


Abstract
Gait disturbance in idiopathic normal pressure hydrocephalus (iNPH) is reminiscent of parkinsonism. Our recent PET study showed reduction in postsynaptic D2 receptor binding concomitant with a normality of presynaptic dopamine transporter binding. Here, we investigated the plasticity of D2 receptor in treating iNPH patients with ventriculoperitoneal (VP) shunting using PET with 11C-raclopride and discuss the contribution of D2 receptor to the pathophysiology of iNPH. Methods: Eight iNPH patients participated in this study. After evaluation of their neuropsychologic abilities, all patients underwent 3-dimensional MRI and quantitative PET measurements twice before and 1 mo after VP shunting. MRI-based morphometric analyses were performed to examine postoperative variations of the ventricles. Estimation of binding potential (BP) for 11C-raclopride was based on Logan plot analysis. Region-of-interest analysis was used to examine changes in 11C-raclopride BP in the striatum. A 2-tailed paired t test was used for evaluating changes in PET and MRI parameters between conditions, and correlation analysis was used to investigate clinicopathophysiologic relevance (clinical vs. in vivo findings). Results: Clinical evaluation revealed significant recovery in a 5-m back-and-forth navigation test and an affect test and a mild increase in Mini-Mental State Examination scores after VP shunting. Significant postoperative increases in 11C-raclopride BP were found in the nucleus accumbens and dorsal putamen, and the increases were significantly associated with emotional (Spearman rank r = 0.66, P < 0.05) and navigational improvement (r = 0.72, P < 0.05), respectively. The 11C-raclopride BP increase in the striaum as a whole correlated significantly with improvement in general cognitive ability. There was a mild ventricular shrinkage after surgery, albeit there was no correlation of its size with clinical and PET parameters. Conclusion: Striatal upregulation of D2 receptor after VP shunting is associated with amelioration of hypokinetic gait disturbance and anhedonic mentation in iNPH patients, indicating that the effect of VP shunting may reside in noninhibition of functionally suppressed D2 receptor in the striatum. D2 receptor responsiveness may indicate a mechanism for iNPH pathophysiology.
The clinical triad for idiopathic normal pressure hydrocephalus (iNPH) consists of gait disturbance, progressive dementia, and urinary incontinence (1), which develop insidiously without causative disorders (2). In the clinical setting, gait disturbance is likely the first sign and important symptom in NPH (3). However, this hypokinetic type of gait disturbance is not unique in other neurologic diseases such as Parkinson's disease (PD) and dementia with extrapyramidal symptoms. To diagnose iNPH, a spinal tap is considered prerequisite, and empirically its effect on gait improvement is the most remarkable (4). Our previous study highlighted a close relationship of gait impairment with putaminal D2 receptor downregulation in iNPH (5). In this study, we investigated whether the reduction in D2 receptor activity is constant even after ventriculoperitoneal (VP) shunting.
The effect of VP shunt surgery on cerebral glucose metabolism is reportedly inconsistent (6), but increases in cerebral glucose metabolism (7) and cerebral vascular response (8) after shunting are likely to parallel clinical improvement in iNPH. Experimental animal studies showed that kaolin-induced reductions in regional cerebral blood flow in kitten (9) and immunoreactivity of subsatatia nigral neurons in rats (10) were restored by VP shunting. Despite these lines of studies, the VP shunt effect on the neurotransmitter system—especially the dopaminergic system, which is important for psychomotor control—remains to be investigated. Therefore, the present study, using PET with 11C-raclopride in combination with evaluation of clinical variables before and after the surgery, was designed to test whether the reduced D2 receptor activity in the striatum can be restored by VP shunting.
MATERIALS AND METHODS
Patients
We studied 8 patients with iNPH who were all naïve to dopaminergic drugs (5 men, 3 women: mean age ± SD, 74.9 ± 2.0 y [range, 72–77 y]; Table 1) and whose diagnoses were based on the clinical and imaging features: gait disturbance, cognitive impairment, sphincter control problem, normal lumber cerebrospinal fluid (CSF) pressure < 20 cm H2O (1,11), ventricular enlargement in the brain, and reduced cortical sulcal space in the superior convexity on coronal viewing of MR images (12). We excluded patients who showed any degree of extrapyramidal symptoms such as rigidity or tremors reminiscent of PD. In addition, a positive response in CSF tap tests (13) after PET measurement confirmed the inclusion of patients with iNPH in the current study. The CSF flow after shunting was controlled using a Codman–Hakim programmable valve system. The current study was approved by the local Ethics Committee of the Hamamatsu Medical Center, and written informed consent was obtained from all participants after a full explanation of the nature of the study.
