


Abstract
The aim of this study was to identify the brain areas that control urinary continence in healthy men by 99mTc-hexamethylpropyleneamine oxime (99mTc-HMPAO) SPECT. Methods: SPECT scans were performed on 15 right-handed healthy male volunteers, 24−45 y old. Each subject was scanned twice without movement in a supine position, and 444 and 555 MBq 99mTc-HMPAO were separately injected intravenously during the following 2 conditions: resting state with an empty bladder and urine-withholding state with a full bladder. The final image during urine withholding was obtained by subtracting the first scan data from the second scan data. The images were analyzed by statistical image analysis software and displayed on Z-score images at a significance threshold of P < 0.05 with correction for multiple comparisons. Results: In the urine-withholding state, as compared with resting, there was a significant increase in tracer activity in the bilateral inferior frontal gyri and the right superior and the middle temporal gyri. Among the regions, the right inferior frontal gyrus was distinctly prominent. When the threshold value was decreased to P < 0.005 without correction, there was a vast network of cortical and subcortical regions involved during urine withholding. Conclusion: Our results suggest that the right inferior frontal gyrus plays an important role in brain control of urinary continence. This study also suggests that brain control of continence can be confirmed by statistical image analysis software using SPECT.
- urinary continence
- urine withholding
- 99mTc-hexamethylpropyleneamine oxime
- statistical image analysis software
- SPECT
Urinary incontinence, which is defined as any involuntary leakage of urine, has long been acknowledged to be a major health problem in the elderly. It is also frequently found in patients with stroke (1), multiple sclerosis (2), Alzheimer's disease (3), multiple system atrophy (4), traumatic brain lesion (5), brain tumors (6), Parkinson's disease (4,7), and other cerebral disorders.
Up to now, human brain imaging studies have focused primarily on the act of micturition itself, especially the comparison between the voiding state and the resting state. Using SPECT, Fukuyama et al. (8) initially reported that the areas activated during micturition in healthy humans were the upper pons, the left sensorimotor cortex, the right frontal cortex, and bilateral supplementary motor areas. A PET study by Blok et al. (9,10) showed that micturition in healthy right-handed females and males was associated with alterations in blood flow within areas in the right pontine tegmentum, the periaqueductal gray (PAG), the right inferior frontal gyrus (IFG), the hypothalamus, and the right anterior cingulate gyrus. Nour et al. (11) revealed that the onset and maintenance of micturition in healthy men was associated with a vast network of cortical and subcortical regions, which included the frontal lobe, postcentral and precentral gyri, globus pallidus, cerebellum, thalamus, midbrain, insula, and anterior cingulate gyrus.
However, little is yet known about brain control of urinary continence, which is most important for patients with incontinence and the elderly. Some earlier studies on patients with cerebrovascular disorders and brain or spinal cord tumors indicated that urinary incontinence was associated with the lesions in both the middle of the pons and the frontal cortex (12–15). Recently, a case report using MRI indicated that the posterior portion of the right anterior cingulate gyrus was associated with the maintenance of continence and the right inferior frontal cortex was associated with the initiation of micturition (16).
In this study, we compared the regional cerebral blood flow (rCBF) during urine withholding with that in resting state to identify the brain areas that control urinary continence in healthy men. SPECT, which permits functional brain imaging of rCBF and is a powerful tool for the noninvasive localization of sensorimotor and psychologic functions, was adopted to study cerebral perfusion using 99mTc-hexamethylpropyleneamine oxime (99mTc-HMPAO). Neurologic Statistical Image Analysis Software (NEUROSTAT) was adopted to analyze SPECT images.
MATERIALS AND METHODS
Subjects
Fifteen right-handed healthy male volunteers were recruited (mean age ± SD, 32.67 ± 7.30 y; range, 24−45 y). No subject had a reported history of urologic, psychiatric, or neurologic disease and all received full information about the study plan. Subjects who had experienced any trouble in voiding in the past were excluded. This study was approved by the Ethics Committee of Asahikawa Medical College, and written informed consent was obtained before inclusion of each subject in the study.
