


Abstract
We evaluated the diagnostic usefulness of combination studies with a statistical mapping method in N-isopropyl-p-123I-iodoamphetamine (123I-IMP) brain perfusion SPECT, cardiac sympathetic nerve function by 123I-metaiodobenzylguanidine (123I-MIBG), and myocardial function by electrocardiographically gated 99mTc-sestamibi (99mTc-MIBI) SPECT for patients with probable or possible dementia with Lewy bodies (DLB). Methods: Twelve patients with probable DLB (7 male, 5 female; mean age ± SD, 72.3 ± 5.63 y; range, 65–82 y) and 9 patients with possible DLB (3 male, 6 female; mean age ± SD, 73.1 ± 9.23 y; range, 59–88 y) were enrolled in this study. 123I-IMP SPECT images were analyzed with 3-dimensional stereotactic surface projections (3D-SSP) and the severity of ischemia was classified objectively using quantitatively analytic and display software; stereotactic extraction estimation (SEE) methods were compared with a normal database. In addition, we evaluated 123I-MIBG heart-to-mediastinum (H/M) uptake ratios. Moreover, we performed 99mTc-MIBI SPECT to evaluate myocardial perfusion and the left ventricular ejection fraction (LVEF) compared with a normal database. Results: 3D-SSP images of group comparison with healthy control subjects showed significantly decreased perfusion in the parietotemporal, occipital cortex, posterior cingulated, and precuneus regions in the probable DLB group but no significant reduction in the possible DLB group. Mean H/M ratios in the probable DLB group were significantly lower than those of the possible DLB group and the control group, respectively. Ten of 12 patients (83.3%) with probable DLB and 1 of 9 patients (11.1%) with possible DLB showed severe reduction in the bilateral occipital lobe and also a low 123I-MIBG uptake. One patient (8.3%) with probable DLB and 2 patients (22.2%) with possible DLB showed no bilateral occipital hypoperfusion but showed low 123I-MIBG uptake. One patient (8.3%) with probable DLB and 6 patients (66.7%) with possible DLB showed no occipital hypoperfusion and normal 123I-MIBG uptake. 99mTc-MIBI gated SPECT did not indicate any wall motion abnormality in any subjects. Conclusion: These results suggest that combined examination of cerebral blood flow with 3D-SSP and SEE analysis, and cardiac sympathetic nerve function with 123I-MIBG, would be a useful supporting diagnostic method in patients with DLB—particularly, in possible DLB and when cerebral blood flow does not indicate occipital hypoperfusion.
- dementia with Lewy bodies
- 3-dimensional stereotactic surface projection
- 123I-MIBG
- 99mTc-MIBI
- gated SPECT
Dementia with Lewy bodies (DLB) has become the second most common type of degenerative dementia next to Alzheimer's disease (AD) (1). An international workshop proposed the first criteria for diagnoses of DLB in 1996 (2). According to these criteria, the core clinical symptoms identified are fluctuating cognition, recurrent visual hallucinations, and spontaneous motor features of parkinsonism, and the distinction between probable and possible DLB is defined, as 2 core features are sufficient for a diagnosis of probable DLB and just 1 feature is required for possible DLB. An accurate and early diagnosis of DLB is important from its viewpoint of adequate prognosis and therapy. In fact, there is some evidence that DLB patients respond positively to treatment with cholinesterase inhibitors (3), whereas neuroleptic medications can induce life-threatening extrapyramidal reactions (4). However, the differential diagnosis of DLB in contrast with other degenerative diseases such as Parkinson's disease (PD), AD, and vascular dementia may not be feasible because of those clinically overlapping symptoms, especially in the case of possible DLB. The reported sensitivity rates for a clinical diagnosis of probable DLB have varied from 0.22 to 0.83 and the specificity from 0.79 to 1.0 (5–8).
Various kinds of imaging procedures and techniques such as conventional MRI, neuroimaging using SPECT, and PET have been used for objective diagnostic methods. In particular, the use of advanced statistical brain imaging analysis, such as 3-dimensional stereotactic surface projections (3D-SSP) and statistical parametric mapping (SPM), has detected occipital hypometabolism or hypoperfusion in DLB (9–13). Statistical mapping methods are excellent in terms of objectivity and reproducibility but do not provide clear anatomic information or the range and extent of an abnormal site in visual assessment of 3D images. In 3D-SSP methods, particularly, topography at the boundary of an abnormal area cannot be shown specifically, making it impossible to quantitatively assess the extent of lesions. On the basis of this limitation, Mizumura et al. developed the stereotactic extraction estimation (SEE) method that was able to identify orientation and increased reduction through classifying stereotactic brain coordinates according to the anatomic structure (14). Techniques for the statistical examination of cerebral blood flow have been developed, but the diagnostic accuracy for DLB using brain imaging is currently limited (11,12).
On the other hand, some reliable and clear evidence has been accumulating for the usefulness of 123I-metaiodobenzylguanidine (123I-MIBG) scintigraphy in the diagnosis of Lewy body disease, such as PD and DLB (15–17). Orimo et al. reported that cardiac sympathetic denervation is a consistent histopathologic feature of Lewy body disease (18).
This study had 2 objectives. One was to evaluate the diagnostic usefulness of combination studies of statistical mapping methods in N-isopropyl-p-123I-iodoamphetamine (123I-IMP) brain perfusion SPECT and cardiac sympathetic nerve function by 123I-MIBG for patients with DLB. To determine the significance of the comparison between occipital reductions in brain imaging and 123I-MIBG reductions in cardiac imaging, 2 different biomarkers for the diagnosis of DLB and pathophysiologic considerations were assessed. To our knowledge, only one study using the same combined methodology for probable DLB reported that 123I-MIBG myocardial scintigraphy might improve the sensitivity in the detection of DLB (19). We confirmed their findings, including not only probable DLB but also possible DLB, and compared the relative utility between probable and possible DLB in this study. Furthermore, we performed myocardial perfusion and function by electrocardiographically (ECG) gated 99mTc-sestamibi (99mTc-MIBI) SPECT studies to examine whether myocardial perfusion and contractility would be reduced by denervation for DLB.
