


Abstract
The purpose of this study was to investigate whether 18F-FDG PET/CT is useful for localizing dystonic cervical muscles in patients with idiopathic cervical dystonia (ICD) by comparing disease severity before and disease severity after botulinum toxin (BT) injection into hypermetabolic muscles. Methods: Six patients with ICD underwent 18F-FDG PET/CT. Dystonic muscles suitable for BT injection therapy were defined as those showing diffusely increased 18F-FDG uptake. Results: Hypermetabolic cervical muscles were identified in all 6 patients. In 2 patients who underwent PET/CT both in a supine position and in a sitting position during 18F-FDG uptake, abnormal hypermetabolic muscles were observed by PET/CT only when patients were in the sitting position with their heads and necks in the adopted abnormal involuntary posture. Symptoms were significantly improved in 4 patients who underwent BT injection therapy guided by PET/CT and who were clinically monitored. Conclusion: 18F-FDG PET/CT is potentially useful for identifying dystonic cervical muscles for BT therapy in patients with ICD.
Idiopathic (primary) cervical dystonia (ICD), sometimes referred to as spasmodic torticollis, is characterized by an abnormal head and neck posture attributable to involuntary tonic or phasic contractions of neck muscles (1). Various options are available for treating patients with ICD, and although no universally accepted treatment protocol exists, denervation with botulinum toxin (BT) is regarded as a first-line treatment for ICD (1,2). The efficacy of BT has been proven in double-blind placebo-controlled studies and open trials, in which BT was found to produce satisfactory relief of symptoms in over 70% of patients (3–5). However, 10%–30% of patients do not respond to BT injection therapy (3,4,6). Furthermore, abnormal head and neck posture is not completely relieved in some patients, despite symptomatic improvement (4). Although diverse causes may explain a poor response or nonresponsiveness to BT, for example, contracture of neck muscles, an inadequate BT dose, and the development of neutralizing antibodies against BT, the poor localization of target muscles is a major cause of treatment failure (1,7). In other words, if BT is not injected into the majority of dystonic muscles or is injected into nondystonic muscles, treatment is likely to be ineffective.
Mapping based on needle electromyography (EMG) is the most widely used method for identifying dystonic muscles in ICD. Needle EMG can detect the abnormal firing of the motor unit action potentials of dystonic muscles (8,9). However, not every neck muscle can be explored with a needle electrode. For example, deep cervical muscles may be beyond reach with a conventional 37-mm needle electrode (10). In addition, accurate placement of the needle electrode tip into a muscle is often difficult in patients with a severe dystonic posture. Moreover, needle EMG is relatively invasive and may cause complications, such as bleeding and infection, and presents electrical hazards (11,12). Therefore, a more accurate, noninvasive method for the localization of dystonic muscles in ICD is necessary.
It is well known that glucose metabolism and 18F-FDG uptake are enhanced in contracting skeletal muscles (13–15); therefore, it was suggested that the degree of 18F-FDG uptake may be associated with the strength of contraction of skeletal muscles (13–15). Moreover, a recently developed integrated PET/CT method was found to provide both metabolic information and anatomic information on hypermetabolic lesions. Therefore, we considered that PET/CT may be able to localize dystonic muscles showing sustained contraction in ICD. In this preliminary study, we investigated whether 18F-FDG PET/CT is likely to be useful for localizing dystonic cervical muscles in ICD by comparing disease severity before and disease severity after BT injection into muscles that were identified as hypermetabolic by PET/CT.
MATERIALS AND METHODS
Subjects
The inclusion criteria used for this study were as follows: all subjects had ICD without any evidence of an identifiable cause of secondary dystonia; the extranuchal area was not affected by the dystonia; and the dystonic posture was not relieved despite conventional muscle relaxant therapy consisting of anticholinergics (trihexyphenidyl), benzodiazepines (clonazepam), and baclofen. From June 2005 to June 2006, 6 consecutive patients with ICD (all men; age [mean ± SD], 37 ± 16 y) visited our hospital, and all met the study criteria. Of these patients, 4 had a history of BT injections into dystonic muscles; these injections were administered on the basis of clinical findings at other institutes 3–6 mo before 18F-FDG PET/CT. None of these 4 patients had experienced relief of dystonic posture despite pain reduction in the nuchal area. The remaining 2 patients had no previous history of BT injection therapy. The ethics review committee at our institute approved the study protocol, and informed consent was obtained from all subjects after they were provided with a full explanation of the tests, procedures, and treatments used and of potential side effects.
