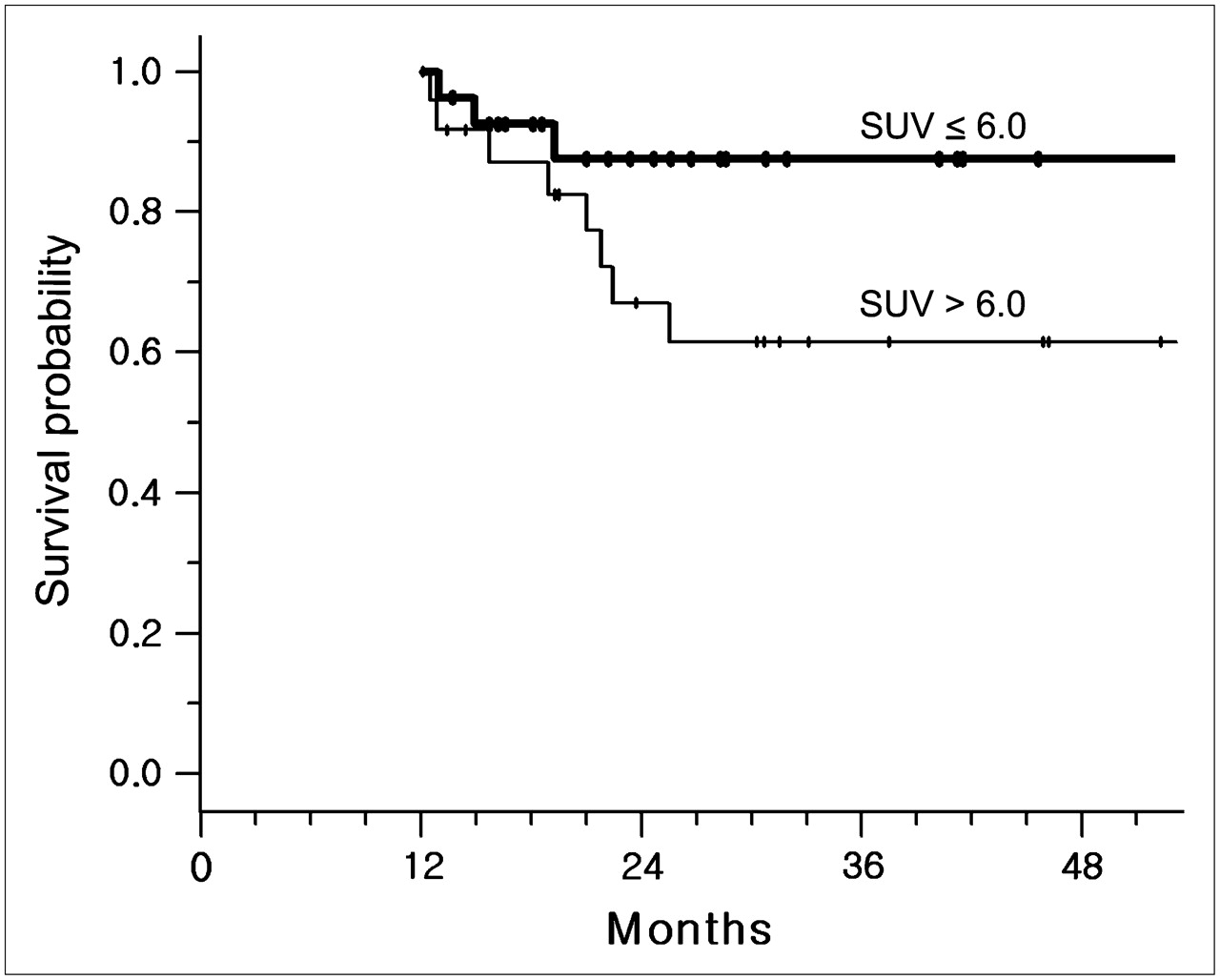
The median SUV of primary tumors was 6.1 (range, 1.5–18.4). The mean tumor SUV of all patients was 5.9 ± 3.2 and was comparable in the surgery and RT groups (5.9 ± 3.5 vs. 5.9 ± 2.8; P = 0.994; Table 1). The mean SUV was significantly higher in the 11 patients who presented with local, regional, or distant failure than that in the remaining controlled patients (8.0 ± 3.4 vs. 5.4 ± 3.0; P = 0.021). Tumor SUV was highly correlated with the size of the primary tumor (Pearson correlation coefficient = 0.59, P < 0.001) but not with histologic grade or TNM stage (P > 0.4). In the absence of an established cutoff for SUV, the median value was used to establish groups of patients with a high (>6.0) SUV and a low (≤6.0) SUV, close to the mean and median SUVs. By univariate analysis, T and SUV categories and treatment modality showed significant correlations with 3-y DFS (P < 0.05), whereas only the SUV category showed a significant correlation with 3-y LC (P = 0.038) (Table 2). The surgery group had a significantly higher 3-y DFS than the RT group (85% vs. 55%; P = 0.036) (Fig. 1). Patients with a low (≤6.0) SUV had a higher 3-y LC (92% vs. 60%; P < 0.04) and DFS (88% vs. 61%; P < 0.04) than did those with a high (>6.0) SUV (Fig. 2).