Clinical Features of Each Patient Before and After Shunting
Psychobehavioral Assessment
As described previously (5), before each PET measurement, all patients received a general cognition test (Mini-Mental State Examination [MMSE]; full score = 30) and an affect test regarding basic affects: happiness, sadness, surprise, disgust, anger, and fear (full score = 20) using cards with different cartoon facial expressions similar to the computer graphics pictures (14), and they underwent a 5-m back-and-forth navigation test (2) before and after surgery. Our preliminary examination showed that 11 healthy subjects (mean age = 50.4 y) scored more than 28 on the MMSE, scored 20 on the affect test, and took less than 10 s in the back-and-forth walk (data not shown).
Scanning Procedures
Each patient underwent a morphologic MRI study twice before and after shunting using a static magnet (0.3-T MRP7000AD; Hitachi) with 3-dimensional mode sampling (acquisition parameters: repetition time/echo time, 200/23; 75° flip angle; 2-mm slice thickness with no gap; 256 × 256 matrices) to evaluate the volumetric changes of the ventricles and to determine the striatal nuclei for setting the regions of interest (ROIs). After the second MRI after surgery, the altered flow of CSF in the VP shunt system was reset to presurgery levels.
The detail of the PET procedure was also described elsewhere (5). In brief, PET was performed using a high-resolution brain-purpose PET camera (SHR12000, Hamamatsu Photonics K.K.; 24 detector rings yielding 47 slices simultaneously; spatial resolution, 2.9 mm; full width at half maximum, 163-mm axial field of view) (15), which acquired imaging data parallel to the anterior commissure–posterior commissure line. After the filtered backprojection (Hanning filter), the reconstructed image resolution became 6.0 × 6.0 × 3.2-mm full width at half maximum, and each resulting voxel measured 1.3 × 1.3 × 3.4 mm. In the first PET study, after acquiring the transmission scan for attenuation correction, serial dynamic scans and periodic arterial blood sampling were performed for 62 min after a slow bolus injection (5-mL total volume) of 370 MBq 11C-raclopride with a specific activity of more than 37 GBq/μmol. Additional arterial blood samples were collected for determination of radioactive metabolites used in a model-based estimation of the binding potential (BP) of the tracer. One month after VP shunting, the second postsurgery PET was performed in the same way as in the first scan except for omission of arterial blood sampling.
Data Analysis
In MRI analysis, we first tested whether postsurgery morphologic changes in the ventricles were present in the MR images on the basis of a previous method (5). Briefly, we measured the degree of the ventricular dilatation as an Evans' index (16) and the size of the frontal horn of the lateral ventricle (17) on the MR images.
In PET analysis, multiple irregular ROIs were drawn bilaterally over the nucleus accumbens, the ventromedial striatum (head of the caudate), the inferolateral (ventral putamen) and superodorsal parts (dorsal putamen) of the striatum, and the cerebellum on the MR images (18). These ROIs were then transferred onto the corresponding dynamic 11C-raclopride images with 6.8-mm slice-thickness data generated after adding 2 consecutive slices using image-processing software (Dr View; Asahi Kasei Co.) on a Sun workstation (Hypersparc ss-20; Sun Microsystems) (19). A morphologic change in the brain due to a variety of ventricular enlargement may cause an error of parameter estimation because of the partial-volume effect. However, the ROI method using individual MRI minimizes the error and the pitfalls of applying a standardized normal brain template to the anatomically distorted NPH brain (20,21). The BP for 11C-raclopride was estimated on the basis of the invasive Logan graphical analysis in the first PET study and on its noninvasive analysis in the second PET study, in which the rate constant k2 was assumed to be the same value as k2 estimated in the first model (22,23). Percentage differences (%Δ) in BP and psychobehavioral scores between preoperative and postoperative conditions were calculated as follows: %Δ = (postoperative – preoperative)/preoperative × 100.
