


Abstract
Lymph node involvement is a major prognostic factor in bladder cancer, but the accuracy of conventional imaging modalities for the prediction of regional and distant metastatic diseases is limited. This study was performed to compare the diagnostic accuracies of contrast-enhanced CT and PET with 11C-choline for the staging of urothelial bladder cancer. Methods: Twenty-seven patients (median age, 69.1 y) who had urothelial bladder cancer and who were referred for radical cystectomy and pelvic lymph node dissection (PLND) on the basis of a histologic evaluation after transurethral resection of bladder cancer (TURB) were studied. PET scanning, using 2 multiring whole-body tomographs, was performed 5 min after intravenous injection of approximately 370–500 MBq of 11C-choline. In addition, conventional bone scintigraphy and contrast-enhanced CT were performed. After imaging, cystectomy and PLND were performed in all patients. Pathologic 11C-choline uptake that could not be explained by intestinal activity was noted as a positive result. Node positivity was determined by size on CT: nodes measuring more than 1 cm in the long axis were described as being positive for tumor. Histopathologic findings were used as a reference. Results: The presence of residual bladder cancer (pTa–pT4) was correctly detected in 21 of 25 histologically tumor-positive patients (84%) by CT and in 24 of 25 patients (96%) by 11C-choline PET. Lymph node involvement was correctly detected in 4 of 8 patients (50%) by CT and in 5 of 8 patients (62%) by 11C-choline PET. The median size of the 3 nodes with false-negative PET results was 9 mm (range, 6–21 mm), and the median size of the metastatic lesions within the lymph nodes was 3 mm (range, 1–15 mm). CT resulted in 6 (22%) false-positive lymph nodes, whereas none was demonstrated by 11C-choline PET; these data indicated a significantly higher accuracy of PET than of CT (P < 0.01). Both modalities missed a small peritoneal metastasis verified by histologic evaluation. No positive results were obtained from bone scintigraphy. Conclusion: These preliminary data suggest that 11C-choline PET is comparable to CT for detecting residual bladder cancer after TURB but appears to be superior to CT for the evaluation of potential additional lymph node metastases. 11C-choline PET should be further evaluated for staging in patients who have bladder cancer and who are scheduled for radical cystectomy.
Urothelial bladder cancer is a common neoplasm of the urinary tract (1). At the time of diagnosis, 75%–85% of patients have superficial tumors (<pT2), and 15%–25% have a muscle-invasive disease (≥pT2) (2). The extent of bladder wall infiltration is an important parameter, as it determines further therapeutic options. To evaluate the local extent of tumors and to histologically verify disease, transurethral resection of bladder cancer (TURB) is usually performed. This procedure also may have curative intent for superficial tumors. For invasive bladder cancer, radical cystectomy and pelvic lymph node dissection (PLND) are considered the treatments of choice, superior to radiation therapy and organ-conserving surgery with regard to local tumor control and survival (2). In 12 studies totaling 6,127 patients undergoing radical cystectomy and PLND for bladder cancer (pTa–pT4), the mean incidence of lymph node metastases was 22.2% (range, 15.0%–28.1%). Furthermore, a positive correlation with tumor stage was observed: pTa, 0%; pTis, 0.6%; pT1, 6.1%; pT2, 17.9%; pT3, 35.9%; and pT4, 49.3% (3–14). Recent literature showed evidence that extended PLND (vs. standard PLND) may prolong survival (15). Therefore, a more accurate predictive test to assess nodal disease before surgery would be highly desirable.
