


Abstract
Adenoviral Na/I symporter (NIS) gene transfer has emerged as a promising method for myocardial gene imaging but concern over possible perturbation of cardiac function persists. In this study, we addressed this issue with cultured cardiac cells and serial echocardiography, creatine kinase (CK) measurements, and histologic examination of rats intramyocardially injected with an adenovirus that expresses both NIS and enhanced green fluorescent protein (EGFP) (Ad.EGFP.NIS) or a control virus (Ad.EGFP). Methods: H9C2 cardiac myoblasts differentiated into cardiomyocytes were evaluated for the effect of Ad.EGFP.NIS and Ad.EGFP infection on viable cell number and 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) assays. Rats injected intramyocardially with 3 × 108 plaque-forming units of Ad.EGFP.NIS (n = 9) or Ad.EGFP (n = 8) underwent serial echocardiographic measurements of heart rate, left ventricular (LV) dimensions, ejection fraction (EF), and fractional shortening (FS) on the day before and on days 4 and 9 after gene transfer. Five Ad.EGFP.NIS rats also underwent repeated 123I imaging from which ratios of cardiac to mediastinal counts (C/M ratios) were obtained. Separate rats underwent serial measurements of serum CK, myocardial myeloperoxidase assays, and microscopic assessment of inflammation. Results: Cultured cardiac cells showed no change in cell viability or proliferation at 4 and 9 d after Ad.EGFP.NIS or Ad.EGFP infection compared with controls. 123I scintigraphy demonstrated high cardiac radiouptake at Ad.EGFP.NIS injection sites by days 2 and 4 (C/M ratios, 5.0 ± 0.6 and 5.1 ± 1.0, respectively), followed by a complete loss of uptake by day 9 (C/M ratio, 1.4 ± 0.0). Serial echocardiography revealed no difference in heart rate, LV dimensions, or functional parameters between Ad.EGFP.NIS and Ad.EGFP groups at any given time. Mild reductions in LVEF and LVFS by day 9 compared with baseline were similar for both Ad.EGFP (88.2% ± 6.4% vs. 79.6% ± 5.0% for LVEF and 0.55 ± 0.10 vs. 0.44 ± 0.05 for LVFS) and Ad.EGFP.NIS groups (88.0% ± 5.4% vs. 78.7% ± 4.6% for LVEF and 0.54 ± 0.09 vs. 0.42 ± 0.05 for LVFS). Serial serum CK and myocardial myeloperoxidase activities were not elevated in either group, in contrast to substantial increases found after ischemia–reperfusion injury. Histology revealed similar mild inflammatory cell infiltration restricted to the injection site for both groups. Conclusion: The results of this study demonstrate that myocardial NIS gene imaging does not cause significant myocardial injury or perturbed cardiac function, other than mild effects likely due to adenoviral vector–associated host response. Thus, this practical and convenient reporter gene strategy can be used safely for noninvasive myocardial gene imaging in living subjects.
Cardiac gene transfer holds promise as a potential molecular therapeutic approach for treating such diseases as myocardial ischemia and heart failure (1–3). Gene delivery techniques are also a powerful research tool to help unveil the molecular and cellular basis of myocardial pathophysiology. Among the several gene delivery methods used in the cardiovascular system, adenoviral vectors allow high transduction efficiency and have demonstrated the greatest utility to date (3–6). For the widespread application of cardiac gene transfer for preclinical research and in the clinical arena, it is critical to be able to monitor the magnitude and spatial distribution of transgene expression, to evaluate change of expression levels over time, and to assess how these parameters correlate with functional improvement. As such, reporter gene techniques have recently been developed to provide noninvasive imaging of gene expression in the heart of living subjects (7,8). Myocardial injection of adenovirus containing the herpes viral thymidine kinase gene in rats allows precise imaging of gene expression using PET and radiolabeled thymidine analogs (9,10). More recently, adenovirus-mediated Na/I symporter (NIS) gene delivery has been confirmed to provide convenient and accurate monitoring of gene expression in rat myocardium using γ-cameras and widely available free radionuclides (11–13).