Data Acquisition
Each subject was scanned twice without movement in a supine position. First, in the resting state, 444 MBq of 99mTc-HMPAO were injected intravenously while the subject lay supinely on the scanning table with an empty bladder and eyes closed in a quiet examination room. 99mTc-HMPAO was generated by reconstituting HMPAO with freshly eluted 99mTc-pertechnetate and was used within 30 min. Two minutes after the first injection, SPECT scanning was performed for 10 min with a 4-head γ-camera (SPECT 2000H; Hitachi Medico), using low-energy, high-resolution, parallel-hole collimators. Sixty-four projections were obtained on a 64 × 64 matrix in a step mode, with an acquisition time of 10 s per step and an energy window of 20% centered at 140 keV. The in-plane full width at half maximum of this system was 7.4 mm. Attenuation and scatter corrections were not performed.
After the first scan, furosemide (20 mg) was administered in a drop infusion, and an additional 555 MBq of 99mTc-HMPAO were injected intravenously when the subject sensed the urge to void in the urine-withholding state with a full bladder. The condition of a full bladder was confirmed by the subject moving his right index finger. The second scan was performed in the same way as the first. The subjects were permitted to void 5 min after the second injection. The interval between the first scan and the second scan was 16–37 min (mean, 25 min). If any sensation or behavior changed in the subject, the changes were recorded by the examiner.
Projection data were transferred to a dedicated data-processing unit (γ-Vision RW-3000; Hitachi Medico). The data were processed with a Butterworth filter (cutoff frequency, 0.55 cycle/cm; order, 8) and reconstructed into transaxial sections of 4.0-mm-thick images in planes parallel to the orbitomeatal line. Because the second scan data included the radioactivities from both resting and urine-withholding states, the final image of urine withholding was obtained by subtracting the first scan data from the second scan data. The image subtraction was performed after reconstruction by the data-processing unit. The process was done with an arithmetic operation that took the 2 scans as input and produced as output subtraction images whose pixel values were simply those of the second scan minus the corresponding pixel values from the first scan, thereby removing residual brain uptake of the first scan on the second scan.
Statistical Analysis
In this study, NEUROSTAT, which was developed by Minoshima et al. (17), was adopted to evaluate the change in rCBF.
Stat_1tZ, analysis software of NEUROSTAT, which can conduct a paired t test of 2 corresponding groups using cross-sectional images, was adopted to analyze the change in rCBF between the urine-withholding and the resting states. The process of analysis included 6 steps and was done as follows: anatomic standardization was performed first after coregistration of the 2 corresponding images, and then the pixel count was normalized. Averaging of the subtraction image was done after voxel-by-voxel subtraction of the 2 corresponding images. The last steps were performing the paired t test and creating the Z-score image in which the Z score was calculated by transforming the t statistic to the normal distribution using a probability integral transformation (18). Results were shown on 2 Z-score images (increase and decrease images), and detailed information was recorded in a text file.
Because there were so many voxel-by-voxel comparisons, many t values would reach a conventional level of significance by chance. Considering this, the correction for multiple comparisons is necessary. Therefore, the statistical significance was defined as P < 0.05 with correction for multiple comparisons (18), and a significance level of P < 0.005 without correction was used to report the trends in activated areas, for this level of significance giving sufficient protection against false-positive findings (19).
Another significance level of P < 0.001 without correction was also used to report the trends in activation to compare with the previous studies (9–11), in which this threshold was used.
RESULTS
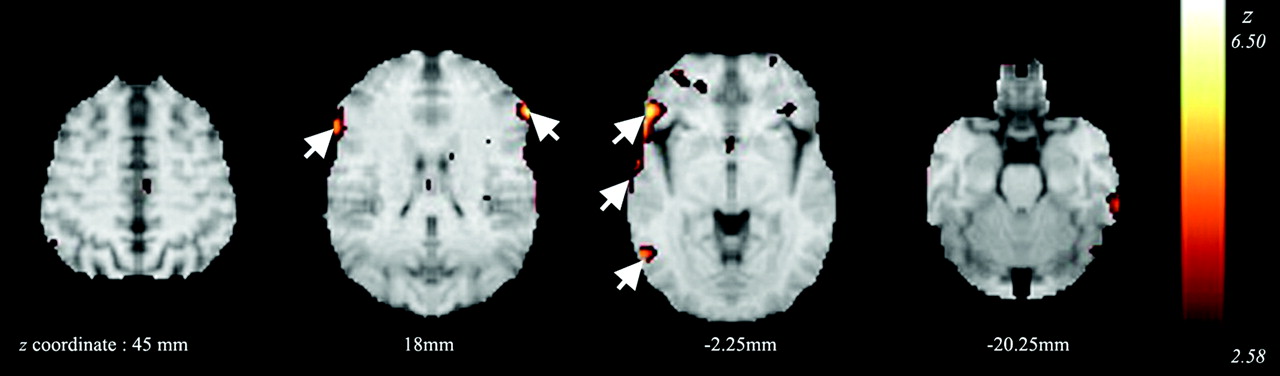
Thirty SPECT scans in the resting and the urine-withholding states from 15 subjects were obtained. In this study no changes (including pain) were recorded, except movement of the index finger. According to the result of Stat_1tZ with correction for multiple comparisons (P < 0.05), in the urine-withholding state, as compared with resting, there was a significant increase in tracer activity in the bilateral IFG (BA45, BA47, where BA is Brodmann area), the right superior temporal gyrus (STG) (BA22, BA38), and the middle temporal gyrus (MTG) (BA21, BA37) (Table 1; Fig. 1). Among these regions, the right IFG was the most prominent in both the Z score and the extent of the region (indicated by the number of voxels).