PLND is usually performed together with radical cystectomy because current modalities for the staging of lymph node status (lymph node staging) are still unsatisfactory. In fact, conventional techniques for lymph node staging, such as contrast-enhanced CT and MRI, depend on morphologic information for diagnosis, and the detection of metastatic lymph nodes is insufficient (16,17) and may be difficult when their size is not increased (16–18). Thus, the only accurate method for lymph node staging is the histologic analysis derived from a surgical procedure (15). In contrast to CT and MRI, PET is based on functional rather than morphologic criteria, and its role in the staging and restaging of cancer has been widely recognized (19). However, the most extensively used tracer in oncology, the glucose analog 18F-FDG, has not been successfully applied in bladder cancer because its physiologic urinary excretion interferes with the imaging of pelvic tumors (20). More recently, 11C-choline was successfully used to visualize various cancers (21). Because of the negligible excretion of 11C-choline into the urinary system, 11C-choline PET has been applied in particular to pelvic malignancies, for which low background radioactivity is critical for successful imaging (22).
The purposes of this study were to compare the diagnostic accuracy of 11C-choline PET with that of CT in the preoperative staging of urothelial bladder cancer and to verify the results by comparison with histopathologic analysis, the gold standard.
MATERIALS AND METHODS
Patients
Twenty-seven consecutive patients (median age, 69.1 y; range, 45–81 y) who had histologically proven urothelial bladder cancer and who were referred for radical cystectomy and PLND were enrolled into this study. All cancers were staged by TURB with histologic analysis to establish the local extent of the disease, abdominal CT was used to assess the presence of lymph node metastases and to detect tumor extension beyond the bladder wall, and bone scintigraphy was used to evaluate the presence of bone metastases. The decision regarding surgical treatment was based on clinical data and instrumental and histologic results at TURB. In particular, patients with muscle-invasive tumors and recurrent superficial bladder cancers for which TURB and intravesical instillation therapy were ineffective were referred for radical cystectomy.
Imaging was performed 22.8 ± 18.6 (mean ± SD) d (range, 5–64 d) after the TURB procedure and 23.9 ± 29.7 d before surgery (radical cystectomy and PLND).
Imaging results were compared with the results of histologic analysis of the specimens obtained from cystectomy and PLND. Twenty patients had bladder muscle infiltration (pT2–pT4), whereas the remaining 7 were identified as having superficial bladder cancer (pTa, n = 1; pT1, n = 3) or carcinoma in situ (Tis, n = 1) or as being negative for tumor tissue (pT0, n = 2) after the TURB procedure. Any positive finding by imaging in the presence of Tis or in absence of tumor (pT0) was considered a false-positive result.
Patients with preoperatively known distant metastases, neoadjuvant chemotherapy for bladder cancer, previous radiation therapy of the pelvis, and other secondary malignancies were excluded from this study. Details of the study were explained to all patients by a physician, and written informed consent was obtained. The study protocol was reviewed and approved by the Ethics Committee of the Technische Universität München.
11C-Choline PET
11C-choline was synthesized as described by Hara et al. (21). 11C-choline PET studies were performed with 2 multiring whole-body PET scanners (either ECAT HR+ or EXACT HR; CTI/Siemens) with very similar physical performance characteristics (23,24).
After patient positioning on the scanner table, a transmission scan with approximately 30 million counts per bed position was obtained with rotating 68Ge rod sources for segmented photon attenuation correction of the emission scan. PET emission scanning started 5 min after intravenous injection of approximately 370–500 MBq of 11C-choline and included 6 bed positions starting from the pelvis and moving to the neck. Emission imaging was performed in the 2-dimensional mode, with 5 min for the first bed position and increasing to 12 min for the sixth bed position, and with a matrix of 128 × 128 pixels. Emission data were corrected for randoms, dead time, and attenuation, and an iterative reconstruction algorithm based on ordered-subset expectation maximization with 4 iterations and 8 subsets was applied for both the emission scan and the transmission scan. Ordered-subset expectation maximization images underwent 5-mm full width at half maximum gaussian postsmoothing and were zoomed with a factor of 1.2.