Because any genes that alter myocardial cell physiology could potentially result in perturbed cardiac function, an important step to further facilitate the widespread application of myocardial gene imaging is to substantiate the safety of the technique in vivo. NIS gene transfer has been investigated extensively in animal models to assess its utility for imaging of gene expression within various organs (14–17) and as a method for targeted radioiodine therapy of cancer (18,19). However, possible untoward effects of high NIS activity on the function of cells that do not normally express the transporter have not been investigated to date. This may be a particular concern for cardiomyocytes, where transferring the ability to enhance the intracellular influx of sodium and various anions could adversely affect the contractile function of the heart. Furthermore, with adenoviral vectors, elicited local immune responses may further contribute to compromised cardiac function. Therefore, we investigated the safety of myocardial NIS gene imaging through cultured cardiac cell experiments and by serial echocardiographic measurements of cardiac function and biochemical or histologic evidence of cardiac injury in rats injected intramyocardially with either an adenovirus that expresses both NIS and enhanced green fluorescent protein (EGFP) or a control adenovirus that expresses only EGFP.
MATERIALS AND METHODS
Recombinant Adenoviral Vectors
Ad.EGFP.NIS is a replication-deficient vector based on human adenoviral serotype 5 that contains cytomegalovirus promoter-driven expression cassettes for the EGFP gene and the full-length human NIS complementary DNA (cDNA) substituted for E1 through homologous recombination. This vector has been shown to produce parallel levels of separate NIS and EGFP proteins in rat myocardial tissue (11). Ad.EGFP, which carries a cytomegalovirus promoter-driven EGFP gene, was used as the control vector. The viruses were amplified in 293 cells, and viral titer was determined by plaque assay.
Cultured Cardiomyocyte Adenoviral Gene Transfer and 123I Treatment
The cellular effects of adenovirus-mediated NIS gene expression and 123I incorporation were evaluated in H9C2 cells that were differentiated into cardiomyocytes. H9C2 cells, myoblasts derived from rat embryonic cardiocytes, were obtained from the American Type Culture Collection and maintained in Dulbecco's modified Eagle medium supplemented with 10% fetal calf serum (FCS) under standard 37°C, 5% CO2 in air conditions. Cells split at a low density in 12- or 24-well dishes were cultured in 10% FCS culture medium for 1 d and then differentiated into cardiomyocytes by methods described by Ménard et al. (20). Briefly, cells were cultured in medium containing 1% FCS with replacement of culture medium every 2 d. Stimulation was performed daily for 7 d with 10 nmol/L all-trans-retinoic acid (Sigma), using aliquots that were used only once after storage at −20°C and were freshly diluted at the time of experiments.
Cardiomyocyte differentiation was verified by immunofluorescent staining with a polyclonal antibody that specifically recognizes the cardiac marker myosin light chain 2v (MLC-2v) (C-17; Santa Cruz Biotechnology, Inc.). Cells rinsed with phosphate-buffered saline (PBS) were fixed with 4% paraformaldehyde for 30 min, permeabilized with 0.03% Triton X-100 (Sigma) for 5 min, and then washed with PBS 3 times. Blocking of nonspecific sites was performed by incubating cells with 3% bovine serum albumin at 37°C for 30 min. Cells were incubated for 1 h at 37°C with the primary antibody (1:100 dilution) in 3% bovine serum albumin solution. Cells were then washed with PBS and incubated for 1 h at 37°C with fluorescein isothiocyanate–conjugated donkey antigoat secondary antibody (1:400 dilution; Santa Cruz Biotechnology, Inc.), and finally inspected under a fluorescent microscope.
Cardiomyocyte differentiated cells were infected with 10 multiplicities of infection (MOIs) of Ad.EGFP or Ad.EGFP.NIS, whereas control cells were not infected. At 4 and 9 d after adenoviral infection, cells were treated with 0 or 185 kBq (0 or 0.5 μCi) of 123I for 6 h. Cells then underwent evaluation for viability and proliferation using direct cell counting in conjunction with 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) assays. Counting the number of cells was achieved by mixing equal volumes of trypan blue (Sigma) to trypsin-ethylenediaminetetraacetic acid–harvested cells followed by direct cell counting using a hemacytometer. For MTT assays, 50 μL of 2 mg/mL MTT stock solution (Sigma) were added to the culture medium. After incubation at 37°C for 4 h, the culture medium was aspirated and 200 μL of dimethyl sulfoxide (Sigma) were added to dissolve MTT-formazan crystals. One hundred microliters of solution from each well were transferred to a 96-well microplate and measured for absorbance at 570 nm.