Univariate Analysis for LC and DFS
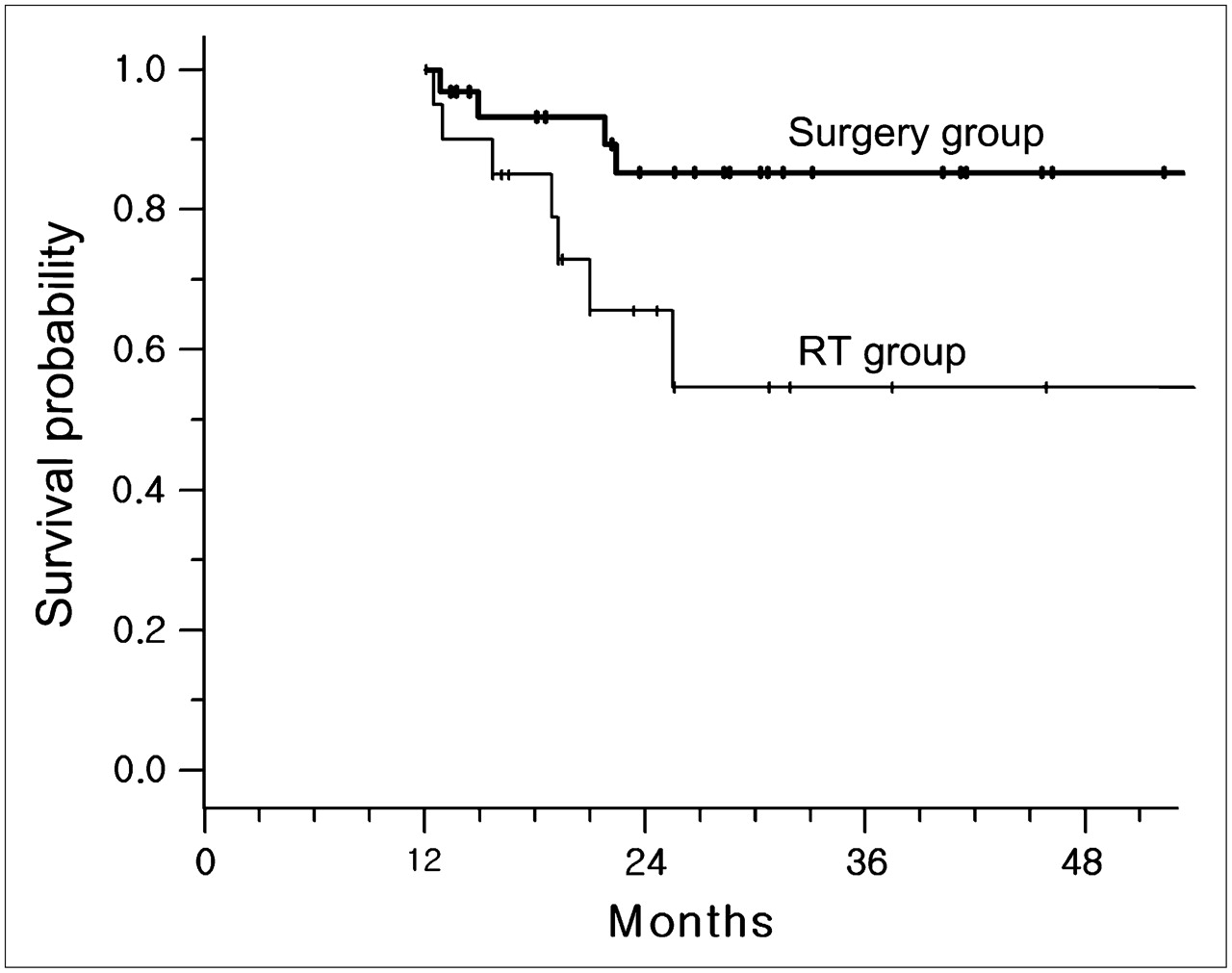
Actuarial DFS in patients treated with surgery (n = 31) or RT (n = 21) as primary treatment modality (P = 0.036).

