


Abstract
The aim of this study was to evaluate whether 18F-fluorodihydroxyphenylalanine (18F-FDOPA) PET is accurate for the diagnosis and follow-up of any type of well-differentiated digestive endocrine tumor and to assess its performance compared with standard somatostatin receptor scintigraphy (SRS) using 111In-pentetreotide. Methods: We reviewed the results of 33 evaluable 18F-FDOPA PET and 111In-pentetreotide SRS examinations performed between March 2002 and September 2005 in 30 patients referred for documented well-differentiated digestive endocrine tumor. Results: The sensitivity and accuracy of 18F-FDOPA PET were significantly better for carcinoid tumors (defined according to the World Health Organization 2000 classification) (n = 19) than for noncarcinoid tumors (n = 14)—that is, 93% versus 25% for sensitivity (P < 0.01) and 89% versus 36% for accuracy (P < 0.01), respectively. In contrast, the performances of 111In-pentetreotide SRS did not differ according to the carcinoid or noncarcinoid type of the primary endocrine tumor—that is, 81% versus 75% for sensitivity and 79% versus 71% for accuracy, respectively. In carcinoid tumors, comparison between 18F-FDOPA PET and 111In-pentetreotide SRS showed that 18F-FDOPA PET more accurately evaluated the extent of disease than 111In-pentetreotide SRS. 111In-Pentetreotide SRS did not reveal any additional lesions in any case. Conversely, in noncarcinoid tumors, the extent of the disease was more accurately evaluated in all cases by 111In-pentetreotide SRS than by 18F-FDOPA PET. Conclusion: This preliminary study emphasizes the importance of a precise histologic characterization of well-differentiated digestive endocrine tumor to select the best radiopharmaceutical. 18F-FDOPA PET appears to be useful in carcinoid tumors and could become the first-line scintigraphic imaging modality for these tumors, but 111In-pentetreotide SRS appeared to be a better first-line scintigraphic imaging modality for noncarcinoid digestive tumors.
- 18F-FDOPA PET
- 111In-pentetreotide somatostatin receptor scintigraphy
- well-differentiated digestive endocrine tumor
Endocrine tumors of the gastrointestinal tract are relatively uncommon neoplasms, characterized by their marked heterogeneity. These digestive endocrine tumors are known to express somatostatin receptors. Somatostatin receptor scintigraphy (SRS), therefore, corresponds to the reference examination among the various available functional imaging modalities (1). However, 111In-pentetreotide SRS presents certain drawbacks due to the limited resolution of SPECT, which is especially disadvantageous when looking for primary tumors that can be very small and due to its high physiologic accumulation in the spleen, liver, and biliary and digestive tracts. Therefore, other functional imaging techniques are necessary to complement morphologic imaging. FDG PET has been demonstrated to be useful only in poorly differentiated tumors (2–4). 18F-Fluorodihydroxyphenylalanine (18F-FDOPA) PET is based on the capacity of endocrine tumor cells to take up, decarboxylate, and store amino acids, such as 3,4-dihydroxyphenylalanine (DOPA) (5). In the particular case of digestive endocrine tumors, 2 studies (6,7) have demonstrated that 18F-DOPA PET (18F-FDOPA PET) is superior to 111In-pentetreotide SRS on a per-lesion basis. In these 2 studies, most of primaries were classified as carcinoid tumors. According to the World Health Organization (WHO) 2000 classification (8,9), neuroendocrine tumors (now called endocrine tumors) are categorized into well-differentiated benign tumors, well-differentiated carcinomas, and poorly differentiated carcinomas. The sometimes-confusing term “carcinoid” must now be used only for well-differentiated tumors with serotonin reactivity, which supports a midgut origin (10,11). The aim of this study was to evaluate the performances of 18F-FDOPA PET according to the nature of digestive endocrine tumors, distinguishing carcinoid tumors from other well-differentiated digestive endocrine tumors. A head-to-head comparison with 111In-pentetreotide SRS results was also performed.
MATERIALS AND METHODS
Patients
Between March 2002 and September 2005, 39 18F-FDOPA PET and 111In-pentetreotide SRS examinations were performed on consecutive patients with histologically proven well-differentiated malignant digestive endocrine tumors. Thirty-three of these 39 patients satisfied the criteria for evaluation of the results of both examinations. The detailed context of each of these 33 evaluated examinations, performed on 30 patients (16 female, 14 male; mean age, 60 y; range, 40–73 y), is reported in Table 1.
Patient Characteristics
Seventeen 18F-FDOPA PET and 111In-pentetreotide SRS examinations were performed on 15 patients with a known small bowel carcinoid tumor: 4 for staging after resection of the primary tumor, 1 for suspicion of incomplete resection of the primary tumor, 2 for restaging, 8 for suspicion of recurrence, and 2 for systematic follow-up.