Activation pattern of urine withholding vs. resting at a significance threshold of P < 0.005 (Z = 2.58−6.50) without correction for multiple comparisons. Bilateral IFG and right STG and MTG are indicated by arrows, which were activated at a significance threshold of P < 0.05 (Z > 4.48) with correction for multiple comparisons.
Brain Areas with Increased Activity with Correction for Multiple Comparisons During Urine Withholding
When the threshold value was decreased to P < 0.001 (Z > 3.09) without correction for multiple comparisons, we found additional trends in activation in the following brain areas: bilateral superior frontal gyri (SFG) (BA10, BA11), bilateral precentral gyri (BA6), the left inferior temporal gyrus (ITG) (BA20, BA37), the left caudate nucleus, the right middle frontal gyrus (MFG) (BA9, BA10), and the inferior parietal lobule (IPL) (BA40).
Furthermore, bilateral cingulate gyri (BA24, BA32), the left MFG (BA47), the left middle occipital gyrus (MOG) (BA19), the left insula (BA13), the right thalamus, and the right caudate nucleus were also found with increased activity when the threshold value was decreased to P < 0.005 (Z > 2.58) without correction.
Areas with increased activity as trends without correction during urine withholding are indicated in Table 2.
Brain Areas With Increased Activity as Trends Without Correction During Urine Withholding
As a whole, the brain areas activated during urine withholding were bilateral frontal lobes (SFG, MFG, IFG, and precentral gyrus), bilateral temporal lobes (right STG and MTG, left ITG), bilateral cingulate gyri, bilateral caudate nucleus, the right IPL, the right thalamus, the left MOG, and the left insula. These regions constituted a vast network of cortical and subcortical structures. Among these regions, bilateral IFG and the right STG and MTG reached a statistic level of P < 0.05 with correction for multiple comparisons.
DISCUSSION
The aim of this study was to identify the brain areas that control urinary continence in healthy men by SPECT. Thereby, we performed SPECT on 15 healthy men and compared rCBF during urine withholding with that in the resting state. In fact, both urine withholding itself and some somatic discomfort due to the full bladder, which are difficult to differentiate, might cause the changes in rCBF during urine withholding. In this study, we could not differentiate between them, but both might be critical for brain control of urinary continence. Thus, some regions that were activated during urine withholding might be due to the somatic discomfort, not to urine withholding itself.
In this study, furosemide, which was a loop diuretic, was used. Furosemide inhibits the coupled Na+/K+/2Cl− transport system in the luminal membrane of the thick ascending limb of the loop of Henle. Thus, it reduces the reabsorption of NaCl and increases potassium excretion in the distal renal tubule and exerts a direct effect on electrolyte transport at the proximal tubule. It is well known that furosemide lowers system blood pressure and has been used in the treatment of hypertension, although it cannot cure hypertension. Furosemide is also effective in reducing intracranial pressure, although the effect is slow and weak, and it is usually used as an adjunct to enhance the effect of osmotic diuretics (21,22). We know that in healthy subjects the relationship between cerebral blood flow (CBF) and mean arterial blood pressure (MABP) is dominated by an autoregulatory mechanism that tends to maintain CBF relatively constant, despite changes in MABP in the range of 60−150 mm Hg (23). Up to now, no report indicated that furosemide could affect CBF significantly in healthy humans; however, it has been confirmed that CBF after furosemide remained similar to that before furosemide in the study of ponies during severe exercise (24). In these circumstances, although furosemide (20 mg) was administrated before the second scan in this study, it might not affect the CBF significantly.