Actuarial DFS using cutoff of 6.0 for SUV of 18F-FDG (low vs. high SUV, n = 27 vs. 25) (P = 0.036).
Factors significantly influencing DFS in univariate analysis and the site of the primary tumor were included in the Cox proportional hazards model. The parameters (T and SUV categories and treatment modality) showing statistical correlation with survival were accounted for by stratifying according to tumor site. Both LC and DFS rates were significantly lower in patients with a high SUV (P < 0.05), and DFS tended to be higher in the surgery group than in the RT group (P = 0.054) (Table 3).
Cox Proportional Hazards Models for LC and DFS
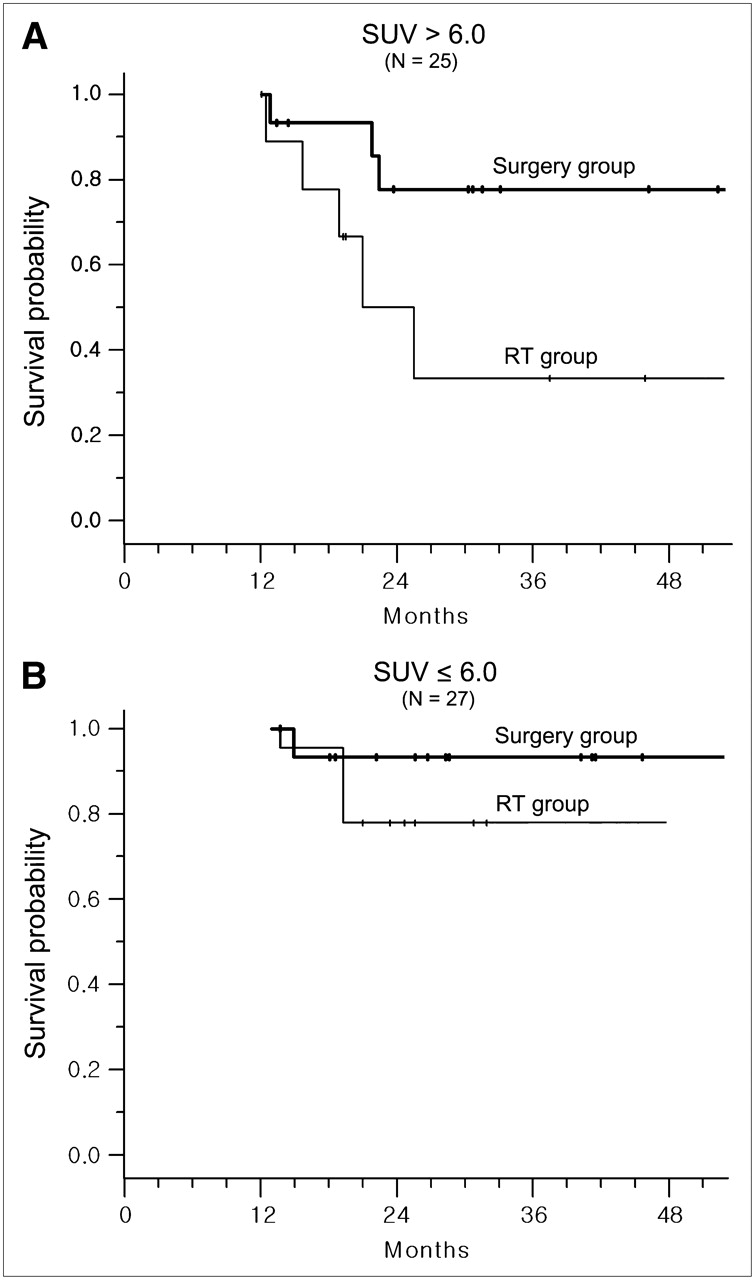
We also compared DFS in patients with high and low SUVs relative to those of the treatment subgroup (Fig. 3). Among the 25 patients with a high SUV > 6.0, 3-y DFS was higher in the surgery group (n = 15) than that in the RT group (n = 10) (78% vs. 33%; P = 0.043) (Fig. 3A). However, among the 27 patients with a low SUV ≤ 6.0, 3-y DFS was similar in the surgery (n = 16) and RT (n = 11) groups (93% vs. 78%; P = 0.329) (Fig. 3B).
