


Abstract
Safety, targeting, and antitumor efficacy of pretargeted radioimmunotherapy using anti-carcinoembryonic antigen (CEA) hMN-14 × m734 bispecific antibody (BsmAb) and 131I-di-diethylenetriamine pentaacetic acid (DTPA)-indium hapten were evaluated in a phase I study performed on patients with CEA-expressing tumors. Methods: Twenty-two patients with nonmedullary thyroid carcinoma (non-MTC) (group I, 13 patients) or medullary thyroid carcinoma (MTC) (group II, 9 patients) were enrolled. These patients received a 75 mg/m2 (11 patients) or 40 mg/m2 (11 patients) dose of BsmAb and escalating activities of 131I-di-DTPA-indium 5 d later. Toxicity and tumor response were assessed in 20 patients who received a therapeutic (>2.2 GBq) hapten dose of radioactivity. Results: The percentage of lesions detected by immunoscintigraphy after injection of the therapeutic dose of hapten was 70% on an anatomic-site basis. High bone uptake was relatively frequent. A transient grade I or II hepatic toxicity was observed in 5 patients (45%) injected with 75 mg/m2 of BsmAb and in 1 patient (11%) injected with 40 mg/m2. No other nonhematologic toxicity was observed. With 75 mg/m2 of BsmAb, hematologic toxicity was high: 5 cases of grade III or IV leukopenia (45%) and 5 cases of grade III or IV thrombopenia (45%). With a 40 mg/m2 dose of BsmAb, hematologic toxicity was reduced significantly: 3 cases of grade III or IV leukopenia (33%) and 1 case of grade III or IV thrombopenia (11%) (P = 0.02). Toxicity was significantly higher in MTC patients than in non-MTC patients (P = 0.019). Nine cases of tumor stabilization of 3 mo to more than 12 mo were observed (45%), 6 in the MTC group and 3 in the non-MTC group. The rate of disease stabilization was significantly higher with 75 mg/m2 of BsmAb (64%) than with 40 mg/m2 (22%) (P = 0.04). Human antimouse antibody elevation was observed in 1 patient (8%) and human antihuman antibody in 4 (33%). Conclusion: A BsmAb dose of 40 mg/m2 and a 5-d interval appeared to be a better dose/schedule regimen, with acceptable toxicity. Under these conditions, the maximal tolerated activity was 3 GBq of 131I-di-DTPA-indium in MTC patients. In non-MTC patients, dose escalation should continue.
- bispecific antibodies
- carcinoembryonic antigen
- medullary thyroid carcinoma
- pretargeting
- radioimmunotherapy
Radioimmunotherapy (RIT) is a validated therapeutic modality for the treatment of non-Hodgkin's lymphoma. Several clinical studies have shown high response rates for both myeloablative and nonmyeloablative doses and improved survival for myeloablative doses in patients with recurrent or refractory lymphoma (1,2). Mainly because of a low therapeutic index with the current 1-step RIT using directly labeled antibodies, RIT has not yet shown sufficient antitumor effects in the more radioresistant solid tumors of metastatic disease for it to be considered a new therapeutic option (3,4).
Pretargeting strategies have been proposed to overcome this problem (5,6). In the first step, an unlabeled antitumor immunoconjugate is injected. In a later step, when the immunoconjugate has sufficiently cleared from the circulation, the radionuclide is injected coupled to a rapidly clearing reagent with high affinity for the immunoconjugate prelocalized in the tumor. Interesting clinical results have been obtained with the avidin/biotin system, with the help of one or several chase steps to clear excess high-affinity (dissociation constant, 10−15 mol/L) antibody–avidin complexes (7). The affinity enhancement system is another pretargeting technique that uses a bispecific monoclonal antibody (BsmAb) and a radiolabeled bivalent hapten. In this system, the affinity of the hapten for the BsmAb is limited (dissociation constant, 10−8 mol/L), but the bivalent hapten binds avidly to the immunoconjugate bound to the surface of target cells, whereas hapten–BsmAb complexes in the circulation can dissociate and excess hapten is cleared, at least in part, through the kidneys. Increased tumor–to–normal tissue ratios and reduced toxicity have been demonstrated in animal RIT studies (8–11). Preclinical studies to further improve tumor-to-blood ratios by a chase step are in progress (12). Two phase I/II clinical trials assessing the murine anti-carcinoembryonic antigen (CEA) × anti-diethylenetriamine pentaacetic acid (DTPA)-indium BsmAb (F6 × 734) and 131I-di-DTPA-indium hapten in 27 patients with medullary thyroid carcinoma (MTC) and in 15 patients with small cell lung carcinoma (SCLC) recurrences showed encouraging therapeutic results (13,14). However, hematologic toxicity was high, especially in MTC patients, and immune responses of the patients to the murine immunoglobulin were frequent. Further optimization of the treatment and the development of chimeric or humanized BsmAb appeared to be necessary.
The purpose of this prospective study was to evaluate the safety, tumor targeting, and antitumor efficacy of the chimeric hMN-14 (humanized CEA antibody) × m734 (murine antihapten-chelate antibody) BsmAb administered at 2 different doses and escalating 131I-di-DTPA-indium hapten activity injected 5 d later. Patients with CEA-positive tumors were enrolled in a phase I clinical RIT trial designed to optimize pretargeting parameters. Preliminary pharmacokinetic and dosimetric results of this trial have been published (15).