MATERIALS AND METHODS
Subjects
Twelve patients with probable DLB (7 males, 5 females; mean age ± SD, 72.3 ± 5.63 y; range, 65–82 y) and 9 patients with possible DLB (3 males, 6 females; mean age ± SD, 73.1 ± 9.23 y; range, 59–88 y) were enrolled in this study between October 2004 and December 2005. Patients and their clinical features are summarized in Table 1. The diagnosis of probable or possible DLB was made clinically according to the criteria reported in 1996 by the Consortium of DLB (2). The onset of dementia and parkinsonism in all patients was shown within 1 y (2). On the basis of this definition, all probable DLB patients in our study were regarded clinically as DLB, not as PD with dementia. The severity of dementia was assessed using the Mini-Mental State Examination (MMSE), whereas the severity of motor disability was determined according to the staging of Hoehn and Yahr (Hoehn–Yahr). The mean MMSE score were 21.1 ± 4.8 in the probable DLB group and 17.1 ± 7.2 in the possible DLB group. Fluctuation was evaluated using the Clinician Assessment of Fluctuation scale (20). The studies were performed prospectively, and fully informed consent was obtained; all patients or their families agreed to undergo all examinations and participate in this study. All patients had a normal resting ECG and chest radiography, and no patients had any clinical evidence of cardiac disease or cerebral infarction. All patients underwent MRI of the brain, which was used for differential diagnosis.
Clinical Features of Patients with Probable and Possible DLB
Ten subjects (5 male, 5 female; mean age ± SD, 63.3 ± 6.1 y; range, 52–71 y) who underwent 123I-IMP SPECT at Fujita Health University and retrospectively had normal perfusion and almost no reduced (Z score < 1) area in 3D-SSP analysis were selected for the healthy control subjects of the 123I-IMP study. Six subjects (2 male, 4 female; mean age ± SD, 76.2 ± 11.3 y; range, 56–90 y) who underwent 123I-MIBG and 99mTc-MIBI studies at Fujita Health University and had normal early and delayed heart-to-mediastinum (H/M) uptake ratios on 123I-MIBG planar image (123I-MIBG SPECT demonstrated normal myocardial accumulations visually and 99mTc-MIBI SPECT demonstrated normal myocardial accumulations and normal left ventricular ejection fraction [LVEF] in gated SPECT, retrospectively), and had normal ECG and chest radiography, were selected for healthy control subjects. The healthy control subjects of the 123I-IMP studies and the cardiac studies were different. This research was approved by the Ethical Review Board of Fujita Health University, School of Medicine. We have performed the following image studies—123I-IMP, 123I-MIBG, and 99mTc-MIBI—only for the patients with suspected probable or possible DLB.
123I-IMP Brain SPECT
For approximately 15 min, we performed SPECT data collection (2 s/step, 30 steps, 5 angles, 3 repeats) 15 min after intravenous injection of 222 MBq (6 mCi) of 123I-IMP (patient in quiet room with eyes closed). The matrix size was 128 × 128, and the collection window was 159 keV (±10%). For prefilter and absorption correction, the Ramp–Butterworth filter (order 8, cutoff 0.50) and the radial postcorrection method were used, and images were reconstructed using the backprojection method. The image voxel size was 2 mm/pixel. The SPECT system used was a ring-type γ-camera (HEADTOME SET-080; Shimadzu Co.) with a general-purpose fanbeam collimator.
123I-MIBG Planar H/M Scintigraphy and 99mTc-MIBI Cardiac Gated SPECT
Planar and SPECT scans were performed with a dual-head γ-camera equipped with a low-energy, general-purpose collimator (ADAC Vertex-Plus; Hitachi). Within 1–2 wk before or after 123I-IMP SPECT, 99mTc-MIBI and 123I-MIBG were performed on the same day during quiet respiration without breath-holding. Each patient was not given any medications that have been reported to influence 123I-MIBG metabolism. 123I-MIBG anterior planar and SPECT images were obtained 20 min (early images) and 4 h (delayed images) after intravenous injection of 111 MBq (3 mCi) of 123I-MIBG. The acquisition time of the planar image was 360 s. The matrix size of the planar image was 256 × 256 and the SPECT image was 64 × 64, respectively, and the collection window was 157 keV (±10%). For prefilter and absorption correction, the Ramp–Butterworth filter (order 8, cutoff 0.45) was used. The image voxel size of the planar image was 1.64 mm/voxel and of the SPECT image was 5.12 mm/voxel, respectively. For 123I-MIBG SPECT studies, detectors were set up to form a 90° angle. Then, 1 h after an intravenous injection of 600 MBq (16.2 mCi) of 99mTc-MIBI, the anterior planar image, the non–ECG gated SPECT, and the gated SPECT data were collected. For SPECT studies, detectors were set up to form a 90° angle. Sixteen frames per cardiac cycle were acquired during 180° rotation in a 64 × 64 matrix from the 45° right anterior oblique projection to the 45° left posterior oblique projection, with each head performing a 90° rotation in the continuous acquisition mode.
Data Analysis
The obtained data from 123I-IMP SPECT images were analyzed with Neurostat/3D-SSP developed by Minoshima et al. using an image-analysis software, iSSP version 3.5 (21,22), and data were normalized to the mean global activity. Then we applied the analysis software, SEE, developed by Mizumura et al. (14). We divided the whole brain into segments according to SEE methods (level 2, lobe level classification; level 3, gyrus level classification) and assessed the extent of an abnormal region in each segment and the severity (14).
For 123I-MIBG images, we calculated the early and delayed H/M ratios with the regions-of-interest (ROIs) method on the anterior view of the planar image. An irregular circular ROI on the left ventricle was drawn manually and a square ROI was set on the upper mediastinum area (Fig. 1). When the 123I-MIBG accumulation in a heart was indistinct, we referred to an anterior planar image of the 99mTc-MIBI examination in the same patient. For 123I-MIBG SPECT images, we evaluated visually on short-axis, horizontal long-axis, and vertical long-axis views.