18F-FDG PET/CT
All patients fasted for at least 6 h before the PET/CT study but were allowed water and muscle relaxant medications. To prevent nonspecific 18F-FDG uptake by muscles not related to ICD, muscle relaxants consisting of anticholinergics (trihexyphenidyl), benzodiazepines (clonazepam), and baclofen were administrated to all patients before PET/CT. PET/CT scans were performed with a Discovery LS PET/CT scanner (GE Healthcare). Whole-body CT from head to thigh was performed with a continuous spiral technique on an 8-slice helical CT scanner with the following parameters: 80 mAs (tube current [mA] × scan time [s]), 140 keV, 5-mm section width, and table feed rate of 5 mm per rotation. Next, an emission scan was performed from head to thigh at 4 min per frame at 45 min after the intravenous administration of 370 MBq of 18F-FDG. CT data were used for attenuation correction, and PET images were reconstructed with an ordered-subsets expectation maximization algorithm (28 subsets, 2 iterations). CT and PET scan data were accurately coregistered on an Xeleris workstation (GE Healthcare). Standardized uptake values (SUVs) were acquired from attenuation-corrected images, and the amount of 18F-FDG injected, patient body weight, and cross-calibration factors between PET and the dose calibrator were recorded. CT, PET, PET/CT, and maximum-intensity-projection PET images were reviewed by one nuclear medicine physician. When increased 18F-FDG uptake was observed in head and neck muscles, the maximum SUV and the name of each hypermetabolic muscle were recorded.
Clinical Evaluation and BT Therapy
To evaluate ICD severity, the Tsui Scale (0–25 points) and the Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS) were applied to each patient; measurements were taken in the sitting position by a single examiner before BT therapy (16–18). For the TWSTRS, the severity (0–35 points) and disability (0–30 points) subscales were used. The Tsui Scale and the TWSTRS were also applied after treatment by the same examiner.
Target muscles for BT therapy were selected on the basis of clinical evaluations, which included pattern of movement, visible and palpable muscle contractions, and PET/CT findings. We assumed that the degree of 18F-FDG uptake in cervical muscles correlated with the severity of ICD. In other words, the maximum SUV of each cervical muscle was used as the major criterion for selecting a target muscle. Because BT is very expensive and its maximum permitted dose per injection is limited, the following hypermetabolic muscles were excluded as targets for BT therapy: longus capitis muscle (percutaneous injection of BT is technically impossible); suboccipital small muscles, such as obliquus capitis superior muscle and rectus capitis posterior major and minor muscles (considering their small size and alleged muscle actions, the influence of these muscles on dystonic posture may be small); and semispinalis capitis/cervicis muscles, trapezius muscle, and scalene muscle (considering their alleged muscle actions and relatively low SUVs, the influence of these muscles on dystonic posture may be small). The hypermetabolic obliquus capitis inferior muscle was considered a target muscle because it is already known to be one of the common dystonic muscles in ICD.
BT injections into target muscles were performed with a Teflon (DuPont)-coated monopolar needle electrode cannula guided by EMG. For deep cervical muscles adjacent to a major artery or the major nerve trunk (e.g., obliquus capitis inferior and longus colli muscles), BT was injected under CT or ultrasonographic guidance.
RESULTS
Patient clinical characteristics are summarized in Table 1. Three patients had pure rotational torticollis, and the other 3 patients had laterocollis in addition to rotational torticollis. Anterocollis was also seen in 2 patients. Dystonic head rotation was the most prominent and most disabling symptom in all patients.