MATERIALS AND METHODS
Eligibility
Patients more than 18 y old, with histologically proven CEA-expressing tumors (MTC or cancer of the colon, rectum, stomach, esophagus, pancreas, gallbladder, breast, or lung) and at least 1 known tumor site measurable by CT or MRI, were eligible for the study. Those with MTC were considered a separate group. All patients had a Karnofsky performance status of at least 70% and a minimum life expectancy of 3 mo. For entry into the study, patients were required to be at least 4 wk beyond any major surgery, external radiotherapy, or chemotherapy. The patients were required to have normal levels of bilirubin (≤1.5 × the upper limit of normal), creatinine (≤1.5 × the upper limit of normal), leukocytes (≥4,000/mm3), granulocytes (≥2,000/mm3), and platelets (≥100,000/mm3). Pregnant or breast-feeding women were excluded, as were premenopausal women not willing to practice adequate birth control methods during the study and for 3 mo afterward. Patients with another known type of intercurrent cancer, a psychiatric disorder, or an unstable condition not allowing isolation during therapy were also excluded. The protocol was approved by the local ethics committee. All patients gave written informed consent.
Preparation, Labeling, and Testing of Reagents
The anti-CEA × anti-DTPA-indium BsmAb hMN-14 × m734 was provided by IBC Pharmaceuticals, Inc., as a 4 mg/mL solution. This BsmAb was constructed by coupling an equimolar amount of the Fab′ fragment of the humanized anti-CEA monoclonal antibody (mAb), hMN-14, to the Fab′ fragment of the murine anti-DTPA-indium mAb, m734, activated by o-phenylene-bismaleimide. The immunoreactivity of the BsmAb for CEA was determined to be 85% by the use of size-exclusion chromatography to measure the fraction of a radioiodinated sample that is shifted, in the presence of excess CEA, toward a shorter retention time as a result of binding to CEA. The ability of the BsmAb to bind to the radiolabeled peptide was similarly demonstrated by size-exclusion high-performance liquid chromatography by measuring the shift of the radiolabeled peptide toward a shorter retention time upon binding to the BsmAb. The bivalent hapten used was N-α-(diethylenetriamine-N,N,N′,N″-tetraacetic acid-N″-acetyl)-tyrosyl-N-ε-(diethylenetriamine-N,N,N′,N″-tetraacetic acid-N″-acetyl) lysine (di-DTPA-TL), obtained by reaction of DTPA dianhydride with tyrosyl-lysine diacetate (9). The di-DTPA-TL hapten was saturated with nonradioactive indium chloride and radiolabeled with 131I under contract by CIS Bio International, using the IODO-GEN method (Pierce). The specific activity of the resulting 131I-di-DTPA-indium hapten was 38–62 MBq/nmol. The radiochemical purity was greater than 95% by paper chromatography. Bindability, measured by incubation in m734 antibody-coated tubes, was greater than 90% (16).
Antibody and Hapten Infusions
In the first part of the study, patients were infused with a 75 mg/m2 dose of BsmAb over 30–45 min. This dose was determined as described earlier from the pharmacokinetic and dosimetry results on 12 patients who received escalating doses of BsmAb (15). Escalating activities of 131I-di-DTPA were administered 5 d later. The first activity level of 131I-di-DTPA was 1.8 GBq/m2 in the non-MTC and MTC patient groups. In the second part of the study, patients received 40 mg/m2 of BsmAb and escalating activities of 131I-di-DTPA 5 d later. The first activity level of 131I-di-DTPA was 2.3 GBq/m2 in the non-MTC group and 1.8 GBq/m2 in the MTC group. The first activity levels were determined from 2 previous phase I/II clinical studies of escalating hapten activity in patients with MTC and SCLC recurrences (13,14). Each successive level of radioactivity was 0.5 GBq/m2 higher than the last. At least 3 patients were included at each level. The dose-limiting activity level was considered to be that producing 1 case of grade IV toxicity. The activity level immediately below the dose-limiting level was considered the maximal tolerated activity. A shielded PerfuCis pump (CIS Bio International) was used for hapten infusion. Patients were kept in lead-shielded rooms for 5–10 d. Using a detection probe, we measured the emission rate 1 m from the patient at the end of the hapten infusion, 4 h later, and every day for 10 d. Patients remained in lead-shielded rooms until the radioactivity emission had decreased to less than 25 μSv/h. To protect the thyroid gland of non-MTC patients from inappropriate irradiation, we gave them 30 drops of a saturated solution of potassium iodine by mouth 3 times daily, from 3 d before until 14 d after the injection of 131I-di-DTPA.
Immunoscintigraphy
Whole-body immunoscintigraphy was performed 3–10 d after the hapten infusion. Anterior and posterior views were obtained with a dual-head camera (DST XL Sophy; Sopha Medical Vision) equipped with a high-energy collimator. The list-mode (step and shoot) method was used. Whole-body immunoscintigraphy images were analyzed by 2 nuclear medicine physicians, who reached a consensus on the findings. A metastatic lesion was defined visually as a focus of increased uptake of radioactivity relative to the adjacent or contralateral region or as diffuse increased uptake in the spine and pelvis. True-positive results corresponded to an abnormal finding on immunoscintigraphy confirmed by histopathology or by another imaging technique (CT, bone scintigraphy, or MRI) performed 30 d before or after the imaging study. True-negative results consisted of normal imaging findings confirmed by histopathologic examination or another imaging technique. A finding that was negative on immunoscintigraphy was considered to be false negative if positive on 1 other imaging method plus histopathology or on 2 other imaging methods. A false-positive finding was one positive on immunoscintigraphy but negative on the other imaging methods and histopathology. The percentage of detected lesions was calculated on an anatomic-site basis using the following formula: (true-positive/true-positive + false-negative) × 100.