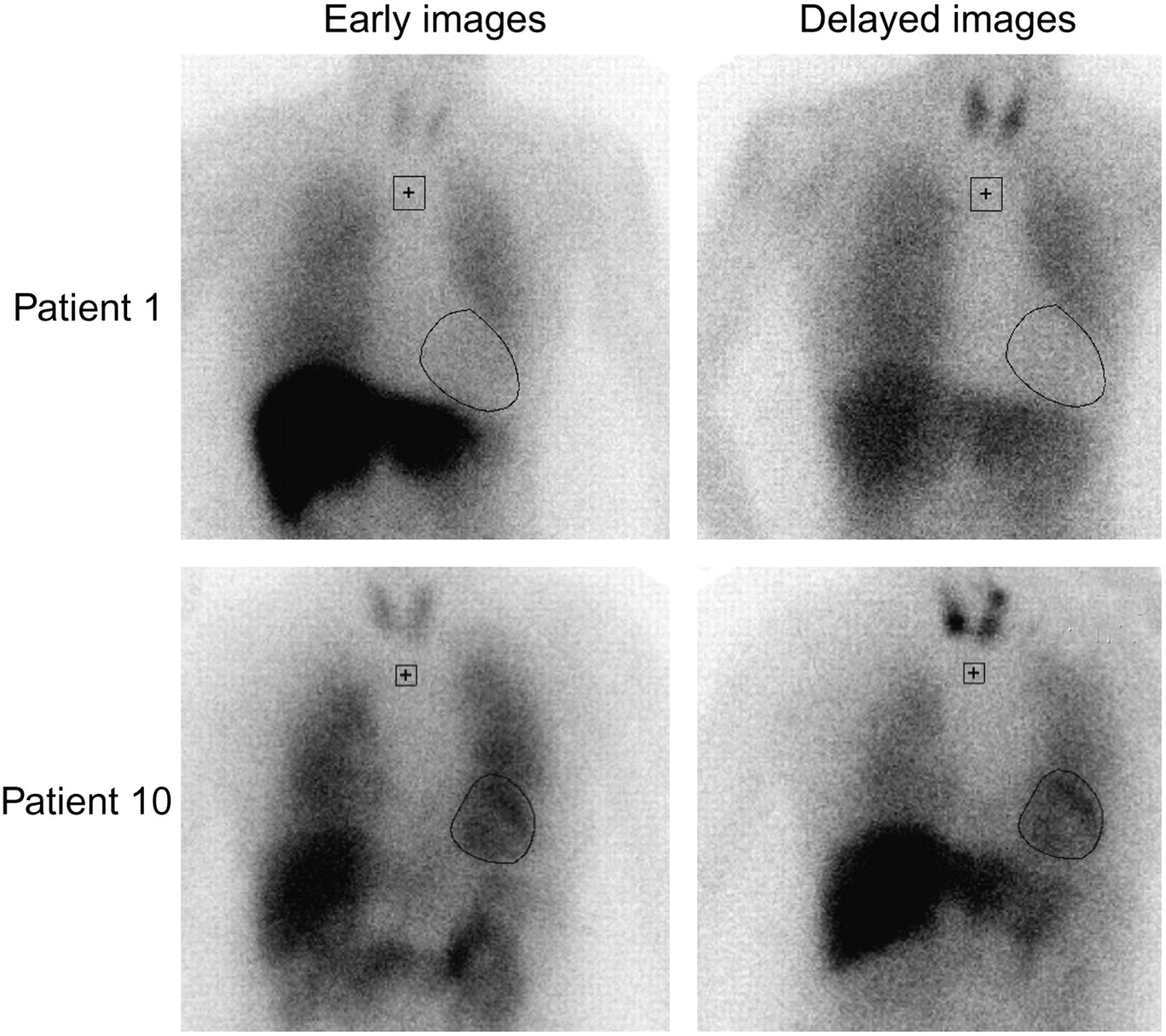
123I-MIBG images in early and delayed phase in 2 patients with probable DLB. Patient 1 shows low 123I-MIBG uptake in both images (H/M ratio: early, 1.33; delayed, 1.14). In contrast, patient 10 shows normal uptake in both images (H/M ratio: early, 2.05; delayed, 2.04).
For 99mTc-MIBI myocardial perfusion SPECT, we evaluated visually the same as for 123I-MIBG SPECT. The LVEF was calculated by ECG gated SPECT with a quantitative gated SPECT (QGS) program, which provides information about left ventricular wall motion (23).
Differences between 2 groups were compared by an unpaired t test. All data are expressed as the mean ± 1 SD value. The minimum level of significance was designated as P < 0.05.
RESULTS
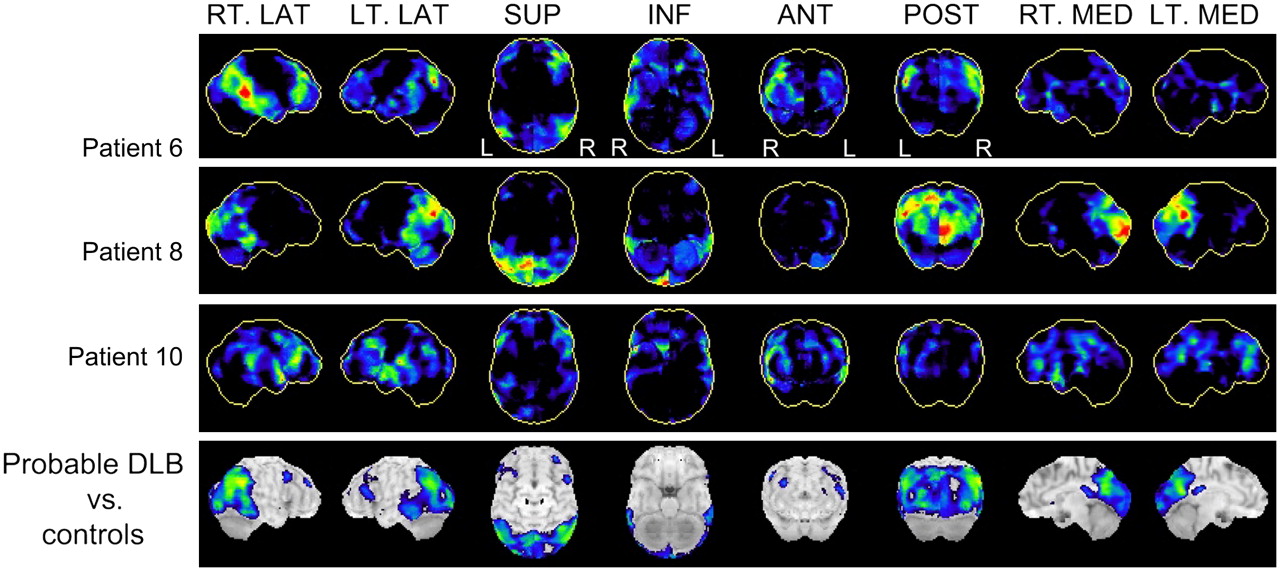
3D-SSP images of a group comparison between the probable DLB group and the healthy control subjects clearly demonstrated reduced perfusion in the parietotemporal, occipital cortex, posterior cingulated, and precuneus regions (Fig. 2). In the probable DLB group, 3D-SSP images of 10 patients, such as patient 8, revealed typical findings of DLB at occipital hypoperfusion (Fig. 2). 3D-SSP images of 1 patient (patient 6) showed moderate reduction of the frontal, parietal, and temporal lobes and mild-to-moderate reduction of the precuneus and posterior cingulate gyrus, but a mild reduction of the occipital lobe and the primary sensorimotor cortex was spared, so that this reduction pattern was considered as likely due to AD (Fig. 2). 3D-SSP images of another patient (patient 10) showed heterogeneous reduction of the whole brain cortex, so that this reduction pattern was considered as not likely to be a DLB pattern (Fig. 2). Table 2 shows the SEE results of 3 representative patients (patients 6, 8, and 10). This SEE result showed a high extent and severity of the occipital lobe, posterior cingulated, and precuneus gyrus in patient 8, whereas a low extent and severity of these regions is evident in patients 6 and 10.