Rat Intramyocardial Adenovirus Injection and Ischemia–Reperfusion Injury
Sprague–Dawley rats (300–350 g) were studied under protocols approved by the Institutional Guidelines on the Use and Care of Animals. Rats anesthetized with ketamine (80 mg/kg) and xylazine (10 mg/kg) were mechanically ventilated with room air, and sternotomy was performed to expose the beating hearts. The anterolateral wall of the left ventricle (LV) was injected with 3 × 108 plaque-forming units (pfu) of either Ad.EGFP.NIS (n = 9) or Ad.EGFP (n = 8) in 100-μL volumes using a 30-gauge needle. All 17 rats underwent serial echocardiography after intramyocardial adenovirus administration, and all 9 rats of the Ad.EGFP.NIS group were also subjected to intravenous administration of 74 MBq of 123I on days 2, 4, and 9. Separate rats underwent measurements of serum creatine kinase (CK) levels serially after Ad.EGFP.NIS (n = 3) or Ad.EGFP (n = 3) injection. After these animals were sacrificed, myocardial tissue was subjected to myocardial myeloperoxidase (MPO) assays and histologic assessment of inflammatory response.
Four rats underwent myocardial ischemia–reperfusion injury without adenoviral gene transfer as positive controls of myocardial injury. Briefly, rats anesthetized with xylaine and ketamine were mechanically ventilated with room air, and sternotomy was performed to expose the beating hearts. Myocardial ischemia was induced by ligation of the left anterior descending coronary artery for 40 min with a 6.0 silk suture approximately 3–4 mm from its origin. The chest wall was then closed, and the rats were sacrificed 3 d later.
Serial Scintigraphic Imaging with 123I After Gene Transfer
Five rats of the Ad.EGFP.NIS group underwent scintigraphic imaging at 2, 4, and 9 d after myocardial gene transfer. Anesthetized animals were injected in a tail vein with 74 MBq of Na123I (Korean Atomic Energy Research Center, Seoul, Korea), and a 20-min image was acquired 40 min later using a conventional γ-camera (Monad XLT; Trionix Research Laboratory) with a 20% energy window centered at the energy peak and a 256 × 256 pixel matrix. A lead pinhole collimator with a 5-mm aperture and a focal length of 18 cm was used, and the distance from the pinhole to the rats was approximately 6 cm.
To semiquantitate the level of myocardial 123I uptake from the images, 5 × 5 pixel-sized rectangular regions of interest were placed on the myocardial region showing increased uptake and on the upper mediastinal region (as background activity), from which ratios of cardiac to mediastinal counts (C/M ratios) were calculated.
Echocardiographic Assessment of Cardiac Dimensions and Function
Animals of Ad.EGFP.NIS (n = 9) and Ad.EGFP (n = 8) groups underwent serial echocardiography at baseline (day –1) and on day 4 and day 9 after myocardial gene transfer. After animals were anesthesized, anterior chest hair was removed with clippers, and the rats were secured to a table. Transthoracic echocardiography was performed with a 13-MHz linear transducer (model 15L8 probe; Acuson), and parameters were obtained using current ultrasound technology following the American Society of Echocardiography guidelines (21). Briefly, M-mode and 2-dimensional echocardiographic images were recorded in the parasternal long- and short-axis views, and thickness of the intraventricular septum and the posterior wall and LV dimensions were determined at the tips of the papillary muscle. LV end-systolic and end-diastolic areas were traced in single-plane apical 4-chamber view, and the ejection fraction was calculated following Simpson's rule using the modified single-plane method. LV mass was calculated with a regression formula using wall thickness and LV dimension values as used previously for adult rats (22).