Dosimetry
Dosimetry was calculated as previously reported (17). Briefly, cumulative activity in the whole body, tumor, liver, and kidney was determined from whole-body scintigraphy. Images were corrected for attenuation and dead time. The positioning of the patient was made reproducible by the use of a system based on laser sources. Radiation doses absorbed by tumor targets and normal tissues were calculated according to the MIRD scheme. The tumor volume (and thus the mass) was estimated from CT sections and the mass of normal tissues using reference values.
Safety Evaluations
All adverse events occurring from study entry through 12 mo after therapeutic dosing were recorded and graded using the common toxicity criteria (version 2.0) of the National Cancer Institute. Only events occurring after that time and considered possibly or probably related to the study drug were recorded. Safety was assessed by physical examination 15 and 30 d after RIT and at 3, 6, and 12 mo; complete peripheral blood cell counts were obtained every week for 2 mo and at 3, 6, and 12 mo after therapy; and renal and hepatic function was evaluated at 15, 30, 45, and 60 d and at 3, 6, and 12 mo after therapy. Vital signs were monitored before and for 24 h after the infusions.
Human Anti-BsmAb Responses
Anti-antibody responses were monitored before administration of BsmAb and at 1 or 2 mo and at 3 and 6 mo after hapten injection. An antiidiotype enzyme-linked immunosorbent assay was used for human antihuman antibody (HAHA), and the ImmuStrip HAMA-Fragment assay (Immunomedics) was used for human antimouse antibody (HAMA) (18). Positive results for HAMA were those greater than 100 ng/mL. For HAHA, the enzyme-linked immunosorbent assay was performed as follows. Microtiter plates were coated with hMN14 IgG, and the antiidiotype response was detected by mMN14 IgG horseradish peroxidase. The standard curve was established with a rat antiidiotype to hMN14 (WI2; Immunomedics) and was linear between 3.125 and 100 ng/mL. For the assay, each patient sample was diluted 10-fold with 1% bovine serum albumin/phosphate-buffered saline and tested in triplicate. Each patient sample was also spiked with 50 ng of WI2 per milliliter and tested. The assay was considered valid if the spike recovery was between 50% and 150%.
Measurements of Blood Biomarkers
Blood biomarkers (CEA and calcitonin) were measured before administration of the BsmAb and at 1, 3, 6, and 12 mo after the hapten injection. Blood CEA concentrations were determined using the Kryptor rapid random-access immunoassay analyzer (Brahms Diagnostica). A concentration greater than 10 ng/mL was considered abnormal. Blood calcitonin concentrations were measured by radioimmunoassay (Schering-CIS Bio International); positive results were those greater than 10 pg/mL.
Response Criteria
Tumor responses were assessed at 1, 3, 6, and 12 mo after treatment. In addition to physical examinations, tumor biomarker concentrations, CT, and MRI were used to assess therapeutic response. A biomarker response was defined as a decrease of at least 25% in CEA or calcitonin. A complete response was defined as the disappearance of all detectable tumors, and a partial response as a decrease of 50% or more in the sum of the products of the longest perpendicular diameters of all measured lesions. Disease progression was defined as an increase of at least 25% in the diameter of existing lesions, the appearance of new lesions, or an increase of at least 25% in tumor biomarker concentrations. Stabilization was defined as no more than a 25% change in the diameter of existing lesions or biomarker concentrations.
Statistical Analysis
Toxicity and efficacy for the different groups were compared using the Fisher exact test. P values of 0.05 or less were considered significant. BMDP statistical software (version 7.0; Statistical Solutions) was used for the analyses.
RESULTS
Patient Characteristics
Twenty-two patients with cancer of the colon, rectum, lung, or pleura (group I, 13 patients) or with MTC (group II, 9 patients) were enrolled (Table 1). These patients received a 75 mg/m2 (11 patients) or 40 mg/m2 (11 patients) dose of BsmAb and 1.9–5.5 GBq of 131I-di-DTPA 5 d later. Patients 24 and 35 did not receive a full dose of therapeutic activity of the hapten and were not included in the toxicity and response evaluations.
Demographics and RIT Outcome
Adverse Events Associated with BsmAb and Hapten Infusions
Infusions of BsmAb and hapten were tolerated well. Grade I malaise was observed in 2 patients, starting at the end of the antibody infusion in one patient and 15 min after the end in the other. Grade I or II adverse events were observed in 5 patients after the hapten infusion, with malaise at the end of the infusion, erythema 2–4 h after the infusion, and pain and nausea 24 h after the infusion. These symptoms subsided spontaneously.
Nonhematologic and Hematologic Toxicity
A transient grade I or II hepatic toxicity was observed in 5 patients (45%; patients 17, 19, 20, 27, and 29) injected with 75 mg/m2 of BsmAb and in 1 patient (11%; patient 34) injected with 40 mg/m2. Two of these patients (patients 19 and 27) had known liver metastases with preexisting hepatic dysfunction. Hepatic toxicity was observed 19–58 d after infusion of the hapten (median, 33 d). The duration ranged from 8 to 49 d (median, 14 d). No other nonhematologic toxicity was observed. At a 75 mg/m2 dose of BsmAb, hematologic toxicity was high, with 5 patients having grade III or IV leukopenia (45%) and 5 having grade III or IV thrombopenia (45%) (Table 2). At a 40 mg/m2 dose of BsmAb, hematologic toxicity was significantly reduced, with 3 having grade III or IV leukopenia (33%) and 1 having grade III or IV thrombopenia (11%) (P = 0.02). Toxicity was significantly higher in MTC patients than in non-MTC patients (P = 0.019) (Table 2). White blood cells and platelets reached their nadir at 27–44 d (median, 41 d) and 20–41 d (median, 28 d), respectively, after the hapten injection. The duration of the nadir was 3–31 d (median, 8 d) for white blood cells and 6–64 d (median, 13 d) for platelets. With adequate treatment (platelet transfusions, granulocyte colony-stimulating growth factor factor), all patients recovered from their grade III or IV toxicities.