Another affecting factor that should be mentioned is movement of the index finger. In this study, the subject moved his right index finger to indicate that his bladder was full. We knew that moving the index finger was normally accompanied by a small activation in the motor cortex, which includes BA4 (primary motor cortex) and BA6 (premotor cortex and supplementary motor area). In this study, when the threshold was defined as P < 0.05 with correction for multiple comparisons, we did not find any activation in BA4 or BA6. When the threshold was defined as P < 0.001 without correction for multiple comparisons, we found activation trends in bilateral precentral gyri (BA6). Thus, activation of bilateral precentral gyri might be due to the moving the index finger, not urine withholding.
In this study, using SPECT with Stat_1tZ, we confirmed that urine withholding was associated with a vast network of cortical and subcortical regions in healthy male subjects. Bilateral IFG, especially the right side, were distinctly activated during urine withholding at a significance threshold of P < 0.05 with correction for multiple comparisons.
As early as 1960, urinary incontinence was found, for the first time, in 13.2% with frontal lesions in 167 patients (25). Later, in 1964, Andrew and Nathan (14) pointed out that a region in the frontal lobe was important in the higher control of micturition by investigation of selected cases, including cerebral tumors, intracranial aneurysms, brain injury, and leucotomies. Following this paper, many lesion studies in patients with cerebrovascular disorders and brain tumors indicated that urinary incontinence was associated with the lesions in the frontal cortex (12,13,15,26). A PET study demonstrated the blood flow was increased in the right frontal operculum during urine withholding in healthy female subjects at a significance level with corrected P < 0.05 (10). In 2001, Athwal et al. (27) found that increasing bladder volumes resulted in increased brain activity in bilateral frontal lobes at a threshold of P < 0.05 without correction. A clinical study of the brain and urinary tract function on 128 geriatric patients with established urinary incontinence, by Griffiths (28), also confirmed that the frontal areas, especially on the right, were associated with urge incontinence by SPECT.
The right IFG has been previously described to be involved in attention mechanisms (29) and the selection of response to a situation (30). It might play a role in making the decision of whether or not to void at the particular time and place (9) and modulation of urinary control (15). We suggest that the frontal lobe, especially the right IFG, plays an important role in brain control of urinary continence.
In this study, we found additional activation in the right STG and MTG during urine withholding with corrected P < 0.05, which was reported less. In a series of stroke patients, urinary dysfunction was found in 14% with temporal stroke (1). Several articles (31–33) reported that the seizure of temporal lobe epilepsy patients was characterized by an aura of ictal urinary urge. Griffiths (28), who performed SPECT on 73 incontinent patients and found 10 patients with regional underperfusion in the right temporal lobe and 10 patients with regional underperfusion in the left temporal lobe, also supported our result. Moreover, we also found activation in the left temporal lobe, although it did not reach a significance level with correction for multiple comparisons. Blok et al. (9) reported an opposite result, that the activity of the right MTG was decreased during urine withholding, but it was not significant for multiple comparisons. We do not have an adequate explanation for the discrepancy between our results and those of Blok, which might be resolved by the further studies. We suggest that the temporal lobe, especially the right STG and MTG, was associated with urine withholding, although it was not so prominent.
In our study, when the threshold value was dropped to P < 0.005 without correction for multiple comparisons, we found additional trends in activation in bilateral cingulate gyri and caudate nucleus, the left MOG and insula, the right IPL and thalamus, besides bilateral SFG and MFG, precentral gyri, and the left ITG.