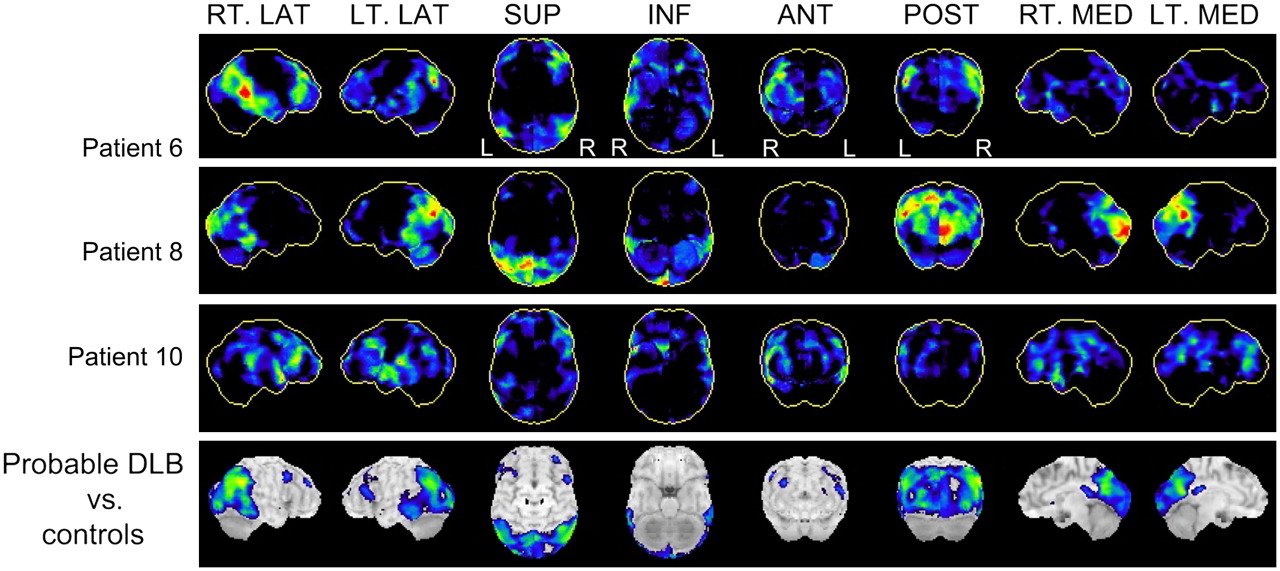
Representative 3D-SSP images of DLB (patient 8), 2 patients who demonstrated mild occipital hypoperfusion (patients 6 and 10), and group analysis between probable DLB group and healthy control subjects. 3D-SSP images of patient 6 show moderate reduction in frontal, parietal, and temporal lobes and mild-to-moderate reduction in precuneus and posterior cingulate gyrus, but mild reduction of occipital lobe, and primary sensorimotor cortex is spared so that this reduction pattern is considered as likely AD. 3D-SSP images of patient 8 show typical findings of DLB with occipital hypoperfusion. 3D-SSP images of patient 10 show heterogeneous reduction of entire brain cortex so that this reduction pattern is considered as not likely to be DLB pattern. 3D-SSP images of group comparison between the probable DLB group and healthy control subjects clearly demonstrated a reduction in parietotemporal, occipital cortex, posterior cingulated, and precuneus perfusion. RT.LAT = right lateral; LT.LAT = left lateral; SUP = superior; INF = inferior; ANT = anterior; POST = posterior; RT.MED = right medial; LT.MED = left medial.
SEE Results from 123I-IMP Analyses of 3 Patients with Probable DLB
Group comparison 3D-SSP images between the possible DLB group and healthy control subjects showed no significant reduction (Fig. 3). In the possible DLB group, 3D-SSP images of only 1 patient (patient 18) showed a typical DLB reduction pattern. Seven of 9 patients demonstrated no occipital hypoperfusion and the extent ratios and severity were low. One (patient 13) of these 7 patients showed moderate reduction in the frontal and temporal lobe, but not in other regions. This reduction pattern was considered as likely frontotemporal lobe dementia. Four patients, such as seen in patient 21, of these 7 patients showed severe reduction in the frontal, parietal, temporal lobes, precuneus, and posterior cingulate gyri, but no reduction in the occipital lobe, and the primary sensorimotor cortex was spared so that this reduction pattern was considered to be AD. One patient (patient 19) also exhibited a reduction pattern like AD, but unilateral mild occipital hypoperfusion was observed on the left side. Table 3 shows the SEE results of 4 representative patients (patients 13, 18, 19, and 21). This SEE result showed the high extent and severity of the bilateral occipital lobes in patient 18, whereas this appears in the unilateral occipital lobe in patient 19. The limited extent and severity of the occipital lobe were seen in patients 13 and 21.