Patient Clinical Characteristics
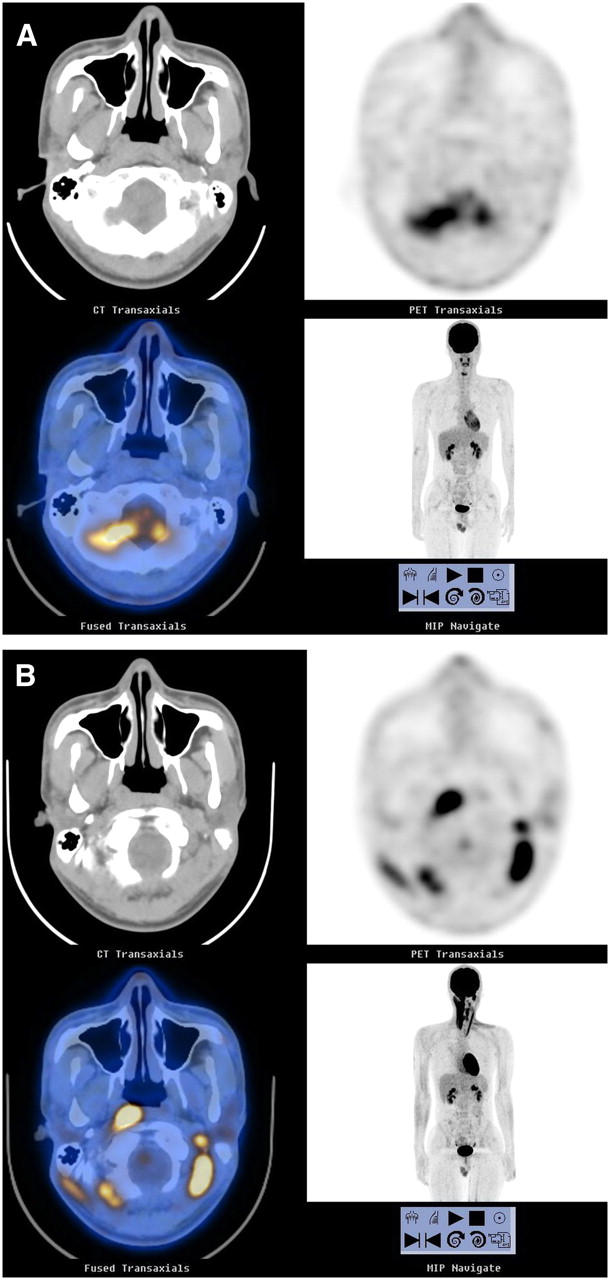
Table 2 shows the 18F-FDG PET/CT results and responses to BT therapy. At the time of PET, patients 1–5 were in the supine position during the 18F-FDG uptake period. Although abnormal 18F-FDG uptake was observed in the cervical muscles of patients 1–3, no significant abnormal 18F-FDG uptake was observed in the cervical muscles of patients 4 and 5. 18F-FDG PET/CT was repeated in patients 4 and 5 while the patients maintained a sitting position with their heads and necks in the adopted abnormal involuntary posture during the 18F-FDG uptake period without making any effort to correct this posture. Abnormal 18F-FDG uptake was observed in the cervical muscles of these 2 patients during repeat PET/CT (Fig. 1). Patient 6 was in a sitting position during the 18F-FDG uptake period. Overall, increased 18F-FDG uptake in cervical muscles was observed in all 6 patients.
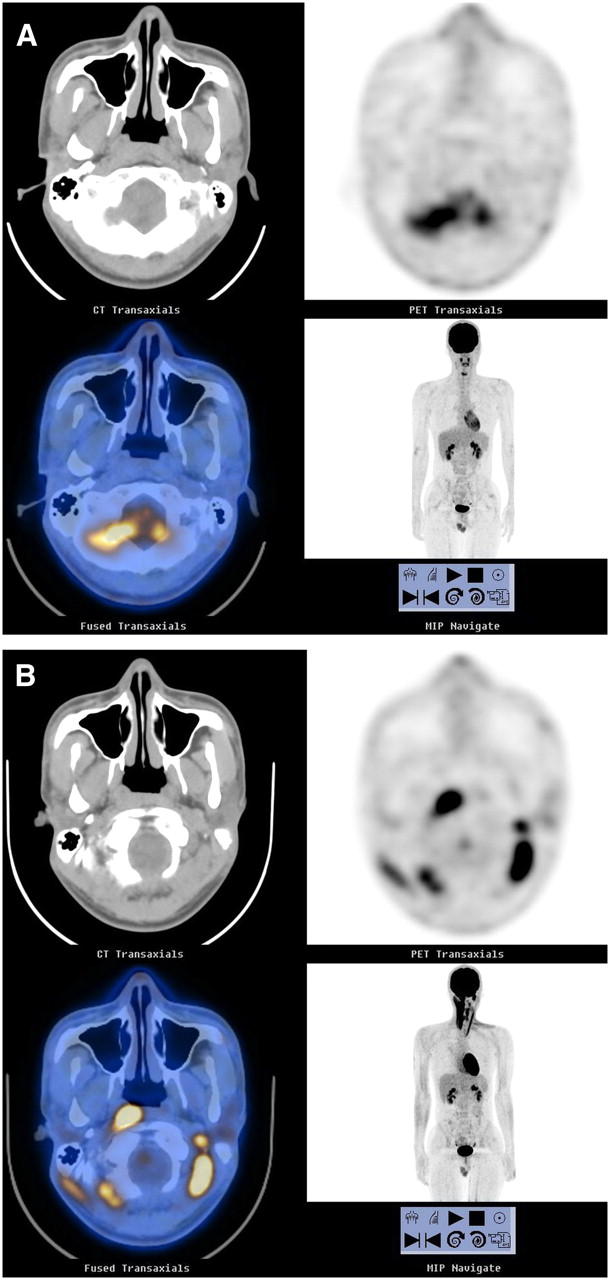
PET/CT images of 21-y-old male patient with right-side cervical dystonia (patient 5). (A) Initial PET/CT performed in supine position during 18F-FDG uptake period, showing no significant abnormal uptake in cervical muscles. (B) Repeat PET/CT performed in sitting position during 18F-FDG uptake period, showing significant abnormal uptake in bilateral cervical muscles. MIP = maximum intensity projection.
Results of 18F-FDG PET/CT and Response to BT Injection Therapy
The number and mean maximum SUVs (mean ± SD) of hypermetabolic cervical muscles were 9.3 ± 3.5 per patient (range: 5–13) and 5.6 ± 2.7 (range: 2.3–15.9), respectively (Table 2). For all hypermetabolic muscles, increased 18F-FDG uptake was observed throughout almost the entire muscle area. The most commonly encountered hypermetabolic cervical muscles were the ipsilateral splenius capitis and obliquus capitis inferior muscles, and these were affected in all 6 patients. The second most commonly observed hypermetabolic cervical muscles were the ipsilateral longus capitis muscle and the contralateral sternocleidomastoid and obliquus capitis superior muscles, which were affected in 5 patients.