Total Serum CK Assays
Separate Ad.EGFP.NIS-injected (n = 3) and Ad.EGFP-injected (n = 3) rats were evaluated for evidence of myocardial injury as assessed by CK and MPO activity and histologic findings. These animals underwent serial assays for serum CK activity at 3, 7, and 14 d after myocardial gene transfer. Rats that did not undergo any intervention (n = 3) were negative controls, and rats at 3 d after myocardial ischemia–reperfusion injury (n = 4) were positive controls. Serum was obtained from 100 μL of blood sampled from the tail vein, and quantitative determination of total CK activity was performed with the N-acetyl cysteine–activated assay method on an automated clinical chemistry analyzer (Roche Diagnostics).
MPO Assays and Histologic Assessment of Inflammatory Response
Rat myocardium extracted 14 d after Ad.EGFP.NIS or Ad.EGFP injection was snap-frozen (n = 3 for each group). Cryosections of 10-μm thickness were obtained, fixed in 0.5% glutaraldehyde, and then washed with PBS. The sections were stained with hematoxylin, and a single pathologist who was unaware of the study groups inspected the sections under a light microscope to assess the magnitude of inflammatory reaction. Sections were visually graded for the extent of inflammatory reaction as localized or diffuse and for the level of inflammatory cell infiltration as mild, moderate, or severe.
The remaining myocardial tissue was homogenized and assayed for MPO activity as an index of inflammatory injury following a previously described method (23). Briefly, weighed frozen myocardial tissue was mixed with 5 mL of ice-cold 5 mmol/L phosphate buffer (pH 6), freeze/thawed 3 times, sonicated, and then homogenized in 0.5% hexadecyltrimethyl ammonium bromide (Sigma) in 50 mmol/L phosphate buffer (pH 6). After centrifugation at 12,500g at 4°C for 15 min, the supernatants were collected and reacted with 0.167 mg/mL of o-dianisidine dihydrochloride (Sigma) and 0.0005% H2O2 (Sigma) in 50 mmol/L potassium phosphate buffer (pH 6). The change in absorbance at 460 nm at 25°C was monitored with a spectrophotometer for several minutes. Results are expressed in units of MPO per gram of wet weight, which is defined as the enzymatic activity that degrades 1 μmol of H2O2 per minute at 25°C. MPO activities in myocardial tissue of negative control rats and rats 3 d after myocardial ischemia–reperfusion were also assayed for comparison.
Data Analysis
The significance of difference in cell number, MTT assay results, cardiac radiouptake ratio, echocadiographic measurements, serum CK level, and MPO activity was analyzed by Student t tests. Data are given as mean ± SD or mean ± SE as indicated, and P values < 0.05 were considered significant.
RESULTS
Effect of Adenoviral Gene Transfer and 123I Incorporation on Cultured Cardiomyocytes
H9C2 cells stimulated with retinoic acid for 7 d exhibited positive staining for MLC-2v, consistent with cardiomyocyte differentiation of the cells. Infection of these cells with 10 MOIs of either Ad.EGFP or Ad.EGFP.NIS led to high transgene expression levels, as assessed by fluorescence intensities observed on day 2 (data not shown). There was no difference in viable cell numbers at 4 and 9 d between Ad.EGFP-infected, Ad.EGFP.NIS-infected, and uninfected control cells (with or without 123I treatment) (Fig. 1A). Similarly, there was no difference in MTT assay results at days 4 and 9 after Ad.EGFP or Ad.EGFP.NIS application, either with or without 123I treatment, compared with controls (Fig. 1B). These results indicate that, under our experiment conditions, neither NIS overexpression nor incorporation of 123I causes significant effects on cultured cardiac cell viability or proliferation.