Hematologic Toxicity
Human Anti-BsmAb Responses
Anti-antibody responses were monitored over a period of at least 1 mo for 12 patients and are summarized in Table 3. HAMA elevations were observed in 1 patient (8%) and HAHA elevations in 4 patients (33%). Seven patients were monitored for at least 3 mo after RIT. For 3 patients, the HAHA response was observed only later than 3 mo after RIT. In 2 patients, HAHA titers decreased slowly with time.
Human Anti-BsmAb Immune Responses
Targeting Efficiency
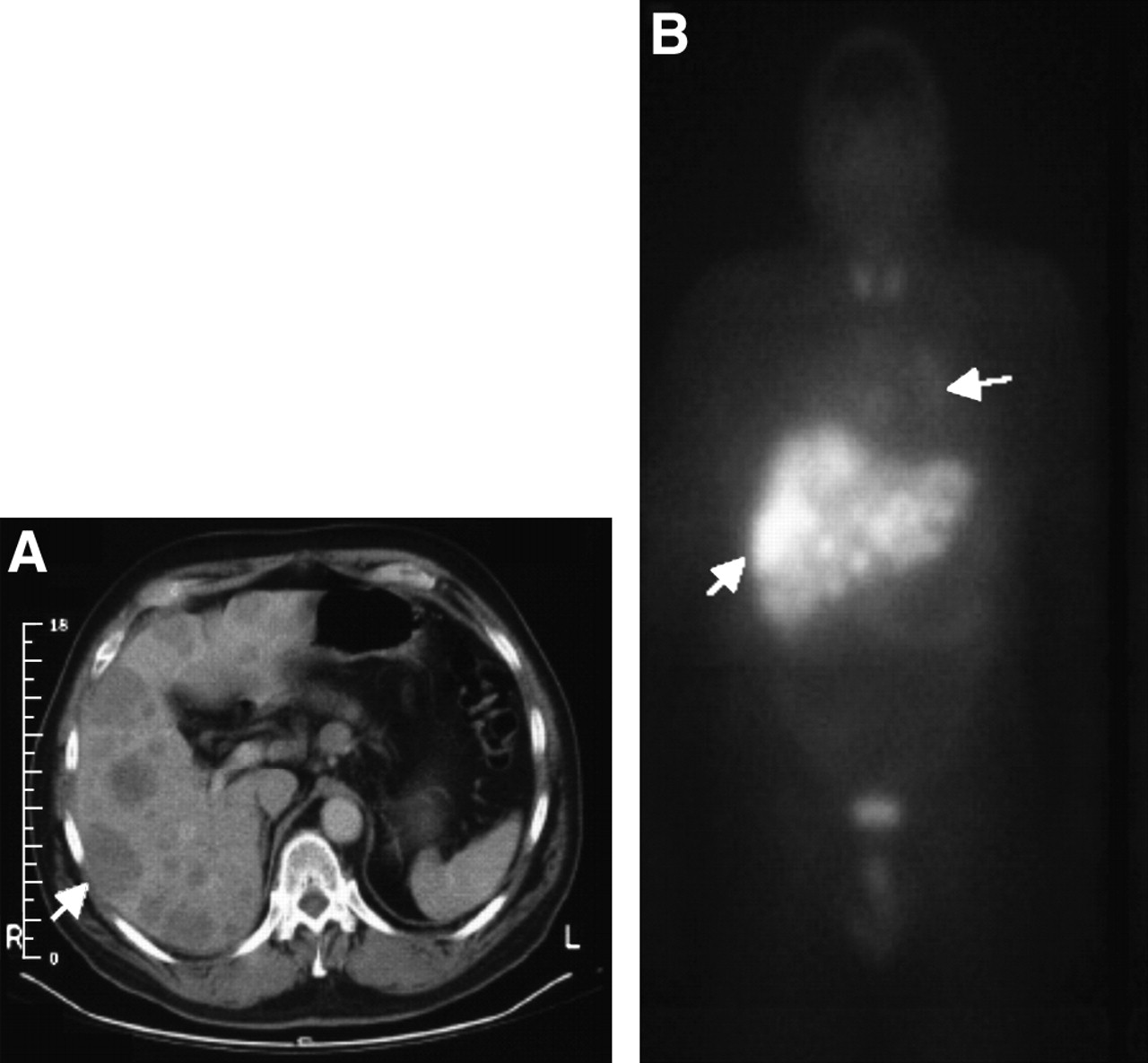
The targeting results are summarized in Table 4. The overall percentage of detected lesions on an anatomic-site basis was 70% for the 19 evaluated patients (49 anatomic sites). The lesions that were not imaged corresponded mainly to lung (32% false-negative) and liver (54% false-negative) metastases that were, generally, less than 1 cm in diameter. Figure 1 shows hapten targeting observed in a patient with liver and lung tumors. High bone uptake was relatively frequent. Uptake in the pelvic and spinal skeleton was qualitatively evaluated in 19 patients. High homogeneous or heterogeneous diffuse uptake was observed in 9 patients, including 7 patients with MTC, 1 with SCLC, and 1 with colon carcinoma. Bone scanning was performed for all patients, and MTC patients also underwent MRI. Six of these 9 patients had either bone or bone marrow metastases demonstrated by MRI or bone scans (Fig. 2). Altogether, 78% of MTC patients and only 15% of non-MTC patients had high uptake in the pelvic and spinal skeleton. Figure 3 shows an MTC patient with targeting of bone and chest metastases and high bone marrow uptake and an SCLC patient with targeting of chest and liver metastases but no bone marrow uptake.