In 2 patients, follow-up Tsui Scale and TWSTRS administrations were not possible because of BT therapy refusal (patient 4) and follow-up loss (patient 6). In the remaining 4 patients who underwent BT therapy guided by PET/CT, symptoms were significantly improved, according to reductions in the Tsui Scale scores (from 10.0 ± 2.9 to 1.8 ± 1.3, an 82% reduction) and TWSTRS scores (severity: from 21.3 ± 2.1 to 5.8 ± 5.3, a 73% reduction; disability: from 19.8 ± 1.9 to 3.8 ± 3.8, an 81% reduction) (Table 2). In patient 1, symptoms were completely relieved after BT therapy. Follow-up PET/CT after BT therapy was available for patient 3 and showed a significant reduction in metabolism in BT-treated muscles (Fig. 2).

PET/CT images of 42-y-old male patient with left-side cervical dystonia (patient 3). (A) Abnormal diffuse 18F-FDG uptake was observed in left longus colli muscle on initial PET/CT images (maximum SUV = 6.8). (B) After BT injection into this muscle, symptoms improved. 18F-FDG uptake of left longus colli muscle was also markedly reduced on follow-up PET/CT images (maximum SUV = 2.6). MIP = maximum intensity projection.
DISCUSSION
Our preliminary results suggest that 18F-FDG PET/CT is useful for localizing dystonic cervical muscles in patients with ICD. PET/CT enabled the visualization of abnormal hypermetabolic muscles in all 6 subjects. Furthermore, all 4 patients with ICD who underwent PET/CT-guided BT injection therapy experienced a significant improvement in symptoms, according to the Tsui Scale and the TWSTRS; in 3 of these patients, previous BT injection therapy guided by clinical findings had failed. These findings support the notion that hypermetabolic muscles observed by 18F-FDG PET/CT can be considered target muscles for BT injection therapy in patients with ICD.
In the present study, PET/CT failed to localize hypermetabolic cervical muscles in 2 of 5 patients (40%) in the supine position during the 18F-FDG uptake period. However, hypermetabolic cervical muscles were observed in all 3 patients in the upright sitting position during the 18F-FDG uptake period, even though their heads and necks remained in the adopted abnormal involuntary posture. These results suggest that the sitting position with an abnormal dystonic posture during tracer uptake may improve PET/CT sensitivity over that obtained with the supine position.