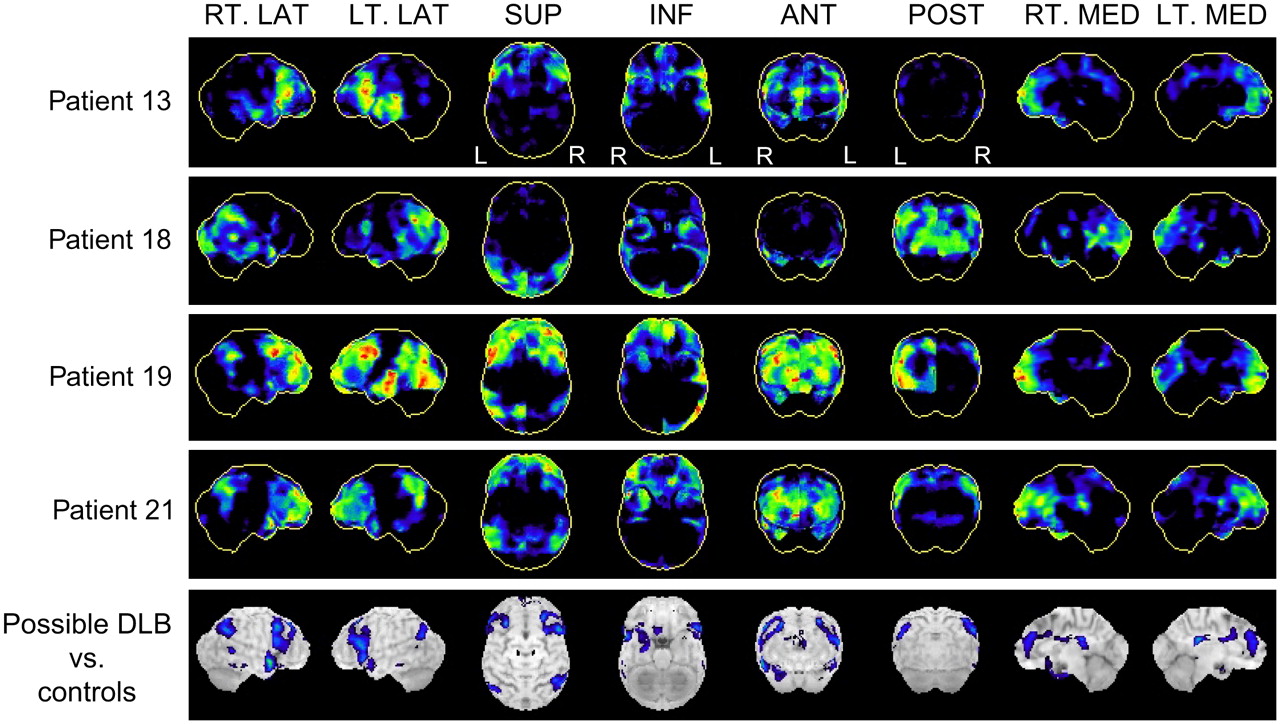
3D-SSP images of 4 patients with possible DLB and group analysis between possible DLB group and healthy control subjects. 3D-SSP images of patient 13 show moderate reduction in frontal and temporal lobe, but not other regions, so this reduction pattern is considered as likely frontotemporal lobe dementia. 3D-SSP images of patient 18 show typical reduction pattern of DLB. 3D-SSP images of patients 19 and 21 show severe reduction in frontal, parietal, and temporal lobes and mild-to-moderate reduction in precuneus and posterior cingulate gyrus, and primary sensorimotor cortex is spared so that this reduction pattern is considered as AD, but patient 19 shows unilateral mild occipital hypoperfusion on left side. 3D-SSP images of group comparison between possible DLB group and healthy control subjects show no significant reduction. RT.LAT = right lateral; LT.LAT = left lateral; SUP = superior; INF = inferior; ANT = anterior; POST = posterior; RT.MED = right medial; LT.MED = left medial.
SEE Results from 123I-IMP Analyses of 4 Patients with Possible DLB