Nine 18F-FDOPA PET and 111In-pentetreotide SRS examinations were performed on 8 patients with a noncarcinoid tumor (pancreatic in 5 patients, duodenal in 2 patients, and gastric in 1 patient). Five examinations were performed for staging (with on-site primary tumor in 4 cases and after resection of the primary tumor in 1 case), 1 examination for restaging and 3 for suspicion of recurrence.
Finally, the last 7 18F-FDOPA PET and 111In-pentetreotide SRS examinations were performed on 7 patients to look for the primary tumor after diagnosis of well-differentiated metastatic lesion(s) and for staging. The final diagnosis was carcinoid tumor in 2 cases and noncarcinoid tumor in 5 cases.
As 18F-FDOPA is not yet an approved radiopharmaceutical in France, individual authorization for each patient was obtained from Agence Française de Sécurité Sanitaire des Produits de Santé, the French Medicines Agency.
Histologic and Immunohistochemical Findings
The tumors were classified as carcinoid or noncarcinoid on the basis of the histologic and immunohistochemical characteristics reported by the pathologists. An endocrine carcinoma arising in the small bowel with a low proliferative index (expressed in the report as a small number of mitoses or expression of Ki-67 antigen in <5% of cells) and containing serotonin was classified as carcinoid according to the new WHO classification. Endocrine carcinomas arising from any other digestive site, with a low proliferative index and without serotonin expression, were classified as well-differentiated noncarcinoid tumors.
18F-FDOPA PET
PET Cameras.
Between March 2002 and July 2004, PET was performed in 25 cases (Table 2) with a C-PET (ADAC) dedicated PET machine comprising full-ring detection by 6 NaI(Tl) curve continuous crystals, 25-mm thick. Acquisition was performed in 3-dimensional (3D) mode for emission and included transmission images by an external Cs source for attenuation correction. Slices were reconstructed by using an iterative algorithm (ordered-subsets expectation maximization). The 8 examinations since July 2004 (Table 2) were performed on a GEMINI PET/CT system (Philips) that combines a helical dual-slice CT and a 3D PET machine comprising 29 arrays of 616 gadolinium oxyorthosilicate crystals each. Crystal dimensions are 4 × 6 × 20 mm3. Reconstructions with and without attenuation correction were performed with a 3D iterative algorithm (row-action maximization-likelihood algorithm).
18F-FDOPA PET Imaging Protocol.
Patients were told to remain fasting for at least 6 h before the examination. 18F-FDOPA was provided as Iasodopa by Iason. The intravenous injection of 2 MBq/kg body mass of 18F-FDOPA when C-PET was used or 5 MBq/kg body mass for PET/CT with GEMINI was performed via an infusion line connected to saline. Immediately after injection, a first set of images was acquired on the abdomen, before excretion of 18F-FDOPA by the biliary tract that was subsequently seen on images acquired 1 h after injection. One hour after injection, and after the patient had voided, whole-body PET was acquired with the patient's arms above the head. This scan included the skull, neck, torso, and upper part of the thighs. Since July 2004, a low-dose helical CT scan (for attenuation correction and localization of the foci of 18F-FDOPA uptake) has been performed with the GEMINI machine (scan field of 600 mm, increment of 5 mm, slice thickness 6.5 mm, pitch of 1.5, 0.75 s per rotation, matrix 512 × 512, 120 kV, 40–100 mA·s) before PET acquisition.
111In-Pentetreotide SRS
111In-Pentetreotide SRS was performed in different centers (including our own) 4 and 24 h after intravenous injection of about 200 MBq of 111In-pentetreotide according to the European Association of Nuclear Medicine published guidelines (12). The median time interval between 18F-FDOPA PET and 111In-pentetreotide SRS was 20 d (range, 1–210 d) and SRS was performed before 18F-FDOPA PET in most cases (30 cases). Twenty-one 111In-pentetreotide SRS examinations were performed in our center with the following procedure: acquisitions, performed using a triple-head IRIX Philips camera, consisted of a whole-body scan and 2 SPECT acquisitions including the whole torso 4 h after injection. A second series of SPECT acquisitions including the torso was performed 24 h later.
Data Analysis and Endpoints
18F-FDOPA PET slices and rotating maximum-intensity-projection displays were evaluated by visual inspection both with and without attenuation correction. Any focus with an intensity that appeared to be greater than background and that could not be explained by physiologic activity was considered to be indicative of tumor tissue. Normal 18F-FDOPA uptake was seen in the striatum and pancreas (6) and subsequent elimination was seen in the biliary, digestive, and urinary tracts. 111In-Pentetreotide SRS examinations were interpreted on site in each center.
At the time of interpretation, the observer was informed about the results of the conventional diagnostic methods but was completely unaware of the patient's final outcome.