At rest, skeletal muscle accumulation of 18F-FDG is relatively low. However, even in healthy subjects, variable uptake may be observed in head and neck muscles because of stress-induced muscle tension. The characteristic appearance of this normal physiologic 18F-FDG uptake in cervical muscles is symmetric uptake in bilateral posterior cervical and bilateral trapezius muscles (19). In the present study, we administered muscle relaxants before 18F-FDG injection to prevent nonspecific muscle uptake because of stress-induced muscle tension. However, although the use of muscle relaxants may prevent widespread symmetric cervical muscle uptake, 18F-FDG uptake not related to stress-induced muscle tension may be encountered in some muscle groups, such as the sternocleidomastoid and trapezius muscles, in healthy subjects; however, uptake in these muscles is usually limited to muscular insertion sites (20). In the present study, 18F-FDG uptake by cervical muscles was asymmetric and unilateral and involved almost the entire muscle area. In addition, we instructed every patient to keep the head and neck still during the 18F-FDG uptake period. Therefore, the hypermetabolic character of the cervical muscles observed in the present study can be interpreted as being a result of involuntary active contraction.
Involuntary active contraction of cervical muscles may not be attributable to true dystonic activity, as it may be caused by a compensatory reactivity to dystonic contraction. To reduce the likelihood of this possibility, we instructed patients not to attempt to correct their abnormal involuntary postures during 18F-FDG uptake periods. Thus, although some unintentional compensatory contraction may have occurred during 18F-FDG uptake periods, we believe that the influence of any compensatory contraction on 18F-FDG accumulation in cervical muscles likely was slight and that the hypermetabolic cervical muscles located by PET/CT reflected the actively contracting dystonic muscles responsible for ICD. In addition, we presumed that the degree of 18F-FDG uptake by cervical muscles was correlated with the severity of ICD, because severely contracting dystonic muscles use more glucose. We used the maximum SUVs of hypermetabolic muscles as the criterion for target muscle selection; with this strategy, all 4 patents treated with BT injections achieved significant symptomatic improvement.
Our study has several limitations. First, the number of subjects enrolled was too small to prove the usefulness of PET/CT in patients with ICD. Only 2 patients underwent PET/CT both in the supine position and in the sitting position during the 18F-FDG uptake period. Further study of a larger number of subjects is necessary to determine the influence of patient position and posture during the 18F-FDG uptake period. In addition, no patient enrolled in the present study had pure laterocollis or anterocollis/retrocollis. Second, muscle denervation caused by prior BT injections before PET/CT may have influenced our results, as it may have prevented PET/CT detecting dystonic muscles. Third, BT therapy was successful in 3 patients for whom previous BT therapy at other institutes had failed. Besides the use of PET/CT, we cannot exclude the possibility that other factors, such as differences in BT injection skill, doses of BT, and effect of repetitive BT therapy, may have affected our results. Fourth, we did not compare PET/CT and EMG mapping as techniques for finding dystonic muscles in patients with ICD. Because our initial purpose was not a comparison between PET/CT and EMG mapping, most baseline EMG mapping was performed before PET/CT scanning, and the only routinely examined muscles were the splenius capitis, sternocleidomastoid, and upper trapezius muscles. Further controlled study comparing PET/CT with EMG mapping in ICD is required.
CONCLUSION
The present study suggests that 18F-FDG PET/CT is potentially useful for identifying dystonic cervical muscles in ICD patients and that this identification leads to satisfactory clinical results after intramuscular BT treatment. In addition, our findings indicate that optimal patient posture and position during tracer uptake may improve PET/CT sensitivity in terms of identifying dystonic muscles. The ability of PET/CT to localize both superficial and deep cervical muscles and the noninvasiveness of PET/CT favor its use for the evaluation of ICD versus needle EMG. Further prospective studies with large numbers of subjects are needed.
Acknowledgments
This study was supported by the Korean Health 21 R&D Project, Ministry of Health and Welfare, Seoul, Republic of Korea (02-PJ3-PG6-EV06-0002).
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication June 14, 2007.
- Accepted for publication August 23, 2007.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.