Tumor Imaging Results
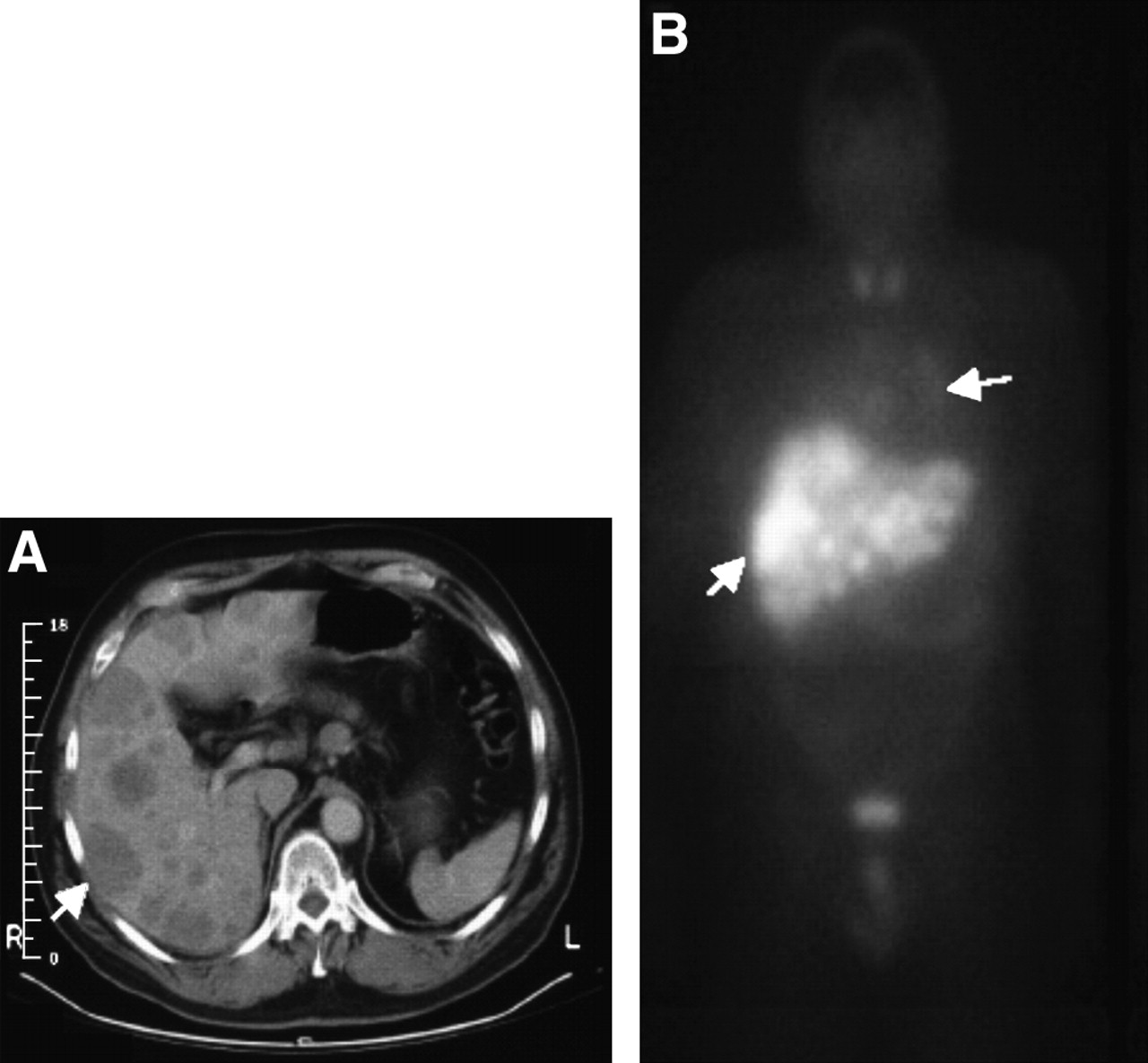
Images of SCLC patient showing thoracic and liver tumor involvement (arrows). (A) CT scan obtained before RIT shows multiple liver metastases. (B) Scintigraphy image (anterior view) obtained 7 d after injection of 131I-hapten shows targeting of thoracic and liver metastases.