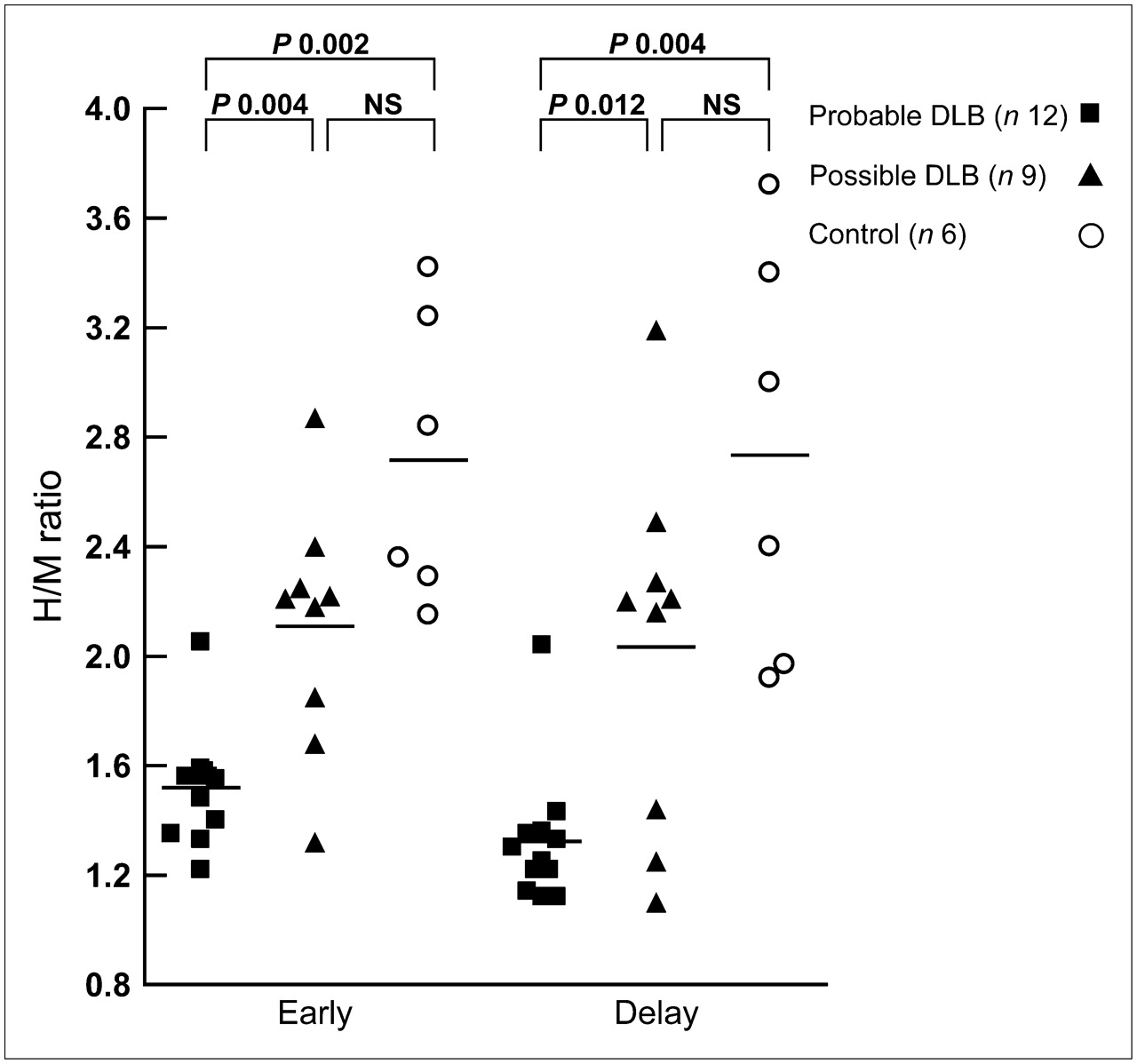
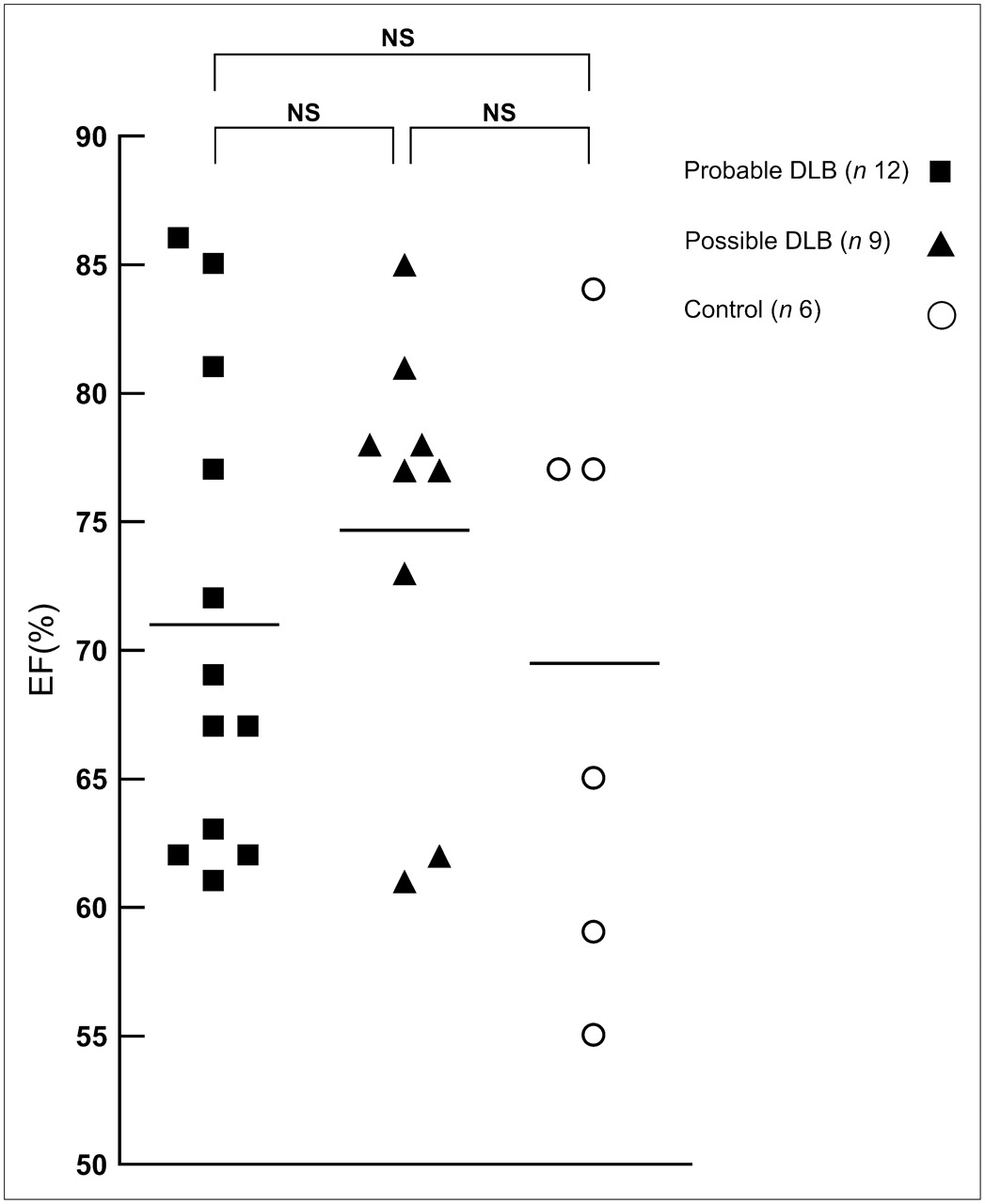
Table 4 provides a summary of 123I-MIBG and 99mTc-MIBI cardiac scintigraphy in patients with probable DLB. Both the early and delayed cardiac 123I-MIBG uptakes were markedly decreased in 11 of 12 patients except for 1 patient (patient 10) showing normal uptake in both images (Fig. 1). The mean early H/M ratio (1.52 ± 0.21) and delayed H/M ratio (1.32 ± 0.25) in the probable DLB group were significantly lower than those in the possible DLB group (early: 2.11 ± 0.45, P = 0.004; delayed: 2.03 ± 0.66, P = 0.012) and the control group (early: 2.72 ± 0.53, P = 0.002; delayed: 2.74 ± 0.75, P = 0.004), respectively (Fig. 4). 99mTc-MIBI myocardial SPECT determined there was no perfusion defect in any patient, and ECG gated SPECT also showed no wall motion abnormality of the entire LV. There was no significant difference between the probable DLB group (LVEF: 71.0% ± 9.15%) and the possible DLB group (LVEF: 74.7% ± 8.14%, P = 0.35) and the control group (LVEF: 69.5% ± 11.52%, P = 0.79), respectively (Fig. 5).