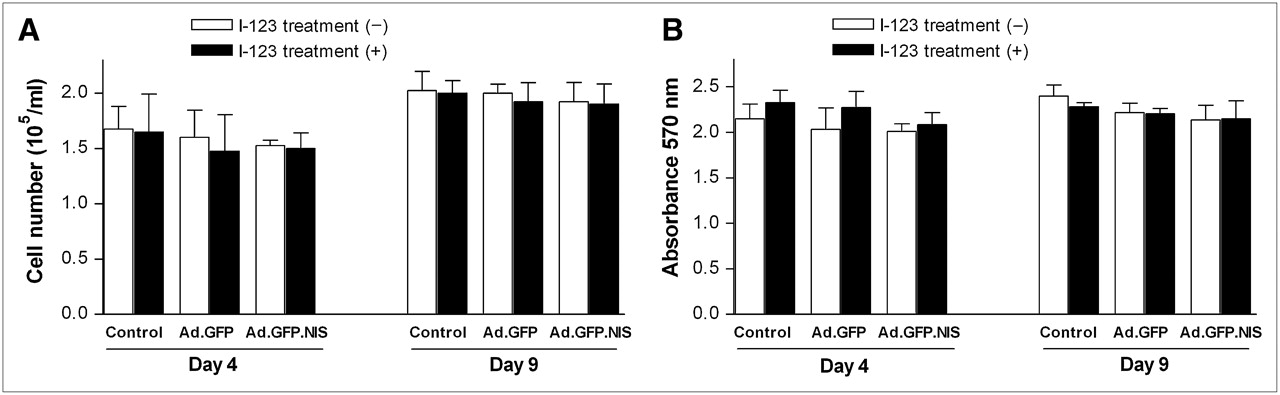
Effect of adenoviral gene transfer and 123I treatment on cultured cardiac cells. (A) Number of viable cells at 4 and 9 d after infection with 10 MOIs of Ad.EGFP or Ad.EGFP.NIS and in uninfected controls. Cells were incubated with 0 or 185 kBq (0 or 0.5 μCi) 123I for 6 h at days 4 and 9. (B) MTT assay results of cells treated as in A. Cells are H9C2 myoblasts differentiated into cardiomyocytes by stimulation with retinoic acid. All results are mean ± SD of 4 samples obtained from a single experiment (representative of 2 experiments).
Serial 123I Scintigraphy and Time Course of Cardiac Radiouptake
At 2 d after gene transfer, all 5 rats among the Ad.EGFP.NIS group that underwent 123I scintigraphy demonstrated intense focal radiouptake localized to the virus-injected region of the heart. Scintigraphy repeated at 4 d also showed high cardiac radioactivity of comparable intensity. In contrast, the same animals imaged at 9 d revealed a complete loss of cardiac radiouptake (Fig. 2A). Semiquantitative measurements of image-based C/M ratios closely corresponded to the visual findings: The ratio was high on days 2 and 4 (5.04% ± 0.62% vs. 5.09% ± 0.99%, respectively; P = not significant) but was dramatically reduced to blood-pool levels by day 9 (1.38% ± 0.05%; P < 0.0001 compared with 2- and 4-d levels; Fig. 2B). These findings indicate that NIS protein is present in high levels in the heart between 2 and 4 d after direct NIS adenovirus injection but declines to levels below the threshold for detection with 123I imaging by day 9.

Time course of cardiac 123I uptake. (A) Serial scintigraphic rat images at 2, 4, and 9 d after myocardial injection with 3 × 108 pfu of Ad.EGFP.NIS (n = 5). Arrow denotes focal cardiac 123I uptake consistent with site of adenovirus injection. (B) Semiquantitative C/M ratios expressed as mean ± SE of values obtained from 5 animals.
Serial Echocardiographic Measurements of Cardiac Function and Dimension
The results of serial transthoracic echocardiography measurements before and after myocardial adenoviral gene transfer are summarized in Table 1. At baseline, Ad.EGFP and Ad.EGFP.NIS group rats had similar heart rates, LV dimensions, and cardiac functional parameters, which are also consistent with previously reported values observed for normal Sprague–Dawley rats (21). Follow-up echocardiography demonstrated that, even after adenovirus injection, the Ad.EGFP and Ad.EGFP.NIS groups did not differ in heart rate, LV dimensions, and functional parameters at days 4 and 9. When postinjection parameters were compared with baseline levels, LV dimensions were increased slightly, and LVEF and LV fractional shortening (LVFS) were reduced slightly at day 9 for both Ad.EGFP and Ad.EGFP.NIS groups, but to similar magnitudes between the 2 groups. No arrhythmia or any other significant ECG abnormalities were observed during serial echocardiography in either AdV.EGFP.NIS or AdV.EGFP group.