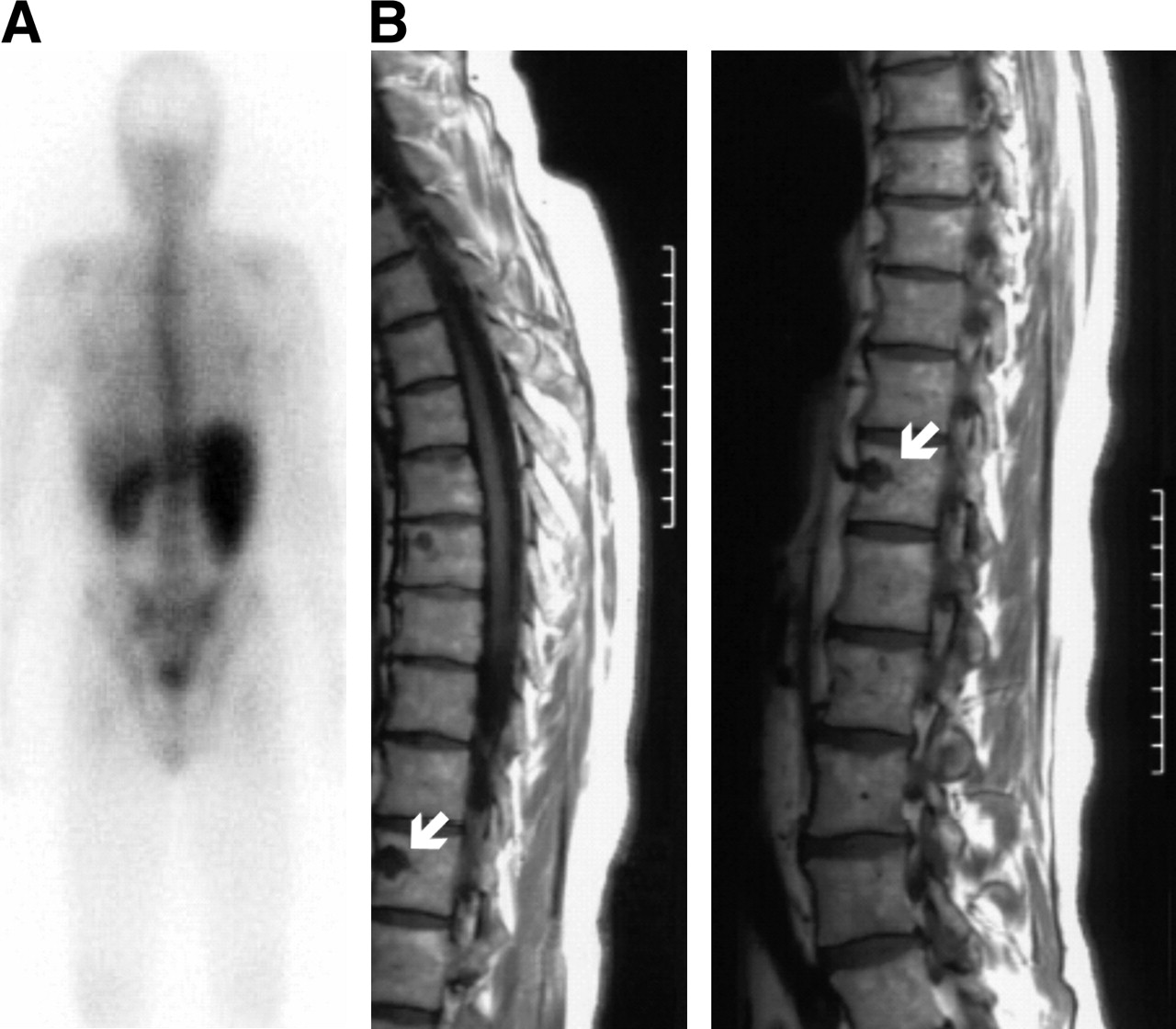
(A) Scintigraphy image (posterior view) obtained 7 d after injection of 131I-hapten shows high bone marrow uptake in MTC patient. (B) MR image of same patient indicates bone marrow metastases (arrows).

Scintigraphy images (posterior view) illustrate distribution of 131I-hapten in MTC patient (A) and SCLC patient (B). Bone marrow uptake is higher in MTC patient.
Dosimetry
Eleven patients were assessable at 75 mg/m2 and 10 patients at 40 mg/m2. With a 75 mg/m2 dose of BsmAb, mean tumor absorbed dose (evaluation of 15 lesions) was 10.7 Gy (range, 1.7–53.5 Gy), and with a 40 mg/m2 dose, mean tumor absorbed dose (evaluation of 14 lesions) was 18.5 Gy (range, 2.4–49.3 Gy). With a 75 mg/m2 dose of BsmAb, whole-body, liver, and kidney mean doses were 0.38 Gy (range, 0.14–0.57 Gy), 1.9 Gy (range, 0.7–3.5 Gy), and 2.4 Gy (range, 1.5–3.9 Gy), respectively, with respective tumor–to–normal tissue mean ratios of 25 (range, 3.0–102), 6.2 (range, 0.5–31), and 7.0 (range, 0.8–33). With a 40 mg/m2 dose of BsmAb, whole-body, liver, and kidney mean doses were 0.33 Gy (range, 0.25–0.41 Gy), 1.4 Gy (range, 0.7–2.3 Gy), and 2.1 Gy (range, 1.5–4.1 Gy), respectively, with respective tumor–to–normal tissue mean ratios of 55 (range, 7.1–150), 14 (range, 1.5–73), and 8.5 (range, 1.4–22).
Responses
Tumor responses are summarized in Table 1. Nine cases of stabilization of 3 mo to more than 12 mo were observed (45% of the 20 patients receiving a therapeutic hapten activity): 6 in the MTC group and 3 in the non-MTC group. The rate of stabilization was significantly higher with 75 mg/m2 of BsmAb (64%) than with 40 mg/m2 (22%) (P = 0.04). These cases of stabilization corresponded to a morphologic tumor and biomarker stabilization. The duration of tumor response correlated with the duration of biomarker response in all patients except patient 01-36, in whom biologic progression preceded tumor progression (Table 1). For MTC patients 01-19 and 01-27, therapeutic efficacy was evaluated by imaging only, because of large fluctuations in calcitonin and CEA blood levels. No obvious correlation was seen between tumor marker fluctuations and HAMA or HAHA levels.