Thirty-three examinations were evaluated according to histology of lesions after further surgery or biopsy (n = 19) or a follow-up period of >6 mo (mean, 21 mo; range, 6–36 mo) (n = 14) (Table 2). All 33 18F-FDOPA PET examinations and the corresponding 33 111In-pentetreotide SRS examinations were analyzed separately on a per-patient basis. The head-to-head comparison between 18F-FDOPA PET and 111In-pentetreotide SRS results was also performed on a per-patient basis. A “site-based” evaluation was also performed using the following categories:
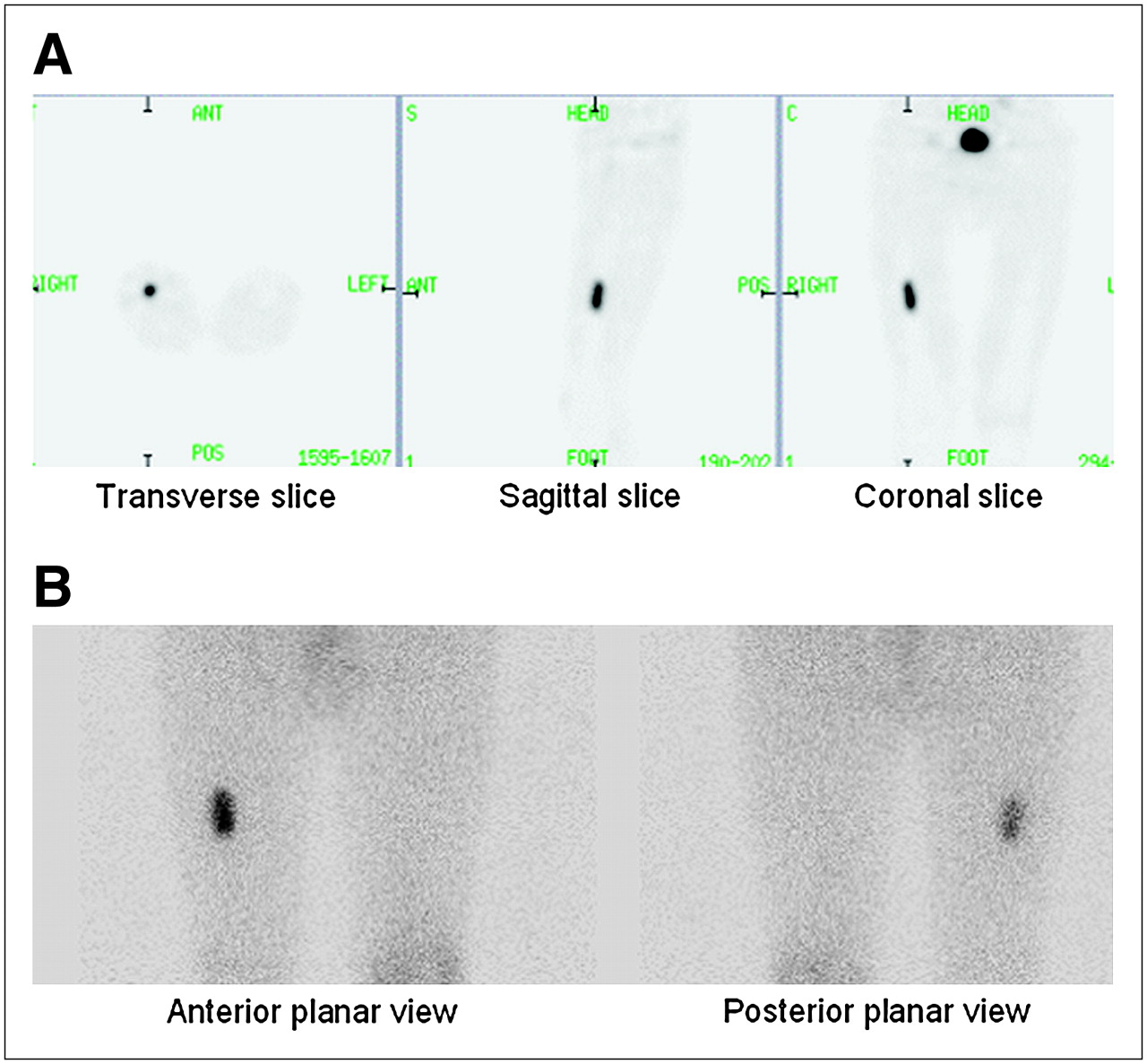
18F-FDOPA PET = 111In-pentetreotide SRS (Fig. 1): Both examinations were negative, or both examinations were positive with a comparable number and intensity of pathologic foci, or both examinations gave incorrect results.