Echocardiographic Measurements Before and Serially After Intramyocardial Ad.EGFP or Ad.EGFP.NIS Injection
Serum CK Activity and Myocardial MPO Levels and Inflammatory Cell Infiltration
Neither Ad.EGFP group nor Ad.EGFP.NIS group demonstrated a significant increase in serum total CK activity at 3, 7, and 14 d after myocardial transfer compared with negative controls. In contrast, positive controls that had undergone myocardial ischemia–reperfusion injury had serum CK levels elevated to 7-fold of negative controls (Fig. 3A). Similarly, myocardial tissue MPO activity 14 d after injection of Ad.EGFP and Ad.EGFP.NIS was not elevated compared with negative controls, whereas it increased significantly 3 d after myocardial ischemia–reperfusion injury (Fig. 3B).
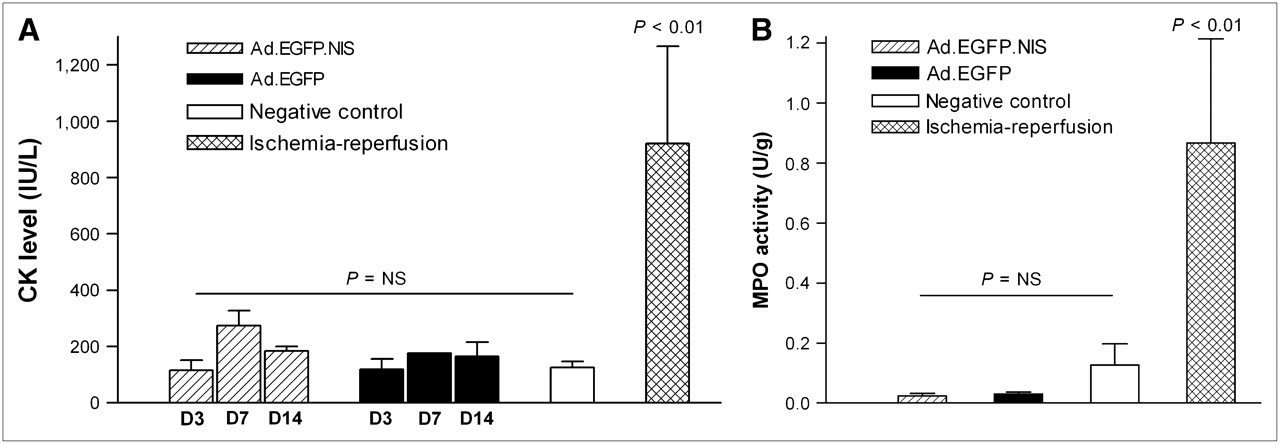
Serum CK and myocardial MPO activity. (A) Total serum CK activity (mean ± SE; IU/L) at 3 (D3), 7 (D7), and 14 (D14) d after myocardial injection of Ad.EGFP.NIS (n = 3) or Ad.EGFP (n = 3), in negative controls (n = 3), and at 3 d of ischemia–reperfusion (n = 4). (B) Myocardial MPO activity (mean ± SE; U/g) in rats as in A (14 d after adenovirus injection). NS = not significant.