DISCUSSION
Pretargeting techniques are considered to be promising for RIT of solid tumors but require careful optimization of the dose of pretargeting BsmAb, of the administered activity, and of the interval between injection of the pretargeting agent and injection of the labeled product. Here, we have reported toxicity, imaging results, and efficacy assessments for 20 of 35 patients included in a study to determine the optimal BsmAb dose, hapten activity, and pretargeting interval. A previous study of the pharmacokinetics and dosimetry results for these 35 patients found that the optimal BsmAb dose was 40 mg/m2 with a 5-d interval (15). Indeed, with a 7-d interval, a 10 or 30 mg/m2 dose resulted in fast elimination and low hapten tumor uptake and dosimetry, whereas 50 or 100 mg/m2 resulted in favorable tumor accretion of the hapten. The dose of BsmAb was thus set at 75 mg/m2, and the pretargeting time was reduced to 5 d. With these parameters, tumor hapten uptake was favorable, but hapten blood clearance was too slow, resulting in high blood and whole-body dosimetry. This finding indicated that the BsmAb dose was too high with a 5-d pretargeting interval. Reduction of the BsmAb dose to 40 mg/m2 accelerated hapten clearance without compromising tumor dosimetry (15). Tumor targeting, as well as the toxicity and efficacy of the treatment, were then assessed in the 20 patients injected with BsmAb doses of 40 and 75 mg/m2, and therapeutic activities of the 131I-labeled hapten as reported here.
The imaging findings could be interpreted as not entirely supporting the conclusions of the earlier dosimetry study. In that study, targeting was evaluated in terms of dosimetry calculated for all tumor sites at which tumor size and radioactivity uptake could be quantified over time by scintigraphy (15). Here, imaging results are discussed with respect to the number of imaged tumor sites per anatomic area and are expressed in terms of sensitivity. The sensitivity calculations reported in Table 4 show that a BsmAb dose of 40 mg/m2 and a 5-d interval may not be as good as the higher dose of 75 mg/m2. In the dosimetry study, the number of assessed tumors was much lower because we considered only clearly delineated tumor sites at which a tumor could be measured by imaging, possibly introducing a bias in the comparison of the 2 dose levels. The important point here is that activity uptake was detected in a large fraction (70%) of tumor sites with the hapten, thus reducing the risk that high uptake was limited to a small fraction of tumors.
The toxicity data reported here confirm earlier observations that hematologic and hepatic toxicities were markedly reduced with the 40 mg/m2 dose of BsmAb, compared with the 75 mg/m2 dose. This finding is consistent with dosimetry calculations that showed higher whole-body and liver mean radiation doses at 75 mg/m2 (0.38 and 1.9 Gy for whole body and liver, respectively) than at 40 mg/m2 (0.33 and 1.4 Gy for whole body and liver, respectively). No relationship was observed between prior therapy or immune response and toxicity. Toxicity appeared related primarily to dosing parameters and was significantly higher in the MTC group than in the non-MTC patients who had received a greater number of prior treatments. This finding agrees with our previous studies that showed a lower maximum tolerated dose in MTC patients than in SCLC patients for affinity-enhancement-system pretargeted RIT (13,14). The hematologic toxicity can be explained by a diffuse metastatic involvement of the bone marrow. Previous imaging studies showed a high frequency of bone or bone marrow involvement in advanced MTC (19). Seventy-eight percent of MTC patients in this study had diffuse bone metastases detected by MRI or bone scanning. In the MTC group, despite the use of optimized pretargeting conditions (BsmAb at a dose of 40 mg/m2), 1 case of grade IV hematologic toxicity was observed, preventing further dose escalation. In the non-MTC group receiving a 40 mg/m2 dose of BsmAb at a 5-d pretargeting interval, none of the criteria defining the dose-limiting toxicity were observed (no grade III or IV hematologic toxicity of more than 14 d or grade III or IV nonhematologic toxicity). Thus, doses of the 131I-di-DTPA hapten could be escalated beyond 5.5 GBq in this group. Because of the very different toxicity profiles in the MTC and non-MTC patients and the 2 dose groups, the relationship between toxicity and whole-body dosimetry reported previously (15) was not clearly demonstrated. Whole-body doses of between 14 and 52 cGy were given to all the patients discussed here except for 1 non-MTC patient, who received 57 cGy and showed transient grade IV hematologic toxicity. Such whole-body doses are not supposed to be toxic, but dosimetry calculations did not take into account skeletal uptake, which certainly contributed to bone marrow exposure.