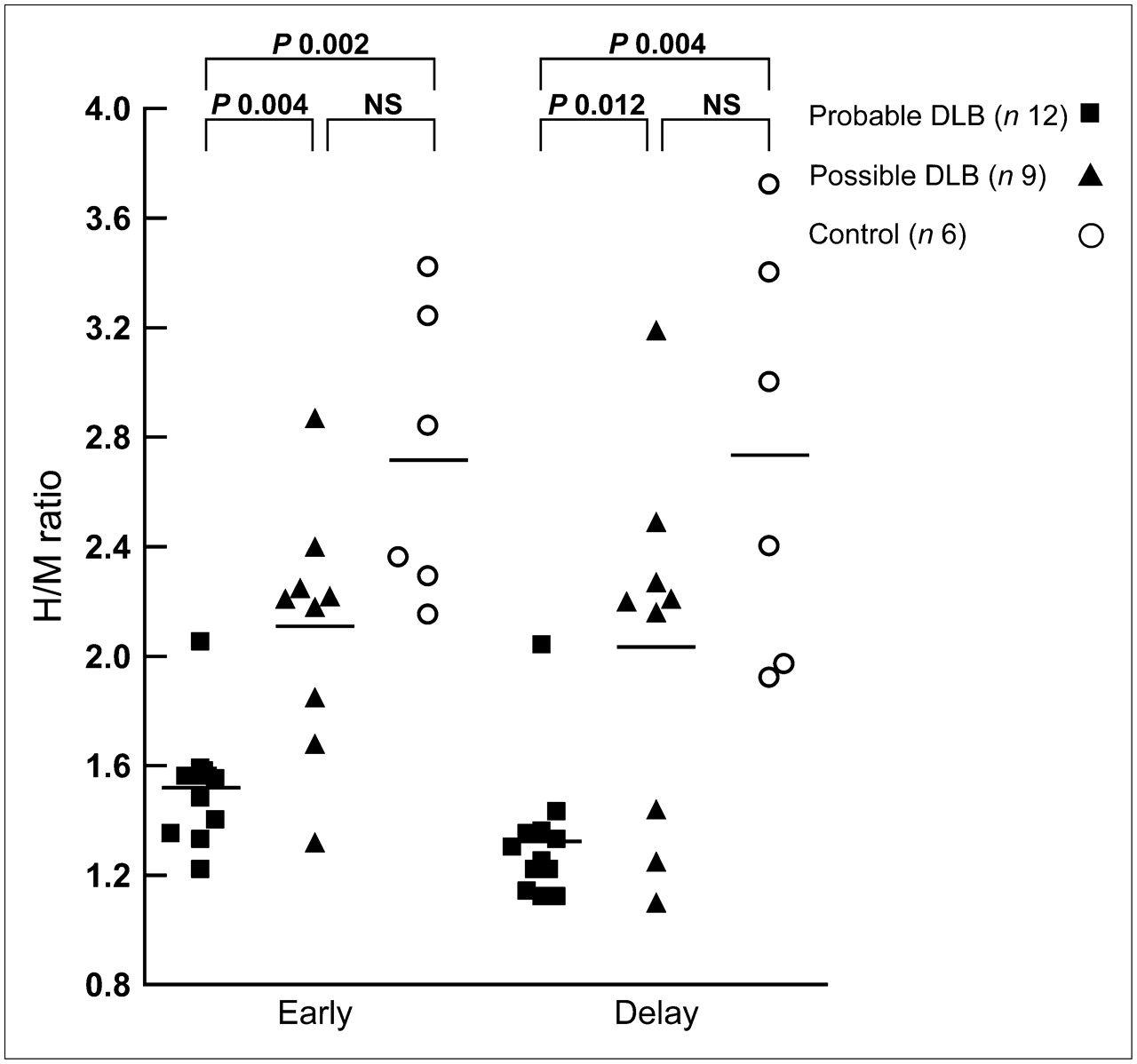
Mean early H/M ratio (1.52 ± 0.21) and delayed H/M ratio (1.32 ± 0.25) in probable DLB group were significantly lower than those in possible DLB group (early: 2.11 ± 0.45, P = 0.004; delayed: 2.03 ± 0.66, P = 0.012) and control group (early: 2.72 ± 0.53, P = 0.002; delayed: 2.74 ± 0.75, P = 0.004), respectively. NS = not significant.

There was no significant difference between probable DLB group (LVEF: 71.0% ± 9.15%) and possible DLB group (LVEF: 74.7% ± 8.14%, P = 0.35) and control group (LVEF: 69.5% ± 11.52%, P = 0.79), respectively. NS = not significant.
Summary of 123I-MIBG Cardiac Imaging and 99mTc-MIBI Cardiac Gated Study of Patients with Probable DLB
On early and delayed images, 6 of the 9 possible DLB patients exhibited normal 123I-MIBG uptake, but 3 patients (patients 18–20) demonstrated low 123I-MIBG uptake. The summary of 123I-MIBG and 99mTc-MIBI cardiac scintigraphy in the possible DLB group is shown in Table 5.
Summary of 123I-MIBG Cardiac Imaging and 99mTc-MIBI Cardiac Gated Study of Patients with Possible DLB
Table 6 shows a summary of the results of these combination examinations between 123I-IMP and 123I-MIBG for probable and possible DLB. Ten patients with probable DLB (83.3%) and 1 patient with possible DLB (11.1%) exhibited bilateral occipital hypoperfusion and low 123I-MIBG uptake. One patient with probable DLB (8.3%) and 2 patients with possible DLB (22.2%) exhibited no occipital hypoperfusion but did exhibit low 123I-MIBG uptake. One patient with probable DLB (8.3%) and 6 patients with possible DLB (66.7%) exhibited almost no occipital hypoperfusion and normal 123I-MIBG uptake.
Summary of Results of 123I-IMP Brain SPECT and 123I-MIBG Cardiac H/M Ratios for DLB
DISCUSSION
In the present study, we evaluated and confirmed the diagnostic usefulness of combination studies of cerebral blood flow with 3D-SSP/SEE analysis and cardiac sympathetic function for patients with probable and possible DLB. In the probable DLB group, almost all patients presented the DLB pattern in both examinations, whereas many patients with possible DLB presented no DLB pattern in both examinations. In both groups, there were a few patients who showed no DLB pattern in the 123I-IMP study but did show the DLB pattern in the 123I-MIBG study. These results support the utility of the combination study, which was more useful in the possible DLB group. Moreover, we evaluated myocardial perfusion and function by ECG gated 99mTc-MIBI SPECT to examine whether myocardial perfusion and contractility would be reduced by the denervation. No subjects with probable or possible DLB exhibited a perfusion defect or wall motion abnormality of the entire LV.
It has been reported that occipital hypoperfusion—including the precuneus and posterior cingulate gyrus using SPECT or hypometabolism using PET—is seen in clinically diagnosed DLB patients (9–13). In our study, 12 patients presented here are consistent with these previous results. However, several investigators did not find occipital hypofunction in DLB or significant differences in metabolic or perfusion patterns of DLB and AD (24–26). In addition, the reported sensitivity and specificity of diagnosis for DLB using brain imaging in some autopsy-proven studies have varied (11,12). In our study, 9 patients demonstrated no occipital hypoperfusion or unilateral occipital hypoperfusion and exhibited low extent ratios regardless of having a clinical diagnosis of DLB. In particular, many patients in the possible DLB group exhibited regional blood flow patterns such that AD and frontotemporal lobe dementia were suspected to coexist. Thus, differences in the perfusion SPECT pattern do have some value in differentiating DLB, but the diagnostic accuracy of those techniques is currently limited.
123I-MIBG scintigraphy was developed to evaluate cardiac sympathetic function and is used in a variety of cardiac diseases and disorders, such as coronary artery disease, cardiomyopathies, and heart failure (27,28). Recently, the tracer has been applied to patients with neurodegenerative diseases such as PD, DLB, and related disorders (15–17,29). Taki et al. suggested a low H/M ratio could be used as a specific marker for Lewy body disease (29). In our study, cardiac 123I-MIBG uptake was markedly decreased in 91.7% of probable DLB, as previously reported, but only 33.3% of possible DLB. Ten patients with probable DLB (83.3%) and 1 patient with possible DLB (11.1%) with typical findings of DLB on both brain perfusion and 123I-MIBG examinations were indeed DLB on follow-up. The combination of brain perfusion SPECT and 123I-MIBG examination was useful for 8.3% (1/12) in the probable DLB group and 22.2% (2/9) in the possible DLB group because these patients were indicated by specific findings of DLB or PD on 123I-MIBG examination but exhibited either mild reduction or no reduction in the occipital cortex. One patient with probable DLB (8.3%) and 6 patients with possible DLB (66.7%) may not, in fact, have DLB because these patients yielded negative findings of DLB on both brain perfusion and 123I-MIBG examinations. This one patient with probable DLB was regarded as having vascular dementia in the later clinical course and the 3D-SSP findings do not contradict this diagnosis. Four patients with possible DLB were similarly regarded as having AD; 1 patient was regarded as having frontotemporal lobe dementia and 1 patient was regarded as having vascular dementia in the later clinical course. Thus, we assume that combining images using 123I-MIBG scintigraphy with cerebral blood flow SPECT might be particularly important when perfusion does not indicate reduction of the occipital cortex, regardless of an original clinical diagnosis of DLB, as Hanyu has reported (19).