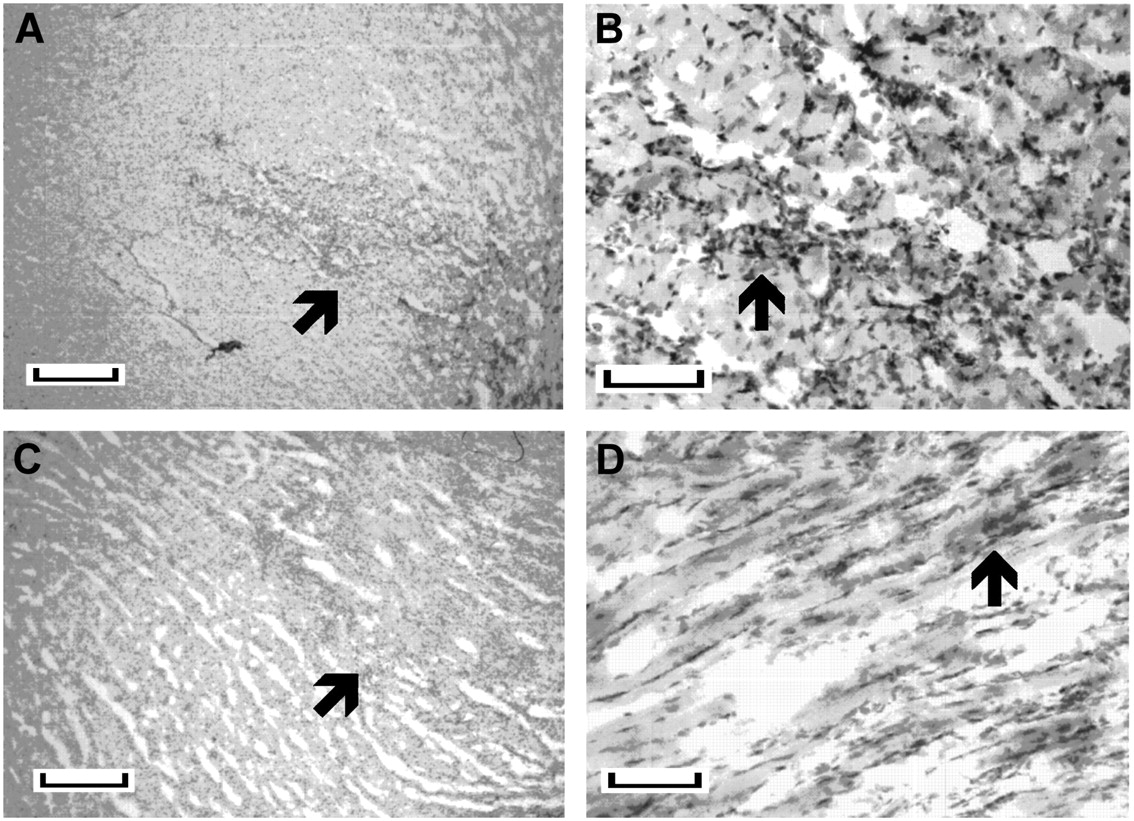
Microscopic inspection of myocardial microsections revealed comparable mild inflammatory cell infiltration restricted to relatively small areas, consistent with the injection site for both Ad.EGFP and Ad.EGFP.NIS groups (Figs. 4A–4D).

Hematoxylin-stained myocardial microsections obtained 14 d after intramyocardial injection of Ad.EGFP.NIS (A and B) or Ad.EGFP (C and D). Arrows indicate areas of localized inflammatory infiltration, consistent with injection site. Length of bar indicates 400 μm for A and C and 100 μm for B and D.
DISCUSSION
In this study, we show that adenoviral NIS gene transfer does not affect the viability or proliferation of cultured cardiac cells and that imaging of adenovirus-mediated cardiac NIS gene expression in living rats can be performed without significant injury or functional disturbance of the heart. Serially measured echocardiographic LV function and serum CK levels showed no difference between animals injected intramyocardially with Ad.EGFP and those injected with Ad.EGFP.NIS. Extracted myocardial tissue showed no increase in MPO activity, and histologic evidence of myocardial inflammatory injury was mild and restricted to the injected region for both groups of animals. These results demonstrate the safety of overexpressing NIS protein in the myocardium for reporter gene imaging, which appears to be as harmless on cardiac function as the widely used reporter EGFP.