FIGURE 1.Suspicion of recurrence of small bowel carcinoid tumor in patient with right thigh pain and pathologic radiographic appearance of right femur. 18F-FDOPA PET (A) and 111In-pentetreotide SRS (B) were both TP, showing isolated focus of uptake in right femur. Biopsy confirmed bone metastasis, and radiotherapy of bone lesion was performed.
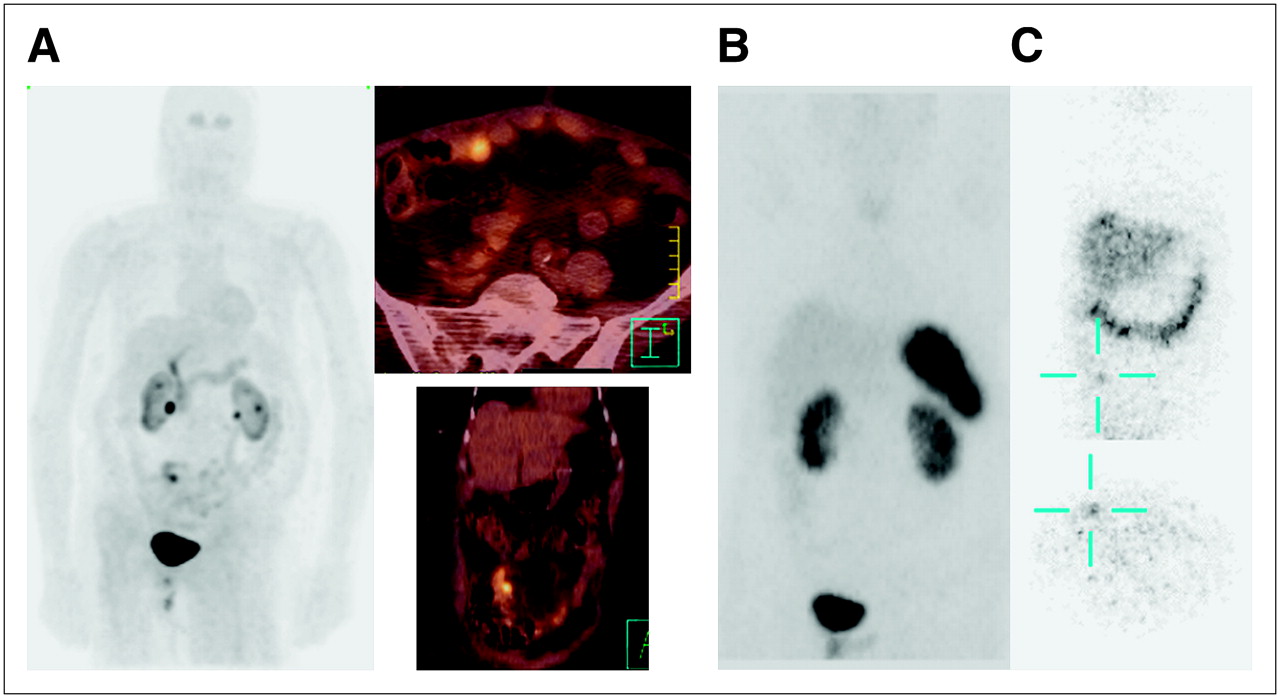
18F-FDOPA PET > 111In-pentetreotide SRS (Fig. 2): 18F-FDOPA PET was true-positive (TP) and 111In-pentetreotide SRS was false-negative (FN), or both examinations were TP on a per-patient basis with a greater number of foci visualized on 18F-FDOPA PET than on 111In-pentetreotide SRS, or foci were clearly identified on 18F-FDOPA PET and only reported as doubtful on 111In-pentetreotide SRS.
FIGURE 2.Search for primary tumor after detection of bilateral ovarian metastases of well-differentiated endocrine tumor. Bilateral ovariectomy was performed as part of radical surgery for uterine carcinoma. CT and contrast-enhanced bowel x-rays were negative. Primary tumor was clearly identified with 18F-FDOPA PET/CT (A), but 111In-pentetreotide SRS provided a doubtful result with negative images 4 h after injection of 111In-pentetreotide (B) and a doubtful abdominal focus 24 h after injection (C). Primary small bowel carcinoid was subsequently successfully resected.