Contrast-Enhanced CT
CT examinations were performed with a Sensation 16 scanner (Siemens). The following scan parameters were used: tube current, 180 mA/s; voltage, 120 kV; collimation, 16 × 0.75 mm; reconstructed slice thickness, 5; and reconstruction increment, 5 mm. Scans of the abdomen and pelvis were performed in the craniocaudal direction in the portal-venous phase (70-s scan delay) after intravenous injection of 150 mL of iodine contrast agent (Imeron 300; Altana). For 7 patients, single-slice scanners were used with the following parameters: voltage, 120 kV; tube current, 180 mA/s; collimation, 7 mm; table feed, 10 mm; and slice thickness, 5–7 mm. Scans were performed in the portal-venous phase (70-s scan delay) after intravenous injection of 150 mL of iodine contrast agent.
Bone Scintigraphy
Whole-body anterior and posterior planar images were acquired 3 h after intravenous injection of approximately 740 MBq of 99mTc-methylene diphosphonate (99mTc-MDP) by use of a dual head γ-camera equipped with a high-resolution collimator. The linear speed of acquisition was 12.5 cm/min.
Image Data Analysis
99mTc-MDP scintigraphy, CT, and PET images were interpreted by consensus by 2 experienced radiologists and 2 nuclear medicine physicians unaware of the results of the other investigations. 11C-choline PET images, reconstructed in transaxial, coronal, and sagittal views and corrected for attenuation, were assessed for focal pathologic tracer uptake to suggest the presence of residual bladder tumor tissue (after TURB) and lymph node or distant metastases. Semiquantitative analysis also was performed for 11C-choline PET studies by normalizing the amount of tracer uptake in any lesion detected to the injected dose and patient body weight to obtain a standardized uptake value (SUV).
At CT, bladder cancer was identified as wall thickening, as a mass lesion projecting into the lumen of the bladder, or as an extravesical mass (1). Lymph node metastases were considered when a nodal enlargement (>10 mm in the long axis) was depicted.
Bone scintigraphy anterior and posterior planar images were qualitatively analyzed separately and in a masked fashion on a computer monitor. Any localized increase in 99mTc-MDP uptake was considered metastatic, except for “hot spots” attributable to traumatic lesions or osteoarthrosis.
Surgical Procedure and Histologic Evaluation
The surgical procedure, including radical cystectomy and PLND, was performed as previously described (15), taking into account the results of 11C-choline PET and CT. The diagnosis of bladder cancer and the presence or absence of lymph node metastases were based on routine histologic examination of surgical specimens and the TNM classification system (pTa–pT4). Lymph node involvement was staged as pN1 or pN2 (25). The lymph node density (LND), defined as the total number of positive lymph nodes divided by the total number of lymph nodes removed, was calculated as well (15).
Statistical Analysis
Calculation of PET and CT sensitivity, specificity, and accuracy for detecting bladder cancer and lymph node neoplastic involvement was based on a per-patient analysis including the results of histopathologic examination after cystectomy and PLND. Standard definitions were used to calculate the parameters (26). Differences in accuracy were analyzed by McNemar testing for paired variables. A P value of <0.05 was considered significant.
RESULTS
At histologic analysis after radical cystectomy and PLND, 25 of 27 patients (93%) had remaining viable tumor tissue in the bladder wall after previous TURB. CT discovered 21 and 11C-choline PET discovered 24 of these 25 tumor-positive patients (84% and 96%, respectively). The total number of histologically proven lesions was 34 (residual bladder cancer, n = 25; lymph node metastases, n = 8; peritoneal metastasis, n = 1). CT depicted 25 of 34 lesions (73%) (residual bladder cancer, 21/25; lymph node metastases, 4/8; peritoneal lesion, 0/1). 11C-choline PET depicted 29 of 34 lesions (85%) (residual bladder cancer, 24/25; lymph node metastases, 5/8; peritoneal lesion, 0/1). Figure 1 shows an example of residual bladder cancer with lymph node metastasis detected by both CT and 11C-choline PET. The degree of 11C-choline uptake, measured as the mean SUV in the lesion, ranged from 1.5 to 6.9 (mean, 3.3) in bladder cancer tumors and from 1.6 to 3.8 (mean, 3.1) in lymph node metastases.