Statistical Analysis
To test changes in MR morphometric measures and BPs after shunting, the 2-tailed, paired Student t test was used. Psychobehavioral scores between conditions were compared using a 1-tailed, paired Student t test. Spearman rank correlation was tested between psychobehavioral scores and BPs in each region. The significance level for all statistics was defined as a P value < 0.05.
RESULTS
Psychobehavioral Changes After Shunting
As shown in Table 1, there was significant improvement in the navigation time scores (%Δ = 18.8% ± 6.5%) and the affect scores (%Δ = 5.4% ± 3.7%) (P < 0.05, paired t test). A slight increase was found in the MMSE scores (%Δ = 2.6% ± 3.6%) but not in the micturition scores (%Δ ≈ 0%) after shunting. No patients had postoperative deterioration in their daily activities.
Morphometric Measures
As shown in Table 2, MRI-based morphometric measures did not show any significant changes in size, although a slight tendency for reduction in the lateral ventricles was observed (about 6% reduction).
MRI-Based Morphometric Changes After Shunting
11C-Raclopride BPs
As shown in Table 3, the paired Student t test showed that the levels of BPs for 11C-raclopride were significantly higher in the nucleus accumbens bilaterally, dorsal putamen bilaterally, and left ventral putamen after shunting (P < 0.05).
Changes in BP for 11C-Raclopride Before and After Shunting
Correlation Between In Vivo Parameters and Clinical Improvement
Spearman rank correlation analysis showed a significantly positive correlation between percentile changes (%Δ) in 11C-raclopride BP after surgery in the left nucleus accumbens and the affect score (Fig. 1A, y = 2.76x + 0.71, r2 = 0.43), and a more robust correlation between the changes in the dorsal putamen and the navigation time (Fig. 1B, right: y = 0.78x − 6.23, r2 = 0.56; left: y = 1.23x − 8.62, r2 = 0.45). In addition, the averaged 11C-raclopride BP change in the whole striatum was found to correlate positively with a rise in the MMSE scores (Fig. 1C, right: y = 2.51x + 1.71, r2 = 0.62; left: y = 2.68x + 5.16, r2 = 0.46).
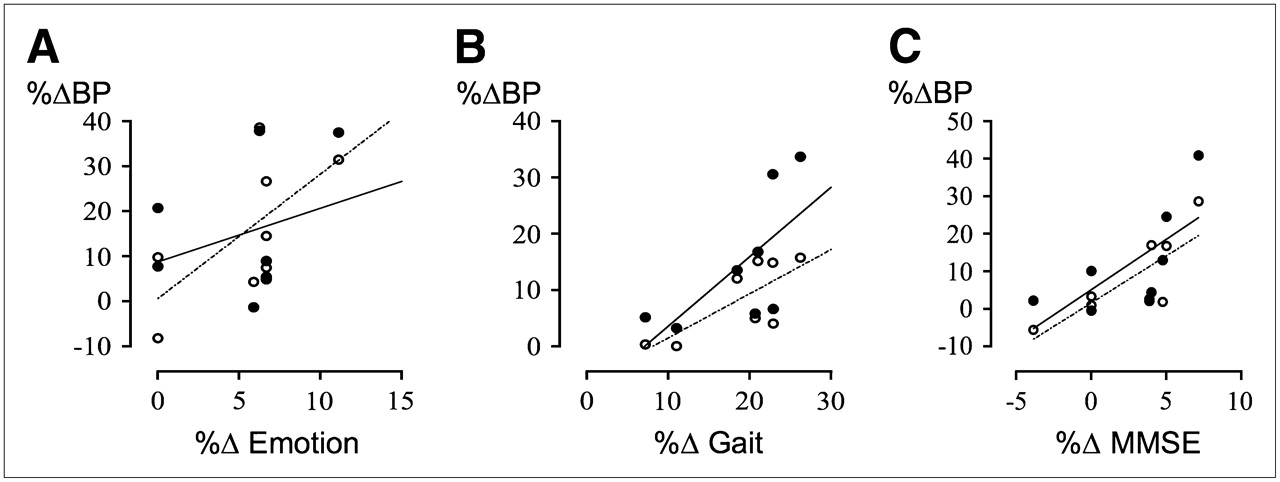
Correlations of emotional cognition changes with 11C-raclopride BP changes in nucleus accumbens (A), of navigation time changes with those in dorsal putamen (B), and of MMSE score changes with those in whole striatum (C) on right (○, dotted line) and left (•, solid line) side of brain.