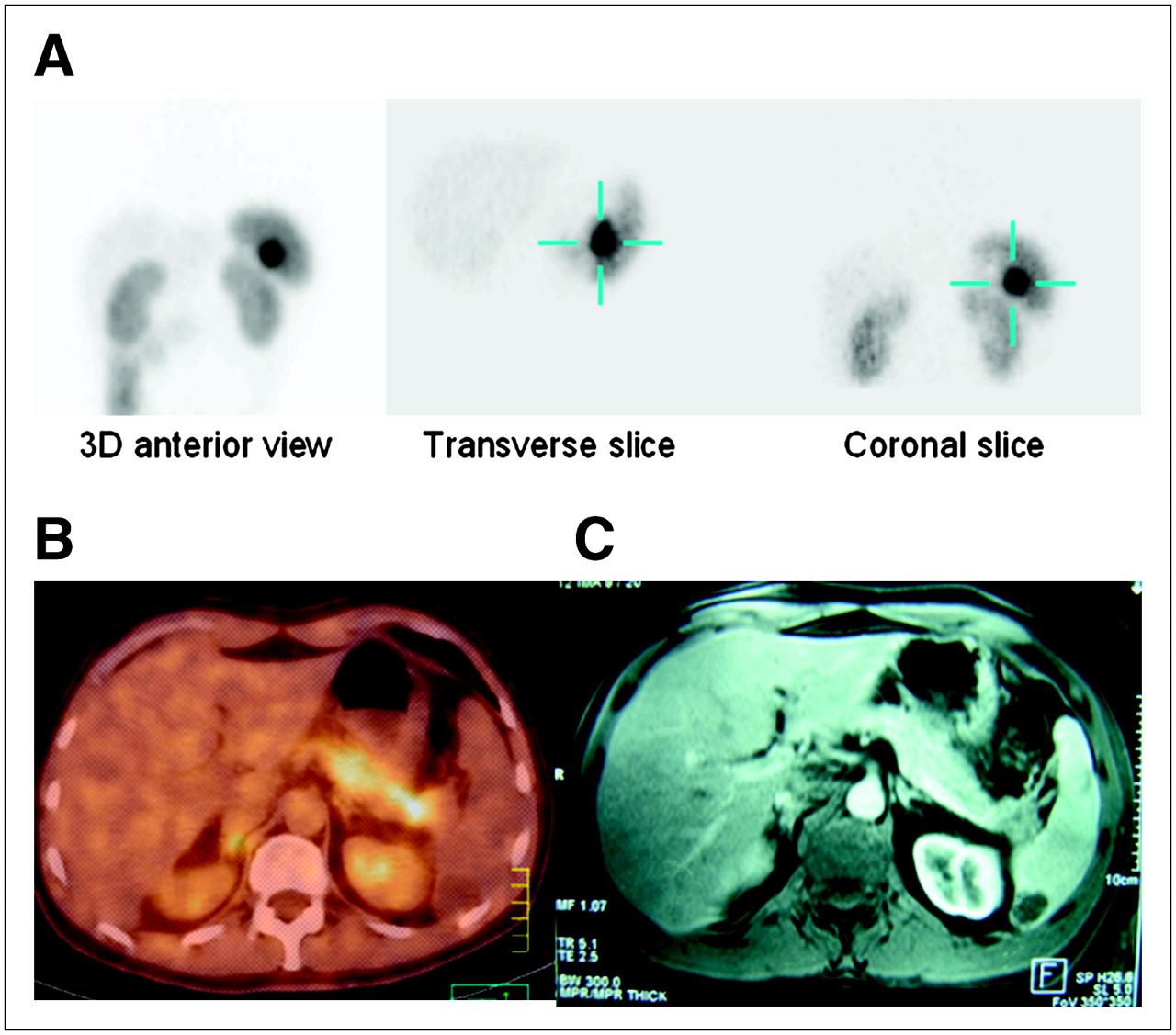
18F-FDOPA PET < 111In-pentetreotide SRS (Fig. 3): 18F-FDOPA PET was FN and 111In-pentetreotide SRS was TP, or both examinations were TP on a per-patient basis with a greater number of foci visualized on 111In-pentetreotide SRS than on 18F-FDOPA PET, or foci were clearly identified on 111In-pentetreotide SRS and were only reported as doubtful on 18F-FDOPA PET.
FIGURE 3.Search for primary tumor after surgical resection of liver metastases of well-differentiated endocrine tumor. 111In-Pentetreotide SRS was TP, showing intense uptake in tail of pancreas (A), subsequently visualized on MRI (C). 18F-FDOPA PET was FN (B) with physiologic heterogeneous uptake of 18F-FDOPA by healthy pancreas with no pathologic uptake in tail of pancreas. Image seen on MRI in spleen corresponded to a cyst.
Results of 33 Evaluable 18F-FDOPA PET and 111In-Pentetreotide SRS Examinations on Per-Patient Basis and FDOPA/SRS Comparison
The anatomic sites that were finally considered to be involved on the basis of histology or follow-up are reported in Table 2. The following sites were assessed separately: liver, abdominal lymph nodes or peritoneum, small bowel, pancreas, thorax, and bone.
Statistical Analysis
The Fisher exact test was used to compare the performances of each imaging modality according to tumor histology (carcinoid vs. noncarcinoid). As each examination consisted of 2 imaging modalities (paired results), the McNemar test was used to compare the performances of 111In-pentetreotide SRS versus 18F-FDOPA PET.