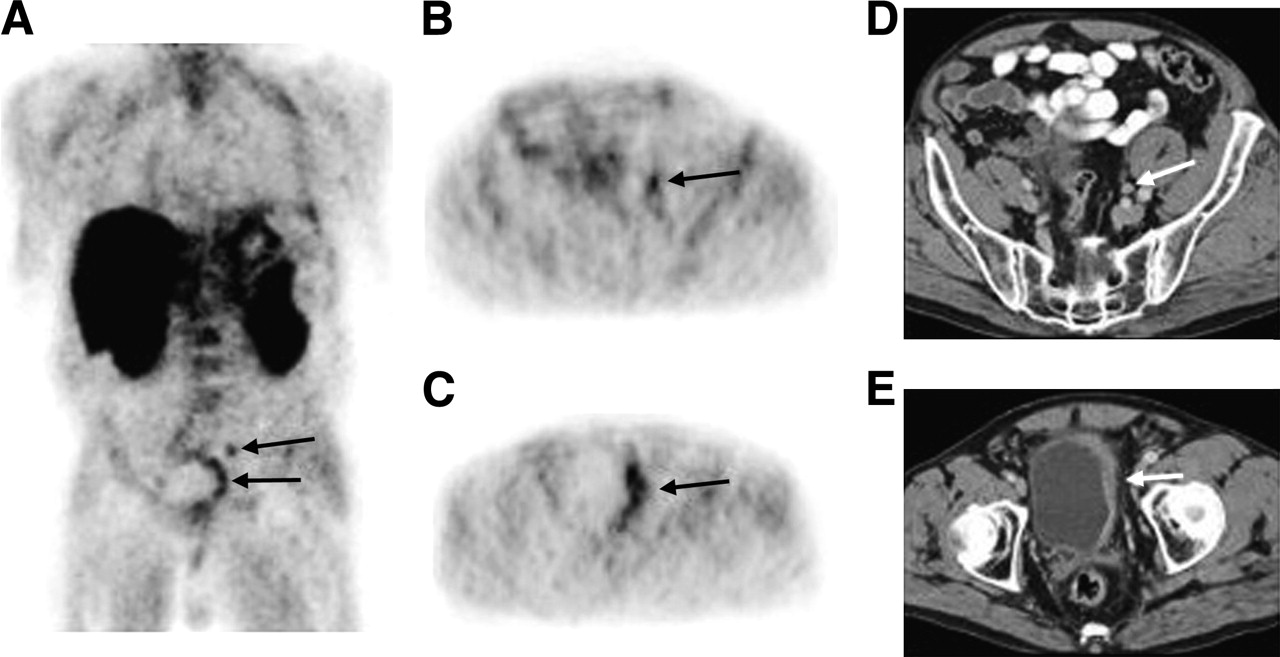
Increased 11C-choline uptake (arrows) at left pelvic lymph node superior to bladder and at left bladder wall on coronal whole-body PET image (A) and on corresponding transaxial PET images (B and C). Corresponding CT images show marginally enlarged lymph node (D) and bladder wall thickening (E) (arrows).
A total of 373 lymph nodes were removed (mean, 14.4; median, 14.0 per patient). A total of 101 lymph nodes (mean, 14.4; median, 12.0 per patient) showed involvement (pN1 or pN2). For LND, the following values were calculated: mean LND, 14.9%; median LND, 16.7%. In patients with lymph node involvement, the mean size of the lymph nodes was 12 mm (median size, 11 mm), and the respective lymphatic lesion (metastasis) measured, on average, 8.3 mm (median, 7 mm).