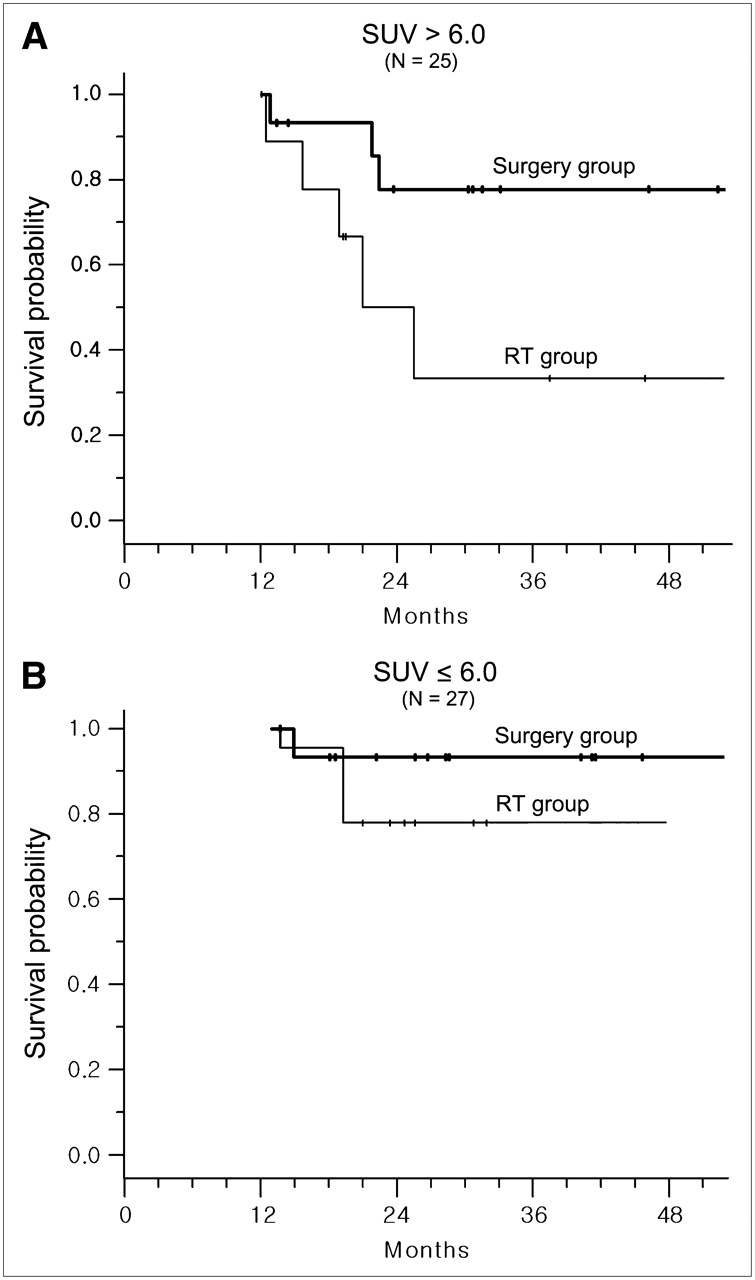
Actuarial DFS in patients treated with surgery or RT as primary treatment modality in patients with tumor SUV ≤ 6.0 and SUV > 6.0. In 25 patients with SUV > 6.0, primary surgery followed by RT (n = 15) resulted in a statistically better survival than did RT with chemotherapy (n = 10) followed by surgical salvage (A; P = 0.043). In 27 patients with SUV ≤ 6.0, there was no significant difference between surgery plus RT (n = 16) and RT plus chemotherapy (n = 11) (B; P = 0.329).
In the RT group, the complete response after RT plus chemotherapy seemed to be higher in the 10 patients with a low SUV than that in the 11 patients with a high SUV (90% vs. 64%) but the difference was not statistically significant, due to the relatively small number of patients (P = 0.157). However, 3-y DFS in the RT group was significantly higher in the patients with a low SUV than that in patients with a high SUV (86% vs. 30%, P = 0.039).
DISCUSSION
Outcome indicators in patients with head and neck cancer have traditionally been derived from clinical and pathologic features (10). Despite careful evaluation of established prognostic factors in head and neck patients, it is currently impossible to reliably predict treatment outcomes, even in patients within the same TN category (11). Identification of additional prognostic factors for locoregional control and survival—particularly, biologic parameters—may allow the development of individualized strategies that lead to improved LC and survival. Increased glycolysis has been observed in cancers (12), and high 18F-FDG uptake has been reported to be an indicator of poor prognosis in head and neck cancers (8,9,13,14). Several studies have suggested that 18F-FDG PET can identify this subset of patients (13,14). Our multivariate analysis of the entire series of patients showed that, in oropharyngeal SCC, the SUV was an independent prognostic factor for survival. Our results confirmed prior findings, showing that high 18F-FDG uptake was generally associated with tumor aggressiveness and a less favorable survival outcome.