For both tests, a level of P < 0.05 was considered to correspond to a statistically significant difference.
RESULTS
The overall performances of 18F-FDOPA PET and 111In-pentetreotide SRS on a per-patient basis are reported in Table 3. The sensitivity of 18F-FDOPA PET and SRS was 63% and 78%, respectively, and their accuracy was 67% and 76%, respectively. These differences were not significant according to the McNemar test.
18F-FDOPA PET and 111In-Pentetreotide SRS: Overall Diagnostic Performances on Per-Patient Basis
18F-FDOPA PET on Per-Patient Basis in Carcinoid Tumors
18F-FDOPA PET was accurate in 17 of the 19 examinations (14 TP and 3 true-negative [TN]) and inaccurate in 2 cases (1 false-positive [FP] and 1 FN) (Tables 2 and 4).
18F-FDOPA PET: Diagnostic Performances on Per-Patient Basis
The FP result corresponded to examination 3. 18F-FDOPA PET was performed to detect residual disease 6 mo after surgery for an extensive small bowel carcinoid tumor with a previous TP 18F-FDOPA PET examination. Serum chromogranin A (128 ng/mL; normal < 100 ng/mL) and urinary 5-hydroxyindoleacetic acid (5-HIAA) (8.9 mg/24 h; normal < 8 mg/24 h) concentrations remained slightly elevated. 111In-Pentetreotide SRS was negative. 18F-FDOPA PET/CT showed a focus suggestive of a pathologic right external iliac lymph node. Surgery, guided by 18F-FDOPA PET/CT, was performed 1 mo later; no disease was found in the right lymphadenectomy specimen but 2 metastatic left iliac lymph nodes were resected.
The PET/CT FN result (examination 6) can be explained by the small size (3 mm) of a second small bowel carcinoid tumor found on systematic partial resection of ileum performed because of persistent clinical symptoms several months after resection of the first primary tumor.
In 1 TP case (examination 18, Fig. 2), 18F-FDOPA PET/CT and 111In-pentetreotide SRS, performed to detect the primary tumor after resection of ovarian metastases of a well-differentiated endocrine tumor, revealed a small bowel carcinoid primary tumor (this small primary tumor, not detected by morphologic imaging and contrast-enhanced bowel x-rays, was clearly identified by 18F-FDOPA PET/CT, but was considered to be doubtful on 111In-pentetreotide SRS).
In patient 17 (examination 19), the primary tumor, though not localized by any morphologic or functional imaging modality, was considered to be a carcinoid on the basis of elevated serum serotonin levels (3.8 μg/mL; normal < 1.7 μg/mL). This examination was classified TP on a per-patient basis due to 18F-FDOPA and 111In-pentetreotide uptake by liver metastases.
18F-FDOPA PET on Per-Patient Basis in Noncarcinoid Tumors
18F-FDOPA PET was accurate, on a per-patient basis, in 5 of 14 cases (3 TP and 2 TN) and inaccurate in 9 FN cases (Tables 2 and 4).
The 9 FN results (examinations 20–22, 24–26, 28, 30, and 33) remained unexplained in these well-differentiated lesions larger than 1 cm in diameter; 3 of these examinations were performed with the PET/CT system.
Comparison of Performances of 18F-FDOPA PET According to Histology (Carcinoid vs. Noncarcinoid)
The sensitivity and accuracy of 18F-FDOPA PET were significantly better in carcinoid tumors (93% and 89%, respectively) than in noncarcinoid tumors (25% and 36%, respectively) (P = 0.0007 for sensitivity and P = 0.002 for accuracy; Fisher test) (Table 4).
111In-Pentetreotide SRS on Per-Patient Basis in Carcinoid Tumors
111In-Pentetreotide SRS was accurate in 15 of 19 examinations (13 TP and 2 TN) and inaccurate in 4 cases (3 FN and 1 FP). One FN result was explained by the small size (3 mm) of the lesion (examination 6, which was also FN on 18F-FDOPA PET/CT [detailed analysis earlier]). One FN result corresponded to the FP result of 18F-FDOPA PET previously described (examination 3). One FN result was observed in patient 13, referred for unexplained elevation of urinary 5-HIAA levels. 18F-FDOPA PET gave a TP result, showing multiple foci in the thorax and abdomen, leading to a treatment by chemoembolization (Tables 2 and 5).
111In-Pentetreotide SRS: Diagnostic performances on Per-Patient Basis
111In-Pentetreotide SRS on Per-Patient Basis in Noncarcinoid Tumors
111In-Pentetreotide SRS was accurate in 10 of 14 examinations (9 TP and 1 TN) and inaccurate in 4 cases (1 FP and 3 FN). The 3 FN results (examinations 21, 22, 25) were not explained in these well-differentiated lesions greater than 1 cm in diameter (18F-FDOPA PET was also FN) (Tables 2 and 5).