Lesions in the forebrain, including the anterior cingulate gyrus, have been reported to cause urge incontinence (14,15). We found that the brain activity in bilateral cingulate gyri was increased during urine withholding, whereas Blok et al. (9,10) found decreased activity in the right anterior cingulate gyrus. The decrease in activity in the cingulate gyrus during urine withholding reflects a general suppression of sensory input or motor output. Blok et al. (9,10) considered that the anterior cingulate gyrus might be a level setting system, facilitating certain blueprints of behavior, and while urine was withheld, the antifacilitation was necessary—that is, the urge of voiding had to be inhibited. Athwal et al. (27) found the cingulate gyrus had increased activity as the bladder volume increased, while activity decreased as the subject felt the urge to void. The right anterior cingulate gyrus was considered to be associated with the maintenance of continence by a MRI study (16). It would be reasonable that when the urine was withheld, not in a strong urge to void, the cingulate gyrus was activated to work to maintain continence, and when the feeling to void was very strong, the activity of the cingulate gyrus might be decreased to stop maintaining continence for the initiation of voiding. The cingulate gyrus is known to have direct connections with brain stem nuclei and to be involved in regulation of autonomic and emotional responses to external stimuli (34,35). Therefore, it is possible that the cingulate gyrus was activated during urine withholding.
The thalamus and caudate nucleus were first reported to be associated with urine withholding in healthy subjects, although the thalamus has been reported to be associated with micturition in previous studies (9–11). The thalamus and caudate nucleus both belong to the forebrain, the lesion or hypoperfusion in which has been reported to cause or be associated with urge incontinence (14,15,28).
Blok et al. (10) demonstrated that the blood flow was increased in the right anterior insula during urine withholding in healthy female subjects at a significance level with corrected P < 0.05. A study from Nour et al. (11) indicated that the left insula showed a tendency to activate when urine withholding was compared with resting. The insular cortex might contain a primary cortical visceral representation, and its connections might underlie autonomic integration with behavioral and emotional events (36,37). Therefore, it is reasonable that activation of the insula represents the bladder with full urine and integrating the autonomic information of urinary continence during the urine-withholding state.
The right IPL and the left MOG have been mentioned in some lesion studies, although they were rarely reported previously, except the report by Athwal et al. (27), in which the parietal lobe was activated with increasing bladder volume in healthy men. In 1960, urinary incontinence was found in 6.3% with parietal tumors of 167 patients (25). Urinary dysfunction was also found in 20% with parietal stroke of 72 stroke patients (1). Griffiths (28) found 22 incontinent patients with regional underperfusion in the right parietal lobe and 10 with regional underperfusion in the left occipital lobe of 128 geriatric patients. Thus, the parietal and occipital cortices are also associated with urine continence.
It is well known that the involuntary urinary continence center is located in the pons, which was concluded from animal studies (38–40) as well as human studies (9,10). However, in our study, no significant increased activity was found in the pons. We have no explanation for this finding except to attribute our finding to the resolution of SPECT.
In this study, we used Stat_1tZ to analyze the data, and the number of voxels analyzed by Stat_1tZ is 176,455. The statistical significance is defined as P < 0.05 with correction for multiple comparisons (18); the corresponding Z value is >4.476 (P < 0.000004). Thus, the number of expected voxels P < 0.000004 is 0.71; in fact the number of observed voxels is much more than it, so the results are very significant.
To our knowledge, this is the first time that SPECT with NEUROSTAT was adopted to study the brain control of urinary continence in healthy men, whereas previous studies of functional brain imaging, including SPECT and PET, all used statistical parametric mapping (SPM). Although both SPM and NEUROSTAT are powerful techniques for statistical analysis of the brain perfusion SPECT, NEUROSTAT was found to be more suitable than SPM in anatomic standardization of atrophied brains (41). As urinary incontinence is common in the elderly, whose brains have a different degree of atrophy, and SPECT is more widely performed than PET worldwide, it would be easy to popularize the study of urinary disorders using SPECT with NEUROSTAT. In fact, to conclude whether it would be better to use NEUROSTAT than SPM in the study of urinary incontinence, further comparisons must be performed between the 2 methods in different age groups with incontinence.
This study would be very useful for clinicians to determine whether the cause of urinary incontinence is a central disorder and to determine the treatment. In this study, we compared only the resting state with urine withholding without voiding, so we cannot say anything about the comparisons between resting and voiding states and urine withholding and voiding states. Furthermore, the subjects of this study were all males, so nothing can be said about the brain control of urinary continence in females, which could be similar to that in males.
CONCLUSION
In summary, urinary continence is primarily associated with bilateral IFG and the right STG and MTG, although a vast network of cortical and subcortical regions is also activated during urine withholding. Among these regions, the right IFG plays an important role in brain control of urinary continence. This study also suggests that brain control of urinary continence can be confirmed by SPECT using NEUROSTAT.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication December 19, 2005.
- Accepted for publication March 22, 2006.




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.