The 4 lesions depicted by 11C-choline PET but not detected by CT were 1 lymph node (Fig. 2) and 3 bladder lesions that were later confirmed as being positive for tumor tissue at histologic examination. The 5 lesions not detected by both modalities were in the bladder wall (n = 1), at the lymph node level (n = 3), and on the peritoneal surface (n = 1) (only microscopically evident). In particular, in 5 patients with lymph node involvement and nodes found positive by PET (PET-positive nodes), the median size of the affected nodes was 14 mm (range, 6–20 mm), and the median size of the metastatic lesions within the lymph nodes was 10 mm (range, 5–16 mm). In 3 patients with lymph node involvement and PET-negative nodes, the median size of the affected nodes was 9 mm (range, 6–21 mm), and the median size of the metastatic lesions within the lymph nodes was 3 mm (range, 1–15 mm).
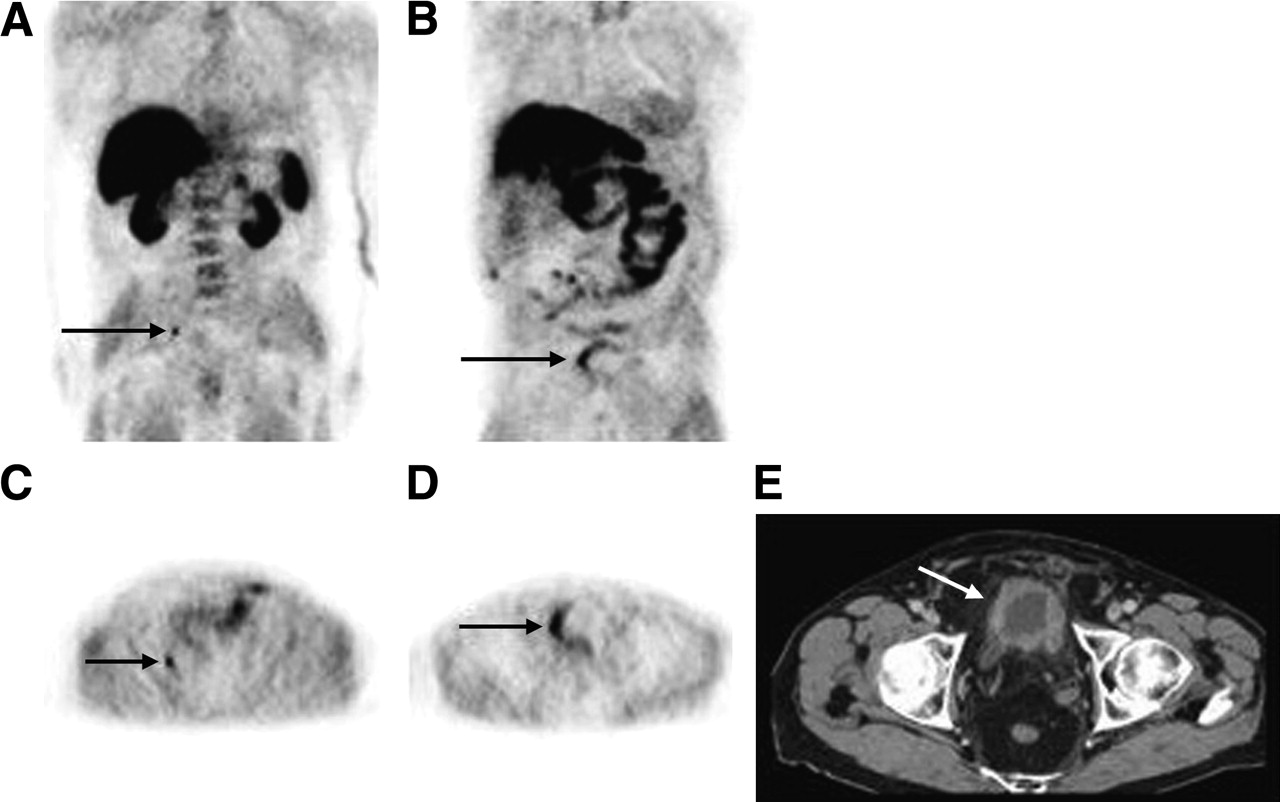
Increased 11C-choline uptake at right lymph node lateral and dorsal to bladder and at right bladder wall on coronal whole-body PET images (A and B) and on corresponding transaxial PET images (C and D). CT image shows concentric bladder wall thickening (E) (arrow).