In this study, therapeutic efficacy was modest, with no complete or partial responses. Dosimetry calculations showed that the mean tumor dose did not differ between the group treated with 40 mg/m2 (18.5 Gy; range, 2.4–49 Gy) and the group treated with 75 mg/m2 (10.5 Gy; range, 1.7–53 Gy). Dosimetry calculations could not be correlated reliably with clinical observations (progression vs. disease stabilization), because of the small number of patients with stable disease for whom tumor dosimetry was quantifiable. A stabilization rate of 45% was observed, with prolonged disease stabilization occurring in about half the MTC patients. These results are especially encouraging because most patients in this study were at advanced stages of disease, with a large tumor burden and high tumor marker concentrations (i.e., conditions in which internal radiotherapy is expected to be of little benefit) (4). Preclinical and clinical studies have shown favorable therapeutic results with affinity-enhancement-system RIT in MTC, probably because the tumor is well vascularized and strongly expresses CEA (10,11,20,21). A dosimetry and pharmacokinetics clinical study comparing the targeting of several types of tumors showed the highest tumor uptake values for colorectal cancer and MTC (22). Because the half-life of uptake is longer for MTC tumors, they received higher mean irradiation doses. Moreover, small metastases, particularly in the spine, are often observed in MTC patients, and dosimetric studies showed that small lesions received potentially tumoricidal irradiation (1.1–3.8 cGy/MBq) (13,17). A higher stabilization rate was observed with 75 mg/m2 than with 40 mg/m2, but more MTC patients were in the group treated with the higher BsmAb dose (6/11 vs. 3/9). However, even if tumor targeting is better with 75 mg/m2, the low toxicity observed with 40 mg/m2 should allow us to increase hapten radioactivity in non-MTC patients, and this increase should increase the tumor dose and probably also RIT efficacy.
This study also showed that chimerization (human-murine BsmAb) reduced the immune response rate but did not entirely solve the problem of immunogenicity. This result is not surprising, because no antibody response was observed in an earlier clinical study with hMN-14 in which 19 patients received a 0.5- to 20.0-mg injection of mAb (23). However, the immune response rate is lower than that observed with the parental murine MN-14 mAb; HAMA developed in 64% of antibody-naive patients who received a 16- to 100-mg injection of 131I-MN-14 (24). In comparison, in the earlier affinity-enhancement-system RIT trial using the fully murine BsmAb, the immune response rate was higher, with HAMA observed in 9 (53%) of the 17 assessed patients (13). However, fully humanized recombinant BsmAb has now been prepared (25) and should replace the chimeric chemical constructs in the future, solving the problem of immunogenicity and also reducing manufacturing costs.
CONCLUSION
In conclusion, this study confirms the previous pharmacokinetic and dosimetry analyses. Most disease stabilization occurred with the 75 mg/m2 dose of BsmAb administered at a 5-d interval, but the rate of hematologic toxicity was relatively high. With a 40 mg/m2 dose of BsmAb and a 5-d interval, hematologic toxicity was reduced, making it possible to safely administer higher radionuclide doses. This study also confirmed that the risk of severe hematologic toxicity is higher in MTC patients than in patients with other CEA-expressing tumors and that the maximum activity that may be administered in advanced MTC is limited to 1.8 GBq/m2. Nevertheless, encouraging therapeutic results have been observed. A phase II study using this optimized pretargeted RIT should begin soon, with evaluation of response rate, time to progression, and overall survival as end-points in 2 separate groups of MTC patients: those with minimum residual disease (elevated calcitonin without imaging evidence of disease) and those with measurable disease. In non-MTC patients, this study shows that hapten doses of 5.5 GBq and higher could be tolerated, probably increasing antitumor efficacy. Several authors have suggested that, for the management of relatively aggressive solid tumors, RIT should be used in minimal disease and in combination modalities (4). Because synergistic antitumor effects between RIT and chemotherapy have been demonstrated in animal studies (4,26,27), this possibility should be tested against solid tumors in future clinical trials of pretargeted RIT.
References
- Received for publication July 4, 2005.
- Accepted for publication October 5, 2005.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Pretargeting: A Path Forward for Radioimmunotherapy
- Intraperitoneal Pretargeted Radioimmunotherapy for Colorectal Peritoneal Carcinomatosis
- Current Landscape in Clinical Pretargeted Radioimmunoimaging and Therapy
- Therapy of Myeloid Leukemia using Novel Bispecific Fusion Proteins Targeting CD45 and 90Y-DOTA
- "Catch-and-Release" Anti-Carcinoembryonic Antigen Monoclonal Antibody Leads to Greater Plasma and Tumor Exposure in a Mouse Model of Colorectal Cancer
- Pretargeted Imaging and Therapy
- Establishment of the In Vivo Efficacy of Pretargeted Radioimmunotherapy Utilizing Inverse Electron Demand Diels-Alder Click Chemistry
- Immuno-PET Using Anticarcinoembryonic Antigen Bispecific Antibody and 68Ga-Labeled Peptide in Metastatic Medullary Thyroid Carcinoma: Clinical Optimization of the Pretargeting Parameters in a First-in-Human Trial
- Phase II Trial of Anticarcinoembryonic Antigen Pretargeted Radioimmunotherapy in Progressive Metastatic Medullary Thyroid Carcinoma: Biomarker Response and Survival Improvement
- Convergent Potency of Internalized Gelonin Immunotoxins across Varied Cell Lines, Antigens, and Targeting Moieties
- Pretargeted 177Lu Radioimmunotherapy of Carcinoembryonic Antigen-Expressing Human Colonic Tumors in Mice
- An experimental and theoretical evaluation of the influence of pretargeting antibody on the tumor accumulation of effector
- Multifunctional Antibodies by the Dock-and-Lock Method for Improved Cancer Imaging and Therapy by Pretargeting
- Pathology Underrates Colon Cancer Extranodal and Nodal Metastases; Ex vivo Radioimmunodetection Helps Staging
- Pretargeted Anti-Carcinoembryonic-Antigen Radioimmunotherapy for Medullary Thyroid Carcinoma
- Radioimmunotherapy of Solid Tumors: The Promise of Pretargeting Strategies Using Bispecific Antibodies and Radiolabeled Haptens