DISCUSSION
This study shows that D2 receptor availability was enhanced by VP shunting in iNPH and that this increase was associated with clinical improvements in gait and cognition, which are characteristically compromised in this disease. This resiliency of D2 receptor availability in iNPH may be an explanation for the observed clinical recovery, especially in gait performance and emotional drive. Because of this recovery, iNPH may be referred to as a “treatable dementia.”
The reduction in 11C-raclopride binding at baseline in iNPH may be explained by 2 mechanisms: downregulation or loss of D2 receptors. Although the elevation of endogenous synaptic dopamine competes with 11C-raclopride binding and reduces its PET signal (23,24), a significant increase in dopamine release was unlikely in the present study because the basal level of the presynaptic marker 11C-2β-carbomethoxy-3β-(4-fluorophenyl) tropane (11C-CFT) does not change in iNPH patients (5) and because the content of a monoamine metabolite, homovalinic acid, is reportedly lower in ventricular CSF (25). Considering that the D2 receptor is involved in relaying motor information from the cortex (26), downregulation of D2 receptor is a more likely explanation for the observed reduction of 11C-raclopride binding. Because the level of glutamate is reportedly elevated in the ventricular CSF of the hydrocephalic brain (27), it is possible that long-term excitability caused by excessive glutamate in the cortex perturbs dopamine release in the striatum (28), leading to downregulation of the postsynaptic D2 receptor and attenuation of D2 receptor function. One report on humans suggesting the presence of a metabolically hyperactive condition in the hydrocephalic brain (29) is in line with this cerebral excitability. In addition to this functional alteration theory, the loss of axons in the white matter (30), the reduced number of the rat striatal cholinergic neurons (31), and the finding that PD-like extrapyramidal signs were seen in D2 receptor–lacking knockout mice (32) all support the possibility of DA neuronal loss. Therefore, downregulation or loss of D2 receptors may be significantly involved in the impairment of corticostriatal neuronal transmission in iNPH.
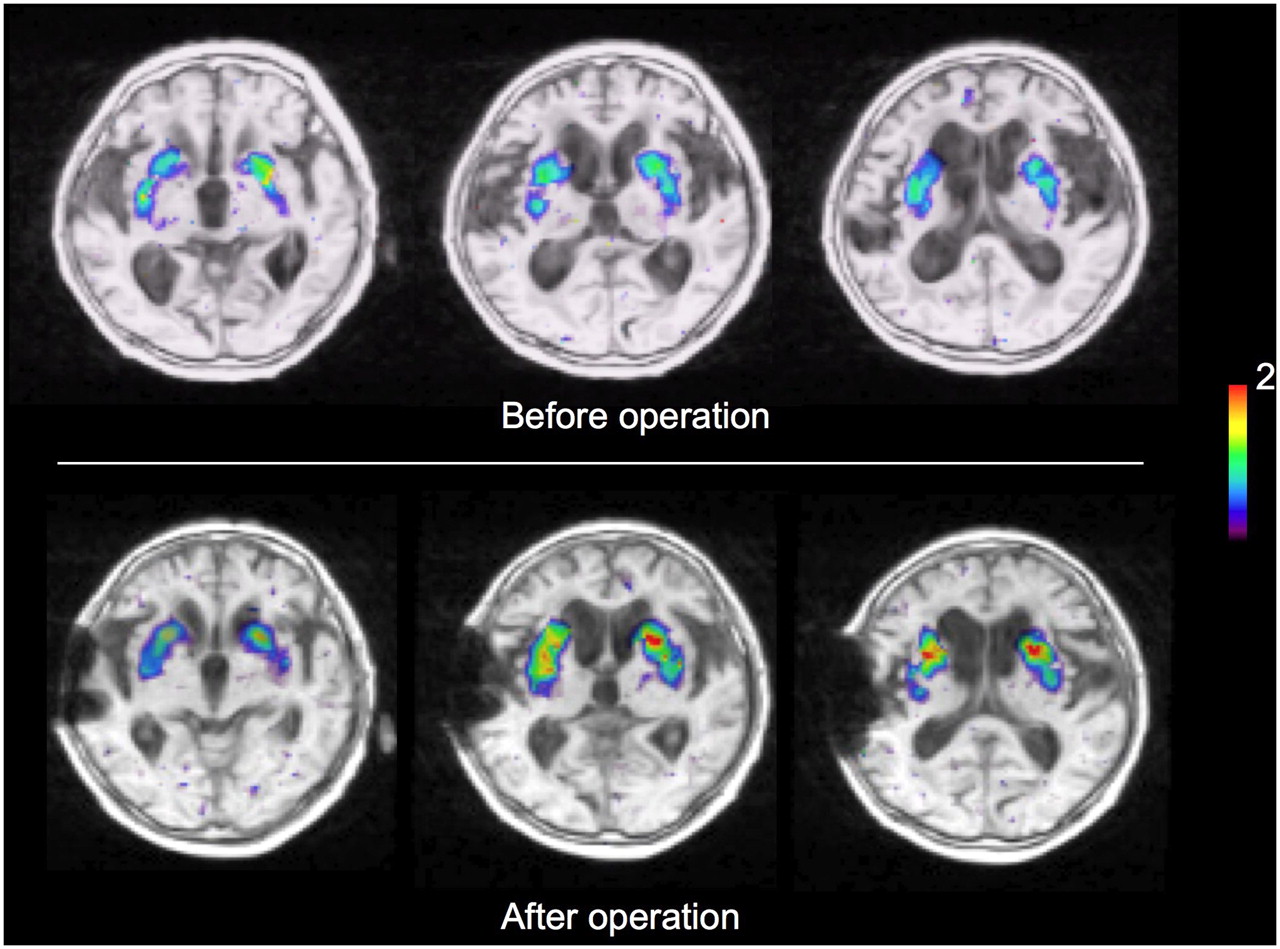