In 2 of 27 patients, the TURB procedure resulted in the complete resection of bladder cancer (stage pT1 or pT2 at TURB), as verified by histologic evaluation of the cystectomy specimen (pT0). CT correctly detected the absence of disease in both patients, whereas PET yielded a false-positive result in 1 patient (stage pT1 at TURB). In a single patient, a mucosal Tis lesion found at the time of resection was considered undetectable by PET and CT. Because the PET and CT results were positive, detection of this lesion was counted as a false-positive result for PET and CT. For all false-positive results (pT0 and Tis), histologic examination verified the presence of significant inflammatory tissue in the bladder wall.
Histologic evaluation yielded negative results for lymph node metastases after PLND in 19 of 27 patients (70%). The absence of tumor involvement was correctly diagnosed in 13 of these 19 patients (68%) by CT and in all 19 patients (100%) by 11C-choline PET. The 6 false-positive results of CT were enlarged lymph nodes, histologically proven to be reactive. In 2 patients, focal 11C-choline uptake was noted at the inguinal level, but this finding was considered to represent a postsurgical inflammatory response and was not considered in the data analysis.
A small peritoneal lesion, histologically proven after surgery, was not detected by either CT or 11C-choline PET. None of the patients had positive findings at bone scintigraphy, and distant soft-tissue metastases were detected by neither CT nor 11C-choline PET.
CT and 11C-choline PET results and corresponding sensitivity, specificity, and accuracy for staging of residual bladder cancer and lymph node involvement are presented in Tables 1 and 2. The overall accuracy of 11C-choline PET was significantly better than that of CT at the lymph node level (P < 0.01) but not at the level of the bladder wall.
Contrast-Enhanced CT and 11C-Choline PET Findings at Bladder (TU) and Lymph Node (LN) Levels
Sensitivity, Specificity, and Accuracy of Contrast-Enhanced CT and 11C-Choline PET for Detecting Possible Residual Bladder Cancer After TURB and Lymph Node (LN) Involvement
DISCUSSION
For advanced bladder cancer, PLND in combination with cystectomy is performed at most institutions. However, the justification for the routine use of lymph node dissection has been questioned because of the increased morbidity and uncertain benefit of PNLD, because only 15%–28% of patients are found to have lymph node metastatic disease at histologic analysis (4,5,10,13,14). Although guidelines for the PNLD surgical procedure are still controversial, there is a growing acceptance of the notion that the noninvasive diagnosis of lymph node involvement of disease would be beneficial. Recent progress in diagnostic imaging by CT and MRI with contrast enhancement has allowed the lymph node staging of bladder cancer, but the results have been generally disappointing. With cross-sectional imaging modalities, metastatic lymph node involvement is assessed by size, which can be misleading, especially after TURB is performed. PET techniques are based on functional rather than morphologic criteria, and their role in the staging and restaging of cancer has been increasingly recognized. However, the most widely used PET tracer, 18F-FDG, is inappropriate for the imaging of bladder cancer patients because its physiologic urinary excretion interferes with the imaging of tumors in the urinary tract (20). More recently, Hara et al. introduced 11C-choline as a PET tracer for the whole-body imaging of various malignancies (21). 11C-choline generally displays high uptake in tumor tissues and is regarded as a favorable tracer for pelvic malignancies because of its negligible secretion into the urinary system.
The mechanism of 11C-choline uptake has been studied and is related to the biosynthesis of phospholipids, which are essential components of all cell membranes. Because carcinogenesis is characterized by enhanced cell proliferation, increased levels of phospholipids are present. The presence of choline transporters also seems to be involved in the process of 11C-choline uptake in tumor cells, but this mechanism is still under investigation. Moreover, one of the most studied oncogenes, ras, has been shown to activate choline kinase and phospholipase D, 2 enzymes responsible for the synthesis of phosphatidylcholine. In addition to their essential function as structural components of cell membranes, phospholipids are involved in the modulation of transmembrane signaling and thereby in cell proliferation and transformation (27).