The FP result corresponded to examination 32 performed in patient 29. 111In-Pentetreotide SRS was doubtful in the abdomen (and 18F-FDOPA PET was negative) in a context of abdominal pain during follow-up of a well-differentiated pancreatic tumor. The recurrence was not confirmed and the patient remained in persistent remission 2 y after this examination.
Comparison of Performances of 111In-Pentetreotide SRS According to Histology (Carcinoid vs. Noncarcinoid)
The sensitivity and accuracy of 111In-pentetreotide SRS were not significantly different in carcinoid tumors (81% and 79%, respectively) and noncarcinoid tumors (75% and 71%, respectively) (P > 0.05; Fisher test) (Table 5).
Comparison of 18F-FDOPA PET and 111In-Pentetreotide SRS on Per-Patient Basis
No significant difference was observed between the performances of 18F-FDOPA PET and 111In-pentetreotide SRS in terms of the overall results (Table 3) and the results for carcinoid tumors. However, in noncarcinoid tumors, 6 examinations were FN with 18F-FDOPA PET, although they were TP with 111In-pentetreotide SRS, corresponding to a significant difference in sensitivity between the 2 imaging techniques (P = 0.03; McNemar test).
Comparison of 18F-FDOPA PET and 111In-Pentetreotide SRS on Per-Site Basis
This approach illustrates the capacity of each imaging technique to evaluate the extent of disease. In carcinoid tumors, 18F-FDOPA PET appeared to be equal to or better than 111In-pentetreotide SRS in all tumor sites assessed. Conversely, in noncarcinoid tumors, 111In-pentetreotide SRS was equal to or better than 18F-FDOPA PET in all tumor sites assessed (Table 2).
Results of Examinations Performed to Detect Primary Tumor
Among the 7 18F-FDOPA PET and 111In-pentetreotide SRS examinations performed in this context, the primary tumor was demonstrated by 18F-FDOPA PET or 111In-pentetreotide SRS in 2 cases and by morphologic imaging or endoscopy in the other 5 cases. In patient 16, 18F-FDOPA PET and 111In-pentetreotide SRS demonstrated a diagnosis of primary small bowel carcinoid tumor (Fig. 2). In patient 18 (Fig. 3), 111In-pentetreotide SRS (and MRI) detected the primary tumor in the tail of the pancreas, corresponding to a well-differentiated noncarcinoid tumor.
DISCUSSION
The present study evaluated the performances of 18F-FDOPA PET and 111In-pentetreotide SRS in well-differentiated digestive endocrine tumors, distinguishing carcinoid tumors and noncarcinoid tumors according to the new WHO classification. Only 2 studies have addressed the use of 18F-FDOPA PET in digestive endocrine tumors: one study (6) performed on 17 patients with gastrointestinal endocrine tumors and the other study (7) performed on 23 patients, including 21 patients with an endocrine gastroenteropancreatic tumor and 2 patients with a nondigestive primary endocrine tumor. The term “carcinoid” used in these 2 studies actually encompassed a wide range of tumors, some of which would no longer be characterized as carcinoid: poorly differentiated tumors or tumors with negative immunohistochemical detection of serotonin. The main result of the present study was that 18F-FDOPA PET appeared to be significantly more accurate in carcinoid tumors than in noncarcinoid tumors with an accuracy of 89% and 36%, respectively, on a per-patient basis. Although it is difficult to compare the results of our study with those of the 2 previous studies, because of different definitions of carcinoid tumor, the article by Hoegerle et al. showed that 18F-FDOPA PET had better performances in well-differentiated tumors with positive immunohistochemical detection of serotonin than in moderately differentiated tumors or with negative immunohistochemical detection of serotonin (6), which is in accordance with our results. In the study by Ahlström et al. (13), using 11C-DOPA and PET in pancreatic endocrine tumors, only half of these tumors (11/22) were detected by 11C-DOPA PET. This result is also in accordance with the relatively poor performance of 18F-FDOPA PET observed in noncarcinoid pancreatic endocrine tumors (only 1 pancreatic lesion detected out of 7).