Both low uptake on PET/SPECT with reduced occipital activity and low uptake of 123I-MIBG have been cited as “supportive features” in the revised criteria for the clinical diagnosis of DLB (30). On the basis of our results, we believe problems could arise if only the findings of perfusion are used, particularly in relation to the reduction of occipital cortex for differential diagnosis. First, flow reduction in the occipital lobe may not necessarily be present. Second, the exact pathophysiology of the occipital changes is currently unknown. Third, findings in the occipital lobe are easily affected by the scanning environment. Fourth, it is common to have difficulty with decision making for reduction of the occipital cortex in mild cases because blood flow in the occipital cortex is usually higher physiologically than that in the other cortices (31,32)—even if some correction is possible using statistical brain function analysis. In contrast, 123I-MIBG scanning combined with perfusion SPECT appears to have the advantage. A diagnosis in the early period of illness or even in the preclinical stage might be possible because Lewy body–type degeneration in the cardiac plexus is observed in almost all patients with incidental Lewy body disease (33), and sympathetic nerve fibers are markedly decreased in number in all patients with PD regardless of the presence or absence of orthostatic hypotension (18,34). Moreover, 123I-MIBG uptake reduction does not correlate with disease duration (15,17). These supporting diagnoses using combined imaging techniques would be especially important for possible DLB rather than probable DLB—because the presence of only one core feature is sufficient for a diagnosis of possible DLB (2), and it would be difficult to differentiate patients with DLB presenting with only dementia in the early clinical course from those with AD (35,36) and it might prove difficult to differentially diagnose patients with only parkinsonism from PD or other parkinsonian syndromes. McKeith et al. reported, in an autopsy study, relationships between primary and secondary clinical diagnoses that confirmed previous reports that the majority of DLB cases also met criteria for the other dementia subtypes, particularly possible AD (8). According to this report, the majority of probable DLB patients were diagnosed neuropathologically as DLB, but the majority of possible DLB patients were not diagnosed pathologically as DLB, but as progressive supranuclear palsy or AD. This suggests the critical importance of a correct differential diagnosis in possible DLB cases.
Recently, there has been evidence that dopamine transporter imaging using SPECT may also have a role in distinguishing DLB from AD, with a multicenter study reporting that abnormal scans had a mean sensitivity of 77.7% for detecting clinical probable DLB, with a specificity of 94% for excluding non–DLB dementia, which was predominantly due to AD (37). In contrast, because the sensitivity and specificity of current 123I-MIBG studies for probable DLB are very high (15–17), it might be expected at present that 123I-MIBG could be superior to a dopamine transporter as a diagnostic tool. Although we cannot conclude which is superior to dopamine transporter imaging or other brain imaging, including perfusion SPECT—because the reported sensitivity and specificity of diagnosis for DLB using these studies have varied (11,12,37)—brain perfusion, 123I-MIBG, and dopamine transporter imaging might be complementary each other.
MIBG–MIBI mismatch often can be observed in acute myocardial infarction and transient myocardial ischemia attacks such as unstable angina pectoris or vasospastic angina pectoris (38,39). In our patients, there was no history or sign of cardiac disease or ECG abnormalities. Although these “complete mismatch” instances between MIBG and MIBI SPECT would be expected to be a characteristic feature of DLB, MIBI study may not be necessary in the differential diagnosis of other forms of degenerative dementia and related disorders. However, we studied a patient in which the EF decreased temporarily during the progressive course of a probable DLB patient. In this instance, the LVEF decreased from 67% to 48% on the second study, but there was no perfusion defect and the 123I-MIBG findings were approximately constant. The LVEF recovered to 58% on the recent study, although the reason for this is unclear. Therefore, long-term follow-up cardiac 123I-MIBG and 99mTc-MIBI SPECT studies—in particular, LVEF, as well as histopathologic evaluation with autopsy in DLB patients—are warranted in the future.
The present study has several limitations. First, the number of subjects studied is small. It will be important to validate the clinical diagnostic efficiency of this technique in a larger cohort of patients. Second, the diagnosis was carefully determined on the basis of clinical findings and imaging but has not been confirmed by autopsy thus far. Follow-up imaging studies have been performed (data not shown) and confirmations by autopsy will be performed in the future. Third, we selected healthy control subjects for the 123I-IMP study—with minor neurologic symptoms and no reduced area in 3D-SSP analysis—and selected healthy control subjects for the 123I-MIBG and 99mTc-MIBI study—with normal H/M ratios on 123I-MIBG planar imaging and with 99mTc-MIBI SPECT demonstrating normal myocardial accumulations and normal LVEF in gated SPECT. The healthy control subjects of the 123I-IMP studies and the cardiac studies were different. We should have compared patients and the same age-matched control group in the 123I-IMP, 123I-MIBG, and 99mTc-MIBI studies. Further prospective studies are warranted in the future.
CONCLUSION
These results suggest that combined examination of cerebral blood flow with 3D-SSP/SEE analysis and cardiac sympathetic nerve function with 123I-MIBG would be useful as a supporting diagnostic method in patients with DLB—particularly, when cerebral blood flow does not show occipital hypoperfusion and is, therefore, more useful in the possible DLB group. Cardiac perfusion and contractility may not be influenced by the denervation found on evaluation at the present time. Although a complete mismatch between MIBG and gated MIBI SPECT might be the characteristic features of DLB, long-term follow-up cardiac 123I-MIBG and 99mTc-MIBI SPECT studies as well as histopathologic evaluation at autopsy in DLB patients are warranted in the future.
Acknowledgments
The authors thank all staff at the Nuclear Medicine Division, Fujita Health University Hospital. This work was presented at the 54th Annual Meeting of the Society of Nuclear Medicine in Washington, D.C., June 2–6, 2007.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication March 28, 2007.
- Accepted for publication July 24, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}