11C-choline has been reported to successfully visualize various tumors with a high signal-to-background ratio, including slowly growing tumors, such as prostate cancer, which are often 18F-FDG negative (22,28,29). Furthermore, with 11C-choline, a high signal-to-noise ratio can be achieved in tumors located in the pelvis, in which background radioactivity is low (28,30,31).
The principal disadvantage of 11C-choline is the short half-life of 11C (20 min), limiting its use to centers with an on-site cyclotron. Therefore, 18F-labeled analogs of 11C-choline have been developed (32,33). The principal mechanism of uptake of 18F-labeled choline analogs is very similar to that of 11C-choline. However, the most relevant difference is the significant secretion of radioactivity into the urinary system resulting from 18F-labeled analogs, compared with that of 11C-choline. Although urinary activity from 18F-labeled analogs could be overcome with aggressive hydration, diuresis, and irrigation catheters, it represents a relevant disadvantage for pelvic imaging.
The usefulness of 11C-choline PET for the detection of lymph node involvement has been shown for prostate cancer by de Jong et al. (34). The reported sensitivity, specificity, and accuracy for lymph node staging of prostate cancer were 80%, 96%, and 93%, respectively, suggesting that this technique has a higher sensitivity than CT or MRI. False-positive results may occur because of focal bowel activity or reactive lymph nodes (30,34). False-negative findings have been described for lymph node lesions smaller than 1 cm in diameter. In addition, de Jong et al. (35) recently reported the first clinical experience on the visualization of bladder cancer with 11C-choline PET. They showed that 11C-choline uptake in bladder cancer is feasible for visualizing the extent of tumor because of the virtual absence of urinary activity. In addition, premalignant and small noninvasive tumors did not show increased 11C-choline uptake.
The present study compared, for the first time, the value of 11C-choline PET and contrast-enhanced CT for the staging of advanced bladder carcinoma with rigorous histologic analysis (including lesion size measurements) as a reference. In our series of 27 patients after radical cystectomy and PLND, the number of correctly detected lesions was marginally higher with 11C-choline PET than with CT. In particular, the sensitivity of 11C-choline PET was superior to that of CT for both the detection of residual bladder wall involvement and lymph node staging. The presence of false-negative results obtained for both bladder cancer sites (n = 1) and lymph node involvement (n = 3) by 11C-choline PET likely is related to its restricted spatial resolution, limiting its sensitivity for small lesions. In this study, the actual sizes of cancerous lesions within involved lymph nodes were measured. 11C-choline PET failed to demonstrate 1 larger (15 mm) metastatic lesion as well as 2 additional lesions that were below the resolution of the PET scanners (1 and 3 mm). All remaining lymph node metastatic lesions (between 5 and 16 mm) were correctly identified.
In the present study, PET and CT acquisitions were performed with different scanners. We consider it unlikely that this fact had a significant influence on the study results. With regard to PET, both scanners have very similar physical performance characteristics (23,24). More importantly, image reconstruction was performed in identical ways; the method of image reconstruction has been demonstrated to influence SUV measurements by as much as 25% (36). With regard to CT, the most important parameters that define image quality in the transverse plane, slice thickness, tube voltage, and tube current, and contrast phase (portal-venous phase) were very similar or identical for the CT scanners used. Therefore, besides a better resolution in the z-axis, the most significant difference would be the faster scan time of a 16-slice scanner than of a single-slice scanner. However, all scans were of diagnostic quality, and only transverse planes were analyzed. We did not include multiplanar reconstructions or 3D reconstructions, in which z-axis resolution would have been important. Therefore, the use of different scanners is regarded as being of minor relevance to the results of this study.