The secondary objective of the present study was to compare the results of 18F-FDOPA PET with those of 111In-pentetreotide SRS. This comparison included several biases related to the limited sample of each subgroup, the retrospective nature of the study, replacement of the PET machine by a PET/CT machine during the study, the quality of 111In-pentetreotide SRS examinations that were not performed and reviewed in the same center, and the nonrandomized order of examinations (111In-pentetreotide SRS preceded 18F-FDOPA PET in 30 of the 33 cases). However, in well-differentiated noncarcinoid digestive tumors, we observed the poor diagnostic performances of 18F-FDOPA PET (sensitivity and accuracy of 44% and 50%, respectively, on a per-patient basis, with FN results in lesions larger than 1 cm observed with both PET and PET/CT) contrasting with the better performances of 111In-pentetreotide SRS (sensitivity and accuracy of 83% and 84%, respectively, on a per-patient basis). Conversely, the extent of disease was more accurately evaluated in carcinoid tumors in the present series by 18F-FDOPA PET than by 111In-pentetreotide SRS. A selection bias cannot be ruled out for this finding, as 111In-pentetreotide SRS is much more readily available than 18F-FDOPA PET: Patients with obvious results on 111In-pentetreotide SRS were probably not referred to our center for 18F-FDOPA PET.
According to the data of Becherer at al. (7), 18F-FDOPA PET more reliably demonstrated skeletal involvement than 111In-pentetreotide SRS and also had a better sensitivity than 111In-pentetreotide SRS for the detection of liver metastases, lymph nodes, and intestinal tumors, although 18F-FDOPA PET and 111In-pentetreotide SRS were both unsatisfactory in detecting lung metastases. Hoegerle et al. (6) emphasized the superiority of 18F-FDOPA PET compared with 111In-pentetreotide SRS to detect lymph nodes, especially when they measured about 1 cm. In the present study, we observed that 18F-FDOPA PET was equal to or superior to 111In-pentetreotide SRS for evaluation of the extent of disease regardless of the anatomic site in carcinoid tumors and that, conversely, 18F-FDOPA PET was inferior to 111In-pentetreotide SRS for the assessment of noncarcinoid tumors. In carcinoid tumors, 18F-FDOPA PET was superior to 111In-pentetreotide SRS for the detection of liver metastases in 7 of 8 cases and for the detection of lymph nodes or peritoneal lesions in 6 of 10 cases. The only case with a skeletal lesion was detected on both 18F-FDOPA PET and 111In-pentetreotide SRS. No lung metastases were assessed in this series; the only thoracic lesion corresponded to a lymph node that was detected on both 18F-FDOPA PET and 111In-pentetreotide SRS.
In noncarcinoid tumors, 111In-pentetreotide SRS was superior to 18F-FDOPA PET for the detection of liver metastases in 3 of 5 cases and for the detection of lymph nodes or peritoneal lesions in 4 of 5 cases. Pancreatic tumors were detected by 111In-pentetreotide SRS alone in 2 cases, by both 18F-FDOPA PET and 111In-pentetreotide SRS in 1 case, and by neither modality in 4 cases. In the only case of bone metastases, SRS detected the skeletal lesions, although 18F-FDOPA PET was negative. Therefore, the present study should be considered to be a phase II study, suggesting the superiority of 18F-FDOPA PET over 111In-pentetreotide SRS in the various settings of carcinoid tumors (detection of the primary tumor, staging, restaging, detection of occult recurrences). Our study emphasizes the importance of precise histologic characterization of the tumor, based on the new WHO classification, to optimize the imaging strategy.
CONCLUSION
In conclusion, 18F-FDOPA PET could potentially be the first-line molecular imaging technique in carcinoid tumors, but can only be used in noncarcinoid tumors as a complementary modality after failure of a conventional approach, including 111In-pentetreotide SRS.
A prospective phase III comparative study with stricter inclusion criteria and centralized reading is necessary to demonstrate the superiority of 18F-FDOPA PET/CT in carcinoid tumors.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication February 6, 2006.
- Accepted for publication June 12, 2006.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- High Tumor Uptake on 18F-FDOPA PET/CT Indicates Poor Prognosis in Patients with Metastatic Midgut Neuroendocrine Tumors: A Study from the Groupe detude des Tumeurs Endocrines and ENDOCAN-RENATEN Network
- Diagnostic Role of PET/CT Tracers in the Detection and Localization of Tumours Responsible for Ectopic Cushings Syndrome
- Equivalent Dose Rate 1 Meter from Neuroendocrine Tumor Patients Exiting the Nuclear Medicine Department After Undergoing Imaging
- 18F-Fluorodihydroxyphenylalanine PET/CT in Patients with Neuroendocrine Tumors of Unknown Origin: Relation to Tumor Origin and Differentiation
- The clinical value of [18F]fluoro-dihydroxyphenylalanine positron emission tomography in primary diagnosis, staging, and restaging of neuroendocrine tumors
- Manipulation of [11C]-5-Hydroxytryptophan and 6-[18F]Fluoro-3,4-Dihydroxy-L-Phenylalanine Accumulation in Neuroendocrine Tumor Cells
- 6-L-18F-Fluorodihydroxyphenylalanine PET in Neuroendocrine Tumors: Basic Aspects and Emerging Clinical Applications