In the present study, iNPH D2 receptor downregulation was attenuated at 1 mo after VP shunt surgery (Fig. 2 illustrates an example of this phenomenon). A previous PET study showing significant increases of glucose metabolism in the cerebral cortical areas after surgery in iNPH (7) and a microdialysis study showing a postoperative reduction in the glutamate content of the cerebral cortex in iNPH patients (33) indicate that VP shunting may augment cortical neuronal activities partly by inhibiting neurotoxic effects in the cerebral cortex. This, in turn, could have stimulated dopamine release (28) and enhanced the activity of the D2 receptor in the striatum in the present study. Postoperative recovery of gait and emotion were related to the responsiveness of regional D2 receptor in the striatum, which was in line with findings that the dorsal putamen is involved in foot movement (23,34) and the nucleus accumbens is involved in higher motivation processing (35). The presence of variations of CSF dopamine metabolite content in responders and nonresponders to shunting (36) suggests a varying degree of stimulation of postsynaptic dopamine neurons after shunting.

PET/MRI fusion parametric images of quantitative 11C-raclopride BP in an iNPH patient before and after shunting. Color bar denotes BP for 11C-raclopride (0–2).
The limitation of the present study is the observation of PET and clinical variables at one time point. It was reported that patients continued to improve for up to 24 mo, and about half of the initially improved patients had subsequent deterioration (37). This indicates that the time of our study was within the period of brain plasticity in progress, possibly potentiated by shunting. In this respect, additional PET with 11C-raclopride may be of great value for further clarification of changes in D2 receptor availability during clinical deterioration in the decision of reintroduction of shunt surgery.
CONCLUSION
In summary, we show regional upregulation of postsynaptic D2 receptors concomitant with clinical improvement 1 mo after VP shunting of iNPH patients. Therefore, the D2 receptor might be a potential therapeutic target in iNPH.
Acknowledgments
We thank Toshihiko Kanno, Masami Futatsubashi, and Yutaka Naito for their contributions to the PET procedure and tracer synthesis. This research was supported by Health and Labor Sciences Research grants.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication July 17, 2007.
- Accepted for publication September 6, 2007.





{kind=link}
{kind=link}