At the level of the bladder wall, 11C-choline PET yielded false-positive results for 2 patients (considering 1 Tis lesion undetectable). In these 2 patients, the time intervals between TURB and PET were only 5 and 8 d, whereas the intervals were longer than 2 wk in all other patients. Therefore, false-positive results at the level of the bladder wall may have been avoided by use of a time interval of at least 2 wk between TURB and PET. At the lymph node level, no false-positive results were obtained, with the exception of 2 involved inguinal lymph nodes that were considered reactive lymph nodes after surgery. These findings were not considered in the data analysis, because inguinal lymph node metastases from bladder cancer are highly unlikely. Nevertheless, the existence of nonspecific uptake resulting from 11C-choline in inflammatory lesions is an important finding, because it provides evidence for 11C-choline accumulation in inflammatory lesions.
The results of the present study showed that the overall accuracy for detecting lymph node metastatic disease was better with 11C-choline PET than with CT (P < 0.01), mainly because 11C-choline PET was not sensitive to the inflammatory changes seen in pelvic and abdominal lymph nodes by CT when used to assess lymph node size; thus, 11C-choline PET yielded no false-positive results when used to assess lymph nodes. At present, CT is the most commonly used noninvasive study for the staging of bladder cancer. Our data suggest, however, that CT, despite the use of helical thin contiguous sections and intravenous contrast medium, remains limited in this respect. It appears to be clinically relevant that 11C-choline PET yielded fewer false-positive results than did CT, suggesting that 11C-choline PET may be particularly useful in evaluating patients with nodal enlargement or nodes with borderline sizes.
Although no false-positive 11C-choline PET findings were reported for pelvic and abdominal lymph nodes in our series of patients, the use of integrated PET/CT certainly will provide diagnostic benefits, because focal uptake can be better delineated as resulting from lymph node involvement rather than nonspecific focal bowel activity. In addition, integrated PET/CT also will be beneficial for SUV analyses. In the present study, a partial-volume correction based on CT volume data was not considered because PET and CT images were obtained during separate sessions, resulting in different patient positioning. However, PET/CT is expected to improve lesion identification based on SUV measurements, because partial-volume correction can be applied for small lesions without problems related to changes in positioning and markedly different levels of bladder filling.
CT and 11C-choline PET findings were correlated with surgical and histopathologic results. No distant metastases were found in this series. However, 11C-choline PET is a whole-body technique that allows the detection of distant metastases in a single study (29) and thereby allows appropriate changes to therapeutic management. Nevertheless, because of its excellent spatial resolution, CT is expected to be superior to 11C-choline PET for the assessment of the extent of bladder wall involvement, which was not assessed in the present study.
CONCLUSION
Our preliminary data suggest that 11C-choline PET is comparable to CT for detecting primary bladder cancer but promises better sensitivity and specificity than CT for detecting lymph node metastases. The results of the present study support the further analysis of 11C-choline for evaluating locally advanced bladder cancer.
If additional studies, especially those with PET/CT, confirm our results, then a reliable system for the identification of lymph node metastases would be of particular clinical interest. In fact, 11C-choline imaging may allow for the selection of patients for possible neoadjuvant treatment before radical bladder resection. In addition, the identification of metastatic lymph nodes outside the area of standard PLND will allow for the removal of positive nodes detected by 11C-choline, which may translate to survival benefits for patients.
Acknowledgments
We thank the cyclotron crew for the timely production of 11C-choline and the PET technicians for their support of this study.
Footnotes
-
↵* Contributed equally to this work.
References
- Received for publication December 9, 2005.
- Accepted for publication February 11, 2006.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Nodal disease assessment in pelvic malignancy
- Detection of Aggressive Primary Prostate Cancer with 11C-Choline PET/CT Using Multimodality Fusion Techniques
- Preliminary Study of Detecting Urothelial Malignancy with FDG PET in Taiwanese ESRD Patients
- NCCN Task Force: Clinical Utility of PET in a Variety of Tumor Types
- Nuclear Imaging Probes: from Bench to Bedside