There are important reasons to avoid primary surgical therapy for oropharyngeal cancers. Even in their early stages, these carcinomas are associated with a risk for regional lymph node metastases as well as a high risk of bilateral neck disease (1). In addition, there are difficulties in surgical approach and considerable surgical morbidity. Thus, there has been an overall trend toward primary therapy with RT or CRT, especially for patients with advanced disease (1,3–5). However, these combined treatments have substantial toxicity and, therefore, are not suitable for all patients. 18F-FDG uptake by head and neck cancers may be able to predict outcomes after therapy (8,9,13,14). These earlier studies of 18F-FDG PET included patients with tumors at various sites of the head and neck and were primarily concerned with the outcomes of nonsurgical therapies. Primary tumors at multiple sites may be associated with different tumor burdens, which may affect 18F-FDG uptake, treatment response, and survival—thus, leading to potential biases. Therefore, we tested the predictive value of 18F-FDG uptake only in patients with newly diagnosed, resectable SCC of the oropharynx, who were treated with surgery followed by RT or with radical RT combined with chemotherapy.
Our results are generally in agreement with those of other studies on head and neck cancers, including those treated surgically (8,13) or nonsurgically (9,14). We found that patients treated with surgery plus postoperative RT had better LC and DFS outcomes than did patients treated with RT plus chemotherapy, perhaps because one third of the latter experienced locoregional failure after RT or CRT. Although RT combined with chemotherapy has been used increasingly in many institutions, our results suggest that nonsurgical therapy may be not an ideal modality for all patients with oropharyngeal SCC and may be inferior to the traditional therapeutic modality of surgery followed by RT.
We also observed an apparent link between 18F-FDG uptake and individualized therapeutic selection. Complete response to CRT is the single most important predictor of OS in patients with head and neck cancer (15). We found that 18F-FDG PET can reliably predict survival outcomes but not response after CRT. We did not detect a statistical difference in RT or CRT response rate between patients with low and high SUVs, perhaps because of the relatively small number of patients. In patients with a high 18F-FDG uptake who underwent primary RT or CRT, the unfavorable survival outcomes seemed to be closely related to the poor treatment response and increased locoregional recurrence after treatment. The relation between RT or CRT response and survival outcome may become clear by further accumulation of data from patients with oropharyngeal SCC.
Our results also suggest a potential role for 18F-FDG PET as guidance for the primary treatment modality. Local disease control and survival outcomes were generally higher in the surgery group than those in the RT group, and this difference was significant in patients with a high (>6.0) tumor SUV but not in those with a low (≤6.0) tumor SUV. This finding suggests that patients with high tumor 18F-FDG uptake may have improved survival with early surgical intervention followed by RT. Primary RT or CRT may be optional only in patients with low 18F-FDG uptake who hope to avoid surgery and postoperative morbidity.
Poor responders to RT or CRT may also respond poorly to radical surgery, whereas they may benefit from multimodal therapies. Combined-modality therapy has been developed to increase disease control, patient survival, and functional outcome in patients with advanced malignancies (16). The multimodal intensified schedule is usually based on CRT with surgical adjuncts. However, our results suggest that surgery followed by RT may be a better choice for patients with resectable SCC of the oropharynx and high 18F-FDG uptake. This finding suggests the need for additional trials on larger numbers of these patients.
CONCLUSION
We found that high 18F-FDG uptake (SUV > 6.0) was a marker for poor outcome in patients with SCC of the oropharynx, confirming earlier findings showing that pretreatment tumor 18F-FDG uptake represents an independent prognostic factor in patients with head and neck cancers. To our knowledge, this study is the first to compare outcomes of primary therapeutic modalities based on tumor 18F-FDG uptake, and our results suggest that patients with high 18F-FDG uptake may obtain survival benefits from primary surgery followed by RT with or without chemotherapy rather than from primary CRT. Thus, the use of pretreatment 18F-FDG PET in proper selection of the primary treatment modality may lead to the increased survival of patients with aggressive oropharyngeal cancer. However, our conclusions need to be verified by a prospective randomized study involving the groups of patients who undergo more homogeneous treatment modalities.
Acknowledgments
This work was supported by the Ministry of Science and Technology (grant F104AA010009-06A0101-00910) and the Ministry of Health & Welfare, the National R&D Program for Cancer Control (grant 0620160-1), Seoul, Republic of Korea.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication January 4, 2007.
- Accepted for publication February 12, 2007.





{kind=link}
{kind=link}
{kind=link}