Recombinant adenoviral vectors, such as those used in this study, are the most commonly used method of gene delivery to the cardiovascular system because they efficiently transfect quiescent myocardial cells, remain episomal without the risk of insertional mutagenesis, and produce robust transgene expression (4–6). Judging from the strong intensity of cardiac 123I uptake in our study, large amounts of NIS protein were expressed in rat myocardia at days 2 and 4 after Ad.EGFP.NIS injection. By day 9, however, cardiac NIS protein was reduced dramatically to levels below the threshold required for visible 123I uptake. The transient nature of gene expression after myocardial adenoviral gene transfer is a well-described phenomenon, which is attributed, in part, to the episomal nature of adenoviral DNA and also to host immune responses elicited by expression of proteins from nondeleted regions of the viral genome (4,24,25).
NIS is an integral plasma membrane protein of the basolateral membrane of the thyroid follicular cells that mediates a Na-dependent iodide transport process. Nonthyroid cells transduced with NIS cDNA exhibit increases of severalfold in perchlorate-sensitive iodide uptake (14). Although NIS protein is not normally present in cardiac cells, rat cardiomyocytes have been shown to express Na/HCO symporters, which are electrogenic and contribute to the modulation of the resting membrane and action potential (26). Because NIS activity mediates the intracellular influx of sodium and a variety of anions, and is also suggested to be electrogenic (27,28), there may be concern with regard to possible untoward effects of high NIS activity on contractile cardiac function. However, our results show that during the period of high NIS expression at 2 and 4 d after Ad.EGFP.NIS injection and the subsequent loss of expression at day 9, there was no significant difference in echocardiographically assessed cardiac function compared with Ad.EGFP-injected control animals.
On the other hand, both Ad.EGFP.NIS- and Ad.EGFP-injected rats did demonstrate a mild reduction in LVFS and LVEF to a similar degree at day 9 compared with preinjection baseline levels. This finding could be related to direct toxic effects or host-mediated immune responses from adenoviral or reporter proteins. NIS protein is an unlikely culprit as there was no difference in cardiac function between expressing both NIS and EGFP and expressing only EGFP. Rather, the mild functional effect observed is most likely due to proteins expressed by nondeleted regions of first-generation adenoviruses that can be directly toxic and are known to cause brisk immune responses in vivo (24,29). EGFP, a non-self transgene protein, has also been reported to induce a cytotoxic T-lymphocyte–mediated immune response in transplantable murine models (30) and may also have contributed partially to the observed effect.
However, myocardial damage in our study was limited, as serial blood tests did not show evidence of CK release, and myocardial MPO, an enzyme closely linked to cardiovascular injury, was not elevated (31). In addition, histologic examination revealed only mild inflammatory cell infiltration restricted to the region of needle insertion. These results are consistent with several previously published studies in different animal models that have shown the absence of cardiac enzyme elevation and minimal inflammation and necrosis after direct myocardial adenovirus injection (32–34).
The use of NIS as a reporter gene allows imaging of myocardial gene expression that is highly accurate (11,12) and is much less demanding because it can be performed using widely accessible conventional γ-cameras and inexpensive, commercially available radionuclides, without the need for complex on-site radiochemical synthesis. Furthermore, a recent study of myocardial NIS gene imaging using PET and 124I demonstrated higher signal intensity and superior imaging contrast compared with herpes viral thymidine kinase systems (13). The product of herpes viral thymidine kinase genes is accompanied by significant immunogenicity and may be potentially toxic to cells in the presence of nucleoside substrates. Therefore, the absence of significant myocardial injury or perturbation of cardiac function in this study illustrates another potential advantage for NIS genes over herpes viral thymidine kinase genes for myocardial reporter gene imaging.
CONCLUSION
Adenovirus-mediated NIS gene delivery for 123I imaging does not cause significant myocardial injury or adversely affect cardiac function, as assessed by echocardiographic measurements, cardiac enzyme assays, and histologic examination. Thus, this practical and convenient reporter gene strategy can be safely used for noninvasive myocardial gene imaging in living subjects.
Acknowledgments
The authors are grateful to Dr. Anthony Rosenzweig for invaluable discussion and guidance. This work was supported by Samsung grant SBRI C-A6-419-1. This work was presented, in part, at the 52nd Annual Meeting of the Society of Nuclear Medicine, Toronto, Ontario, Canada, June 18–22, 2005.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication April 13, 2006.
- Accepted for publication August 1, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.